
Abstract
Chronic obstructive pulmonary disease (COPD) is a major and increasing cause of morbidity and mortality. Cigarette smoking is the most important risk factor for COPD, and smoking cessation is, in most cases, the most effective way of preventing the onset and progression of COPD. The purpose of the present article was to review the current state of interventions for smokers with COPD. Because 70% of smokers visit a physician annually, primary care providers play a key role in the counseling of all patients at every visit. If smoking cessation is achieved at an early stage of disease, it is associated with a decrease in pulmonary symptoms and improves prognosis and prolonged abstinence. The health benefits of smoking cessation are immediate and substantial, and interventions provided for smokers suggest that multiple modalities are needed. Smoking cessation counseling in combination with nicotine replacement therapy (NRT) appears to be the most effective modality followed by smoking cessation in combination with an antidepressant to enhance prolonged abstinence.
Introduction
Chronic obstructive pulmonary disease (COPD) affects more than 5% of the US adult population and is a major cause of morbidity and mortality.1,2 Of the 6 leading causes of death in the United States, COPD is the only one that continues to steadily increase. 3 Currently, COPD is the fourth leading cause of death in the United States and is projected to be the third leading cause of death by 2020.4,5 COPD also imparts a high economic burden on the health care system, and the 2010 projected direct economic cost for COPD health expenditures is $29.5 billion. 6 Although there are a number of factors associated with the development of COPD (ie, genetic, occupational or environmental exposure, gender, age, respiratory infections, socioeconomic status, nutrition, and comorbidities),4,7-9 cigarette smoking is the primary risk factor for developing COPD. 10 In fact, it has been estimated that 12.5% of current smokers and 9.4% of former smokers have COPD. 11 Additionally, it has been estimated that 20% of smokers will develop progressive COPD, where there is an accelerated rate of decline in forced expiratory volume in 1 s (FEV1) leading to airway obstruction that is not fully reversible. 12
Smoking cessation is the only evidence-based treatment that has been proven to reduce the accelerated rate of lung function decline, decrease symptoms of cough and sputum, and reduce COPD exacerbations.
Smoking cessation is the single most effective therapeutic intervention to reduce the risk of developing COPD as well as to stop its progression.10,13 The health benefits of smoking cessation are immediate and substantial. Smoking cessation is the only evidence-based treatment that has been proven to reduce the accelerated rate of lung function decline, decrease symptoms of cough and sputum, and reduce COPD exacerbations.14,15 In fact, quitting smoking is associated with a short-term, modest (less than 50 mL) increase in FEV1, which lasts around 1 year followed by a resumption of decline in FEV1 but at a nonsmoker’s rate. 15
Quitting smoking not only improves pulmonary function but also provides other benefits. Smoking cessation reduces the risk for lung cancer, the severity and progression of premalignant histological changes, other types of cancer, myocardial infarction, stroke, and chronic lung disease.16,17 In the first year following smoking cessation, there is a 50% reduction in cardiac events, and the risk of stroke is reduced to that of a nonsmoker’s within 5 to 15 years. Smoking cessation results in a 50% reduction in bladder cancer and 30% to 50% decreased risk in former smokers compared with current smokers after 10 years of smoking cessation. Other benefits include elimination of the damaging effects of tobacco on the skin, breath, teeth, and gums as well as the elimination of the expense of cigarettes.16,17 Even among individuals with severe, early onset COPD, smoking cessation has been found to have a benefit on survival. Smoking cessation is therefore beneficial for smokers at any stage of COPD disease progression and is an effective measure to implement during any stage of the disease.
Role of Health Care Providers in Smoking Cessation
About 70% of smokers visit their physician annually, and primary care providers play a critical role in reducing the burden of tobacco-related health problems by helping their patients who smoke to quit. 18 As recommended by the GOLD Guidelines, “health care providers, including physicians, nurses, dentist, psychologists, pharmacists, and others are key to the delivery of smoking cessation messages and interventions.” 10 Because cigarette smoking is a highly addictive behavior and, for many smokers, requires multiple quit attempts before finally succeeding, smoking cessation counseling (SCC) provided by physicians and their staff may help improve the chances of the patient’s successful cessation.
