
Abstract
Background
Magnesium (Mg) is the second most abundant intracellular cation. Ionized Mg is the only active form of Mg. The concentration of ionized Mg could be a potentially novel biomarker for anxiety and depression.
Aim
The aim of this study was to assess the serum concentration of ionized Mg and its correlation with biomarkers of oxidative stress and inflammation in patients with anxiety and depression.
Methods
In this study included 93 respondents were divided into 3 groups: C (control group—18 respondents); A (patients with anxiety disorder, dissociative/conversion disorders and somatoform disorders—36 patients); D (patients with depression—39 patients). Clinical diagnosis was based on ICD-10 criteria. Blood samples were used for standard laboratory analysis, ionized Mg analysis, oxidative stress, and inflammatory parameters.
Results
Statistical significance was recorded between healthy volunteers and patients (anxiety/depression) in ionized Mg values. In anxious patients, malondialdehyde (MDA) had a positive correlation between the parameters of oxidative stress with ionized Mg. In depressive patients, MDA had a positive correlation, and glutathione peroxidase 1 (GPX1) a negative correlation with the concentration of ionized Mg.
Conclusion
Ionized Mg and its correlation with parameters of oxidative stress could be potential biomarkers in anxious and depressive patients.
Introduction
Magnesium (Mg) is the second most abundant intracellular cation. The mechanism of action of magnesium is noncompetitive antagonism of the N-methyl-D-aspartate (NMDA) receptor ion channel. 1 This cation is involved in numerous enzyme reactions, and in many functions within the central nervous system. 2 Mg is used in the treatment of acute and chronic pain, and as a supplement that helps in the treatment of anxiety, depression, Alzheimer’s and Parkinson’s diseases, epilepsy, and stroke. 2 Recent studies have shown that hypomagnesemia is associated with endothelial dysfunction, deterioration of oxidative stress status and inflammation. 1 Since anxiety and depression are disorders that are mediated by altered glutamatergic neurotransmission, with Mg playing a role in blocking this pathway, a correlation between the level of magnesium and psychiatric symptoms has been proposed.3,4
It is estimated that more than a billion people in the world suffer from mental disorders, with a third of life spent with a disability. 5 Anxiety has a prevalence rate of 15% in the general population. Anxiolytic effects in mice were reported after an increase in Mg concentrations. 6 Mg levels correlate with personal anxiety, indicating that Mg supplementation can relieve symptoms of anxiety in humans. 7
Depression is a common psychiatric disorder, with 40% of cases. 8 The relationship between serum Mg and depression was examined in many studies.9,10 Besides the wide range of different pharmacological agents, Mg supplementation exhibited a potent adjuvant effect in the treatment of depression. 11
Low concentrations of total serum Mg have been established in patients with depression and anxiety and are also associated with higher levels of oxidative stress and inflammation12-14,15. The concentration of ionized Mg, which refers to free magnesium ions, has not been examined in these disorders. Ionized Mg is the only active form of Mg. As there is a correlation between the total serum concentration of Mg and anxiety and depression, defining the level of ionized Mg could contribute to a more precise assessment of the causes of the disorder, more precise diagnostics, earlier recognition, and a more precise therapeutic approach. The concentration of ionized Mg could be a potentially novel biomarker for anxiety and depression.
The aim of this study was to assess the serum concentration of ionized Mg and its correlation with biomarkers of oxidative stress and inflammation in patients with anxiety and depression.
Materials and Methods
Respondents
Our study was designed as a cross-sectional study, conducted in a naturalistic setting. All of the patients were recruited in a subsequent matter when presenting to outpatient services at the Clinic for Psychiatry, University Clinical Centre of Serbia. All of the patients who fulfilled the inclusion criteria, and did not fulfill exclusion criteria and were willing and able to participate in the study were recruited. The study was conducted from September 2020 till December 2021. The study included 93 respondents, of which 75 patients were diagnosed for the first time with anxiety and depression. All experiments were approved by the Ethics Committee of the Clinical Center of Serbia (N°505/15). All patients signed informed consent about taking part in the study.
Respondents (n = 93) were divided into 3 groups as follows: C (control group—18 respondents); A (patients with anxiety disorder, dissociative/conversion disorders and somatoform disorders (F41, F44, and F45)—36 patients); D (patients with depression (F32)—39 patients). Clinical diagnosis was based on ICD-10 criteria. Respondents from the healthy group were examined and did not meet the criteria for depressive and anxiety disorders.
