
Abstract
This article summarizes the field of self-directed violence and its prevention focusing on suicidal behavior. Then it describes ways in which health care practitioners, especially preventive medicine specialists, can play a role in preventing these injuries whether they practice in clinical or community based settings. A review of the importance of suicidal behavior as a public health problem, its epidemiology, and prevention approaches are discussed. Suicidal behavior results from an interaction of risk factors but much is known about these factors and many of the injuries due to this phenomenon are preventable. Prevention of suicidal behavior requires collaboration from many sectors, including health care practitioners. Preventive medicine specialists can address this problem that affects individuals, families, and communities by taking an active part as practitioners, researchers, advocates, and through education.
Because of the toll that self-directed violence (SDV) has on all parts of society, it is an important topic for preventive medicine practitioners. The tragic consequences of SDV affect the victims who die or suffer injuries and it has far-reaching effects on families, friends, and communities. In this article, we provide a summary of the problem of SDV and then describe some actions that preventive medicine practitioners can take to address the issue. We define SDV as behavior that is self-directed and deliberately results in injury or the potential for injury to oneself. 1
“Self-directed violence presents major challenges to public health, health care organizations, and individual health care providers in the United States and throughout the rest of the world”
Self-directed violence presents major challenges to public health, health care organizations, and individual health care providers in the United States 2 and throughout the rest of the world.3,4 In this article, we will focus mainly on fatal and nonfatal suicidal behavior (including attempts, interruptions, and preparatory acts), but include some information about the broader topic of SDV which includes nonsuicidal behavior (eg, self-mutilation, with no intention to die). In the United States, suicide has ranked among the top 12 leading causes of death since 1975. In 2007, it was the 11th leading cause of death overall in the United States, responsible for 34 598 deaths 5 or approximately 1 death every 15 minutes. It was the third leading cause of death among people aged 15 to 24 years, fourth among people aged 25 to 44 years, and eighth among those aged 45 to 64 years, 6 showing that suicide is a problem throughout the life span. Although suicide is problematic for many age groups, rates for males are highest among those aged 75+ years, whereas among females the rates are highest among those aged 45 to 54 years.
In public health, we approach the problem of suicidal behavior by asking 4 questions 7 :
What is the problem? (problem description) We collect data on the problem that we can use to better describe and understand the problem and to do something about it. We ask who, what, where, and when did it happen, and to whom.
What are the causes? (risk and protective factor research) We seek to discover what puts people at risk or protects them.
What works to help prevent the problem? (development and evaluation of prevention strategies) We use the knowledge we have of the pattern of the problem to develop and test interventions that might work to prevent it.
How do you do it? (implementation and dissemination of effective strategies) We look at how we can accelerate the dissemination of research findings more quickly and effectively. We also explore how we apply the proven effective interventions broadly in the community in safe and effective ways.
We will use this framework to organize the article.
Problem Description
Mortality
In 2007 (the most recent year of complete US mortality data), 34 598 suicides were counted in the United States. * From 2006 to 2007, the age-adjusted death rate for suicide increased by 3.7%, a statistically significant increase. 5 Years of potential life lost before the age of 75 years (YPLL-75), one measure of premature mortality, is another way of defining the burden of a health problem in the population. In terms of YPLL-75, suicide was the fifth leading cause of YPLL for US residents in 2007. It accounted for 1 009 224 years of potential life lost, which represents approximately 4.9% of YPLL-75 for all causes of death and was preceded in rank by the following causes, in order: cancer, unintentional injury, heart disease, and conditions of the perinatal period. These summary data do not illustrate the variation with which suicide risk and the methods of suicide occur across age, sex, racial/ethnic groups, and geographic regions within the United States.
Age- and sex-specific suicide rates
In 2007, the highest rate of suicides occurred among adults aged 45 to 54 years, whereas children aged 10-14 years had the lowest rates. This pattern differs when suicides are examined by sex. Approximately 80% of suicide victims are males, and their rates are 3.9 times greater than those of females. For males in the United States, the highest rate of suicide is among those aged 75 years and older, and the highest number of suicides occur among middle-aged males aged 40 to 49 years. Among females, the highest rate and the highest number of suicides are among women aged 45 to 54 years.