Interventions delivered by physicians and other health professionals have reportedly yielded significant increases in quit rates as compared with self-initiated strategies. 18 Even interventions delivered by PCPs and their staff that are as brief as 3 minutes have resulted in smoking cessation rates of 5% to10%.10,18,19
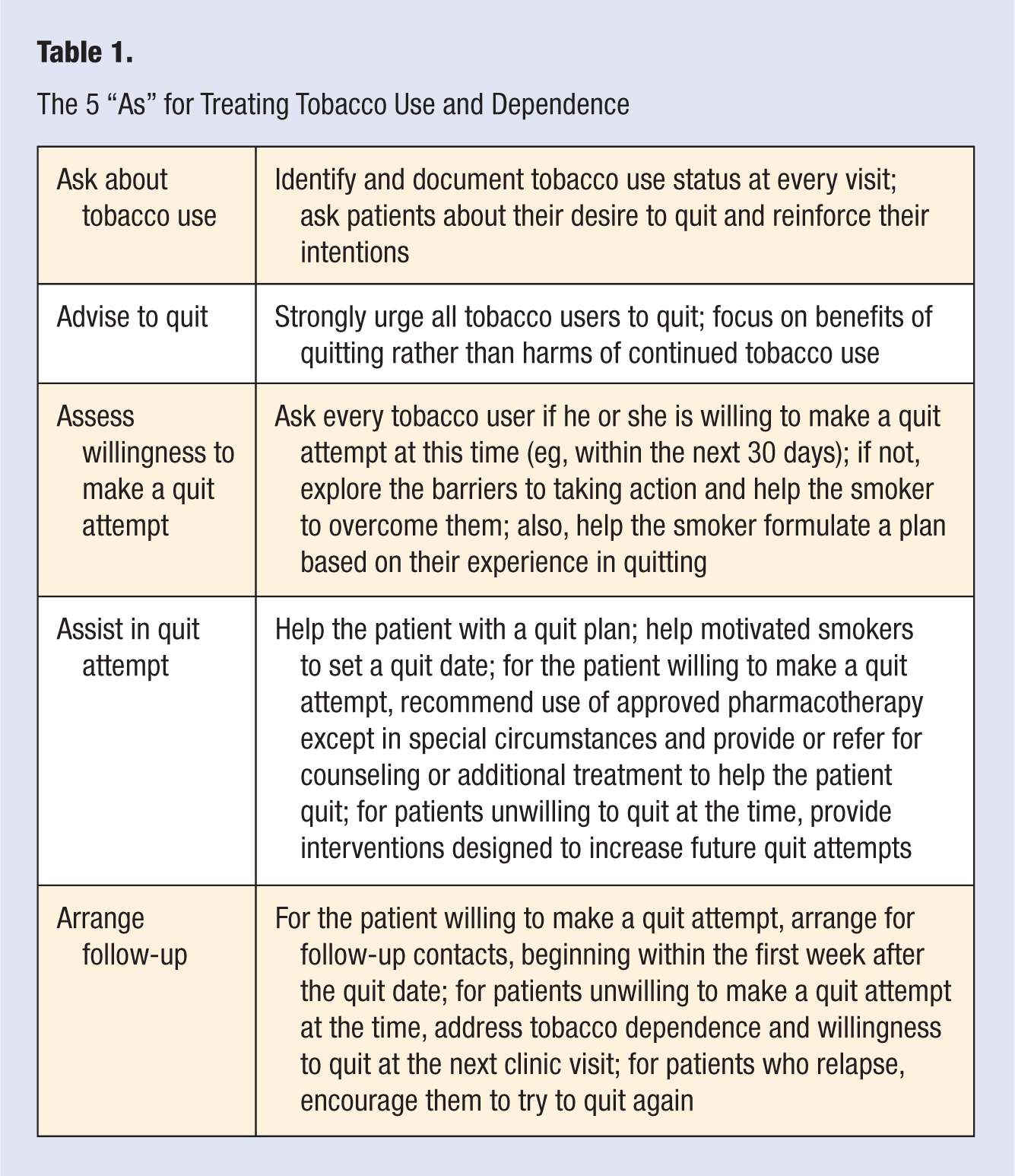
To assist health care providers in helping their patients quit smoking, a strategic framework has been developed by the US Department of Health and Human Services, which recommends a 5-step program (the 5 As for Treating Tobacco Use and Dependence) that is designed to be a brief and effective intervention for tobacco users in the primary care setting (see Table 1).18,20 The 5 major steps include the following: (1) at every visit, ask the patient if he or she uses tobacco; (2) advise the individual to quit smoking; (3) assess their willingness to make a quit attempt; (4) assist those who are willing to make a quit attempt, help motivated smokers to set a quit date, offer first-line pharmacotherapies, and provide or refer the patient for counseling; and (5) arrange for follow-up contacts either in person or via telephone to prevent relapse. 18
The 5 “As” for Treating Tobacco Use and Dependence
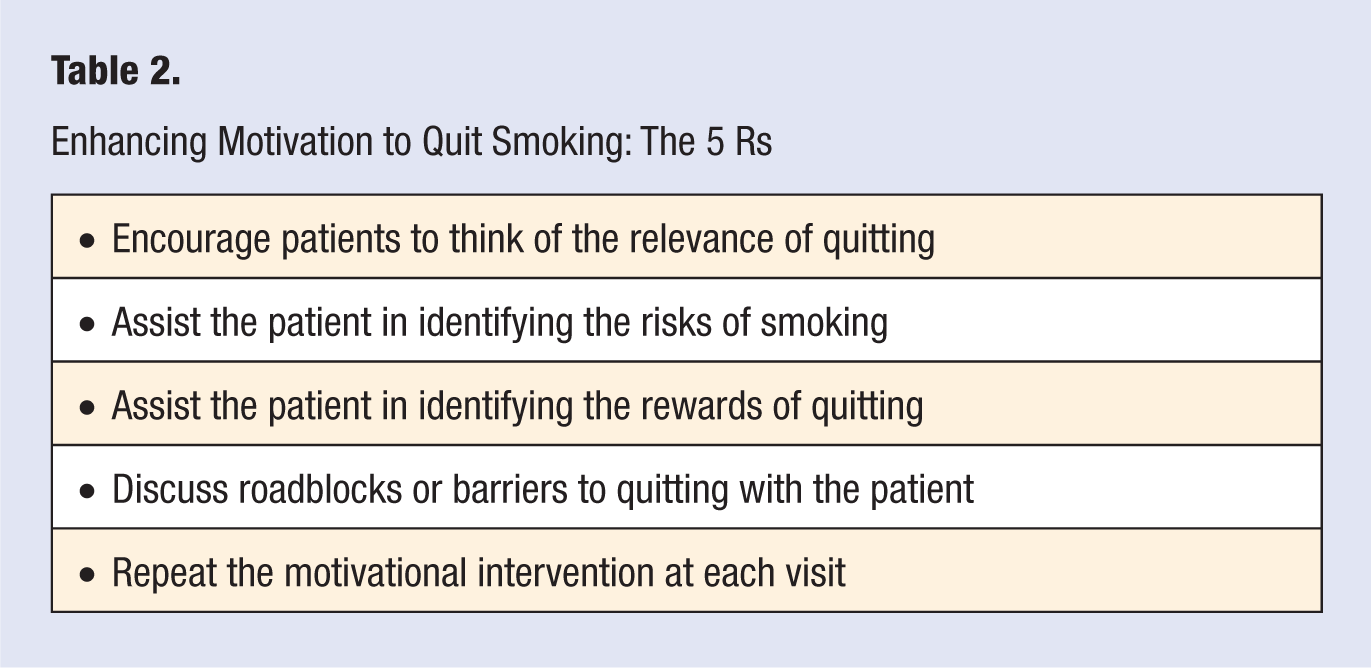
For those smokers who are currently unwilling to make a quit attempt at the present time, the intervention should be designed to promote motivation to quit using the 5 Rs (see Table 2).18,20 Evidence suggests that successful motivational interventions are more likely when the clinician is empathic, avoids arguments, and supports patient self-efficacy.18,21 For those individuals who recently quit, brief relapse prevention treatment should be provided because of the chronic relapsing nature of tobacco dependence (ie, reinforce the smoker’s decision to