
Abstract
“The five-factor model was deemed the most appropriate due the stronger conceptual alignment to the sleep construct.”
Introduction
Lifestyle medicine is the use of evidence-based lifestyle interventions, including physical activity, nutrition, stress management, restorative sleep, avoidance of risky substances, and social connectedness, to treat and manage disease. 1 Comprehensive lifestyle medicine approaches can effectively prevent and treat chronic diseases. The lifestyle medicine discipline is centered around six evidence-based pillars that are deeply connected to well-being as well as disease prevention and management.2,3 This six-pillar framework promotes actionable behavior changes that can have a substantial impact on physical and mental health.
The Lifestyle Medicine Pillars are as follows
3
: 1. Nutrition: A whole-food, predominantly plant-based diet high in fiber and nutrients. This diet is comprised of mostly minimally processed vegetables, fruits, whole grains, legumes, nuts, and seeds. 2. Physical Activity: Daily movement and intentional exercise with the goal of accumulating 150 minutes of moderate intensity physical activity each week. Physical activity should be consistent and include both aerobic and resistance training. 3. Social Connectedness: Healthy social relationships and social networks are essential to physical and mental health. 4. Stress Management: Preventing chronic stress through healthy stress management strategies promotes longevity and mental and physical well-being. 5. Avoidance of Risky Substances: Assessing and addressing the use of risky substances, including tobacco and excessive alcohol, is critical for health. The American Heart Association recommends if people do not drink, they should not start. If people do drink, the American Heart Association recommends limiting the quantity to one drink for a woman and 2 drinks for a man.
4
6. Sleep: Restorative sleep, between 7 to 9 hours with minimal interruptions, is critical for physical and mental health.
The practice of lifestyle medicine is deeply rooted in health behavior changes theories including the transtheoretical model of change, self-determination theory, and the multiple behavioral approach.5,6 The multiple behavioral approach in particular can serve as a theoretical grounding for assessment with lifestyle medicine interventions. The multiple behavioral approach posits that there are connections between lifestyle behaviors, and that successful health behavior change is more likely when working across multiple behaviors. 6 To align with the multiple behavioral approach, assessment tools in lifestyle medicine should by multidimensional and simultaneously assess each of the pillars of lifestyle medicine.
Despite evidence of effectiveness, lifestyle medicine programs and interventions are not widely used in clinical and community settings. This is in part due to the lack of standardized methods of evaluation in the lifestyle medicine field. 7 There is a need for improved psychometric evaluation in health behavior research.8,9 The Health-Promoting Lifestyle Profile-II has been validated in students and international subgroups.10–12 While this measure has strong psychometric support, it is 52 items without demographic items. 13 This length may result in substantial participant burden which can influence response quality. 14 Moreover, the Health-Promoting Lifestyle Profile-II includes health practices that are outside of the scope of lifestyle medicine (i.e., “Indicate the frequency with which you ‘get a second opinion when I question my health care provider's advice’.”). 13 While there are a number of validated instruments that measure lifestyle medicine health behaviors individually, they do not comprehensively assess all six pillars and were not designed for lifestyle medicine program evaluation.15–20 Thus far, there are limited instruments specifically designed for the lifestyle medicine field and very few that have undergone rigorous scale development and psychometric evaluation. 9 A recent lifestyle medicine assessment tool with five components to measure the six pillars demonstrated content and face validity, but did not include a comprehensive psychometric evaluation with tests of dimensionality and reliability.7,8 Additionally, this measure groups items into constructs including connection, movement, substance use, recovery, and nutrition, as opposed to using the six-pillar framework. Many lifestyle medicine programs are utilizing a combination of assessment tools such as the Generalized Anxiety Disorder Screener (GAD-7) 21 and the PHQ-9, 22 but these tools do not explicitly or comprehensively assess lifestyle medicine health behaviors. There are also invalidated tools being used in the field such as the PAVING the Path to Wellness Questionnaire 23 and the Loma Linda and American College of Lifestyle Medicine (ACLM) Lifestyle Medicine Assessment Tool long form and short form. 24 Both of these assessments include questions around the lifestyle medicine pillars in addition to other constructs such as purpose, motivation, weight management, and general health. However, there are not published psychometric evaluations of these assessments at this time. Additionally, the length of these assessments could contribute to participant burden and may hinder the validity of responses. 14
There is a need for comprehensive, short measures with established construct validity and reliability to assess the six pillars of lifestyle medicine in order to fill this gap in research and practice. Establishing “best practice” models and evaluation tools for lifestyle medicine can scale the field and change how health care is delivered to promote whole-person well-being. 25 This study describes the development and psychometric evaluation of the Lifestyle Medicine Health Behavior (LMHB) scale, a multidimensional evaluation tool that comprehensively and individually assesses the six pillars of lifestyle medicine.