During the first psychiatric examination, respondents were recruited according to their medical history and predefined research parameters: general information, personal and family medical history, sociodemographic characteristics, BMI, and physical activity. Respondents filled out a self-rating questionnaire about the level of stress, anxiety, and depression. At the same time, the psychiatrist evaluated the quality of the symptoms on appropriate scales based on the psychiatric examination. Respondents included in the study met the following criteria: age (between 18 and 65 years), a diagnosis in the anxiety disorder, dissociative/conversion disorders and somatoform disorders and depressive disorders, and healthy volunteers, patients not receiving psychiatric therapy (“drug naive”), capable of understanding the purpose of the research. Exclusion criteria included substance abuse, the presence of neurological or other severe physical and metabolic comorbidities, and the inability to provide informed consent.
Psychiatric Assessment
The following questionnaires were used: (1) Beck’s Depression Inventory (BDI) Questionnaire, scale for assessing depression (validated in Serbia 16 ); (2) Depression and Anxiety Stress Scales (DASS-21)—a questionnaire to assess symptoms of anxiety, depression, and stress-related symptoms; this questionnaire was validated on the population in the Republic of Serbia. 17
Beck’s Depression Inventory
The 21 symptoms and attitudes contained in the BDI reflect the intensity of the depression; items receive a rating of zero to three to reflect their intensity and are summed linearly to create a score which ranges from 0 to 63. The 21 items included reflect a variety of symptoms and attitudes commonly found among clinically depressed individuals (eg, Mood, Self-dislike, Social Withdrawal, Sleep Disturbance). The BDI administration is straightforward, and it can be given as an interview by the clinician or as a self-report instrument. 16
The BDI is interpreted through the use of cut-off scores. Scores from 0 through 9 indicate no or minimal depression; scores from 10 through 18 indicate mild to moderate depression; scores from 19 through 29 indicate moderate to severe depression; and scores from 30 through 63 indicate severe depression.
Depression, Anxiety, and Stress Scale
Depression, Anxiety, and Stress Scale-21 self – questionnaire: This instrument was used to assess the symptoms of anxiety, depression, and stress-related symptoms. Questions 3, 5, 10, 13, 16, 17, and 21 formed the depression subscale DAASD (Depression anxiety stress—depression subscale). The total depression subscale score was divided into normal (0-9), mild depression (10-12), moderate depression (13-20), severe depression (21-27), and extremely severe depression (28-42). Questions 2, 4, 7, 9, 15, 19, and 20 formed the anxiety subscale DAASA (Depression anxiety stress—anxiety subscale). The total anxiety subscale score was divided into normal (0-6), mild anxiety (7-9), moderate anxiety (10-14), severe anxiety (15-19), and extremely severe anxiety (20-42).
Questions 1, 6, 8, 11, 12, 14, and 18 formed the stress subscale DAASS (Depression anxiety stress—stress subscale). The total stress subscale score was divided into normal (0-10), mild stress (11-18), moderate stress (19-26), severe stress (27-34), and extremely severe stress (35-42). The available answers were scored on a Likert-scale (ranging from 0 to 3). This instrument was previously validated on the Serbian population. 17
Blood Samples
In addition to the usual diagnostic procedures and collecting of anamnestic data necessary to diagnose a psychiatric disorder, blood samples were taken for standard laboratory analysis. The blood samples were taken before start of therapy, which was usually prescribed for the appropriate symptoms. Blood was taken for biochemical analyses, as well as the analysis of oxidative stress and inflammation parameters, and the level of ionized Mg concentration.
Measurement of the Level of Ionized Mg
The concentration of ionized Mg was measured by clinical chemistry analysis (in cooperation with the Department of Chemistry, Faculty of Medicine, University of Belgrade). Heparinized vacuum tubes were used for the determination of concentrations of ionized Mg. Four mL of venous blood were taken by the standard anaerobic procedure of venipuncture of the cubital vein. Sample analysis was performed within 6 hours of sampling on an analyzer for clinical chemistry, blood gases (Blood Gas Stat Profile Prime Plus Analyzer, Nova Biomedical Corporation, Waltham, USA). The device is registered in the Agency for Drugs and Medical Devices of Serbia, No. 515-02-01758-18-001 from 11/19/2018.