Race/ethnicity- and age group–specific suicide rates
Despite the widespread impact of self-directed violence in the United States, the problem has frequently been misperceived as solely a problem affecting non-Hispanic European American males8,9 and the affluent. 10 Data on suicide rates are available for 5 major ethnic groups: white non-Hispanic, black non-Hispanic, Hispanic, Asian Pacific Islander (A/PI), and American Indians and Alaskan Natives (AI/AN). All references to a specific race refer to non-Hispanic members (eg, non-Hispanic black, non-Hispanic Asian Pacific Islander). Examining the 2007 suicide rates by age group along with race/ethnicity demonstrates several patterns, with the highest rates occurring among AI/AN adolescents and young adults. Rates among AI/ANs, blacks, and Hispanics were highest among adolescents and young adults, then declined or leveled off with increasing age. In contrast, rates among whites were highest among those aged 40 to 54 years. Among A/PIs, rates were highest for those aged ≥65 years. Although the overall rates for AI/ANs are similar to those of whites, the rates among adolescent and young adult AI/ANs aged 15 to 29 years were substantially higher. In each of the racial and ethnic groups, suicide rates were higher for males than for females.
Method of suicide
Firearms are the most common method used in suicides in the United States and accounted for 50.2% of all suicides in 2007. The next most commonly reported methods were suffocation (23.6%), poisoning (18.4%), falls (2.1%), and cutting (1.8%). Other, or unspecified, means accounted for 3.9% of all suicides in 2007. The methods of suicide vary by sex. Among males, firearms accounted for the majority of suicides (55.7%) in 2007, followed by suffocation (24.4%), poisoning (12.5%), and then other methods. Poisoning was the leading means of suicide used by females (40.2%), followed by firearms (29.5%), suffocation (20.6%), and then other methods. The methods of suicide also vary by race/ethnicity. In 2007, firearms were the leading method of suicide among whites (52.2%) and blacks (50.9%). Among Hispanics (40.0%), A/PIs (45.0%), and Native Americans (48.1%), suffocation was the leading method.
Geographical variation
In 2007, age-adjusted suicide rates varied substantially across states, from 22.1 per 100 000 population in Alaska to 5.8 in the District of Columbia (see Figure 1). As in previous decades, age-adjusted suicide rates in the Northeastern states were generally lower than those in other regions (8.3 per 100 000), followed by the Midwest (11.1). The states in the South (12.0) and West (12.8) had the highest rates. When state-specific age-adjusted suicide rates for the United States were ranked from highest to lowest, 10 of the top 11 were states from the western region. **
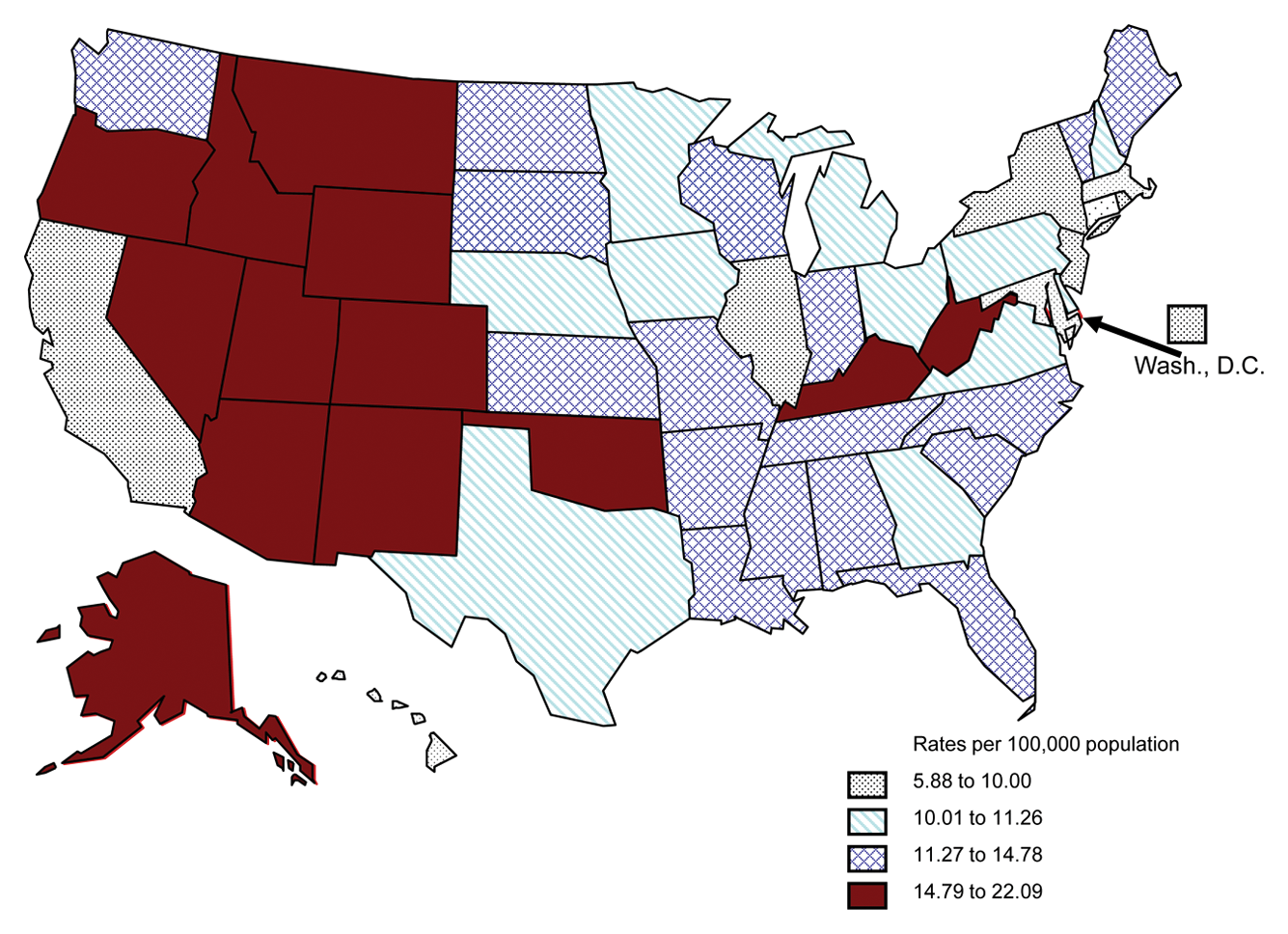
Age-Adjusted Suicide Rates Among All Persons by State: United States, 2007 (US Average 11.26).
Morbidity
The number of suicides reflects only a small portion of the impact of suicidal behavior. Many more people are hospitalized because of nonfatal suicidal behavior than are fatally injured, and an even greater number are treated in ambulatory settings or are not treated at all for injuries due to suicidal acts than those who are hospitalized. 8 Only within the past 20 years have nationally representative statistics been available for suicidal thoughts and behavior among persons in the United States.