Methods
Pilot Study
Literature Review
The steps outlined by Lambert & Newman and other literature on psychometric evaluations26,27 for construct development and validation were used as a guide for this psychometric evaluation (2023), thus the LMHB scale was first developed based on an extensive literature review and expert input. 15 The LMHB scale intends to assess changes in six lifestyle medicine health behaviors, which are known to support chronic disease prevention, management, and reversal. 3 Therefore, the literature review was conducted with 2 aims: define the pillars of lifestyle medicine in the context of existing literature and identify existing measures of each of the pillars. 26 The literature from lifestyle medicine and behavior change science was reviewed extensively and the Lifestyle Medicine Handbook: An introduction to the power of healthy habits by Frates et al. 3 was used to operationalize the six pillars into constructs (2021).
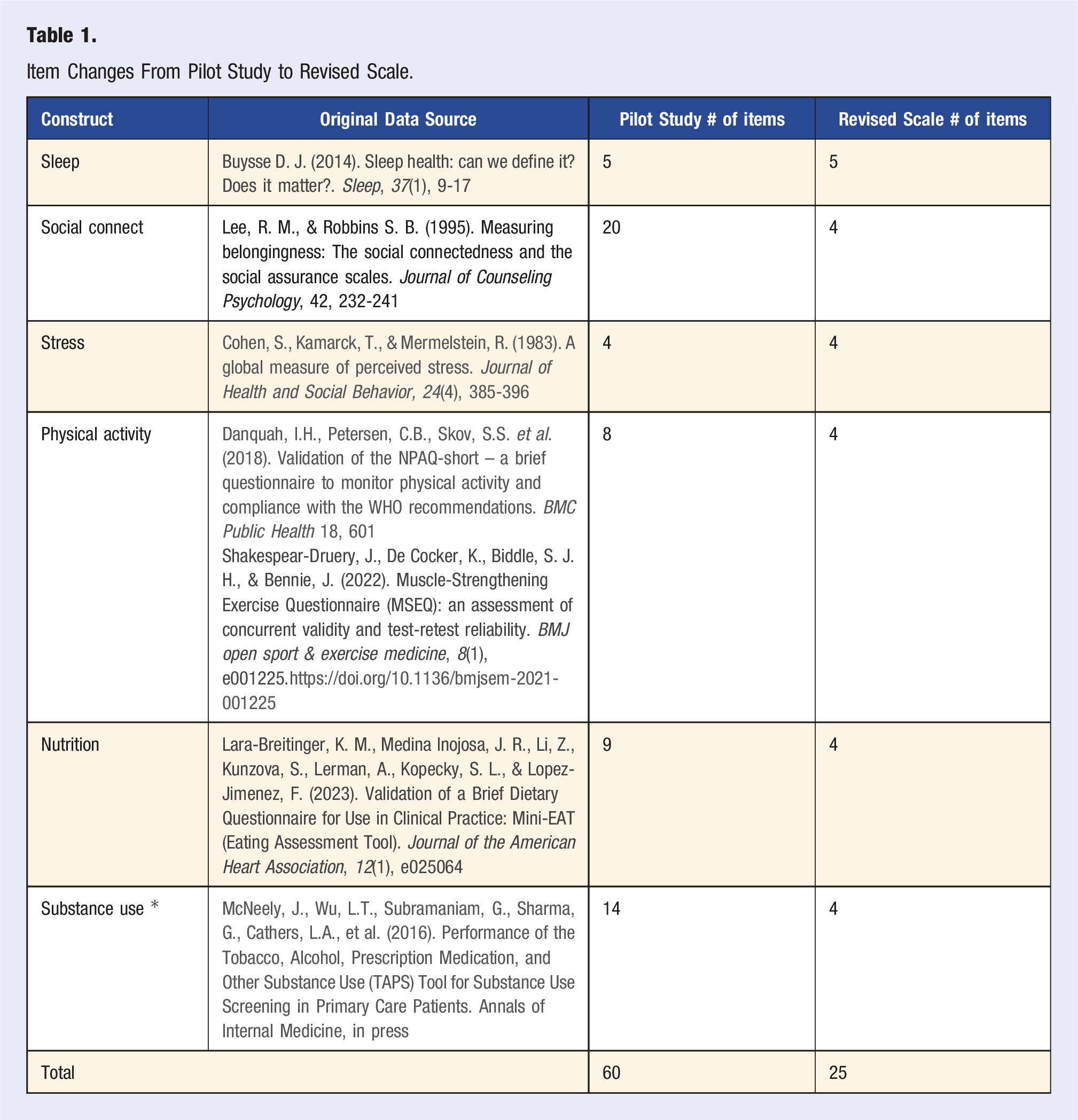
Once existing literature was used to operationalize the six pillars, the definitions were compared with potential measures. 26 Measures for sleep, 16 social connection, 17 stress management, 18 physical activity,19,20 nutrition, 28 and avoidance of risk substances 29 were selected. Seven established, validated scales were reviewed in detail based on their alignment with one of the six pillars of lifestyle medicine: the RU-SATED, a 5-item multidimensional sleep and wakefulness scale 16 ; the Social Connectedness and Social Assurances scales, a 20-item belongingness scale 17 ; the Perceived Stress Scale, a widely used 4-item scale measuring perception of stress 18 ; the 6-item Muscle-Strengthening Exercise Questionnaire 20 20 and the 2-item Nordic Physical Activity Questionnaire-short 19 were both used to assess resistance training and minutes of physical activity, respectfully; the Mini-EAT, a 9-item dietary assessment screener 28 ; and the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST-Lite), a 7-21-item rapid screening tool. 29 The items from these previously validated scales were used to develop the preliminary scale. The scales were used in their entirety for the pilot testing (∼53 items depending on ASSIST-Lite responses). The intention was to use the pilot testing to develop a revised scale with fewer items and eliminate any items that did not align with the lifestyle medicine field. The aim was to develop a survey with a low participant burden so that it could be widely adopted by lifestyle medicine practitioners for a variety of patient populations. The target range was 25-30 questions to keep participants’ interest and promote appropriate response rates. 14 A minimum of 3 items per construct were retained to maintain internal consistency reliability. 15
Pilot Testing Data Collection
Pilot testing was conducted in June 2023 with a convenience sample. A convenience sample was deemed appropriate to test this measurement model because the general population is representative of the population of interest at this stage. 30 The survey was shared via a Qualtrics link with the team’s network. The survey link was shared broadly via email and social media. Participants could complete the survey using a phone, tablet, or computer. Participants needed access to stable internet or data service to complete the survey. After providing consent, participants completed the survey. All questions were optional to reduce participant burden and any discomfort associated with the study. There was no compensation for survey completion. This study has been certified as exempt from IRB review by the Colorado Multiple Institutional Review Board (IRB#: 23-1296).
