
Abstract
Violence is a public health problem that affects people of all ages. In 2007, violence was one of the top 10 leading causes of death in the United States for people from birth to age 64 years. Violence takes many forms, such as child maltreatment, intimate partner violence, sexual violence, self-directed violence, and youth violence. Violence may be best understood and prevented through a public health approach. A focus is placed on preventing violence before it occurs (primary prevention), employing a scientific approach to understand the problem and what action can be taken to prevent it, taking a population perspective that places an emphasis on broad-based changes in communities and society that benefit the largest number of people, and working across sectors (eg, health, justice, education) and integrating knowledge from multiple disciplines (eg, epidemiology, psychology, sociology, medicine). In this article, the authors review the incidence and burden of different forms of violence and the factors that place people at risk for, or protect people from, experiencing violence either as a victim or as a perpetrator. The authors also review strategies based on the best available evidence that may be implemented to prevent violence from occurring, highlighting violence prevention tools for health practitioners. By understanding the burden of violence, the factors that place people at risk for and protect people from experiencing violence, and strategies that can prevent and interrupt violence, health practitioners can play a more active role in enhancing the health and safety of their patients.
The Burden and Consequences of Violence
Violence is a public health problem that affects people of all ages. In 2007, violence was one of the top 10 leading causes of death in the United States for people from birth to age 64 years, accounting for more than 1.3 million years of potential life lost before age 65 years (see Figure 1). Violence occurs interpersonally, and can be directed at oneself: an estimated 18 361 people died by homicide (a rate of 6.09 per 100 000) and 34 598 died as a result of suicide (a rate of 11.27 per 100 000) in 2007. That same year, 1.54 million assault-related injury cases (a rate of 519.2 per 100 000) and 395 320 self-harm injury cases (a rate of 132.7 per 100 000) were treated in emergency departments. 1 In addition to injury and death, violence results in other physical and mental health consequences, including health risk behaviors and chronic conditions. 2 The economic burden of violence is significant. The cost of medical care and productivity losses due to interpersonal and self-directed violence in 1 year (2000) was estimated to be more than $70 billion. 3 The impact of violence can also be seen at the community level, through its association with concentrated disadvantage, eroded economic opportunities and property values, and disrupted social processes, such as social cohesion among neighbors and willingness to intervene for the benefit of the community.4,5
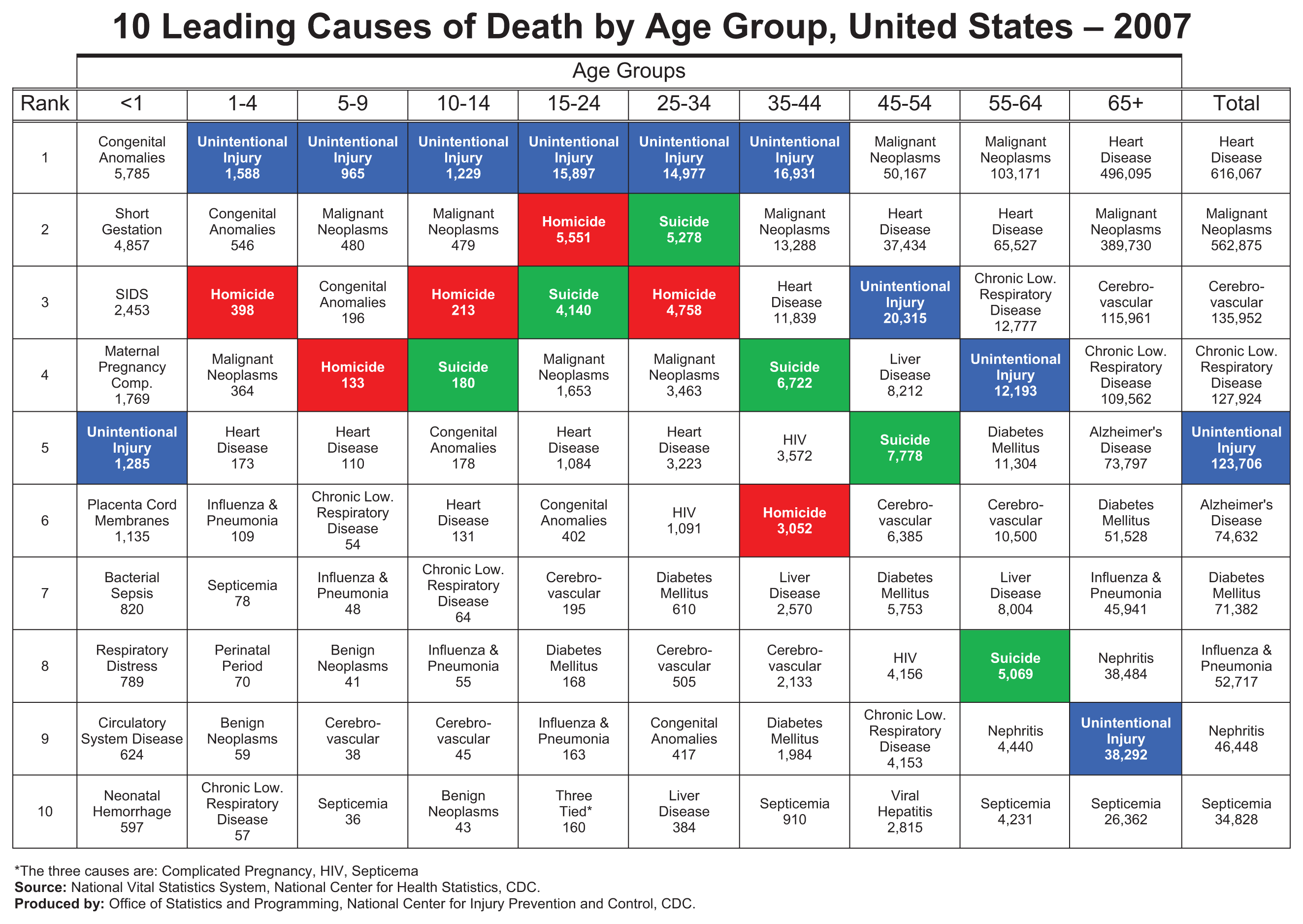
Ten leading causes of death, United States, 2007.