The National Electronic Injury Surveillance System developed by the US Consumer Product Safety Commission was expanded in July 2000 to collect data on all types of nonfatal injuries treated in a nationally representative sample of US hospital emergency departments. During 2009, an estimated 374 486 persons were treated in the United States for nonfatal self-inflicted injuries (rate: 124.0 per 100 000 population). Among females, an estimated 216 867 were seen for these injuries (rate: 145.8); among males, an estimated 157 378 were seen (rate: 102.9). Overall, self-inflicted injury rates were highest among adolescents and young adults. Most (77.8%) of the self-inflicted injuries were the result of poisoning or being cut or pierced with a sharp instrument. 6
Self-report data are also useful in understanding morbidity. Research indicates that possibly 50% to more than 70% of people who engage in suicidal behavior never seek health services.12,13 As a result, prevalence figures based on health records substantially underestimate the societal burden. Since 1990, the Youth Risk Behavior Surveillance System (YRBSS), a school-based system, has measured health risk behaviors (including suicidal thoughts and behavior) among high school students in grades 9 to 12 using a self-administered questionnaire. In the surveys, students answer 4 questions relating to suicidal behavior for the 12 months preceding the survey: whether they seriously considered suicide, made a suicide plan, attempted suicide, and whether any of the attempts had to be treated by a doctor or nurse. In 2009, 13.8% of students in the United States reported that they had seriously considered suicide (10.5% of males and 17.4% of females), whereas 10.9% made a suicide plan (8.6% and 13.2% of males and females, respectively) and 6.3% made an attempt (4.6% and 8.1% of males and females, respectively). The percentage of attempts requiring medical treatment was lower at 1.9% (1.6% and 2.3% of males and females, respectively). The National Survey of Drug Use and Health asks respondents aged 18 years or older about suicidal thoughts and behavior. Annual averages of combined 2008 and 2009 data found an estimated that 8.3 million adults aged 18 years or older (3.7% of the adult population) reported serious thoughts of suicide in the past year, 2.3 million (1.0%) reported making a suicide plan, and 1.1 million (0.5%) reported attempting suicide. 15
Economic Burden
Injuries and deaths resulting from SDV represent a substantial drain on the economic, social, and health resources of the nation. One method of estimating the economic cost of suicide includes using 4 factors: medical expenses of emergency intervention and nonemergency treatment for suicide-related problems, the lost and reduced productivity of people suffering from suicide-related problems, the lost productivity of the loved ones grieving a suicide, and lost wages of those dying by suicide. Unfortunately, no recent study has measured all 4 of those factors. One study estimated that in 2000, the cost of SDV (fatal and nonfatal) was $33 billion ($32 billion in productivity losses and $1 billion in medical costs). 16
Compounding these costs are the unquantifiable costs of loss of life and the emotional trauma experienced by surviving family, friends, and communities that are affected by each person’s fatal or nonfatal suicidal behavior. 17
Risk and Protective Factor Research
Fatal and nonfatal suicidal behavior are influenced by many factors, including biological, psychological, social, cultural, political, and economic issues. 2 In this section, we provide a brief description of the risk and protective factors associated with suicidal behavior for various age groups.
