
Abstract
Purpose. To broadly assess changes in key health behaviors (physical activity, fruit and vegetable consumption, smoking, and alcohol consumption) and one outcome (body mass index) between 2001-2006 and 2011-2016. Design. Repeated cross-sectional study. Setting. The United States of America. Participants. Noninstitutionalized adults age 24 to 39 participating in the National Health and Nutrition Examination Survey. Analysis. We used 2-sample t tests and χ2 tests to compare differences in health behaviors between the 2 time periods. Results. Data revealed a downward trend in both moderate and vigorous physical activity (P = .00), and fruit and vegetable consumption decreased (P = .003). Cigarette smoking decreased (P = .04), and there was no substantive change in heavy drinking between the 2 time periods. Body mass index was higher in the later time period (P = .00). Conclusion. Despite sustained funding efforts, we found little evidence that health behaviors improved between the 2 time periods. Indeed, many health behaviors have remained the same or worsened over time. These findings suggest the need to reflect on the appropriateness of the health promotion approaches being used.
Although there is substantial discussion of social determinants of health and interventions to improve the social ecology of health, a strong focus remains on changing individual health behaviors.
The World Health Organization’s 1948 constitution defined health as a state of complete physical, mental, and social well-being and not merely the absence of disease and infirmity. 1 Despite health being defined as the presence of well-being rather than an absence of disease, more effort has focused on eliminating disease and infirmity than on creating physical mental and social well-being. This can be seen by the focus on preventing specific health behaviors and outcomes in funding streams, for example, cancer prevention and cardiovascular disease prevention. The World Health Organization definition leaves open the possibility that these efforts should be flipped to focus primarily on positive physical, mental, and social well-being and secondarily on the negative health states of disease and infirmity to avoid or move away from. 2 As research has documented in health, 3 business, 4 psychology, 5 sports, 6 and the environment, 7 being stronger and more capable not only enables a better life and improved performance, it also results in the prevention of problems and/or a faster recovery from health-related or other difficulties that arise.
Research has repeatedly documented higher health and a lower burden of disease from engagement in multiple health promoting behaviors. Thus, health care providers and public health practitioners often focus on behavior change to prevent disease. Belloc and Breslow’s classic Alameda County study assessed 7 lifestyle habits (eating breakfast most days, sleeping 7 to 8 hours each night, rarely snacking between meals, maintaining a recommended weight, engaging in physical activity regularly, not drinking to excess, and not smoking) among study participants, and using these lifestyle behaviors, their results demonstrated that habits were cumulatively beneficial. Findings of this research indicated that the more of these behaviors participants regularly engaged in, the better their health. This study also highlighted the value and impact of lifestyle behaviors over other factors such as age. 8 These results and other reaffirming studies about the impact of lifestyle behaviors9-14 resulted in creating a focus for public health efforts on improving lifestyle behaviors.
Although there is substantial discussion of social determinants of health and interventions to improve the social ecology of health, a strong focus remains on changing individual health behaviors. Specific efforts to improve lifestyle behaviors that foster improved health are captured in the Healthy People Agenda, which began in 1990 and focused on creating social and physical environments that promote good health and healthy behaviors across a lifespan. Other governmental organizations, notably the Department of Health and Human Services and the National Institutes of Health, guided the promotion of behavior changes in the United States. Behavior change efforts were predicted to improve the US population’s health status. 15
Much of the focus on health behaviors has been on physical activity, fruit and vegetable consumption, reduction in alcohol consumption, and not smoking. To achieve health benefits and prevent disease and infirmity, recommended health behaviors for adults include engagement in 30 to 60 minutes of moderate to vigorous activity most days of the week. 16 Regarding fruit and vegetable consumption, the US Department of Agriculture recommends adults consume at least 2½ cups of vegetables and 2 cups of fruit per day, noting that more fruit and vegetable intake is better. Excessive drinking has been discouraged and not drinking or drinking only moderately has been recommended. Specifically, the recommendation suggests no more than 1 drink/day for women and 2 drinks/day for men. Due to overwhelming evidence of its negative health impacts, smoking has been discouraged. Body mass index (BMI), which measures and categorizes body weight based on height and weight as underweight, desirable (or normal weight), overweight, or obese, is an outcome of lifestyle behaviors. BMI is a commonly used comparable method for health status assessment; its quantitative nature provides an imperfect but effective impetus for health care professionals to discuss and address the behaviors that contribute to unhealthy BMI ranges. Maintenance of a normal BMI is recommended.
