
Abstract
Background
The elevated mortality rate associated with sepsis is a primary global health concern. The correlation between bicarbonate levels and mortality risk in sepsis remains unclear.
Method
A retrospective cohort study was conducted using data from the MIMIC-IV database, including 12 744 adult sepsis patients. The primary exposure was serum bicarbonate levels, categorized into quintiles. The primary outcome was 28-day mortality, and secondary outcomes included 90-day mortality. Multivariable Cox regression models adjusted for demographic, clinical, and laboratory variables were used to examine the relationship between bicarbonate levels and mortality. Curve fitting and sensitivity analyses were performed to validate the findings.
Results
A U-shaped relationship between serum bicarbonate levels and 28-day mortality was identified. Both low (≤19.0 mEq/L) and high (>26.0 mEq/L) bicarbonate levels were associated with increased mortality risk. Patients with bicarbonate levels between 24.0-26.0 mEq/L had the lowest 28-day mortality. The relationship remained consistent across subgroups, and an inflection point was observed at 25.0 mEq/L. Sensitivity analyses confirmed the robustness of the findings across different data imputations.
Conclusion
This study demonstrates that both low and high serum bicarbonate levels are associated with increased mortality in sepsis patients. The optimal bicarbonate range for minimizing mortality risk appears to be between 24.0-26.0 mEq/L. These findings highlight the importance of monitoring bicarbonate levels in clinical practice, suggesting that maintaining bicarbonate within this range may improve patient outcomes. Further prospective studies are needed to confirm these findings and explore potential therapeutic strategies.

Introduction
Sepsis is a critical condition characterized by multi-organ failure resulting from an aberrant host response to infection. 1 This dysregulated host response is an excessive and uncontrolled systemic inflammatory response, 2 often referred to as an “inflammatory storm.” The release of large amounts of inflammatory factors causes cellular metabolic disruptions and mitochondrial dysfunction, which can lead to multiple organ dysfunction syndrome, including acute respiratory distress syndrome, sepsis-induced cardiac dysfunction, and acute kidney injury (AKI).3,4 Sepsis, characterized by a high mortality rate, represents a major global health concern. 5 In 2017, 11 million deaths were attributed to sepsis worldwide, accounting for 19.7% of all global fatalities that year. 6 The elevated mortality rate of sepsis is closely associated with the complex pathogenic pathways of inflammatory storm, immunosuppression, and metabolic disorders. 7 Early identification and active management of sepsis have been demonstrated to decrease the risk of death in patients. 8 Despite significant advancements in the treatment and management of sepsis, the elevated mortality rate associated with sepsis remains a critical concern.9,10 Therefore, clinicians must promptly identify and manage patients with sepsis who possess an increased risk of mortality.
Disruptions in acid–base equilibrium during sepsis are a prominent research topic. Acid–base homeostasis is essential for cellular metabolism and organ function, and its disruption is strongly associated with the risk of organ failure and mortality in patients with sepsis.11,12 The systemic inflammatory response elicited by sepsis can result in lactate buildup, 13 renal impairment, 14 and abnormal respiratory compensation, which can cause metabolic acidosis or mixed acid–base imbalance. 15 Research indicates that severe acidosis is independently linked to a heightened risk of mortality in critically ill patients, 16 whereas compensated alkalosis may worsen the prognosis by inhibiting the oxygen dissociation curve and aggravating electrolyte imbalances, such as hypokalemia. 17 Although bicarbonate is commonly utilized as a primary indicator of metabolic acid–base imbalance in clinical evaluations,18-20 its prognostic value remains under debate. Previous studies have primarily focused on the increased mortality risk associated with low bicarbonate levels.21,22 Low bicarbonate is considered to be significantly associated with acidosis, 23 reflecting tissue hypoperfusion and mitochondrial dysfunction. 24 However, some clinical observations suggest that high bicarbonate levels may increase cardiovascular mortality, 25 indicating that the relationship between bicarbonate levels and prognosis may not follow a simple linear pattern. Therefore, we hypothesized a U-shaped correlation between bicarbonate levels and mortality rates. We aimed to perform a retrospective cohort study to systematically investigate the relationship between serum bicarbonate levels and 28-day mortality in patients with sepsis.