Suicidal behavior is complex. Although we do not yet have complete understanding of the causes of suicidal behavior, we do know that, in general, individuals with any of the following characteristics may be at greater risk: have a diagnosable mental and/or substance abuse disorder (eg, clinical depression, manic depressive illness, schizophrenia, anxiety disorders, and alcohol abuse); have experienced violence (physical, sexual, intimate partner violence, or child maltreatment); are experiencing difficulty adjusting to adverse life events, such as separation or divorce; have attempted suicide previously; have access to a lethal method; have been incarcerated, or were recently arrested. 2 Research has indicated that it is the interaction of these along with some other factors that increase the risk of suicidal behavior. In other words, the more of these characteristics an individual has, the greater his or her risk of suicide. We will discuss in brief some of the factors associated with suicidal behavior in 3 selected age groups where there are important recognized transition periods.21,22
Older Adults
The proportion of older adults, persons aged ≥65 years, is growing in most Western societies and is the fastest growing age group in the United States. 23 During this stage, the often observed characteristics include physical changes such as limited regenerative abilities and increasing proneness to disease along with psychological aspects such as reflecting back on one’s life. 24 In 2007, persons aged ≥65 years represented 12.6% of the US population but accounted for 15.0% of all suicides. 6 Among males, suicide rates increase with age and are highest among males aged 75 years and older. 6 The highest rates are among older white males age 85 years and older, who have 4 times the overall national rate. Rates are highest for those who are divorced or widowed. However, this group is less likely to have engaged in nonfatal suicidal behavior than younger ages. 20 Some risk factors and protective factors for suicide are similar for older and younger adults; however, the magnitude of these factors might differ by age group (eg, the intensity of depressive symptoms, use of highly lethal methods, 25 and social isolation). 26 Suicide-related risk factors commonly cited for older adults include psychiatric illnesses such as clinical depression, schizophrenia, and alcohol and substance abuse; social isolation (ie, lack of a network of social support involving spouse, relatives, or friends on whom the individual can depend on as a resource); or certain physical health conditions. 27
Middle-Aged Adults
Middle age is roughly defined as persons aged 40 to 64 years. During this stage, persons must learn to handle certain life changes such as divorce, job plateauing or job shifts, children leaving home, declining health or death of parents, or change in their own health status. Females tend to have the highest suicide rates during this age period. Midlife suicides cause tremendous social and personal costs. For example, there are lost contributions to society, lost work productivity and income, interrupted childrearing, and disrupted marriages. It is much more difficult to identify unique suicide-related risk factors among this age group because much of the research on suicidal behavior has focused on youth and older adults. 28 As with all other age groups suicidal behavior occurs among middle-aged adults because of an interaction of factors. Typically among middle-aged adults the factors include socioeconomic issues (ie, financial problems and unemployment), social factors (ie, living alone), and psychiatric illness. However, there does appear to a strong relationship between socioeconomic problems and middle-aged suicides.29,30
Adolescents and Young Adults
This life stage includes the characteristics of risk-taking and establishing intimate relationships and one
Prevention Strategies
Although several publications2-4 have documented the widespread impact of suicidal behavior in the United States and around the globe, 2 important questions come to mind: “Can we prevent it?” and if so, “How do we prevent it?” Unlike some other fields of injury research and other areas of health-related research, the field of suicidal behavior prevention has been stifled by numerous barriers, some unique to the nature of this phenomenon,2,34 including lack of application of sound empirical theories. This has left many within the health care profession skeptical about the preventability of suicide.35,36 How much less willing might the public be to commit resources to this area if health care professionals themselves are unconvinced?