quit, review benefits of quitting, and assist in resolving problems arising from quitting) 18 and because it requires only around 3 minutes of the clinician’s time. Counseling is most likely to be successful when the provider is empathic, promotes patient’s autonomy, and supports the patient’s self-efficacy.18,21
Enhancing Motivation to Quit Smoking: The 5 Rs
For patients who recently quit smoking, providers or their staff should discuss relapse prevention because of the chronic relapsing nature of tobacco dependence. Counseling for those who quit recently should reinforce the decision to quit, review the benefits of quitting smoking, and assist the patient in resolving any residual problems. Most relapses occur within the first 3 months after quitting, particularly within the first 2 weeks; providers (or staff) should therefore provide follow-up visits and relapse prevention counseling during this critical period. 18
Most individuals go through several stages before quitting smoking, and it is helpful to assess the patient’s readiness to quit to determine the most effective program. Prochaska and DiClemente 22 developed a model (the Transtheoretical Model or TTM) that describes an individual’s efforts to change his or her own addictive behavior, and this has proved useful in the design of tailored interventions for smoking cessation. 22 The Stages of Change Model describes the process as individuals progress through the 5 stages of readiness to act on a healthier behavior and provides strategies to guide individuals through the stages of change. The 5 stages include the following: precontemplation, where the smoker does not intend to quit smoking within the next 6 months; contemplation, where the smoker intends to quit smoking within the next 6 months but lacks commitment to actually start changing; preparation, where the smoker decides to quit smoking within the next 30 days; action, where the smoker has made a quit attempt within the past 6 months; and maintenance, when the smoker has remained smoke free for more than 6 months and is working to prevent relapses). 