Pilot Testing Data Analysis
The psychometric properties of the pilot instrument were tested using principal component analysis. Items with low factor loadings (<0.5) 31 those not conceptually aligned with the lifestyle medicine field were removed based on the data analysis results and expert feedback (see Expert Group for more information).
As previously mentioned, the pilot survey was comprised of the full versions of each selected scale. To establish convergent validity between the full scale and the proposed abbreviated version, a mean score was created for each construct to create the overall construct score. A Pearson’s correlation of the average scores for each construct in the LMHB and the validated measures was conducted. We saw moderate to strong correlations between the constructs measured in the LMHB and the validated questionnaires. 32 The correlations for each construct are as follows: sleep r = 0.72, P < 0.001; nutrition r = 0.69, P < 0.001; social connectedness r = 0.82, P < 0.001; and substance use = 0.693, P < 0.001. All these values were above r = 0.50, indicating sufficient correlation to support the convergent validity of the scales. 33
Item analysis with principal component factor analysis was used to analyze preliminary construct validity within each scale of interest. Bartlett’s test of sphericity and the Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy were analyzed to assess how appropriate the items are for factor analysis. The results revealed that Bartlett’s test was significant at P < .001 for all items, supporting suitability for the principal component analysis. The KMOs ranged from 0.402 to 0.909. The KMOs over 0.70 were deemed appropriate for analysis. The constructs with lower KMO values may be due to the small sample size.
Dimensionality was assessed using principal component analysis to assess the internal structure validity of the lifestyle medicine constructs. The principal component analysis looked at each of the six pillars and the items for each construct to see whether the items had a similar pattern of responses. First, eigenvalues were examined to understand the amount of variance explained by each factor. Eigenvalues over 1.0 were retained. A Varimax rotation along with the scree plots were used to examine the significant factors. Factor loadings of the Varimax rotation were examined to understand the patterns across the items. Values over 0.40 with low cross-loading were deemed significant. 30 The values ranged from 0.36 to 0.86. The high values indicated that the item strongly relates to that component. We also calculated the Cronbach’s α coefficients.
Expert Group
An initial pool of 36 items was screened by experts for content validity to ensure the items measured the six constructs of interest. 34 These items were selected from the proposed validated instruments. The LMHB scale was reviewed by 5 experts, including 3 board-certified lifestyle medicine physicians and 2 researchers with survey methods expertise. Experts were asked to rate how representative the item was in measuring the overarching construct (pillar) on an ordinal scale of 1-4. Experts were also asked for open-ended feedback.