Material and Methods
Data Source
This retrospective cohort study utilized data from the Medical Information Mart for Intensive Care-IV (MIMIC-IV). MIMIC-IV is a free, publicly accessible database that contains clinical data of all patients at Beth Israel Deaconess Medical Centre in Boston, Massachusetts, USA, from 2008 to 2019. 26 The Institutional Review Board of the Beth Israel Deaconess Medical Center waived informed consent and shared data. Minghao Liang, the primary author, was granted permission to extract data from the database on November 18, 2022 (ID: 11 506 836), after passing the relevant National Institutes of Health review. All clinical information on patients was anonymized, and the study was conducted in accordance with relevant guidelines and regulations. Our study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 27
Study Population
Adult patients diagnosed with sepsis upon admission were included in this study. Sepsis was defined according to the diagnostic criteria of sepsis 3.0: an increase of 2 points in the sequential organ failure assessment (SOFA) score 28 and suspected infection. 1 We only included patients who were admitted for the first time. Patients with multiple admissions and those admitted to the ICU for less than 48 h were excluded. We excluded patients on renal replacement therapy (RRT) and those with end-stage renal disease. Data lacking bicarbonate levels and associated variables were excluded.
Variables
We incorporated demographic and clinical data upon admission. Demographic data included age, gender, ethnicity, and weight. Clinical data comprised vital signs, laboratory tests, scoring systems, comorbidities, and interventions. Vital signs encompassed urine output (UO), heart rate, and saturation of peripheral oxygen (SPO2). Laboratory tests included platelets, white blood cells (WBCs), potassium, sodium, blood urea nitrogen (BUN), hemoglobin, serum creatinine (SCr), and blood glucose. The scoring systems comprised the Charlson comorbidity index (CCI) 29 and the SOFA score. Comorbidities included diabetes mellitus, AKI, myocardial infarction (MI), chronic pulmonary disease, renal disease, and congestive heart failure (CHF). Interventions included the use of ventilators, loop diuretics, and glucocorticoids.
Primary Variables and Outcome Measures
The primary variable studied was bicarbonate level. Bicarbonate was measured at ICU admission. The principal endpoint of this study was 28-day mortality, whereas the secondary outcome was 90-day mortality.
Statistical Analysis
Data were classified into 5 distinct groups based on serum bicarbonate levels, divided into quintiles: Q1 (≤19.0 mEq/L), Q2 (19.0-22.0 mEq/L), Q3 (22.0-24.0 mEq/L), Q4 (24.0-26.0 mEq/L), and Q5 (>26.0 mEq/L). Continuous variables were compared using either one-way ANOVA or the Kruskal–Wallis H test, depending on data distribution. Categorical variables were analyzed with the Chi-square test. To evaluate the relationship between bicarbonate levels and 28-day mortality, we first applied univariate Cox regression. Subsequently, multivariate Cox proportional hazards models were used to assess the association after adjusting for potential confounders. Three separate models were developed: Model 1 adjusted for basic demographic and clinical parameters (sex, age, ethnicity, weight, heart rate, SPO2, and UO); Model 2 included additional clinical variables such as platelets, WBC, glucose, SCr, hemoglobin, sodium, potassium, SOFA score, comorbidities, and organ dysfunction; and Model 3 incorporated the use of interventions like mechanical ventilation, loop diuretics, and glucocorticoids. Three models were established to account for potential confounders based on the results of univariate regression, relevant literature,30,31 and clinical experience. The continuous bicarbonate variable was also tested for a trend effect using the median value of the quintiles. Non-linear relationships were assessed using restricted cubic splines and curve fitting, with inflection points identified through recursive algorithms.To ensure robustness, sensitivity analyses were performed using multiple imputation for missing data, and additional tests were conducted to examine potential confounding factors across different subgroups. Given that the missing values for all data were <5%, missing data were directly deleted. All analyses were performed using R software (version 4.2.2) and Free Statistical software (version 1.9). Statistical significance was set at P < 0.05.