22 Individuals usually go through a series of steps or stages before they are ready to quit smoking, and the process of quitting smoking may take, on average, between 3 to 4 quit attempts before the smoker succeeds, and this may require repeated interventions.18,20
Smoking Cessation Interventions
Currently, the smoking cessation interventions available include behavioral, pharmacological, and alternative interventions (including hypnotherapy, acupuncture, aversive therapy, exercise, and electrostimulation).
Behavioral Interventions
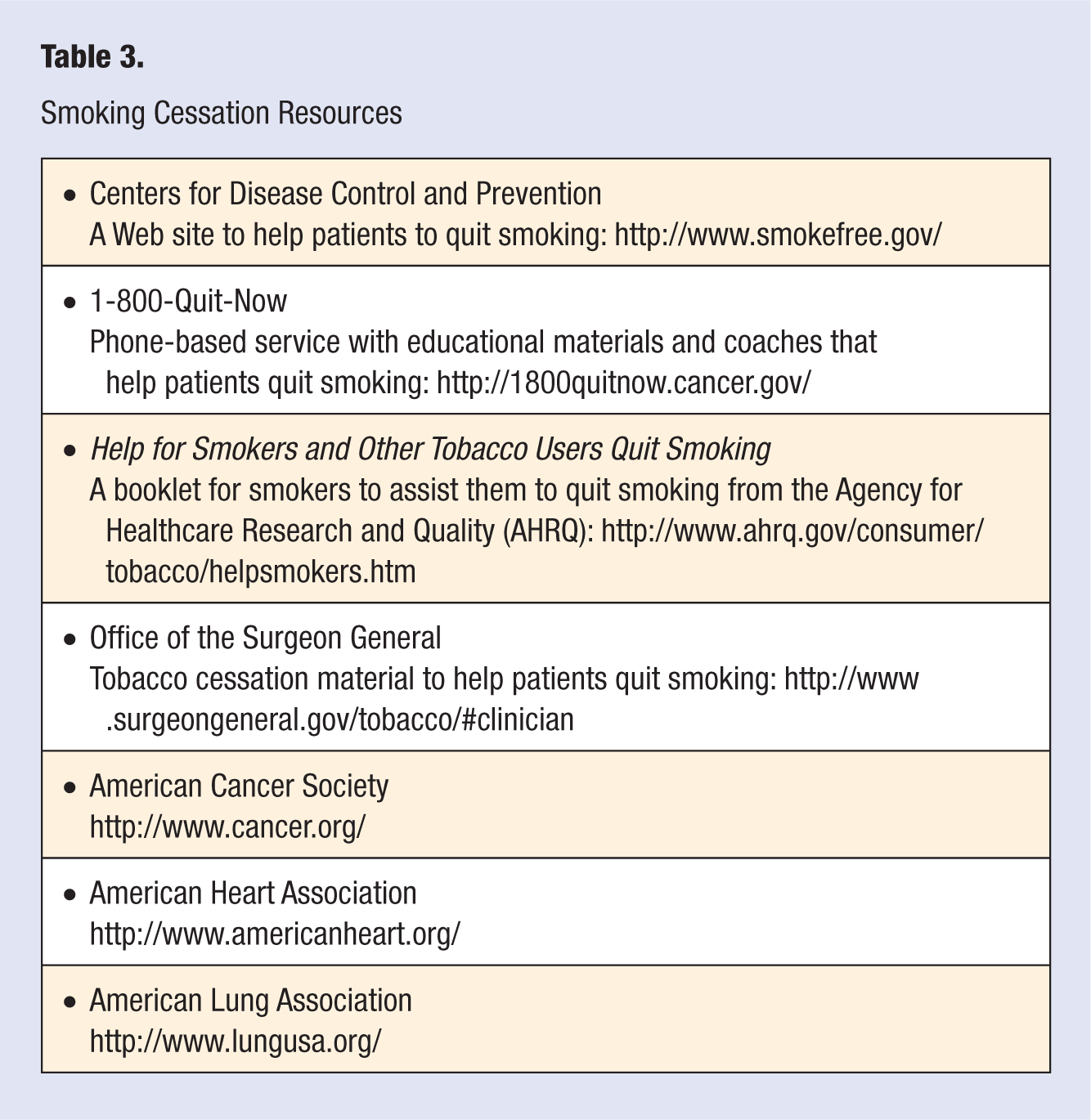
The counseling therapies should assist in motivating the smoker to quit smoking and developing skills and strategies to cope with nicotine withdrawal, and they should also help the smoker identify cues and situations that would lead to temptation or pressure to smoke (see Table 3).
Smoking Cessation Resources
Individual, group, and telephone counseling have been used and have been helpful in smoking cessation.18,19 Whereas brief counseling sessions to encourage smokers to quit smoking result in quit rates of 5% to 10%, there is a strong dose–response relationship between the intensity of the counseling and success in quitting smoking.10,19 Those interventions that are more intense have higher success rates and are more cost-effective than those that are less intensive. The intervention may be intensified by increasing the number of sessions, increasing the length of the session, and/or increasing the duration of the treatment. 