Violence is one of the top 10 leading causes of death in the United States for people from birth to age 64.
Violence is defined by the World Health Organization as “the intentional use of physical force or power, threatened or actual, against oneself, another person, or against a group or community, that either results in or has a high likelihood of resulting in injury, death, psychological harm, maldevelopment, or deprivation.” 6 Violence takes many forms and includes, but is not limited to, child maltreatment, intimate partner violence, sexual violence, self-directed violence, and youth violence. As described in more detail later, different forms of violence affect segments of the population differentially: for example, homicide disproportionally affects African American youth, whereas suicide disproportionally affects older white men. Different forms of violence are related. For instance, suffering abuse in childhood is associated with perpetration of violence in adolescence and early adulthood. 7
Understanding and Preventing Violence
Violence may be best understood and prevented through a public health approach. A focus is placed on preventing violence before it occurs (primary prevention), employing a scientific approach to understand the problem and what action can be taken to prevent it, taking a population perspective that places an emphasis on broad-based changes in communities and society that benefit the largest number of people, and working across sectors (eg, health, justice, education) and integrating knowledge from multiple disciplines (eg, epidemiology, psychology, sociology, medicine). The public health approach is a 4-step process: (a) measuring incidence and burden over time through public health surveillance; (b) identifying factors that place people at risk for, or protect people from, experiencing violence either as a victim or as a perpetrator (ie, risk and protective factors); (c) developing and testing strategies through rigorous evaluation that modify risk and protective factors to prevent violence from occurring; and (d) facilitating the dissemination, adoption, and adaptation of effective strategies in communities to affect change. 8
Public health recognizes that violence is a multifaceted problem that presents many leverage points for prevention. The social–ecological model provides a framework for public health to understand the factors that contribute to violence and where prevention strategies should be focused across multiple levels, including the individual, relationship, community, and societal levels. 2 As reviewed in detail below, individual characteristics and experiences, such as antisocial beliefs and attitudes, social cognitive deficits, and engaging in problem behavior early in life, can increase risk for committing violence later in life. Program strategies that intervene with these factors may prevent violence from occurring. Similarly, relationship characteristics, such as quality of parent–child interaction, family conflict, and peer associations, also influence the likelihood of engagement in violence and can be the focus of prevention efforts. Equally important are characteristics of the community and society at large, such as concentrated neighborhood disadvantage, social disorganization, cultural norms, and social and economic policies. Strategies that address factors across multiple levels of the social ecology simultaneously have the greatest potential for improving the health of large populations.
Forms and Consequences of Violence
Child Maltreatment
Child maltreatment includes any act or series of acts of commission or omission by a parent or caregiver or another person in a custodial role (eg, clergy, coach, teacher) that results in harm, potential for harm, or threat of harm to a child. Acts of commission include physical abuse, sexual abuse, and psychological abuse, and acts of omission, or neglect, include failure to provide basic necessities for a child (including physical, emotional, medical/dental, or education neglect) and failure to supervise. 9 In 2008, an estimated 772 000 children were victims of maltreatment as determined by child protective services (at a rate of 10.3 per 1000), and 1740 children died from maltreatment. During this year, the greatest percentage of children experienced neglect (71.1%), followed by physical abuse (16.1%), sexual abuse (9.1%), psychological abuse (7.3%), medical neglect (2.2%), and other (9%; eg, abandonment, threats, congenital drug addiction). Younger children (eg, under the age of 4 years) were at greatest risk for maltreatment. 10 These numbers likely underestimate the problem given that abuse and neglect does not always come to the attention of authorities. A recent nationally representative survey on children’s exposure to violence from birth to age 17 years found that 1 in 10 children experienced physical or emotional abuse or neglect and 1 in 16 experienced sexual victimization in the 12 months prior to the survey. 11
Child maltreatment can have serious immediate health consequences, including injury and death. For example, traumatic brain injury (otherwise known as “abusive head trauma”) can result from parents shaking their young children as a form of discipline or to quiet them from crying; shaken baby syndrome is one form of abusive head trauma. Death from abusive head trauma is highest for infants (<1 year of age). 12 Child maltreatment also results in long-term mental and physical health consequences, including childhood behavior problems, posttraumatic stress disorder, depression, suicidal behavior, alcohol and drug problems, criminal behavior, teenage pregnancy, promiscuity, and obesity.13,14 The effects of child maltreatment on health may be explained by toxic stress that increases stress hormones and, in turn, affects immune response and brain development (for a detailed examination of the effects of child maltreatment on health, see Leeb, Lewis, and Zolotor, this issue). 14
Intimate Partner Violence
Intimate partner violence (IPV) includes physical violence (eg, pushing, hitting, kicking), sexual violence (eg, abusive sexual contact, rape), threats of physical or sexual violence, and psychological/emotional abuse (eg, humiliation, controlling behavior, isolation) by current or former spouses or nonmarital partners (eg, dating partners, boyfriends/girlfriends). 15 In the last nationally representative survey of IPV victimization conducted from 1995 to 1996 (the National Violence Against Women Survey [NVAWS]), 22.1% of women and 7.4% of men reported physical assault by an intimate partner in their lifetime. Annually, an estimated 1309061 women and 834732 men are physically victimized by an intimate partner. In comparison, 7.7% of women and 0.3% of men reported rape by an intimate partner in their lifetime. Annually, an estimated 201 394 women are raped by an intimate partner (numbers are too low for men to determine a comparable national estimate). 16 IPV resulted in 2340 deaths in 2007. Of these deaths, 70% were females and 30% were males. 17
Intimate partner violence during the adolescent years, termed teen dating violence, has been studied less than partner violence in adulthood. Findings of the Centers for Disease Control and Prevention’s (CDC’s) nationally representative Youth Risk Behavior Surveillance System (YRBSS) revealed that in 2009, nearly 10% of students had been hit, slapped, or physically hurt on purpose by their boyfriend or girlfriend, with 10.3% of males and 9.3% of females reporting victimization. 18 Researchers have yet to determine how and why the patterns of dating violence and related consequences among adolescents might differ from those among adults; yet, it remains an important public health concern that warrants further investigation.