Following the focus on behavior change, progress in achieving improved health among the US population should be related to the extent to which individuals’ health behaviors have changed over time. Changes in the prevalence of health behaviors, both positive and negative, therefore indicate the areas where public health efforts have been effective and where more efforts are needed. However, past research suggests cause for concern. In 2014, the Centers for Disease Control and Prevention found that while some health behaviors had improved between 2005 and 2013, related health indicators did not always move in the expected direction. For example, changes in physical activity and blood pressure sometimes moved in opposing directions. These data provided conflicting information about health indicator trends, behavior changes, and health outcomes. 17 Looking at specific segments of the US population, other studies have noted disappointing decreases in harmful health behaviors over time. In one study that assessed changes in health behaviors between 1988 and 2006 among individuals aged 40 to 74, adherence to healthy habits (normal BMI, physical activity, smoking, fruit and vegetable consumption, and alcohol use) decreased for 3 out of 5 health habits. 18 In a Mississippi Delta study, similar trends of lower adherence to health behaviors were observed. 19
Therefore, this study evaluated data about health promoting actions in multiple areas to determine changes over time. Research on changes in health behaviors have commonly focused on older adults or adolescents. Less research has focused on adults aged 24 to 39, an age range during which health behaviors have a deciding impact on health status in later years. 20 This is also the age range during which many adults become parents and consciously or unconsciously model health behaviors for their offspring. 21 Prior research found that an individual’s 24th birthday marks the end of the period of time referred to as “emerging adulthood” 22 and is most likely the year of life in which individuals are likely to transition into the workforce. To determine the impact of recent efforts to promote healthy behaviors, this study assessed health behavior changes among adults aged 24 to 39 between the years 2001 and 2016 using National Health and Nutrition Examination Survey (NHANES) data. Data about engagement in behaviors to approach and increase such as physical activity and healthy food consumption were collected along with data about behaviors to limit or avoid, such as smoking and drinking. We also assessed changes in resultant BMI.
Methods
The NHANES data between 2001 and 2006 and between 2011 and 2016 were used in this study. NHANES is a biennial survey designed to collect individual-level information on health and nutrition. The survey collects a nationally representative sample from counties across the United States. Our use of public, anonymous surveillance data did not require approval by an ethics committee. Approximately 5000 participants from 15 counties are used to collect the data each year. Only participants whose ages were between 24 and 39 years were included in the current study.
Participants