10 Because the clinician has limited time to counsel patients, clinical staff (ie, physician assistants, nurses, medical assistants, and other staff) may reinforce the brief provider clinician cessation message as well as provide follow-up and support services to patients attempting to quit. 23 Overall, it has been found that the rate of successful smoking cessation at 1 year is 3% to 5% for individuals who have used self-initiated strategies, 7% to 16% for those who receive behavioral therapy, and, based on several meta-analyses, abstinence rates around 25% to 30% in 1 year when both pharmacological and behavioral therapies are combined.18,24
Additional behavioral approaches include the use of telephone counseling. One study of smokers who used a Smokers Telephone Helpline found that those who received 7 telephone counseling sessions for smoking cessation had increased rates of quitting compared with noncounseled smokers (9.1% vs 6.9%). 25 Self-help and print materials may also be used in combination with the telephone counseling. In addition, written self-help material may make a small contribution when given in addition to provider advice.15,18
Pharmacotherapy
For those patients who have been unable to quit or sustain abstinence using behavioral interventions alone, pharmacotherapy is another option. However, for those patients with medical contraindications, special consideration is required before recommending pharmacotherapy. Pharmacotherapy can be divided into 2 groups: nicotine replacement therapy (NRT) and non-NRT therapy. The first-line medications with an established record of efficacy in smoking cessation include both NRT (nicotine transdermal patches, nicotine gum, nicotine nasal spray, nicotine inhalers, and nicotine lozenges) and non-NRT therapies (sustained-release bupropion, which is an antidepressant) that have been endorsed by the US Clinical Practice Guidelines. 18
Nicotine replacement therapy