Results
Study Population and Baseline Characteristics
An initial cohort of 23 828 adult sepsis patients was identified from the MIMIC-IV database. After excluding individuals with ICU stays under 48 h, those receiving renal replacement therapy or diagnosed with end-stage renal disease, as well as records missing key bicarbonate measurements or other covariates, 12 744 patients remained for analysis (Figure 1). As shown in Table 1, the mean age of the cohort was 65.0 ± 16.6 years; 57.1% were male and 64.0% were White. During the first ICU day, 78.7% required mechanical ventilation and 8.4% received loop diuretics. When stratified by bicarbonate quintiles, the highest quintile group demonstrated higher platelet counts and lower WBC counts, whereas the lowest bicarbonate group exhibited elevated SCr and BUN levels. Flowchart of Study Patients. Notes: ICU, Intensive Care Unit Analysis of Baseline Characteristics of Serum Bicarbonate Levels Notes: UO, urine output; WBC, white blood cell count; SCr, serum creatinine; BUN, serum urea nitrogen; CCI, Charlson comorbidity index; AKI, acute kidney injury.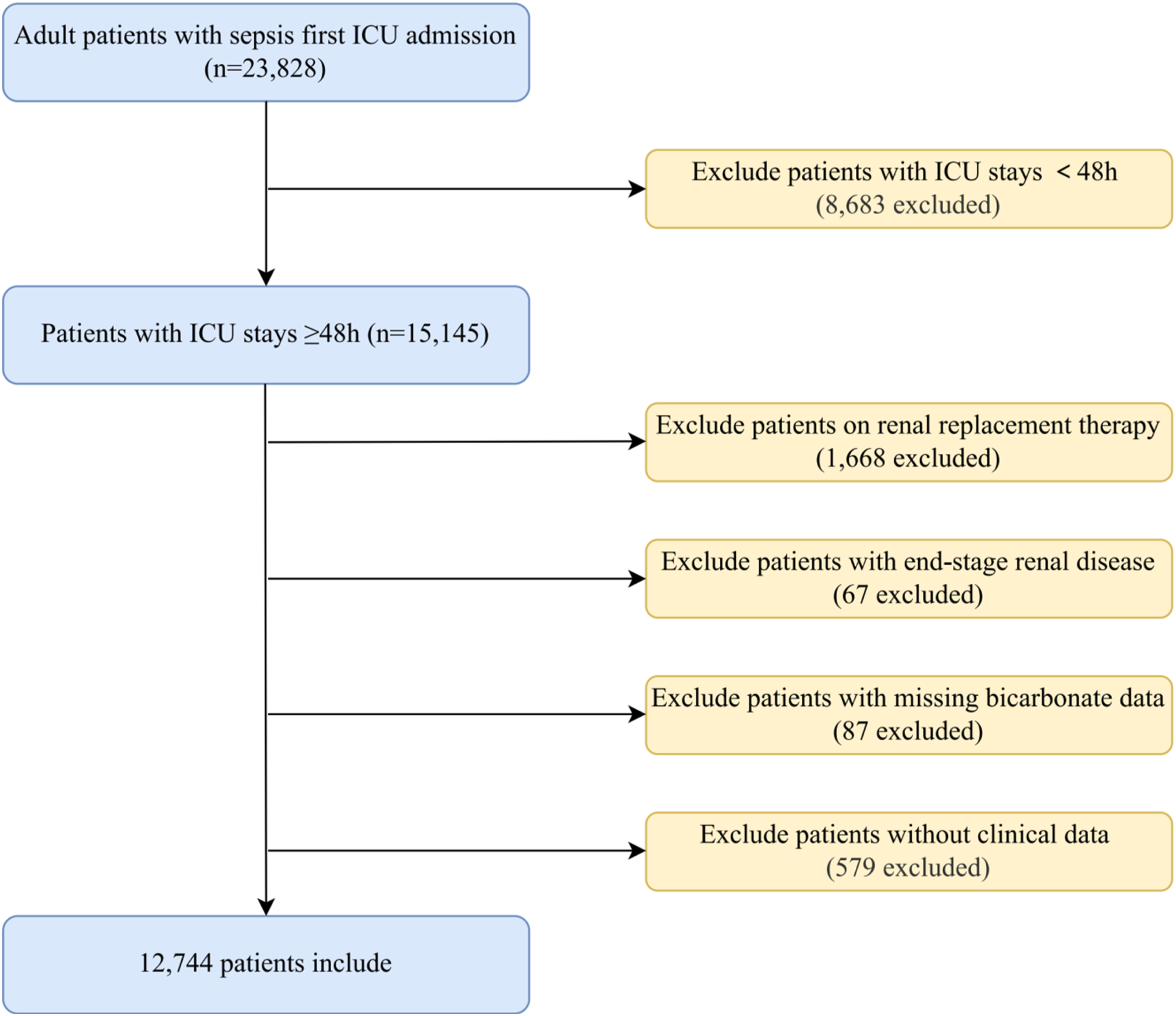

Multivariable Cox Regression Analysis
Association Between Bicarbonate Levels and 28-Day Mortality in Patients With Sepsis

Model 1 adjusted for sex, age, ethnicity, weight, heart rate, SPO2, and UO.