A total of 9018 participants whose ages were between 24 and 39 years were in our study. More than half of them were females (53.3%), had at least some college (57.8%), and were married (51.0%). The average BMI was 28.60 (SD = 7.05), and average fruits and vegetable consumptions was 375.47 g (SD = 363.27 g). Table 1 details participants’ characteristics.
Characteristics of Participants.
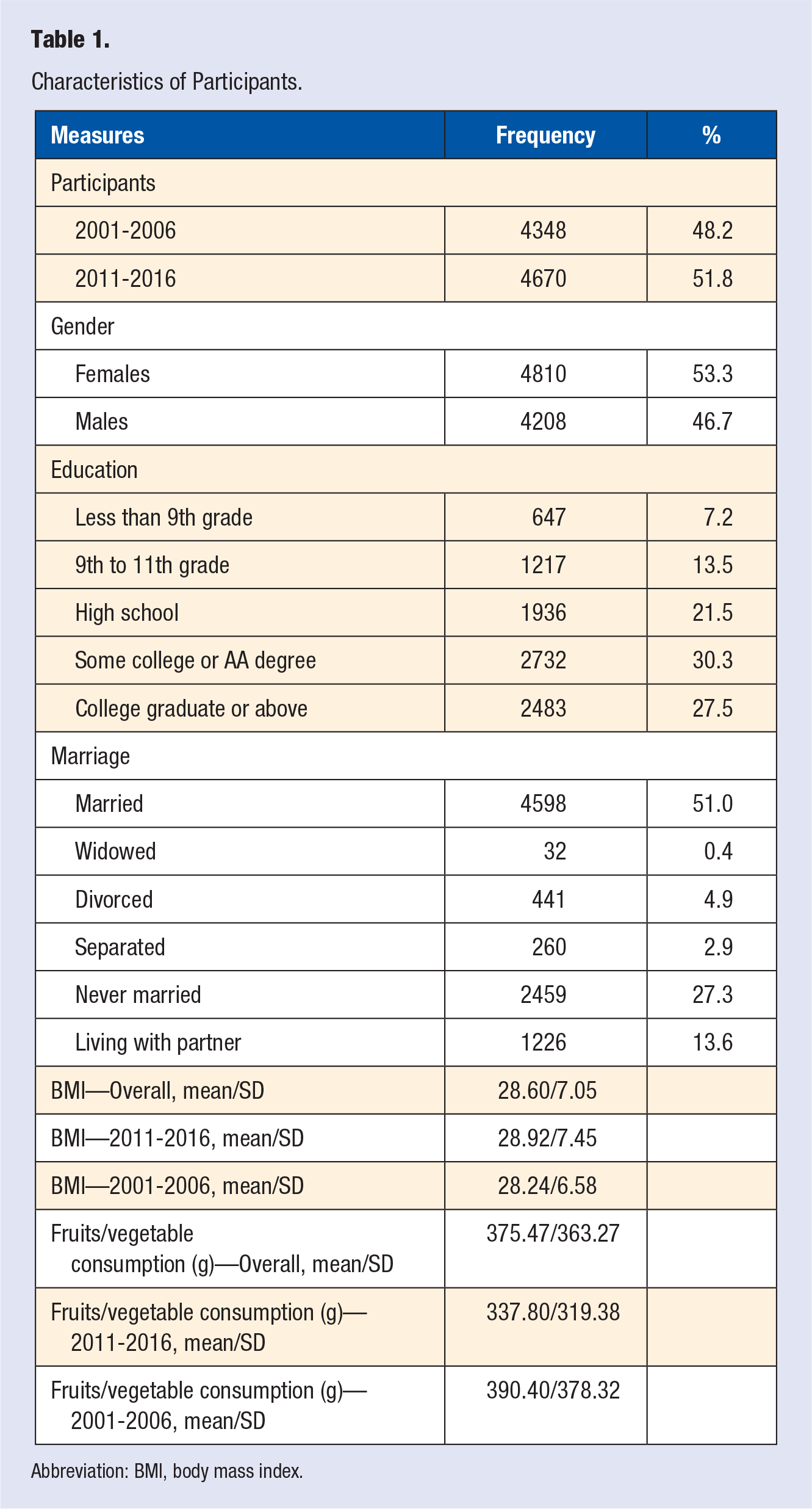
Abbreviation: BMI, body mass index.
Measures
In addition to the behaviors below, we assessed demographic measures of gender, age, education, marital status, height, and weight.
BMI was calculated using height and weight. Then it was categorized into 4 levels, underweight, normal weight, overweight, and obese, based on the classification from the World Health Organization. Underweight is defined as BMI below 18.5. The range of BMI for normal weight is between 18.5 and 24.9. BMI ranging between 25.0 and 29.9 is defined as overweight. A BMI value of 30.0 or above is classified as obese.
Fruits/Vegetables
Fruits and vegetables intakes were measured in grams by recalling the types and amounts of fruits and vegetables consumed during a 24-hour period before the interview.
Physical Activity
Vigorous and moderate physical activities were 2 binary measures with yes and no as response options. The measure used from 2001 to 2005 assessed the physical activities over the past 30 days. However, the measure used from 2006 to 2016 assessed the physical activities in a typical week.
Alcohol Use
Two measures were used to assess drinking behavior. One question was about the number of days of drinking over the past 12 months. The other question only focused on the participants who drank in the past 12 months. It recorded the average number of drinking on those days that participants drank. Two measures and gender were used to obtain a new measure that categorized alcohol use into 3 levels: none, moderate drinking (1 drink per day for females and 1-2 drinks per day for males), and heavy drinking (more than 1 drink for females and more than 2 drinks for males).
Cigarettes Smoking
Smoking status was categorized as nonsmokers, former smokers, and current smokers following a standard practice. 23 The first question asked if participants smoked at least 100 cigarettes in life with yes and no as response options. The second question asked if participants now smoke cigarettes. The response options included every day, some days, and not at all. For everyone who replied “No” to the first question, those respondents were defined as “nonsmokers.” For people who replied “Yes” to the first question but “not at all” to the second question, those respondents were defined as “former smokers.” For people who replied “Yes” to the first question but “every day” or “some days” to the second question, those respondents were defined as “current smokers.”
Data Analysis
Data were analyzed using SPSS version 24.0. Associations between year and outcomes including BMI with 4 categories, vigorous and moderate physical activities, smoking, and drinking were assessed by χ2 tests. The differences of BMI values and consumptions of fruits and vegetables over time were examined using an ANOVA test. Because we combined multiple years and were interested in a comparison of trends rather than population estimates, we did not use NHANES survey weights.