After the review, the feedback was reviewed and discussed with the research team, which included 2 board-certified lifestyle medicine physicians with 15 years of experience in the field and leadership roles in the American College of Lifestyle Medicine. Input from these lifestyle medicine leaders guided the final item selection from proposed validated scales. The decision was made to remove the ASSIST-Lite 29 and replace it with the TAPS tool 35 based on feedback. An open-ended question was also added to assess participant experience with the questionnaire.
Item Changes From Pilot Study to Revised Scale.
Psychometric Evaluation
Data Collection
Participants completed the survey immediately after providing consent. Data collection occurred between August and December 2024. The survey was shared via a Qualtrics link with the team’s network and through the Prolific.ac platform. 36 Prolific Academic collected data from their pre-existing sample using a globally representative population with equal proportions of males and females. The same data collection protocol that used for the pilot survey was utilized again with revised scale.
Survey Instrument
The questionnaire included the revised lifestyle medicine items (25), sociodemographic items (6), and an open-ended feedback item (1). The lifestyle medicine items were pulled from 7 different validated instruments (Table 1), with 3 of the instruments (social connectedness, nutrition, physical activity) adapted to remove items. Sleep 16 included five items (e.g., do you sleep between 6 and 8 hours per day?). Responses included “Never, Rarely, Sometimes, Usually, Always.” Social connection 17 included 4 items (e.g., I feel distant from people). Responses included “Strongly disagree, Disagree, Mildly agree, Agree, Strongly agree.” Stress management 18 included 4 items (e.g., in the last month, how often have you felt that you were unable to control the important things in your life?). Responses included “Never, Almost never, Fairly often, Very often.” Physical activity 19 , 20 included 4 items from 2 different tools. The first 2 items asked about minutes of activity (e.g., on a typical week, how much time do you spend in moderate and vigorous physical activities where your heartbeat increases and you breathe faster? (e.g., brisk walking, cycling, heavy gardening, running, or recreational sports?)). Responses included “Less than ½ hour (less than 30 minutes), ½ an hour - 1 hour (30-90 min), 1 ½ - 2 ½ hours (90-150 min), 2 ½ - 5 hours (150-300 min), More than 5 hours (more than 300 min.)” 19 The second tool was used to ask about resistance training (e.g., do you muscle-strengthening exercise in a usual week?). Responses included “Yes” and “No.” 20 Nutrition included 4 items on dietary intake (e.g., how often do you eat fresh fruits?). Responses included “I do not eat it at all, Less than 1 serving per week, 1-2 servings per week, 3-4 servings per week, 5-6 servings per week, 1 serving per day, 2-3 servings per day, 4-5 servings per day, 6 or more servings per day.” 28 Avoidance of risk substances 35 included 4 items (e.g., how often have you used any tobacco product? For example, cigarettes, e-cigarettes, cigars, pipes, smokeless tobacco). Response options included “Daily or almost daily, Weekly, Monthly, Less than monthly, or Never.” To assess face validity, participants were also asked to share feedback on the survey through an open-ended question (e.g., please provide feedback on this survey. For example, was the survey easy to understand? What would you change about the sequence or wording of questions? How easy or difficult was it to complete this survey and why?).
Data Management
After data collection was completed, the data were cleaned in SPSS and recoded numerically. Cases with 100% of data missing were deleted. Once the data were clean, missing data ranged from 0.30%–5.50%, depending on the item. Given the low percentage of missing data, listwise deletion was used with missing data. A codebook was created, and numeric values were given to each response. Data were transferred to SPSS V.26 for analysis. 37 Once the data was in SPSS, new variables were created for the mean scores of each scale. Reverse-coded items were identified, and new variables were created prior to analysis.