Model 2 adjusted for sex, age, ethnicity, weight, heart rate, SPO2, UO, platelets, WBC, glucose, SCr, hemoglobin, sodium, potassium, SOFA score, diabetes mellitus, AKI, renal disease, chronic pulmonary disease, congestive heart failure, and myocardial infarction.
Model 3 adjusted for sex, age, ethnicity, weight, heart rate, SPO2, UO, platelets, WBC, glucose, SCr, hemoglobin, sodium, potassium, SOFA score, diabetes mellitus, AKI, renal disease, chronic pulmonary disease, congestive heart failure, myocardial infarction, ventilator use, loop diuretic use, and glucocorticoid use.
Notes: HR, hazard ratio; CI, confidence interval; Ref, reference.
Analyses of the U-Shaped Relationship
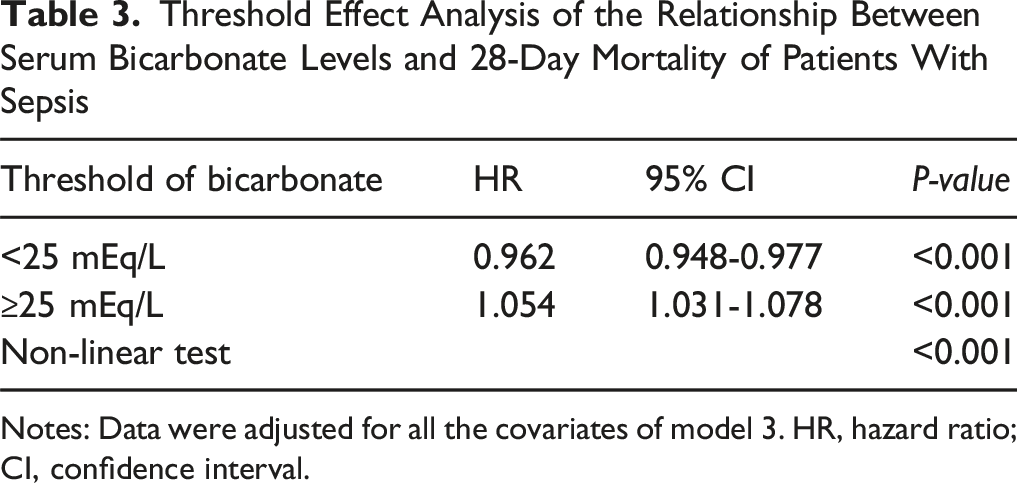
Upon adjusting for covariates in Model 3 (Figure 2), curve fitting revealed a significant U-shaped association between serum bicarbonate levels and 28-day mortality (P for non-linearity <0.01). Specifically, an inflection point was identified at 25.0 mEq/L (Table 3), indicating that below this threshold, each 1 mEq/L increase in bicarbonate was linked to a 3.8% decrease in the 28-day mortality risk (HR: 0.962, 95% CI: 0.948-0.977). However, when bicarbonate levels exceeded 25.0 mEq/L, a 5.4% increase in mortality risk was observed for every 1 mEq/L increase (HR: 1.054, 95% CI: 1.031-1.078). This U-shaped pattern was consistent when examining the relationship between bicarbonate levels and 90-day mortality (Supplemental Figure S1). These findings highlight that both low and high serum bicarbonate levels are associated with higher mortality risks in sepsis patients, with optimal bicarbonate levels around 24.0-26.0 mEq/L. U-Shaped Relationship Between Bicarbonate Levels and 28-Day Mortality Risk. Notes: Adjusted for Covariates in Model 3; Red Solid Line Represents the log2(HR) Value, and the Red Area Represents the 95% CI Threshold Effect Analysis of the Relationship Between Serum Bicarbonate Levels and 28-Day Mortality of Patients With Sepsis Notes: Data were adjusted for all the covariates of model 3. HR, hazard ratio; CI, confidence interval.