Physical and sexual IPV can result in injury, including scratches, bruises, lacerations, broken bones, head injury, muscle injury, and internal injuries, with more female victims reporting injury than male victims. 16 Those experiencing physical and sexual IPV are at greater risk for engagement in risky health behaviors such as smoking, binge drinking, and behaviors associated with HIV risk (eg, intravenous drug use, receiving money or drugs for sex, anal sex without a condom). 19 Physical and sexual IPV victimization is also associated with chronic physical and mental health conditions, including stroke, joint disease, asthma, high cholesterol, heart attack, and heart disease, as well as gastrointestinal, gynecological, and depression symptoms (for a detailed examination of the effects of IPV on health, see Lynberg-Black, this issue).19-22
Sexual Violence
Sexual violence includes completed or attempted sex acts (eg, contact between the penis and the vulva/anus involving penetration; penetration by a hand or object), abusive sexual contact (eg, intentional touching of genitalia, anus, groin, breast, inner thigh, or buttocks), and noncontact sexual abuse (eg, voyeurism, unwanted exposure to pornography, sexual harassment) without the victim’s consent or involving a victim who is unable to consent or refuse. 22 Sexual violence can be perpetrated by current or former intimate partners or spouses, persons in positions of power or trust, friends, acquaintances, other individuals known to victims, and strangers. The NVAWS estimated that 1 in every 6 women and 1 in every 33 men has been raped at some time in their lifetime. 23 A more recent nationally representative survey estimated that 10.6% of women and 2.1% of men have experienced forced sex at least once in their lifetime. 24 A majority of sexual violence victimization occurs before the age of 18 years, with boys experiencing victimization at earlier ages (ie, less than the age of 12 years) than girls, on average.23,24 Surveys among high school youth reveal that 7.4% of youth (10.5% of girls and 4.5% of boys) report having been physically forced to have sexual intercourse when they did not want to. 18 Victims most often know their perpetrators, as intimate partners, family members, or acquaintances.23,24
Immediate consequences of sexual violence include physical injuries; the NVAWS revealed that 31.5% of women and 16.1% of men reported physical injury from rape. 23 Other consequences may appear over longer periods of time after victimization. Women who have experienced forced sexual intercourse have been found to be more likely to engage in risky health behaviors than nonvictimized women, including alcohol and substance use, smoking, and sexual activity with multiple partners, and be at increased risk for other forms of violence, including physical IPV and suicidal thoughts.25,26 Victimized women are at greater risk for somatic disorders, such as fibromyalgia, gastrointestinal disorders, and reproductive and sexual symptoms (eg, chronic pelvic pain, painful menstruation, irregular periods, pain during intercourse, and lack of sexual pleasure).27,28 Sexual violence is also associated with poor mental health outcomes, including anxiety, depression, and posttraumatic stress disorder, as well as suicidal behavior and other negative life consequences (eg, loss of time from work; for a detailed examination of the effects of sexual violence on health, see Basile and Smith, this issue).23,29-31
Self-directed Violence
This form of violence includes behavior that is self-directed and deliberately results in the injury or potential for injury to oneself. Self-directed violence can be suicidal with an intent to die or nonsuicidal (eg, self-mutilation, with no intention to die). The outcome can be fatal (suicide) or nonfatal. Nonfatal suicidal behavior includes attempts, interruptions, and preparatory acts (eg, assembling a method, writing a note, giving things away). Suicidal ideation—thinking about, considering, or planning suicide—is associated with self-directed violent behavior. 32 In 2007, 34 598 people took their own lives (a rate of 11.27 per 100 000), ranking suicide as the 11th leading cause of death. 1 Deaths only tell part of the story: For those aged 65 years and older, 1 suicide is estimated for every 2 to 3 attempts; for those aged 25 years and younger, 1 suicide is estimated for every 100 to 200 attempts. 33
Suicide rates are higher among men than among women, due in part to a higher case fatality rate for men than for women. 1 That is, although more women than men attempt suicide, men are more likely to die from suicide attempts than women, perhaps because men select more lethal means than do women. A greater percentage of men than women choose firearms as a mechanism for suicide (poisoning is more likely among women than men), and the fatality rate for firearm injuries is high. Suicide rates are highest between the ages of 45 and 54 years (17.7 per 100 000), although when rates are examined by sex, it is clear that the highest rates of suicide among women are in this age group, whereas the highest rates of suicide among men occur in those aged 75 years and older (particularly white men in this age group; for a review of how rates of suicidal behavior differ by demographic characteristics, see Crosby, Buckner, and Taylor, this issue). Rates of youth suicide (ages 15-24 years) are also unacceptably high (a rate of 9.7 per 100 000). 1 The 2009 YRBSS revealed that 13.8% of students in grades 9 to 12 seriously considered suicide, and 6.3% reported making at least 1 suicide attempt in the previous 12 months. 18
Other than death, immediate consequences of suicide attempts include injuries. In 2007, 395 320 cases of nonfatal self-harm injuries were seen in US hospital emergency departments (a rate of 132.7 per 100 000). 1 Injury statistics from hospitals still greatly underestimate the problem, as it is estimated that only 25% of those attempting suicide are seen in hospitals. 33 The types of injuries seen in emergency departments are associated with the mechanisms most commonly selected and result in injury more often than death, including poisoning from drug overdose, fractures due to falls, and lacerations from cuts. 1 Suicidal ideation and suicide attempts also have long-term consequences. The greatest predictor of completed suicide is a previous history of suicide attempts. It is estimated that between 10% and 15% of those who attempt suicide eventually die of suicide later in life, with risk accumulating for decades after the initial attempt. 34 Long-term follow-up of youth who exhibited suicidal ideation in childhood and adolescence has shown an increased risk for psychological disorders in adulthood, although the increased risk may be partially explained by a progression of internalizing and externalizing symptoms already present in childhood.35,36 These data highlight the persistence of suicidal behavior over the lifetime, indicating the importance of early prevention and intervention.