Measurement of the Oxidative Stress and Inflammatory Parameters
The concentrations of interleukin 6 (IL-6), glutathione peroxidase 1 (GPX1), superoxide dismutase 1 (SOD1), malondialdehyde (MDA), and tumor necrosis factor alpha (TNF-α) in the serum of investigated respondents were determined by coated enzyme-linked immunosorbent assay (ELISA) kits, according to the manufacturer’s instructions (Elabscience, Wuhan, China); the ELISA kits for determination of concentrations of IL-6 and TNF-α are based on the Sandwich ELISA principle, with plates pre-coated with an antibody specific to human cytokines. The optical density (OD) was measured spectrophotometrically at 450 nm, using a Multiskan EX plate reader (Thermo Fisher Scientific, Vantaa, Finland). The concentration of analytesin the tested samples was calculated by comparing the OD of the samples to the standard curve created with GraphPad Prism 9.0 software (GraphPad Software Inc., San Diego, CA, USA).
Standard laboratory analyses that included complete blood count and biochemical analyses (cholesterol, triglycerides, aspartate aminotransferase (AST), alanine aminotransferase (ALT), gamma-glutamyltransferase (GGT), urea, creatinine, glucose, sedimentation (SE), C-reactive protein (CRP), thyroid status, ionized calcium, cortisol, and prolactin) were performed in the biochemical laboratory of the Clinical Center of Serbia.
Statistics
Depending on the type of variables and the normality of the distribution, results were presented as frequency (percentage), median (range), and mean±standard deviation. Statistical hypotheses were tested using ANOVA and the Kruskal–Wallis test. The correlation between the variables was estimated using Spearman’s correlation coefficient. Statistical hypotheses were analyzed at the level of significance of .05. Statistical data analysis was performed using IBM SPSS Statistics 22 (IBM Corporation, Armonk, NY, USA).
Results
Sociodemographic Characteristics
The study included 93 respondents: 75 patients and 18 healthy volunteers. Average age of our respondents were in the C group—42.5 ± 7.7, A—39.5 ± 9.5, and D—49.5 ± 11.8. There was statistical significance as regards age between depressive patients and the anxiety/healthy volunteers (P < .01). Depressive patients were older than those with anxiety or healthy volunteers.
Sociodemographic Characteristics.

Abbreviation: BMI, body mass index.
Systemic Inflammation and Oxidative Stress Parameters in Anxiety/Depressive Patients
Comparison Between Groups Regarding the Parameters of Inflammation, Oxidative Stress, Stress Hormones (Prolactin and Cortisol).

Abbreviations: PLR, platelet/lymphocytes; NLR, neutrophils/lymphocytes; MLR, monocytes/lymphocytes; DNLR, neutrophils/WBC-lymphocytes; RPR, red blood cell distribution width (RDW) to platelet ratio; SII, PLT x neutrophils/lymphocytes; PAR, platelet/albumin; CRP, C-reactive protein; GPX1, interleukin 6 (IL-6), glutathione peroxidase 1; SOD1, superoxide dismutase 1; MDA, malondialdehyde; TNF-α, tumor necrosis factor alfa.
Statistical analysis was by the Kruskal–Wallis test; multiple comparisons were not performed because the overall test did not show significant differences across samples.
The hormone prolactin displayed a statistically significant difference among groups C, A, and D (P < .005) (Kruskal–Wallis test), and was statistically different between groups C and D (P < .05) (pairwise comparisons, Bonferroni correction). Cortisol did not differ between the groups (P > .005).
Ionized Mg and Ca in Anxious/Depressive Patients
Correlation Between Mg/Ca Concentration. The Relationship Between Ionized Mg and Ca and the Total Concentration of Mg Throughout the Groups.

Abbreviations: Mg, magnesium; iMg, ionized magnesium; Ca, calcium; iCa, ionized calcium.
Statistical evaluation: ANOVA; multiple comparison; the mean difference was significant at the .05 level.
Correlation Between Ionized Magnesium Concentration and BDI/DAAS Scale
Correlation Between Mg and Ca with Scores of the BDI and DAAS Scales.