Subgroup Analysis
We performed curve fitting stratified by age (≤60 and >60), sex (male and female), race (White and other), CHF (yes and no), chronic lung disease (yes and no), and ventilation use (yes and no) to verify that the U-shaped relationship was consistent across subgroups. The results showed a U-shaped relationship between bicarbonate levels and 28-day mortality in each subgroup, similar to the main analysis (Figure 3). This U-shaped pattern was also observed in the subgroup analyses of the relationship between bicarbonate levels and 90-day mortality (Supplemental Figure S2). Subgroup Analysis of the Association Between 28-Day Mortality and Bicarbonate Levels. Notes: Adjusted for Covariates in Model 3; (A), Age; (B), Sex; (C), Ethnicity; (D), Congestive Heart Failure; (E), Chronic Pulmonary Disease; (F), Ventilation. Red and Blue Lines Represent log2(HR) Values, and Red or Blue Areas Represent 95% CI
Sensitivity Analysis
To address potential biases arising from missing data, sensitivity analyses were performed using multiple imputation methods to account for incomplete covariates. This resulted in a final sample size of 13 323 patients. The association between serum bicarbonate levels and 28-day mortality remained consistent after imputation (Supplemental Table S3), with the lowest (Q1: HR: 1.43, 95% CI: 1.24-1.64) and highest (Q5: HR: 1.30, 95% CI: 1.14-1.49) bicarbonate quintiles showing significantly increased risks compared to the reference group (Q4: 24.0-26.0 mEq/L). Furthermore, the U-shaped relationship was confirmed by curve fitting, demonstrating the robustness of our findings even after accounting for missing data (Supplemental Figure S3). Additionally, we extended the analysis to include non-first-time ICU admissions (n = 4852), which also revealed a consistent U-shaped trend, further validating the generalizability of the results (Supplemental Figure S4).
Discussion
The pathogenesis of sepsis is based on an unregulated systemic inflammatory response that causes severe vascular endothelial damage, microcirculatory abnormalities, and tissue hypoperfusion. 32 Although various biomarkers have been found to predict the probability of death in sepsis, there is still potential for improvement.32,33 Our study identified a U-shaped relationship between serum bicarbonate levels and 28-day mortality in patients with sepsis. For bicarbonate levels below 25.0 mEq/L, each 1 mEq/L increase was associated with a 3.8% decrease in 28-day mortality risk (HR: 0.962, 95% CI: 0.948-0.977). In contrast, when bicarbonate levels exceeded 25.0 mEq/L, every unit increase corresponded to a 5.4% rise in mortality risk (HR: 1.054, 95% CI: 1.031-1.078). Both low and high levels of bicarbonate were linked to a higher risk of mortality, with patients having bicarbonate levels between 24.0-26.0 mEq/L showing the lowest 28-day mortality risk.
Bicarbonate is crucial for maintaining the acid–base balance and has been proven to be closely associated with the prognosis of numerous diseases. Research has revealed that bicarbonate is a strong predictor of mortality risk in patients with trauma and has a stronger predictive ability than lactate and base remaining. 34 In a study with 4674 participants, low bicarbonate levels and decreased bicarbonate levels increased the 30-day risk of mortality in patients with acute ischemic stroke. 30 A prospective cohort study demonstrated that low bicarbonate levels are a major risk factor for the development of AKI and renal insufficiency in critically ill patients, whereas high bicarbonate levels do not have this association. 35 However, a cohort study of patients with AKI showed that low bicarbonate levels increased 14-day mortality and AKI progression in patients compared with normal bicarbonate levels, and high bicarbonate levels mitigated this effect. 36 A U-shaped relationship was found between bicarbonate levels prior to receiving RRT and the risk of all-cause mortality in patients with chronic kidney disease. 37 This result suggested a significant variation across populations in the relationship between bicarbonate levels and prognosis. Our study demonstrated a U-shaped relationship between serum bicarbonate levels and 28-day mortality in patients with sepsis, and high and low bicarbonate levels are associated with a poor prognosis in patients with sepsis.