Results
In terms of physical activities, both moderate and vigorous physical activities showed a downward trend. There were significant associations between moderate/vigorous exercise and year, Ps < .5. People in 2001 to 2006 were 1.38 times more likely to get moderate physical activities than those in 2011 to 2016 (odds ratio [OR] = 1.38, 95% confidence interval [CI] = 1.27-1.50). People in 2001 to 2006 were also 1.16 times more likely to have vigorous physical activities than those in 2011 to 2016 (OR = 1.16, 95% CI = 1.07-1.27). ANOVA tests also revealed a significant difference in fruit and vegetable consumption. Participants consumed fewer grams of fruits and vegetables in 2011 to 2016 (mean [M] = 337.80, SD = 319.38) than in 2001 to 2006 (M = 390.40, SD = 378.32), F(1, 2003) = 8.58, P = .003, η 2 = .004.
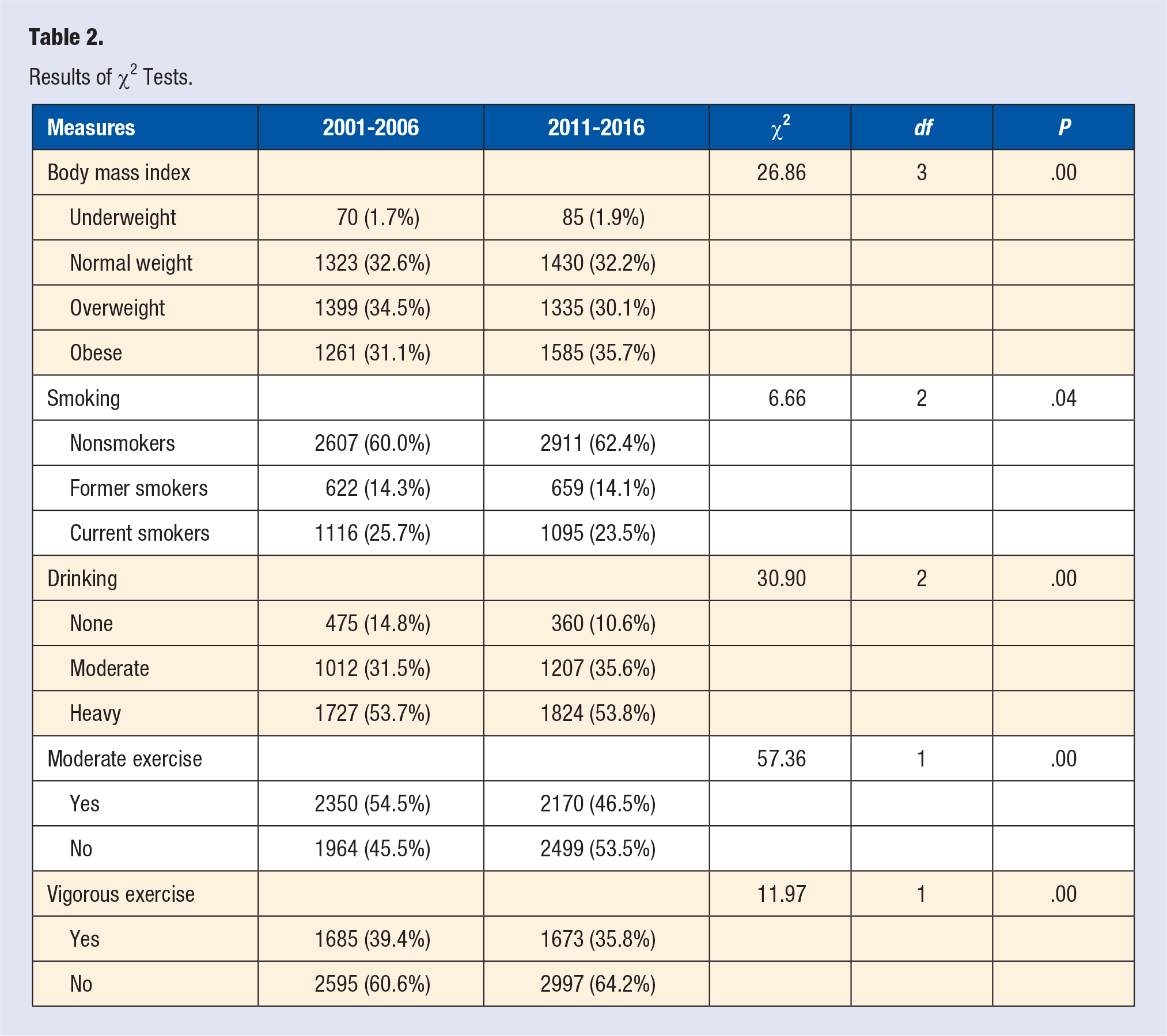
ANOVA test results showed people in 2011 to 2016 (M = 28.92, SD = 7.45) had higher BMI than in 2001 to 2006 (M = 28.24, SD = 6.58), F(1, 8486) = 19.79, P = .00, η 2 = .002. Chi-square tests indicated significant associations between all health-related outcome measures and year, Ps < .05 (Table 2). More people in 2011 to 2016 reported obesity (35.7%) than in 2001 to 2006 (31.1%). As for smoking status, fewer smokers were identified in 2011 to 2016 (23.5%) than in 2001 to 2006 (25.7%). There was no substantive change in heavy drinking between the 2 time periods (53.7% vs 53.8%). However, moderate drinking increased in 2011 to 2016 (35.6%) compared to the percentage in 2001 to 2006 (31.5%).