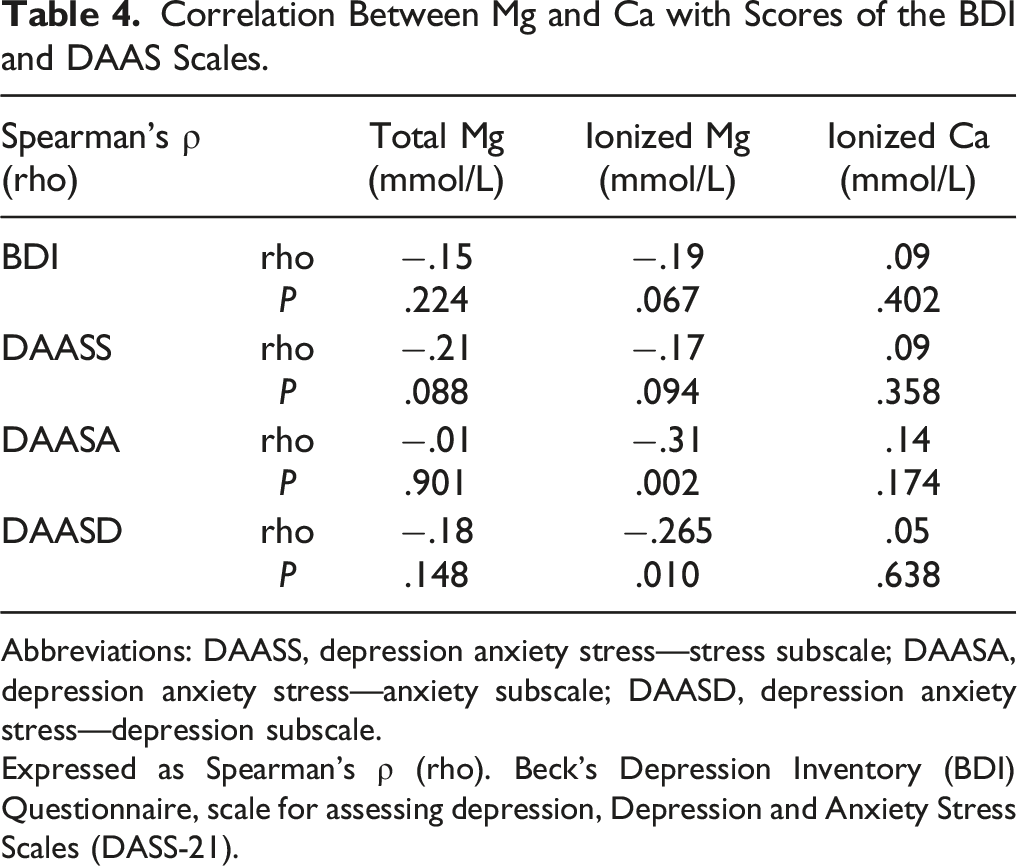
Abbreviations: DAASS, depression anxiety stress—stress subscale; DAASA, depression anxiety stress—anxiety subscale; DAASD, depression anxiety stress—depression subscale.
Expressed as Spearman’s ρ (rho). Beck’s Depression Inventory (BDI) Questionnaire, scale for assessing depression, Depression and Anxiety Stress Scales (DASS-21).
Ionized Mg and the Parameters of Inflammation and Oxidative Stress
Correlation Between Ionized Mg and the Parameters of Oxidative Stress (GPX, SOD1, MDA) and Inflammation (IL-6 and TNF-α) in Healthy Volunteers and Patients.

Abbreviations: GPX1, glutathione peroxidase 1; SOD1, superoxide dismutase 1; MDA, malondialdehyde; IL-6, interleukin 6; TNF-α, tumor necrosis factor alfa.
Expressed as Spearman’s ρ (rho); correlation is significant at the .01 level (2-tailed).
Discussion
For the first time, our study revealed that the correlation observed between ionized Mg and the parameters of oxidative stress could be a potential biomarker in anxious and depressive patients.