Data Analysis
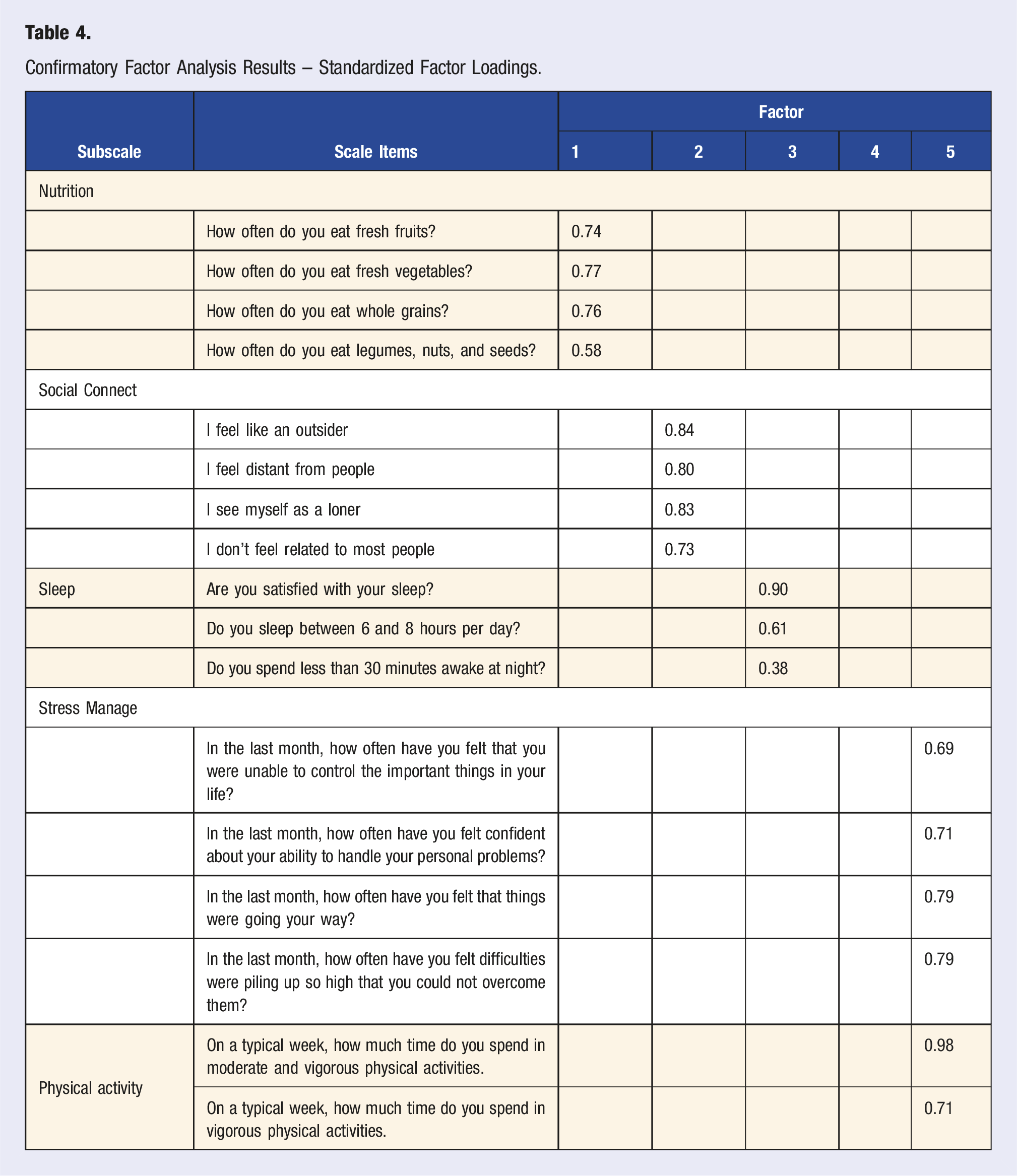
We computed all items’ descriptives (frequencies, means, and standard deviations). We assessed inter-item correlation across items and between constructs to determine whether the items measured distinct constructs. We then conducted confirmatory factor analysis (CFA) in Mplus V.8 38 using Geomin oblique rotation and maximum likelihood estimation. CFA was chosen for this initial validation because we were interested in assessing the dimensional structure of the LMHB scale. 39 We examined the eigenvalues, screen plots, goodness or fit statistics, and parameter estimates to determine an appropriate factor structure. A five-factor model was hypothesized based on the pilot study and the literature. We expected items from each scale to load on the corresponding construct. Substance use was not added to the model, as this was treated as an observed variable. We also examined the Cronbach’s α coefficients between item correlations and α-if-item deleted values as necessary. Cronbach’s α was chosen to assess internal reliability due to its prevalence in health behavior and medical education research.40,41
Results
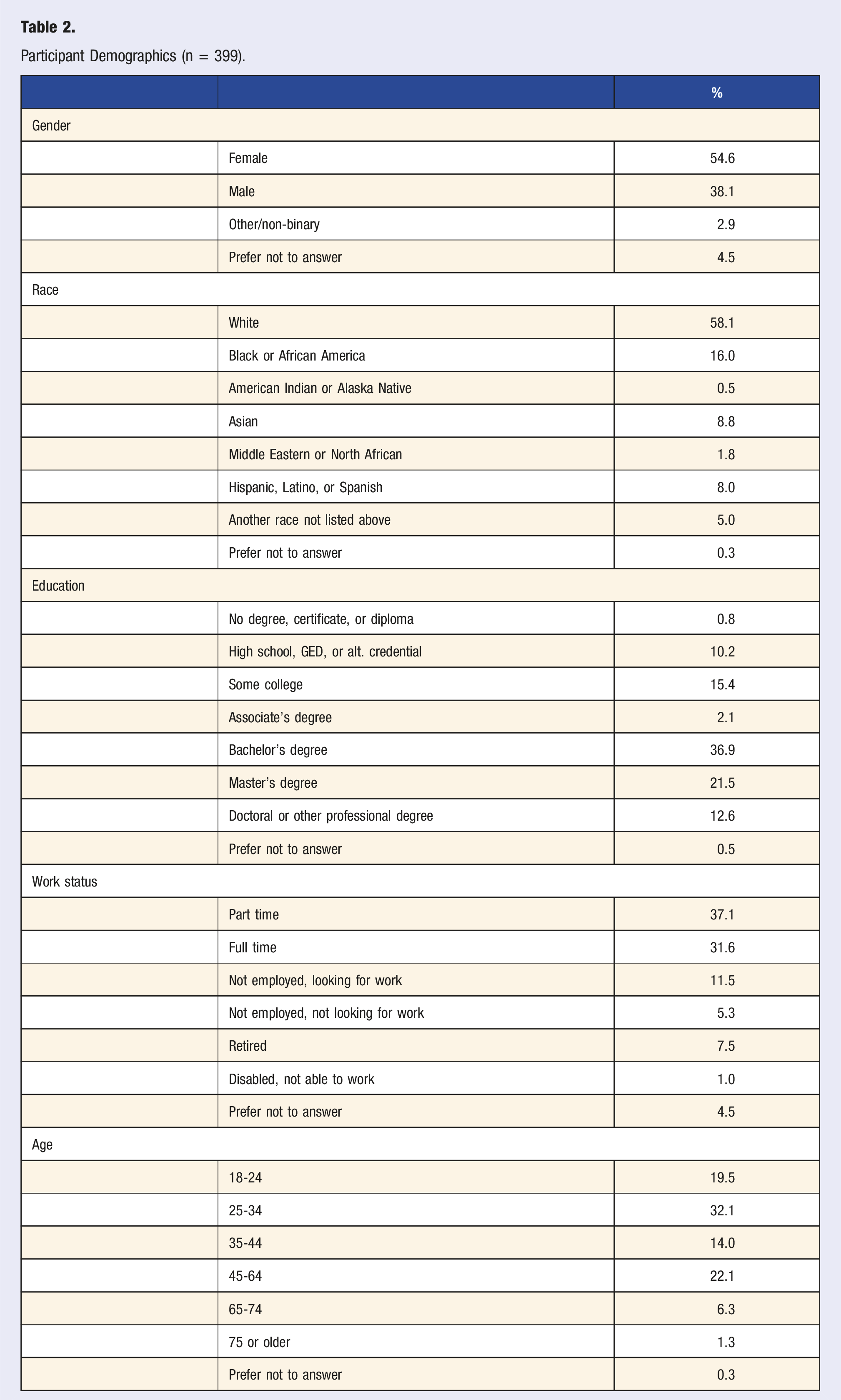
Participant Demographics (n = 399).
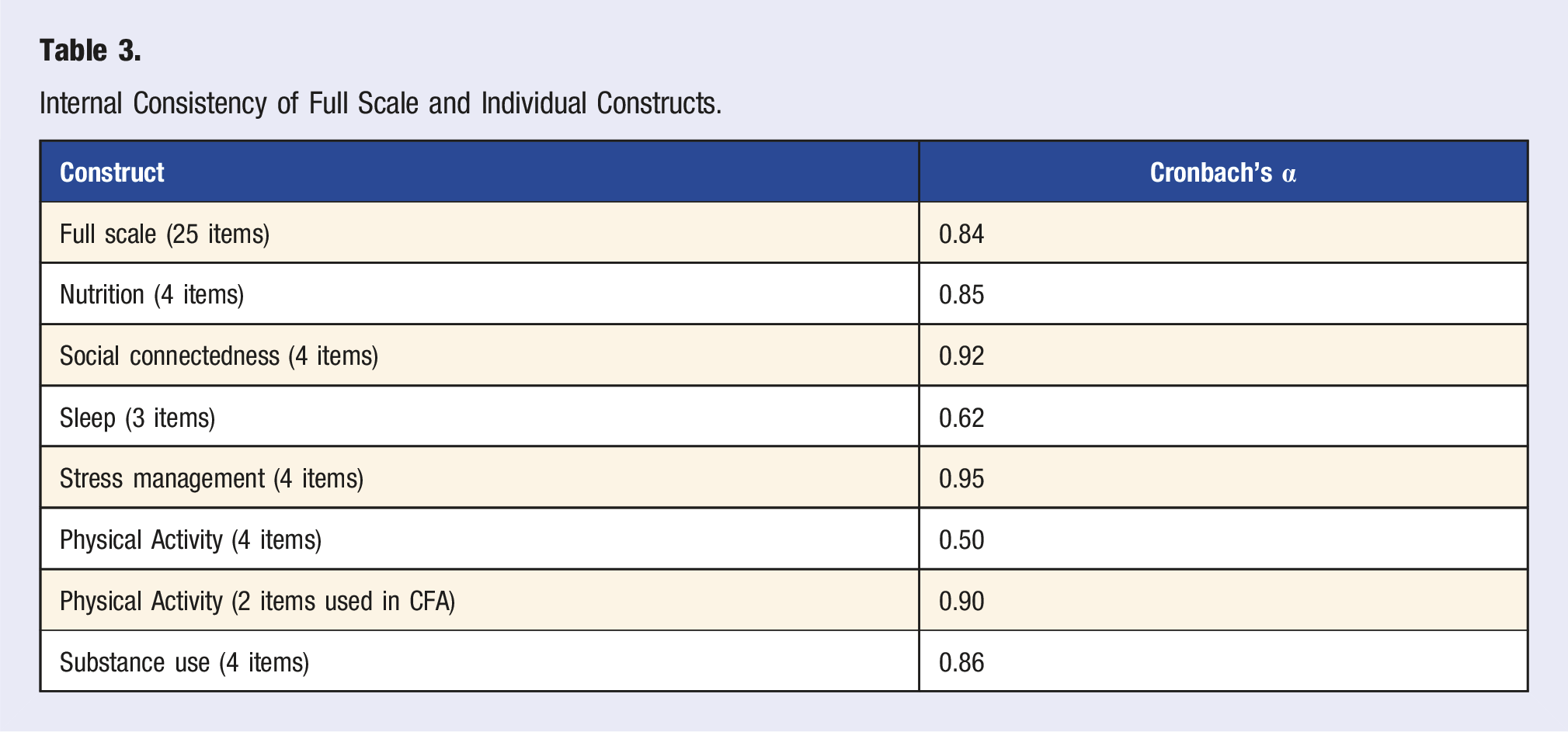
Internal Consistency of Full Scale and Individual Constructs.
Confirmatory Factor Analysis Results – Standardized Factor Loadings.
Participants (n = 120) responded to the feedback item to assess face validity. Approximately 80% of the feedback was positive, with the overwhelming majority discussing how the survey was, “easy to understand.”
Discussion