Results of χ2 Tests.
Discussion
A desired societal goal is to create an environment that encourages, nurtures, supports, and reinforces continued engagement in multiple health promoting actions. Yet we found that for several behaviors, progress between the 2 time periods studied was limited. The NHANES evidence evaluated for this study indicates that, between the years of 2011 and 2016, individuals were not as engaged in moderate or vigorous activity and ate fewer fruits and vegetables. Although heavy drinking did not increase markedly, fewer abstained from drinking and more drank moderately between 2011 and 2016 than did between 2001 and 2006. More positively, smoking rates were lower between 2011 and 2016 than they were from 2001 to 2006. Therefore, the data do not provide evidence of progress toward health promoting actions, despite the substantial resources society has directed toward preventing disease through lifestyle behavior change efforts.
There are 2 implications of our findings: First, these are concerning because food selection choices, the amount of engagement in physical activity, and alcohol consumption have profound impacts on health status. 24 As noted, cumulative health behaviors are important, and these changes were associated with expected increases in BMI. The trend has moved in the wrong direction for several lifestyle behaviors evaluated. Second, these findings may provide an opportunity to reflect on the appropriateness of the approaches being used.
If the current focus on lifestyle behaviors is less effective than desired, research suggests several potential pathways for the future. A multidimensional approach for health improvement should be obvious, because, as noted, health includes physical, social, and mental dimensions. Even so, a single dimensional strategy of risk avoidance and prevention has been used. Evidence from this study indicates existing strategies may be insufficient. Better success was noted from efforts in the area of smoking. 23 Smoking rates have decreased due to multidimensional efforts that included education, bans, and tax increases. These efforts however were focused on trying to inhibit or make undesirable behaviors difficult rather than incentivizing and/or supporting desired behaviors. This suggests multiple approaches are needed to improve the complex of behaviors related to health and disease outcomes. Discouraging trends in health behaviors, as noted in this and other studies, may suggest the use and/or at least the complementary use of multidimensional approaches that includes salutogenesis. A salutogenic approach asks how a person can be moved toward greater health and aims to instigate health causing actions.2,25 This approach may help because research suggests positive physical, social, and mental well-being gains, not merely avoiding disease and infirmity, increases a person’s intention to engage in health promoting actions. 26
Possible influential issues beyond the scope of this article include differences by age and changes to norms of health behaviors or what is considered healthy. For example, future research should investigate if the same pattern of results exists across the life course and if the noted increase in BMI has altered societal norms and how this may affect health behaviors. While some research has associated lower risk with improved health, these findings have not been consistent.10,17 Health promotion, a salutogenic health causing strategy, and prevention, a pathogenic disease preventing strategy, are complementary. 2 Developing an environment that makes healthy behaviors the default and easier or more likely while simultaneously discouraging disease-causing actions would help increase capacity and potential because of increased engagement in health-developing actions. This study indicates efforts to encourage more health promoting actions is needed because engaging in health behaviors have been associated with improved health and lower incidences of disease and infirmity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our use of public, anonymous surveillance data did not require approval by an ethics committee.
Informed Consent
For this type of study formal consent is not required.
Trial Registration
Not applicable, because this article does not contain any clinical trials.