The ionized fraction of magnesium is a physiologically active form of magnesium. Changes in serum protein concentration may affect the total concentration of magnesium without necessarily affecting the ionized fraction or the status of total magnesium in the body. Reliable serum ionized magnesium concentrations can only be obtained by direct measurement and not by calculation from total serum magnesium and albumin. 18 There are numerous studies in which the connection between depression and hypomagnesemia was examined.19,20 Patients with an Mg deficit have depressive symptoms (78.6%).21,22 Differences between the Mg concentration in healthy volunteers and depressive patients have been shown. 23 To date, most studies did not correlate the severity of depression with the concentration of Mg. In the present study, the total concentration of serum Mg in depressive patients was in the normal range and did not differ that in from healthy volunteers. However, ionized Mg was lower in depressive patients in comparison with the control group. Ionized Mg has not been examined so far as described herein, using a special apparatus for measuring its ionized fraction. In our study, the lower concentration of ionized Mg correlated with higher scores on the depression scales. For the first time, besides measuring ionized Mg, we established a dose–response relationship between ionized Mg and higher scores on the depression scale about severity of depression.
Some studies examining anxious patients and Mg concentrations. 24 It was showed that increased levels of Mg contribute to increased synaptic plasticity in regions of the brain, which can lead to a decrease in the memory of fear. Studies have reported the correlation between low levels of Mg and symptoms of anxiety.25-27 In one study however, hypomagnesemia in patients was not linked with general anxiety. 26 In a systematic review, supplementation with Mg did not relieve the symptoms of mild anxiety. 7
The inconsistent results regarding the level and function of Mg in patients with anxiety, depression and affective disorders could be the result of differences in the methodology and used techniques. Ionized Mg as a novel parameter could be more precise and a potential biomarker of some of these disorders. In our study, the total serum concentration of Mg in anxious patients was in the normal range and did not differ in comparison to healthy volunteers. In contrast, ionized Mg was lower in anxious patients in comparison with the control group. The lower concentration of ionized Mg correlated with higher scores on the anxiety scales.
In our study, the total and ionized Mg did not differ between depressive and anxious patients. There was a difference between the concentration of ionized Mg and depressive/anxious patients in comparison with healthy controls, but none between anxious and depressive patients. So, we can conclude that the measurement of ionized magnesium is more precise than total serum Mg level. This is probably because anxiety and depression belong to the same specter of disorders. According to the proposed hypothesis of pathophysiology involving Mg, Spasov et al. 28 concluded that magnesium is important for the function of serotonergic, dopaminergic, and cholinergic systems in rats, and also that hypomagnesemia influences disturbances in these systems. Our results are in correlation with these results.
Mg concentration is directly related to Ca. Ca also has important functions in enzyme systems. 29 In our study, we measured the concentrations of ionized Ca that did not differ in anxious and depressive patients when compared with the control group.
All sociodemographic parameters were similar in the three examined groups. There was only a statistical significance between the age of patients in the depressive group in comparison with the other groups. The average age of depressive patients was higher than that of the other groups. Epidemiological studies indicate that anxiety disorders tend to present earlier in life (third and fourth decade), while a diagnosis of a first major depressive episode has a much broader range of presentation—from adolescence to old age. As such, it is not unusual for patients with major depressive disorder in our study to be slightly older. Moreover, since this was a cross-sectional, naturalistic study conducted in real-life clinical circumstances, our primary concern was to gather the data from patients as they presented.
The serum concentration of Mg is not influenced by either sex or age, except in very old patients, which was not the case in our study. 30 We conclude that hypomagnesemia is correlated with affective disorders, but not with age.
In our study, there were more females than males in each group. Groups had the same gender distribution and did not differ statistically. As regards gender and based on previous research, affective disorders are more likely to manifest in women, which can be explained by hormonal differences. Hormones in women exhibit much higher and more cyclic oscillations than in men, which is reflected on the prefrontal cortex and hippocampus and is responsible for mood swings, with estrogen playing a role in neutralizing stress-free glucocorticoids, and declining estrogen levels with age in women can contribute to depression. 31 Mg deficiency is often associated with a high BMI, metabolic diseases, and diabetes.32-34 The BMI in our subjects had normal values, which excluded the potential impact of malnutrition or obesity on the values of Mg. Also, somatic diseases could influence Mg concentration. Stress is one of the possible causes of disturbed Mg concentration. Stress itself leads to increased release of catecholamines and corticosteroids. On the other hand, low levels of Mg/Ca increase the secretion of catecholamines, and high levels of catecholamines further reduce the concentration of Mg in the body, becoming a vicious circle. 35 There are genetic differences in sensitivity to Mg deficiency as differences in the body’s responses to stress. 36 In our examination, the cortisol levels were not significantly elevated in the study groups. The level of prolactin as an indicator of stress showed a statistically significant difference in depressed patients in comparison to healthy controls.