Youth Violence
Youth violence is the intentional use of physical force or power by a young person aged 10 to 24 years against another person, group, or community, with the youth’s behavior likely to cause physical or psychological harm. 37 Youth violence includes various behaviors that range in severity, such as murder, aggravated assault, robbery, rape, gang violence, bullying, verbal aggression (eg, name calling), and relational/psychological aggression (eg, spreading rumors, social exclusion). Violence can occur in-person as well as through the use of technology, called electronic aggression (eg, harassment, threats, or teasing that occurs through e-mail, a chat room, instant messaging, a Web site, text messaging, or videos or pictures posted on Web sites or sent through cell phones). 38
Youth violence is a public health problem as well as a criminal justice problem. In 2007, 5764 young people age 10 to 24 years were murdered—an average of 16 each day—making homicide the second leading cause of death for people in this age group. Of the homicide victims, 86.3% were male and 13.7% were female, and 83.6% were killed with a firearm. Minority youth are disproportionately affected by violence, for example, homicide rates in 2007 were 7 times greater for African American youth age 10 to 24 years compared with white youth in this same age group. 1 In 2007, youth aged 18 years and younger were involved in 16% of all violent crime arrests. That same year, 1350 youth in this age group were arrested for murder, 57 650 for aggravated assault, 34 490 for robbery, and 3580 for forcible rape. 39 Self-report surveys also illustrate the prevalence of youth violence. The 2009 YRBSS revealed that 31.5% of high school students reported being in a physical fight during the past 12 months and 17.5% reported carrying a weapon (gun, knife, or club) on 1 or more days in the 30 days preceding the survey. 18
Youth violence can result in immediate physical injury. More than 668 000 cases of assault-related injuries among young people aged 10 to 24 years were treated in US emergency departments in 2007. 1 Victimization by peers has been found to be associated with consequences other than physical injury, such as mental health problems (eg, internalizing/depression and trauma symptoms) and psychosomatic complaints (eg, headache, stomachache, and sleeping problems).40-42 Long-term health effects are also evident: Violent victimization in adolescence is associated with an increased risk for mental health problems and substance use in adulthood. 43 Youth who commit violence are also at increased risk for health problems, including alcohol and drug use, high-risk sexual behavior, and psychological disorders.44,45
Predictors of Violence
Assessing and monitoring the magnitude and impact of violence is only the first step in addressing violence as a public health problem. Investigating why violence occurs and which factors increase or buffer against risk is another important step. Public health research draws on many theories of behavior, social processes, and social organization to understand why people behave violently toward others or why some communities experience more violence than others. Violence is seldom the result of a personal lifestyle choice. More commonly, individuals are greatly influenced by the circumstances and context within which they live.
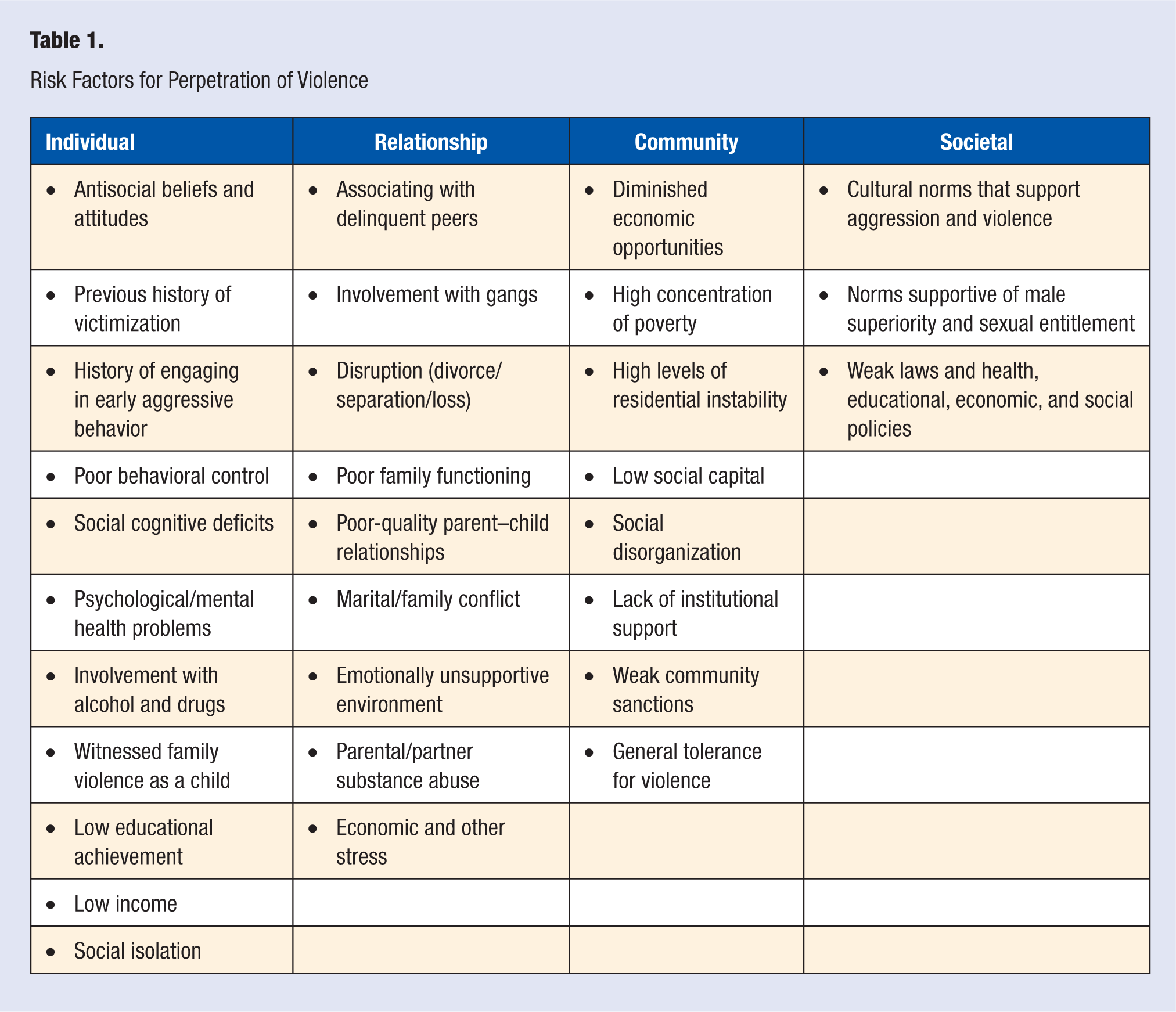
The factors that influence risk for perpetrating violence are present at the individual, relationship, community, and societal levels. These factors are highlighted in Table 1. Psychological and behavioral characteristics such as antisocial beliefs and attitudes, social cognitive deficits (eg, difficulty interpreting social situations), poor emotional and behavioral control (eg, anger/hostility, impulsiveness), previous victimization, a history of engaging in aggressive behavior, and involvement with drugs and alcohol have been linked to multiple types of violence.46-53 For example, youths who endorse highly aggressive attitudes, who exhibit a high level of distrust and estrangement from others, and who lack empathy and guilt are much more likely to be involved in violence than youths without these personality characteristics.54-56 Similarly, research shows that sexually violent men are more likely to have coercive sexual fantasies, to have a preference for impersonal sexual relationships, and are generally more hostile toward women than men who are not sexually violent. 57 Empathy deficits are also common among perpetrators of sexual violence. 58
Risk Factors for Perpetration of Violence
Many of the behavioral factors associated with committing violence are evident before 10 years of age, with signs of early physical aggression being one of the strongest predictors for later involvement in violent behavior. 59 Longitudinal evidence suggests that boys with high levels of physical aggression in childhood, especially in combination with hyperactivity and oppositional behavior, are among the most prone to follow a path of chronic violence into adulthood.7,51,55,59,60 Boys with these characteristics often have trouble in social situations. They make social decisions quickly, perceive the actions and intentions of others as hostile, and have difficulty coming up with nonaggressive solutions to problems.61,62 Not only are boys with these characteristics more likely to engage in violence against other youths, but they are also at higher risk of perpetrating violence against intimate partners and to have more criminal and noncriminal convictions as adults. 46 Early onset of sexual aggression is also one of the strongest predictors of subsequent sexual violence perpetration. 63
Relationships, such as those with peers, intimate partners, and family, also influence risk for violence. Previous research shows that associating with antisocial peers increases the risk for involvement in delinquency and violence manifold.51,64 It also shows that when young people engage in these types of activities with others, both the frequency and the severity of their actions increase.46,64 Gangs are probably the best example of how exposure to delinquent peers can lead to more frequent and severe offending, especially serious violent offending (eg, robbery, rape, and homicide).65,66 For example, in the Rochester Youth Development Study (a longitudinal study of boys followed since the age of 13 years), gang members made up 30% of the sample but were responsible for 86% of the serious acts of delinquency and 68% of the violent acts. 67