Low bicarbonate levels are a clear sign of metabolic acidosis, which may aggravate sepsis via the following mechanisms. First, low tissue perfusion and lactate buildup occur. Tissue hypoxia, enhanced anaerobic metabolism, elevated lactate production, and significant bicarbonate consumption are all consequences of impaired microcirculation in sepsis. 38 Second, mitochondrial dysfunction occurs. Acidosis reduces ATP synthesis and exacerbates the cellular energy deficit by blocking the tricarboxylic acid cycle and inhibiting pyruvate dehydrogenase activity. 39 Third, the activation of NLRP3 inflammasomes and increased release of pro-inflammatory cytokines IL-1β and TNF-α during acidosis enhance the inflammatory response.40,41 The relationship between high bicarbonate levels and the risk of mortality can be interpreted in the following ways. First, elevated bicarbonate levels due to medically induced alkali supplementation. Excessive sodium bicarbonate administration in clinical settings for patients with septic acidosis may result in elevated CO2 production, inducing paradoxical intracellular acidosis and superoxide generation, which facilitates apoptosis. 42 Second, the main symptom and diagnostic marker of metabolic alkalosis is typically high bicarbonate levels. Patients with alkalosis frequently present with comorbidities of hypocalcemia 43 and hypokalemia, 17 which adversely affect their prognosis by inducing respiratory depression, muscular weakness, and cardiac arrhythmias. In the state of metabolic alkalosis, the oxygen dissociation curve shifts to the left, causing difficulties in oxygen and hemoglobin dissociation, further exacerbating hypoxemia and contributing to the increased risk of patient mortality. 44 Alongside metabolic alkalosis, respiratory acidosis induces a compensatory increase in bicarbonate levels. In the presence of hypercapnia, as shown in severe asthma and chronic obstructive pulmonary disease, the kidneys compensatorily enhance hydrogen ion excretion and bicarbonate reabsorption, resulting in high bicarbonate levels.45,46
This study had the following advantages. First, we were the first to examine the relationship between serum bicarbonate levels and 28-day mortality in patients with sepsis. Second, our sample size was reasonably large. Third, we identified a U-shaped relationship between bicarbonate levels and mortality risk by using a curve-fitting method. Some limitations must be acknowledged. First, this work is a retrospective study and will inevitably possess some limitations. Despite adjusting for some covariates, residual confounders and the influence of unmeasured confounders will persist. Second, the MIMIC-IV database does not contain detailed records of base supplementation therapy, such as sodium bicarbonate dose and infusion schedule. Nevertheless, this limitation does not hinder our investigation into the relationship between elevated bicarbonate levels and poor prognosis of patients with sepsis. Third, focusing primarily on English-language literature in the literature search could introduce a potential selection bias. Fourth, we must address potential sources of bias, including possible classification bias in sepsis diagnosis, and we will employ our own database for subsequent investigations. Nevertheless, our research into the relationship between serum bicarbonate levels and prognosis in patients with sepsis is noteworthy.
Conclusion
A U-shaped relationship was observed between bicarbonate levels and 28-day mortality in patients with sepsis. Alterations in serum bicarbonate levels, whether decreased or elevated, were correlated with an increased risk of 28-day mortality. Among all the tested levels, bicarbonate levels of 24.0-26.0 mEq/L were associated with the lowest risk of 28-day mortality in patients with sepsis. This finding suggested that clinicians should prioritize monitoring bicarbonate levels in patients with sepsis. Future prospective studies should determine whether maintaining this optimal interval enhances survival.
Supplemental Material
Supplemental Material - The U-Shaped Relationship Between Serum Bicarbonate Levels and 28-Day Mortality in Patients With Sepsis: A Retrospective Cohort Study of MIMIC-IV Database
Supplemental Material for The U-Shaped Relationship Between Serum Bicarbonate Levels and 28-Day Mortality in Patients With Sepsis: A Retrospective Cohort Study of MIMIC-IV Database by Minghao Liang, Feilong Guan, Lili Sun, Wenjing Xi, Hongling Jia, Yifei Xu, Minyan Jin, Xianhai Chen, Di Huang, Zhanjun Qiu in Dose-Response
Footnotes
Author Contributions
ML designed the study and wrote the manuscript. FG and LS executed database management and contributed to data extraction. WX and HJ performed data cleansing and contributed to the statistical analysis. YX and MJ analyzed the results and improved the graphs. XC, DH, and ZQ revised the manuscript and conducted quality control during the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Natural Science Foundation of China (82274320 and 82374379), Qilu Wellness and Health Leading Talent Training Project in 2020 (rc2021002-03), and Shandong Province Natural Science Foundation (ZR2024MH076).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.