In this section, we describe general models for prevention strategies and then specific suicide prevention programs that could be categorized into the models. We also describe programs that are not suicide-specific but address factors related to suicidal behavior. The majority of strategies for preventing suicidal behavior have historically focused on individuals who have expressed suicidal thoughts and behaviors (eg, made an attempt) using a clinically based, provider-to-patient model. 2 Fewer strategies have focused on primary prevention. Moreover, recent comprehensive reviews of suicidal behavior prevention programs have shown only a limited number of programs, whether clinically oriented or focused on primary prevention, with evidence of having an impact on suicidal acts.38,39 We describe the types of suicide prevention programs, including those with minimal prevention evidence if there is some indication of potential benefit. The programs meeting this criterion have at least one of the following:
are theory-based, meaning the program addresses an empirically based risk or protective factor;
have an evaluation study specific to suicidal behavior showing a significant positive effect;
have an evaluation study not specific to suicidal behavior, but to a relevant risk factor, showing a significant positive effect; or
are judged by experts, based on a systematic review, as being likely to succeed. 39
Public health strategies are traditionally characterized in terms of 3 levels of prevention: primary prevention approaches, which aim to prevent a problem before it occurs; secondary prevention approaches, which focus on the more immediate responses to a problem, such as emergency services following an injury sustained as a result of violence; and tertiary prevention approaches, which focus on long-term care such as rehabilitation and reintegration, attempts to lessen trauma or reduce the long-term disability associated with violent acts. These levels of prevention are defined by their temporal aspect—whether prevention takes place before violence occurs, immediately afterward or over the longer term. However, prevention specialists have increasingly been using a definition of prevention that focuses on the target groups of interest. This definition of prevention characterizes target populations into 3 groups using the terms universal, selected, and indicated. 40
Universal strategies are aimed at groups or the general population without regard to risk or vulnerability such as a suicide prevention curriculum delivered to all students in a school or children in a particular grade.
Selected strategies are aimed at populations that are at heightened risk (ie, have one or more risk factors for suicidal behavior or have a greater probability of developing the problem than other groups in the population; egg strategies aimed at persons with depression or substance abuse problems).
Indicated strategies are aimed at those who have already demonstrated suicidal behavior (ie, have already made a suicide attempt).
Universal strategies, particularly those aimed at broad segments of the general population, may have a greater impact on decreasing morbidity and mortality than those focused only on a small number of high-risk persons. 41 Universal strategies could include media campaigns42,43 that seek to provide information, modify negative social norms, change the way suicide is portrayed in the media or news stories,44,45 or create environmental change. These campaigns often address an aspect of suicidal behavior called contagion, defined as the process by which one suicide facilitates the occurrence of a subsequent suicide. The pathway of contagion can be direct (imitating someone else’s suicidal behavior) or indirect (occurrence of suicides in the community or coverage in the general broadcast or print media may produce a familiarity with and acceptance of the idea of suicide). 43 Policy and environmental-related efforts for the general population that aim to reduce access to means, such as firearms,46,47 self-poisoning, 48 gas, 49 or high places such as bridges 50 are other examples of universal approaches. Many school-based programs have used a universal approach with awareness and skills training projects.39,51 These programs are designed to educate all students about suicide and available resources and teach various skills such as decision making or social problem-solving skills.