Persons at risk for committing violence also tend to come from weak family environments. A weak family environment is one that can include constellations of poor family management and parenting practices, deficiencies in communication and problem solving, low emotional bonding and support, disruption (eg, from a divorce or separation), and family conflict and violence (whether witnessing or experiencing). High family conflict and low family cohesion, for instance, are 2 of the strongest predictors for child physical maltreatment by parents, along with parental perception of the child as a problem. 68 Disruption from a divorce or separation, on the other hand, can disrupt family functioning and affect both parental and child behavior. For example, parental neglect and disruptions in attachment have been linked to both physical and sexual aggression by youth.69,70 Low emotional bonding and support within the family environment as well as economic and other stressors have been linked to IPV and suicidal behavior as well.33,49
Alcohol and drug use are associated with all types of violence both as an individual factor influencing a person’s propensity to commit violence as well as a factor influencing relationships and family environments. 50 However, it is not always clear whether alcohol is a cause or consequence of violence. In the case of youth violence, excessive alcohol consumption might increase impulsivity and make some drinkers more likely to resort to violence in a confrontation or argument. 71 More typically, involvement with alcohol and other substances at an early age is a gateway for later problem behavior, including more serious violent offending during late adolescence and adulthood. 51 Parental alcohol or drug use can also erode parenting skills and complicate parental efforts to discipline and exercise effective monitoring or supervision of children and adolescents—factors that, in turn, increase a youth’s risk of involvement in delinquent and violent behavior.46,51 Parental alcohol abuse is also associated with perpetrating and experiencing child maltreatment as well as other adverse experiences in childhood.68,72
In the case of IPV, studies consistently find a strong association with heavy drinking. 50 Excessive alcohol consumption by one or both partners might worsen financial or child care problems and increase tension and conflict in the relationship. It also has the potential to increase the severity of a violent confrontation between partners. 73 Alcohol can also be a form of self-medication to cope with problems and previous or current experiences of abuse. 20 With suicide, previous research suggests that alcohol intoxication may play a more significant role as a proximal rather than a distal factor in suicide. 74 However, in cases where there is alcohol dependency, the alcohol abuse might be a form of self-medication to alleviate depression or to cope with other stresses in a person’s life. 33 Alcohol and drug abuse are second only to depression and other mood disorders as the most frequent risk factors for suicidal behavior along with a previous suicide attempt.33,75
People are also greatly influenced by the community and societal context within which they live. Interpersonal and self-directed violence is higher in communities where there are limited economic opportunities, where there are high concentrations of poor and unemployed people, where people move frequently, and where there are limited public, mental health, and social services available to residents and fewer civic and voluntary associations.76-78 Communities with these characteristics also lack cohesion or collective efficacy. Factors such as high levels of residential instability along with fewer institutional resources make it difficult for individuals to establish common values and norms and to develop informal ties and support networks.5,78 People living in such neighborhoods often experience social isolation and exhibit lower levels of trust and attachment to the community. 5 High levels of social disorganization also limit the ability and willingness of community residents to intervene in cases of IPV (with the exception of when the threat of that violence has the potential to be lethal) or to supervise and control children and adolescents.78,79
The net effect of these social processes and conditions is a climate that makes violence more likely to occur, especially when coupled with societal and cultural norms that encourage violence; see it as a matter of individual or family privacy; and attach stigma to help seeking. Diminished economic opportunities, neighborhood social disorganization, social and cultural norms supportive of violence, and inadequate access to health and social services are associated with many forms of violence.5,76,79 Although less is known about the factors that serve as protective buffers in the face of risk, previous research suggests that connectedness is a protective factor that can offset many of these negative influences and confer psychological and social benefits that extend well beyond individuals. It is also the one factor that seems to be protective across multiple forms of violence, including child maltreatment, youth violence, IPV, and suicidal behavior.79-82
A Focus on Primary Prevention
The health risks of violence and the burden placed on health systems and society illustrates the need to stop violence before it starts through primary prevention efforts. By intervening in the factors and processes that place people at risk for violence and supporting those that protect people from experiencing violence, we can reduce violence and its consequences. Efforts that focus on the characteristics of individuals, families, communities, and society that influence multiple forms of violence have the greatest potential for having an impact on the health of populations, particularly when implemented across multiple levels of the social ecology simultaneously. It is critical to change beliefs and attitudes that support violence, build social competencies and skills that support positive interpersonal interactions, prevent and reduce the consequences of early victimization and perpetration, and prevent and treat mental health and substance abuse problems. We must also build safe, stable, and nurturing relationships between children and their caregivers; promote respectful relationships between intimate partners; and improve social connectedness between people and between people and community organizations. We need to invest in social institutions that can affect the social determinants of poor health within communities, such as poverty, concentrated disadvantage, and limited economic opportunities. Finally, it is important to change societal norms that support aggression and male superiority over women and reduce the social stigma surrounding mental health treatment and help-seeking behavior. Prevention research has been focused primarily on evaluating programs aimed at the individual and relationship (peer, family) levels; more attention is needed to developing the evidence base of community- and societal-level strategies.