NRT is available over the counter and delivers a fixed dose of the drug over 16 to 24 hours. NRT has been reported to almost double the likelihood of smoking cessation compared with no therapy (odds ratio [OR] = 1.77; 95% confidence interval [CI] = 1.66-1.88). In addition, the nicotine patch combined with another NRT has been reported to be more effective than any single NRT and may be considered if there are no medical contraindications. 20
Bupropion SR
This is an antidepressant that reduces nicotine withdrawal symptoms and cravings. Bupropion blocks the reuptake of dopamine and norepinephrine, which is thought to be the mechanism behind its effect on smoking cessation. Bupropion SR alone or in combination with the nicotine patch significantly increases long-term cessation rates compared with the patch alone (abstinence for the placebo group at 12 months was 15.6% in the placebo group compared with 16.4% in the nicotine patch group, 30.3% in the bupropion group (P < .001), and 35.5% in the group receiving both bupropion and nicotine patch (P < .001).20,27 However, bupropion SR is contraindicated in patients with a history of seizure disorder or uncontrolled hypertension.20,26
Varenicline
Varenicline is a partial nicotinic acetylcholine receptor agonist. It aids smoking cessation by relieving nicotine craving and withdrawal symptoms as well as blocking the nicotine receptors, which prevents the dopamine release associated with nicotine withdrawal. 27 Varenicline has been reported to be the most effective of the available pharmacological treatments for smoking cessation.
Two other medications that have also been endorsed by the US Clinical Practice Guidelines and have been found to be effective in blocking nicotine withdrawal symptoms include clonidine and nortriptyline as second-line therapies, which may be considered if first-line pharmacotherapies are contraindicated or not effective (see Table 4).18,28,29