The LMHB scale was found to be a valid and reliable measure of the six lifestyle medicine pillars in this large sample. Construct validity was confirmed through testing the measurement model and examining reliability with a pilot and larger sample. 15 , 31 The six-factor model with sleep as 2 separate constructs had the strongest model fit. This is unsurprising, as previous validation work on the RU-SATED questionnaire, the source of the sleep items, revealed similar results, indicating that the five items are not intended to load highly together. 45 , 46 This was also consistent with the pilot study data conducted by the researchers. Given the existing literature and pilot work with the RU-SATED questionnaire, 46 the five-factor model was carefully considered and compared to the six-factor model. Ultimately, the five-factor model was deemed the most appropriate due the stronger conceptual alignment to the sleep construct. The final model was a five-factor model as originally proposed, with a factor to represent each of the latent constructs.
The social connectedness (α = 0.92) and stress management (α = 0.95) subscales formed highly reliable subscales, indicating that these scales will consistently measure the construct of interest in the same way each time. The 4-items used for physical activity were not very reliable (α = 0.50), but when just the 2 used in the CFA were tested, the items were reliable (α = 0.90). Overall, the full scale had adequate construct validity, addressing a key need that has not yet been done in lifestyle medicine survey validation work. 7 That said, the assessment of reliability of the LMHB scale need to be built upon; it is essential to assess the reliability of the scale across time and with patient populations of interest.47,48