Prevention research has shown that experiences occurring early in life set individuals on a trajectory for engaging in specific behaviors over the lifetime. For example, emotional, cognitive, and behavioral problems in early and middle childhood are predictive of peer, intimate partner, and sexual violence in adolescence and adulthood.83,84 Many of the risks that make these problems more likely to occur such as poor-quality parent–child relationships, conflict or violence in the home, and poor family functioning are also evident in early childhood. Thus, initiating prevention efforts early is the key to success.
A multidisciplinary approach to preventing violence is required, with preventive interventions located in various sectors, including health, criminal justice, education, and social services. Next, we review examples of effective approaches for preventing each form of violence across multiple sectors and highlight the role of health practitioners, such as nurses and primary care physicians, in preventing violence (Table 2).
Violence Prevention Strategies Informed by the Best Available Research Evidence
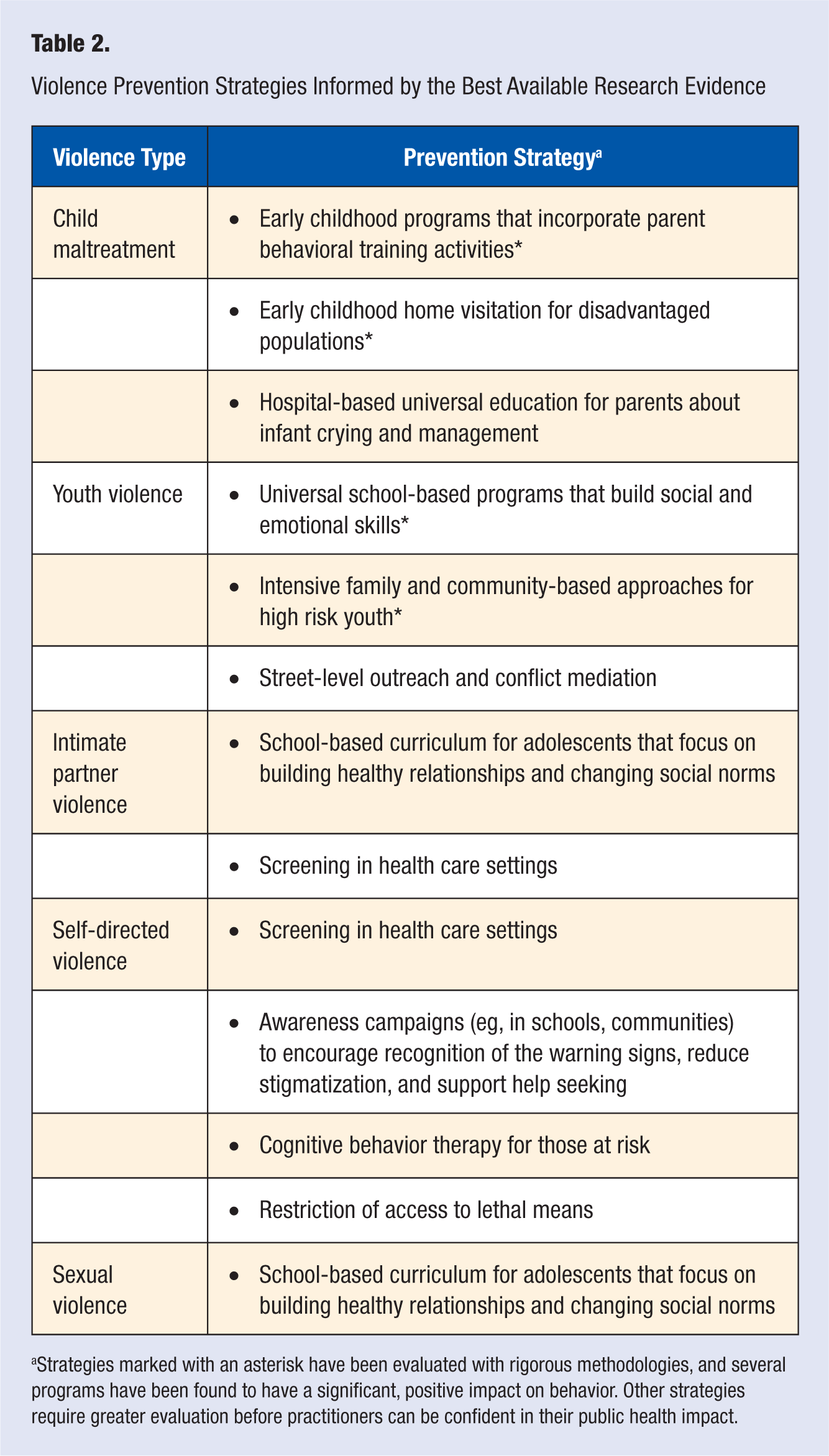
Strategies marked with an asterisk have been evaluated with rigorous methodologies, and several programs have been found to have a significant, positive impact on behavior. Other strategies require greater evaluation before practitioners can be confident in their public health impact.