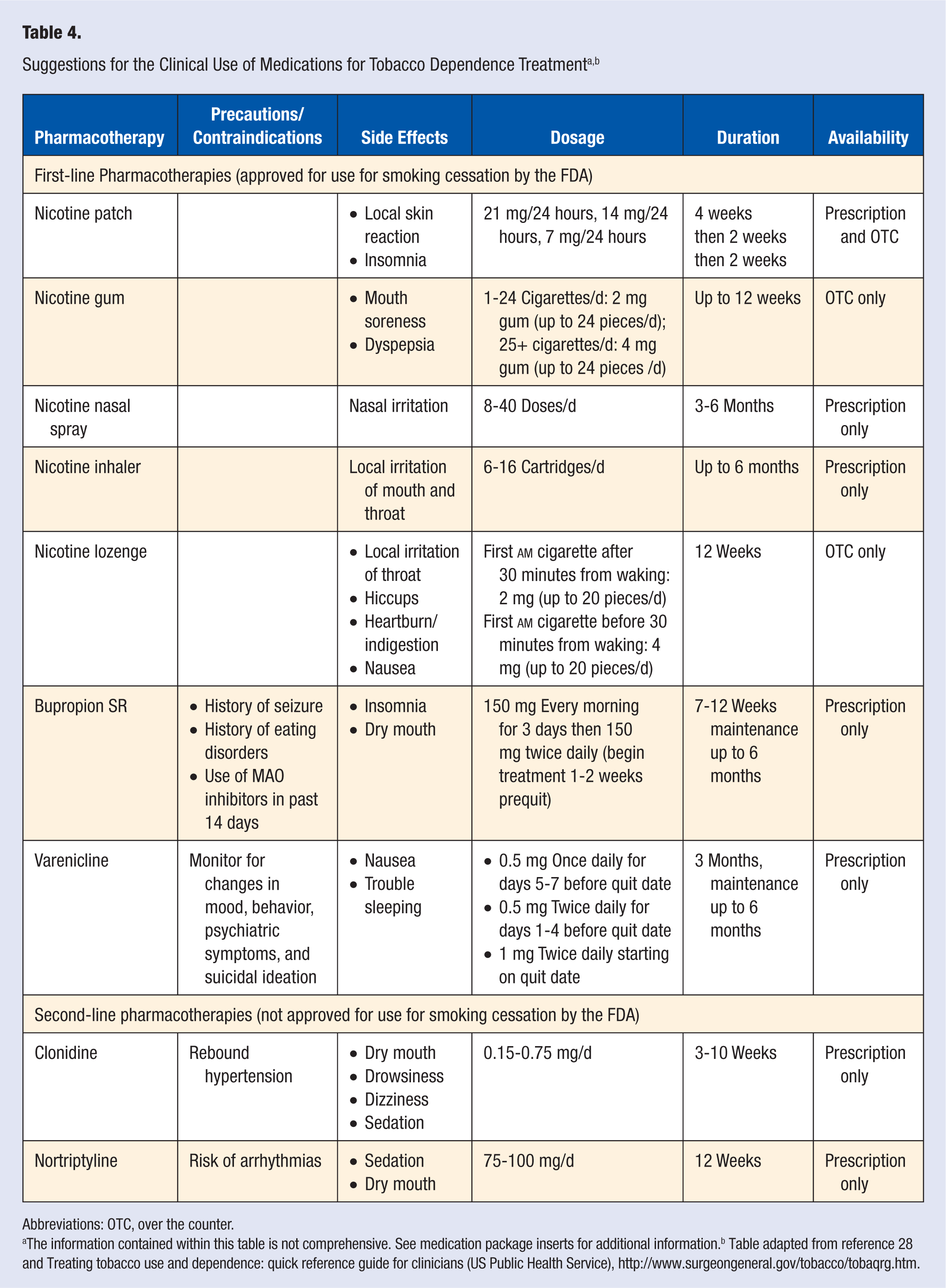
Abbreviations: OTC, over the counter.
The information contained within this table is not comprehensive. See medication package inserts for additional information.b Table adapted from reference 28 and Treating tobacco use and dependence: quick reference guide for clinicians (US Public Health Service), http://www.surgeongeneral.gov/tobacco/tobaqrg.htm.
Wu et al 30 examined the effectiveness of smoking cessation pharmacotherapies in a systematic review and meta-analysis and found that NRT, bupropion, and varenicline all provide therapeutic effects that assist in smoking cessation. The factors that should be considered in prescribing pharmacotherapy should include patient preference, patient’s previous experience, side effects, and level of scientific evidence.
Effectiveness of Smoking Cessation Interventions for COPD Patients
Although there is an extensive literature on the effectiveness of smoking cessation interventions among the general population, smoking cessation studies tailored specifically for COPD patients have been limited until recently. Van der Meer et al 31 performed a systematic review of 5 smoking cessation randomized controlled trials in participants with confirmed COPD. However, of the 5 studies included, no evidence was found with respect to the effectiveness of any of the interventions. More recently, Strassmann et al 32 assessed the effectiveness of smoking cessation interventions for COPD patients. Randomized controlled trials were included if patients had had COPD confirmed by spirometry or physician-diagnosed COPD and if they were of moderate to good methodological quality (see Table 5 for details).
Characteristics of Included Trials a
Table 5 reproduced with permission from the European Respiratory Society Journals Ltd (reference 32).