As discussed in the methods, content validity was established through an expert panel review prior to the pilot testing. Reviewers felt that most of the items were representative of the intended construct. Necessary revisions were made, but careful consideration was taken not to modify the structure of the previously validated instruments, as this can disrupt validity.49,50 Face validity, an informal review of the survey to assess clarity and appropriateness, was established using an open-ended qualitative feedback question. 51 More than 80% of the feedback was categorized as positive. Participants felt that the survey was easy to complete. The constructive feedback was primarily about wanting different options for the demographic question responses. Participants identified a spelling error and a response error. The issues revealed by the open-ended question were addressed.
Implications
The present study advances lifestyle medicine and health behavior research by presenting a simple yet targeted approach to assess lifestyle medicine health behavior change using a psychometrically evaluated scale. 8 Leveraging validated assessment tools such as the LMHB scale can support evaluation efforts in lifestyle medicine research and practice. A validated assessment tool will enhance the rigor of research studies by providing one comprehensive instrument researchers can use to systematically evaluate healthy lifestyle behaviors. Moreover, the LMHB scale is advantageous because it is short and easy to complete, making it more likely to be used in clinical practice and to elicit valid responses. 14 The scale will be useful in practice, allowing practitioners to systematically look at each pillar individually to help patients and practitioners monitor and track progress with adopting and sustaining healthy lifestyle behaviors.