Child Maltreatment
School-based, early childhood programs that provide a stable, enriched learning environment for children and community-based parental behavioral training activities that build positive relationships between parents and their children and enhance skill in managing child behavior problems are most promising for the prevention of child maltreatment.85,86 For example, the Chicago Child–Parent Center program located in impoverished neighborhoods provides preschool education alongside family support services directed toward enhancing parental involvement in their children’s education. Services focus on strengthening parenting skills, vocational skills, and social supports. Lower rates of official child maltreatment reports (ie, child protective service and court records) have been found for parents participating in the child–parent center program, compared with parents of children in alternative early childhood programs. 85
Effective behavioral parent training programs develop parents’ skills in communicating and positively interacting with their children, responding consistently to their children’s behavior, and using time out as a disciplinary strategy. 86 Triple P (Positive Parenting Program) is an example of a multilevel system of parent training interventions that range in intensity and population reach to meet differing family needs. Interventions range from a universal program for all families that uses media strategies to disseminate information on positive parenting (level 1) to intensive parenting sessions for families with severe dysfunction and children with behavioral difficulties that include active skills training, home visits, and clinic observations, combined with a focus on partner communication, coping skills, and parent–child issues (level 5). In a community-level randomized trial, Triple P has been shown to reduce rates of substantiated abuse, child maltreatment–related injuries treated in hospital emergency departments, and out-of-home placements. 87
One evidence-based strategy for preventing child maltreatment that is located within health services is early childhood home visitation for disadvantaged populations. 88 Trained personnel, including nurses, visit parents and children at home during the child’s first 2 years of life and provide information, support, and training about child health, development, and early care. For example, the Nurse Family Partnership aims to improve prenatal health and pregnancy outcomes, care provided to infants and toddlers, and mothers’ educational achievement and workforce participation. This program has been shown to significantly decrease reports of child abuse and neglect and emergency department visits for injuries, particularly for children of poor, unmarried mothers. 89
A promising strategy for preventing abusive head trauma in health systems is being implemented and evaluated throughout North Carolina through a collaboration between the University of North Carolina, the CDC, and other partners (eg, North Carolina hospitals and county health departments, the National Center on Shaken Baby Syndrome). The Period of PURPLE Crying includes a video and accompanying materials (eg, booklets, certificates) that provide new parents information about infant crying (that it peaks at 2 months of age, and it can be unexpected, resist soothing, last 1 to 2 hours, cluster in the evenings, and make the infant look as if he or she is in pain). The program is being administered to every parent of a newborn in hospital nurseries, in the community at prenatal visits or well-child care visits, and through a media campaign. It is anticipated that the program will increase awareness among parents and other caregivers of the characteristics of early crying, the potential for caregiver frustration, and the dangers of shaking a baby and reduce the occurrence and risk factors for abusive head trauma and traumatic brain injury. 90
Youth Violence
Many of the evidence-based prevention strategies for youth violence prevention are located in the education, criminal justice, and social service sectors. Using rigorous scientific standards, the Blueprints for Violence Prevention initiative at the University of Colorado has identified 11 Model programs and 18 Promising programs with significant positive effects on youth violence or risk factors for youth violence. 91 School-based programs and multidimensional treatment foster care are among the strongest evidence-based strategies.92,93 Universal school-based programs that are delivered to all students in school or a grade and build youth’s social competencies and skills have been found to reduce aggression, conduct problems, and other externalizing behaviors. For example, the Life Skills Training program for middle school students teaches youth about violence and the media, anger management, and conflict resolution and results in significant reductions in the incidence of fighting and delinquency. 94
Therapeutic foster care programs that are implemented with high-risk, chronic youth offenders have been found to be effective in preventing repeated violence. Youth who cannot live at home because of severe emotional and behavioral problems are placed in specially trained foster families for a time-limited basis (eg, 6-12 months). For example, Multidimensional Treatment Foster Care (MTFC) is an approach that provides youth with close supervision and supports that reinforce prosocial behavior and bonding with peers, enhance work habits and academic skills, improve parenting skills and decrease family conflict, and set clear expectations and limits for behavior. 95 In this model, youth are placed with trained foster parents who work closely with program staff, other foster parents, and a treatment team consisting of behavior support specialists, youth specialists, family therapists, consulting psychiatrists, daily report callers, and case managers to implement individualized behavior management plans in the home and provide support services (eg, individual youth or family therapy). The strategy and its adaptation have been found to be effective in reducing conduct problems, violence, and delinquency.
For the prevention of youth and community violence, particularly shootings, a promising public health strategy is CeaseFire Chicago. 96 The program focuses on street-level outreach, conflict mediation, and the changing of community norms to reduce violence. CeaseFire relies on highly trained outreach workers and “violence interrupters,” faith leaders, and other community leaders to intervene in conflicts, or potential conflicts, and promote alternatives to violence. One component of the program includes hospital responders that work with emergency room staff, hospital spiritual care, and social workers when gunshot and other violence-related trauma cases present in the emergency room to intervene in conflicts and prevent retaliatory violence. CeaseFire also involves cooperation with police, public education campaigns to instill the message that violence is not acceptable, and the strengthening of communities to build capacity to exercise informal social control and mobilize forces to reduce violence. Evaluation results have been promising in Chicago, signaling a reduction of homicides in most Chicago CeaseFire communities.