Increased oxidative stress is a physiological part of the aging.37-39 Thus far, none of the existing biomarkers of oxidative stress was highly specific for depression and anxiety. 40 The formation of reactive oxygen species (ROS) is the product of cellular metabolism, affecting the function of cell membrane lipids, proteins and nucleic acids, and increased ROS levels underlie many pathological processes. The role of Mg in oxidative stress is referred to in numerous studies, but the precise mechanism of its action has not been determined.
Both oxidative stress and Mg deficiency increase the concentration of ROS, which in turn leads to the development of damage to cells, tissues, organ dysfunction, and the development of inflammation and disease (eg, diseases of the CNS). A link between oxidative stress and reduced Mg intake has not been established. 41 Cernik et al 42 found a correlation between the levels of Mg, plasma superoxide anion, and MDA in persons exposed to chronic emotional stress. Mg deficiency is accompanied by a 2-fold reduction in reduced glutathione (GSH) in erythrocytes as a consequence of increased glutathione transferase activity. 43 Animal studies have shown links between a reduction in Mg, increased MDA, and a decrease in antioxidant markers. 44 Another study in mice showed that a deficiency of Mg leads to decreased activity of glutathione reductase and S-transferase, but that the activity of glutathione peroxidase was not significantly altered. 45 Mg deficiency resulted in the accumulation of MDA and decreased concentration of GSH. 46 In our study, a statistically significant difference in the level of GPX between the control group and anxious/depressive patients was observed. Anxious and depressive patients did not exhibit a significant difference in the concentration of GPX. MDA and SOD1 showed significant differences among the groups. Also, in our study there was a negative correlation between ionized Mg and the level of GPX in depressive patients. Thus, in our depressive patients the lower levels of Mg correlated with higher concentrations of GPX. In the patients, MDA had a positive correlation with the concentration of ionized Mg. Even MDA did not exhibit a significant difference among groups, the enzyme correlated with ionized Mg in anxious and depressive patients. In our study, we observed a correlation between ionized Mg and the parameters of oxidative stress (GPX and MDA); however, these parameters should be examined on a larger population.
Neuroinflammation influences the development of affective disorders. Neuroinflammation and cytokines affect the regulation of neurotransmitters in the CNS, neurogenesis and maintenance of neuroplasticity and all these mechanisms affect the development of affective disorders. 47 The systemic parameters of inflammation such as the mean platelet volume (MPV), platelet distribution width (PDW), plateletcrit (PCT), systemic immune-inflammation index (SII), platelet to lymphocyte ratio (PLR), platelet to albumin ratio (PAR), and red blood cell distribution width (RDW) to platelet ratio (RPR) have roles in major depressive disorder (MDD). 48 In our study, we did not observe significance between these parameters and the examined groups, probably because of the sample size.
According to King, 49 inflammation with increased C-reactive protein (CRP) is the result of reduced Mg. None of the examined parameters of inflammation (CRP, TNF-α, IL-6, the systemic parameters of inflammation) differed among our groups. As the study was performed during the COVID-19 pandemic, patients were isolated and used supplements. Probably, because of this, the patients had not increased levels of inflammatory parameters in our study. IL-6 and TNF-α did not correlate with the concentration of ionized Mg in our study. Strengths of this study are: for the first time, it was measured ionized magnesium in anxious/depressive patients (in drug naïve patients); significant correlation between ionized magnesium and parameters of oxidative stress; and potential biomarkers in these diseases. Limitations of our study are small sample; larger number of patients are required to support our conclusion; and period of examination (pandemia of COVID-19 prolonged examination, smaller number of patients visited doctors).
Conclusion
Ionized Mg and its correlation with parameters of oxidative stress could be potential biomarkers in anxious (Mg-MDA) and depressive (Mg-MDA; Mg-GPX1) patients. However, as this is a pilot study, further studies with a larger number of patients are required to support our conclusion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Education, Science and Technological Development of Serbia (Grant 175023).