Several types of strategies have been directed at individuals who are at a higher risk for suicidal behavior or in a position to assess risk for suicidal behavior within specific at-risk groups. 51 Programs using a gatekeeper training model instruct participants to identify and refer persons at risk for suicidal behavior. The purpose of gatekeeper training is to develop the knowledge, attitudes, and skills to identify individuals at risk, determine the levels of risk, and make referrals when necessary. Those who are trained can be school staff, community members, or physicians. 52 School-based prevention programs that offer support and skills training for high-risk students (eg, those who have had a friend or relative complete suicide) are another example of a selected strategy. 53 Similar efforts have been directed at families who have experienced the loss of a loved one to suicide. Some efforts have lowered access to proximal risk factors for suicidal behavior such as alcohol misuse.54,55
Indicated prevention strategies include clinical or medical interventions56,57 and skill-building support groups for individuals who have experienced suicidal ideation or behavior, 58 case management, and referral resources for crisis intervention and treatment. 59 Two important approaches for suicidal individuals are dialectic behavior therapy (DBT) and cognitive therapy.60,61 There is some overlap in the specific interventions used in either approach, both usually include behavioral analysis and therapy that focuses on problem solving, skills training, and addresses social competence and adaptive coping. Included in this indicated category are programs that address suicidal behavior prevention among the incarcerated population with suicidal ideation or behavior.62,63 Hotlines and crisis centers are other examples. There are few studies that have evaluated the latter strategies, and those that have reach inconsistent findings.64,65
Several organizations have used integrated approaches in which they incorporate universal, selected, and indicated approaches. Although these are challenging to design, execute, and evaluate, because activities occur on multiple levels of prevention, they may have the best chance of success.66,67
There are also programs designed to address other health problems that have potential for reducing suicidal behavior. These programs are not suicide specific but may apply to a range of suicide-inclusive factors, for example, factors that may relate to several health issues such as early antisocial behavior, substance abuse, or child maltreatment.68-70 Interventions for suicide-inclusive factors have the promise to bring a wider range of health benefits in that they may reduce more than one adverse outcome.71,72 Strategies that address the social determinants of health would fit into this category since these determinants are relevant to the factors associated with suicide such as social isolation, population growth, discrimination, addictive behaviors, mental health crises, and stigma associated with help seeking.73,74 Some communities have adopted programs using social determinants of health as a framework for their suicidal behavior prevention efforts.75,76
Role of Preventive Medicine Practitioners
Preventive medicine practitioners approach health in a manner that looks at systemic and population-based interventions to improve the health of individuals. 77 This basic tenet of preventive medicine lends itself to a public health approach for suicide prevention, 78 and preventive medicine practitioners can serve several roles in the prevention of suicide. These roles include clinical responsibilities, advocacy for individual patients and communities, research, and education.
As a clinician, the preventive medicine practitioner may have clinical responsibilities from both the individual patient and population-based perspectives. Preventive medicine practitioners who work in primary care settings, schools, community centers, homeless shelters, and other related locations have the access and opportunity to play a pivotal role in suicide prevention. 79 For guidance on appropriate assessment of suicidal ideation, depression, and other risk factors, preventive medicine practitioners should be aware of specialty organization policy statements and guidelines related to suicide prevention and use them to guide decision making. It is important for practitioners to consider and establish a suicide prevention protocol involving anticipatory guidance, appropriate assessment, and counseling of patients during health maintenance visits. 79
Practitioners should seek evidence-based assessment tools and best-practice models. Resources such as the Substance Abuse and Mental Health Services Administration’s (SAMHSA) National Registry of Evidence-Based Programs and Practices (NREPP) may be helpful. NREPP is a searchable online registry of mental health and substance abuse interventions that have been reviewed and rated by independent reviewers. 80 The registry is designed to assist practitioners in identifying approaches to preventing and treating mental and/or substance use disorders that have been scientifically tested and that can be readily disseminated to the field. A search of the registry reveals several prevention programs associated with suicide and/or its risk factors but many of these programs would likely be considered promising 81 by more rigorous evaluation standards.
Some preventive medicine practitioners who work in local or state health departments or in federal health agencies have a critical opportunity to influence suicide prevention through application of the public health approach.7,9 There is an increased need for assessment priorities to focus on the collection, analysis, and dissemination of data associated with suicide and its risk factors. A supporting focus on community health needs related to suicide is also warranted. Preventive medicine practitioners in public health agencies also serve an important function in comprehensive suicide prevention policies. They may do this by supporting the use of evidence-based research studies in decision-making about suicide prevention policies as well as by participating in the development of such policies. Practitioners who work in public health agencies also have a duty to assure the public that services necessary to achieve suicide prevention goals are provided. This may occur through direct service provision or via partnerships with other governmental agencies, private organizations, or academic institutions.