Intimate Partner Violence
Compared with the other types of violence, much less evaluation research has been conducted to determine the effectiveness of primary prevention strategies for IPV, that is, those strategies that prevent violence before it begins. Most of the programmatic and evaluation efforts have focused on strategies that assist victims after violence has occurred. One exception is the evaluation of school-based programs for the prevention of teen dating violence. Two programs, Safe Dates and The Fourth R: Skills for Youth Relationships, include classroom curriculum for adolescents that focus on building healthy relationships, changing social norms about dating violence, decreasing gender stereotyping, and improving problem solving and conflict management skills. Both programs have illustrated reductions in perpetration of physical dating violence years after program implementation, although the significant effects of the Fourth R are limited to male students.97,98
One of the most controversial prevention approaches in health care settings for the reduction of IPV is routine (universal) screening. It is important that physicians inquire about patients’ experiences with IPV when patients present with signs and symptoms consistent with violence victimization. Assessment tools have been developed for health practitioners to use in these circumstances to aid in detection of abuse and to inform treatment decisions (see Black and Basile and Smith, this issue, for more information about assessment tools and procedures). However, in the universal screening approach, patients are asked about their experiences with IPV through a standardized procedure, regardless of presentation of symptoms, to identify whether intervention is needed. Methods of screening are varied and include physician–patient interviews, audiotape questionnaires, written questionnaires, and computer-based screening. 99 Many screening tools have been developed, yet the extent to which these tools have been evaluated for reliability and validity is limited.100,101 Professional organizations, such as the American Medical Association and the American College of Obstetricians and Gynecologists, have offered recommendations and guidelines that support routine screening of patients for IPV.102,103 However, there are many barriers to implementation of routine screening, including lack of available and effective intervention services if IPV is detected, patient nondisclosure, fear of offending patients or repercussions to patients, lack of provider education about IPV, limited time to conduct screening, and inadequate implementation of tools and procedures following provider education. 104 Furthermore, in 2004, the US Preventive Services Task Force issued a recommendation statement about routine screening for IPV, concluding that there is “no direct evidence that screening for family and intimate partner violence leads to decreased disability or premature death.”105(p382) The recommendation cited the lack of validation of screening instruments, studies that assess the impact of screening on reducing harmful outcomes, and studies that address the potential harms of screening. Since the publication of the recommendation, there has been an increased call for rigorous evaluation of routine screening. A recent randomized trial in Canada compared women who were screened and provided an information card with domestic violence resources with women who received an information card only. 106 Results illustrated no differences in IPV recurrence risk, mental health problems, and quality of life between screened and nonscreened women after rigorous statistical methodologies were employed, and there was no indication of harm associated with screening. The CDC is currently conducting a randomized trial comparing 3 groups of women: women who are screened by computer and provided information on IPV services, women who are provided information on IPV services only, and women who receive neither screening nor IPV service information. Results of the impact of screening on IPV exposure, disability, health care utilization, and mental health are expected in 2012. 107
Self-directed Violence
Routine screening has also been proposed as a prevention strategy for identification of individuals at risk for suicide. The National Strategy for Suicide Prevention, a framework for action developed by a collaborative of advocates, clinicians, researchers, and survivors, has identified primary health care providers as gatekeepers who can recognize behaviors and other factors that place individuals at risk for suicide and intervene before the early signs of risk progress further. 108 Health professionals are in a position to refer patients for specialized assessment and treatment. In 2004, the US Preventive Services Task Force found that there has been limited assessment of the reliability and validity of screening instruments and examination of the effects of preventive interventions for universal, primary care populations that do not have an already identified risk for suicide; furthermore, studies have not adequately addressed whether screening for suicide risk in primary care patients prevents morbidity and mortality. 109 The results of a randomized trial of a preventive intervention, PROSPECT (Prevention of Suicide of Primary Care Elderly: A Collaborative Trial), focusing on depression screening and case management in primary care practices published after the completion of the Task Force review are promising, however. 110 Screening and treatment for depression was a focus, given that depression is a risk factor for suicidal behavior. In the trial, patients were screened for depression, and physicians were notified of depression diagnoses. In the intervention condition, physicians were educated on guidelines for treating depression in elderly patients with use of selective serotonin reuptake inhibitors and interpersonal psychotherapy and collaborated with depression care managers who assisted in offering treatment recommendations, psychotherapy, patient monitoring, and follow-up. The intervention was compared with usual care enhanced by initial physician education on treatment guidelines. The course of depression symptoms was more favorable and suicidal ideation resolved more quickly for depressed patients who received the intervention compared with depressed patients who did not. Although the study did not estimate impacts on attempts or suicides (the study was not of sufficient size to estimate such impacts), it does highlight the potential for impact on risk factors for suicidal behavior.
Other promising approaches to the primary prevention of suicide include public education campaigns to encourage recognition of the warning signs of suicide, reduce the stigmatization of mental health problems, and support help-seeking behavior; cognitive-behavior therapy for those at risk for suicide; and the restriction of lethal means (eg, access to firearms, restrictions on prescription of barbiturates, changing of packaging of analgesics, construction of barriers at jumping sites). 111 More rigorous evaluation of these strategies is needed to understand the impact on suicide rates.
Sexual Violence
A focus on the primary prevention of sexual violence, compared with secondary and tertiary prevention, is a relatively new direction in public health. 112 This is especially true for strategies in health care practices and settings. Only 1 program implemented in the educational setting, Safe Dates (referenced previously for its affects on teen dating violence), has been shown in a rigorous evaluation to decrease sexual violence perpetration in adolescence. 98
Training programs for health practitioners have focused primarily on helping practitioners feel comfortable with approaching sexual violence topics with patients and fostering disclosure of victimization, conducting routine screening for sexual violence victimization, detecting symptoms and treating sexual violence–related injuries and trauma, and referring victims to sexual violence services. Efforts focused on the prevention of perpetration have received even less attention. Thus, there have been limited opportunities for examining the effectiveness of primary prevention approaches. New directions should include a focus on the role of health professionals in primary prevention. Efforts to be considered could entail a focus on the prevention of perpetration, such as service referrals by health care practitioners for those who present with risk factors for sexual violence perpetration (eg, substance use, physical and sexual abuse history, hostility toward women).
Conclusion
Child maltreatment, youth violence, self-directed violence, IPV, and sexual violence pose a significant threat to the public’s health. By understanding the burden of violence, the factors that place people at risk for and protect people from experiencing violence, and strategies that can prevent and interrupt violence, health practitioners can play a more active role in enhancing the health and safety of their patients. In some instances, the role of the health practitioner is to deliver preventive services directly to the patient. At other times, the practitioner’s role is to identify warning signs and refer patients to appropriate preventive services in the community. There are many tools and resources available for practitioners to learn more about violence, the health burden, and prevention strategies (see the appendix for a sample of resources). We encourage practitioners to reach out to other sectors within their local communities to learn more about available preventive services and to develop partnerships and mechanisms of referral.
Footnotes
Appendix
The conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.