By explicitly using the six pillars as a framework for the assessment tool, the LMHB scale is in alignment with the field of lifestyle medicine. This is advantageous to the field, as current questionnaires often used in lifestyle medicine are single pillar focused such as a diet screener or a physical activity assessment. There are some tools that strive to evaluate all six pillars, such as the Lifestyle Assessment Long and Short forms, 24 the PAVING the Path to Wellness questionnaire, and the Lifestyle Medicine Assessment Tool. 7 However, they do not use the six-pillar framework. The Lifestyle Assessment goes beyond the six pillars by addressing weight management and mental health specifically. The PAVING the Path to Wellness questionnaire includes six additional dimensions beyond the six pillars and does not explicitly cover substance use. While these are useful tools that help lifestyle medicine practitioners better understand their patients, the additional dimensions add length to the questionnaire and take the focus away from the six pillars. The Lifestyle Assessment Tool is an appropriate length for use in practice, but it does not comprehensively assess the six pillars. The Lifestyle Assessment Tool has only one stress item and only 2 sleep items, and they are addressed together under the title of recovery. The stress and sleep pillars are essential for lifestyle medicine practitioners to thoroughly assess and address individually, as they are independent and critical to well-being. Moreover, there is some evidence that at least 3 items are needed for a stable construct. 15 It is critical to have a survey tool that thoroughly addresses each of the six pillars and yet is short enough to be completed easily in practice, which is a strength of the LMHB scale.
Beyond the use of the six-pillar framework, the LMHB scale fills a need in the field of lifestyle medicine research and evaluation because it underwent a mixed methods psychometric evaluation. The LMHB scale is unique from existing lifestyle medicine assessment tools in that it has undergone a psychometric evaluation including construct, face, content validity and reliability, as opposed to just content and face validity. 7 The LMHB scale not only fills a gap in the literature but can also improve strength-of-evidence in lifestyle medicine interventions. 52 This scale can be used in lifestyle medicine practice, providing a brief assessment to enhance the implementation of lifestyle medicine interventions in real-world settings. 53 Moving forward, the LMHB scale will be used to assess the effectiveness of lifestyle medicine programs such as the PAVING the Path to Wellness program54-56 in eliciting health behavior changes across the six pillars. With validated assessment tools in place that assess all six pillars in a systematic and meaningful way, clinicians will be able to track behaviors known to impact physical health and mental health. Utilizing a short survey can also support patient education and goal setting to aid in adopting and sustaining healthy lifestyle behaviors.
Limitations
Psychometric evaluation is an iterative process. While the LMHB scale demonstrated acceptable validity and reliability, it is important to continue investigating this scale. A limitation of this work is that the social connectedness items were all negatively worded and seemed to assess loneliness more than social connection. While this aligns with other highly utilized measures of social connectedness such as the UCLA Loneliness Scale,17,57 it does not take a strengths-based approach to social connection. It would be valuable to consider the impact of positive social relationships and community.
Additionally, the psychometric evaluation would be stronger if it included additional quantitative assessments of validity and reliability. The classical test theory approach is limited in its ability to assess item-level properties. Utilizing an item response theory analysis in future validation research would strengthen the analysis by assessing item discrimination and difficulty. Lastly, the demographics of this sample limit the generalizability of the study. A large and more diverse sample is necessary to establish generalizability. It is important that the construct validity of the scale is tested with a sample with more gender, racial, and ethnic diversity to support its use with underrepresented communities. Those interested in using the LMHB scale with their patient population should consider assessing validity for their specific community of interest.
Conclusion
This mixed methods psychometric evaluation demonstrated that the Lifestyle Medicine Health Behavior scale is reliable and has adequate face, content, and construct validity. It is a comprehensive, participant-friendly tool for assessing health behavior across all six pillars of lifestyle medicine with equal emphasis and evaluation of each pillar. Employing valid and reliable tools that individually and comprehensively assess all six pillars will enable lifestyle medicine programs to evaluate their interventions pre and post. In turn, this can help lifestyle medicine programs to scale more effectively.
Footnotes
Acknowledgments
We want to thank the following researchers and practitioners for their instrumental support with the development and review of the LMHB scale. This work was only possible with their methodological and content area expertise. Nicole Tuitt, PhD, Ashley Brooks-Russel, PhD, Courtney Donovan, PhD, Aleksandra Pikula, MD, Sarah Ibrahim, PhD, April Hirschberg, MD, Mahima Gulati, MD.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.