Strassman et al 32 reported that of the 8 randomized controlled trials included in the meta-analysis,32-40 SCC in combination with NRT had the greatest effect on prolonged abstinence, with the odds being 5 times higher (OR = 5.08; 95% CI = 4.32-5.97; P < .001) than with SCC alone (OR = 2.80; CI = 1.49-5.26; P = .001) or SCC in combination with an antidepressant (OR = 1.53; CI = 0.71-3.30; P = .28). 32 The second most effective intervention was SCC combined with an antidepressant, which was 3 times more effective compared with usual care (OR = 3.32; CI = 1.53-7.21; P = .002) versus SCC alone (OR = 1.83; CI = 1.18-2.83; P = .007). 32 SCC alone was of borderline effectiveness compared with usual care (OR = 1.82; 95% CI = 0.96-3.44; P = .07). 32 Of those studies that offered SCC interventions, abstinence tended to be related to the intensity of the counseling. Prolonged abstinence tended to be increased by high-intensity SCC compared with low-intensity SCC, although this was not statistically different (OR = 1.46; 95% CI = 0.44-4.90; P = .54). 32
It was interesting to note that the results of these studies specifically tailored for COPD patients were similar to those for the general smoking population. 32 Although there were variations in the SCC interventions, number of patients recruited, and methods of recruitment (clinic vs hospitalized patients), results suggested that, similar to smokers in general, NRT and antidepressants provide added benefits to SCC interventions for COPD patients (OR = 3.32; 95%CI = 1.53-7.21).41,42
It is of concern that although most smokers (about 70%) would like to stop smoking, only around 44% try to quit each year.18,43 To improve smoking cessation rates, effective treatments that are tailored for COPD patients are needed.
Discussion
COPD is a major and increasing cause of morbidity and mortality. Cigarette smoking is the most important risk factor for COPD, and according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) Guidelines, “smoking cessation is, in most cases, the most effective and cost-effective way of preventing the onset and progression of COPD.” 10 If smoking cessation is provided at an early stage of disease, it is associated with a decrease in pulmonary symptoms, and there is an improvement in prognosis and prolonged abstinence. 10 However, for many smokers, tobacco dependence is a chronic, relapsing disorder and may require multiple attempts before finally succeeding to quit. 17 Additionally, because counseling by a physician has been found to be effective, all patients should be counseled at every visit to help with smoking cessation and relapse prevention efforts once the patient has quit. 11
One of the characteristics of smokers with COPD that will affect the success of the SCC and must be taken into consideration when developing the counseling approach is the presence of psychiatric disorders such as depression or anxiety. It is well known that for smokers with depression or a history of depression, it is more difficult to quit smoking and more difficult to sustain abstinence, and frequent relapses may also occur, requiring repeated interventions. Smokers with a history of current major depression have been found to have lower quit rates than smokers with either no current or past depression. Because depression can occur during withdrawal and smoking cessation may contribute to the occurrence of depression during the postcessation period, depression-prone smokers are less likely to remain abstinent. Therefore, depression should be addressed when providing SCC for COPD smokers with depression. 44
In summary, the health benefits of smoking cessation are immediate and substantial, and interventions offered by the providers for smokers (based on the few trials conducted specifically for smokers with COPD) suggest that multiple modalities are needed. The basic components of the smoking cessation interventions should include simple advice, written self-help materials, individual and/or group behavioral support, nicotine replacement, and/or bupropion SR. Because behavioral interventions alone have had only modest success, drug therapy has been increasingly relied on to assist in smoking cessation interventions. SCC in combination with NRT appears to be the most effective smoking cessation intervention, followed by smoking cessation in combination with an antidepressant to enhance prolonged abstinence. Unfortunately, the current literature is limited, and current interventions available for smokers with COPD have not been effective in sustaining long-term smoking abstinence among COPD patients. Additional research is needed to examine whether interventions tailored specifically for COPD patients will increase smoking quit rates.
Footnotes
Acknowledgements
Table 4 adapted from reference 28 and Treating tobacco use and dependence: quick reference guide for clinicians (US Public Health Service), http://www.surgeongeneral.gov/tobacco/tobaqrg.htm. ![]() reproduced with permission by European Respiratory Society Journals Ltd (reference 32).
reproduced with permission by European Respiratory Society Journals Ltd (reference 32).