Clinicians can extend beyond the provision of good clinical care to advocacy on behalf of patients and communities to collaborate with individuals and organizations in order to prevent suicide. Because of their unique training and practical experience, preventive medicine practitioners can serve as compelling advocates regarding suicide prevention in their communities. A clinician’s obligation to advocacy is grounded in this professional experience and expertise as well as a duty to patients. 82 Their insight can provide a unique perspective to decision makers in the business, private, and government sectors. Advocacy activities may include communicating with regulatory, legislative, and administrative bodies on national, state, and local levels. Activities may focus on policy development, suicide prevention media campaigns, or funding to support suicide prevention education programs and research both for implementation of those approaches with solid evidence and/or promoting evaluation of pilot programs. 78 Prevention specialists with an interest in advocacy may seek opportunities and learn by doing, but they should also consider mechanisms to obtain formal advocacy training. Several regulatory physician organizations recognize the role of clinicians in health advocacy and the need for them to obtain the skills required for effective advocacy.83,84 Preventive medicine practitioners may find such training experiences through seminars or conference sessions at professional specialty conferences or through fellowship experiences. For example, the Physician Advocacy Fellowship sponsored by the Institute of Medicine as a Profession supports physicians in developing or enhancing their advocacy skills by implementing a project in partnership with an advocacy organization. 85 The unique skill set possessed by prevention practitioners also lends itself to active involvement with professional organizations in developing a suicide prevention policy statement on behalf of the organization.
Preventive medicine practitioners are needed to address the deficits in research associated with suicide prevention programming and risk assessment tools. Numerous suicide prevention programs have been created for the primary care and community setting. However, few programs have been evaluated using rigorous, scientifically controlled mechanisms.86-88 Although the importance of primary prevention for suicidal behavior is widely accepted, and there is a need for multiple options to address suicidal behavior such as screening for suicide risk, additional research is needed to develop evidence-based screening tools and practices.89-91 The research deficits have practical implications, as they affect recommendations for screening for suicide risk. The US Preventive Services Task Force (USPSTF) concludes that the evidence is insufficient to recommend for or against routine screening by primary care clinicians to detect suicide risk in the general population.91-93 Practitioners can address these research needs by contributing rigorous, evidence-based models to the extant body of literature and to program repository programs such as NREPP. Practitioners engaged in research may also conduct studies using intentional injury data systems such as the National Electronic Injury Surveillance System (NEISS) and the National Violent Death Reporting System (NVDRS).94-96
Prevention practitioners encompass a broad array of expertise in a variety of areas. However, some practitioners may not have developed proficiency in the subject of suicide prevention. In these cases, practitioners should employ every available opportunity to gain knowledge, including information about suicide risk and protective factors, and the latest evidence for screening, treatment, and prevention modalities. Formal learning options include professional development and continuing education conferences. Noon seminars and journal clubs may also be used. Practitioners should also become aware of community resources for patients and population-based activities. 80 In addition, practitioners must be sensitive to the unique characteristics of the population with whom they interact. Understanding these cultural differences is critical for communicating with people from diverse geographic, ethnic, racial, cultural, economic, sexual orientation, and spiritual or social backgrounds.97,98
Conclusion
Injury from SDV, which includes suicidal behavior, is a major cause of recorded mortality and morbidity throughout the world. The measurable human and economic costs of suicide are enormous; compounding these costs are the unquantifiable costs of loss of life, and the emotional trauma experienced by surviving family, friends, and communities affected by each person’s fatal or nonfatal suicidal behavior. Because of the complex nature of this health risk, it should be approached systematically and with a focus on population-based approaches if we are to make an impact on its reduction. Population-based approaches include several roles for the preventive practitioner. These include responsibilities related to direct clinical service provision and access, research, education, and policy. In this manner, prevention practitioners may contribute to the reduction of access to mechanisms to inflict lethal injury, identification of and treatment for those with modifiable risk factors, and the adjustment of social–cultural–behavioral determinants that contribute to suicide as an alternative.
Prevention practitioners are trained to approach health concerns from the broad scope of an entire community as well as the context of the individual patient. This combined perspective is essential to addressing the population-based, subgroup, and individual issues that are such a prominent part of modern life in the United States.
Footnotes
*
Unless otherwise noted, the source of all mortality data is the Centers for Disease Control and Prevention’s Web-based Injury Statistics Query and Reporting System. 6
**
Northeast = Connecticut, Maine, Massachusetts, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, and Vermont. Midwest = Illinois, Indiana, Iowa, Kansas, Michigan, Minnesota, Missouri, Nebraska, North Dakota, Ohio, South Dakota, and Wisconsin. South = Alabama, Arkansas, Delaware, District of Columbia, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, Virginia, and West Virginia. West = Alaska, Arizona, California, Colorado, Hawaii, Idaho, Montana, Nevada, New Mexico, Oregon, Utah, Washington, and Wyoming.