
Abstract
Fears over radiation have created irrational pressures to dissuade radiography use within chiropractic. Recently, the regulatory body for chiropractors practicing in British Columbia, Canada, the College of Chiropractors of British Columbia (CCBC), contracted Pierre Côté to review the clinical use of X-rays within the chiropractic profession. A “rapid review” was performed and published quickly and included only 9 papers, the most recent dating from 2005; they concluded, “Given the inherent risks of radiation, we recommend that chiropractors do not use radiographs for the routine and repeat evaluation of the structure and function of the spine.” The CCBC then launched an immediate review of the use of X-rays by chiropractors in their jurisdiction. Member and public opinion were gathered but not presented to their members. On February 4, 2021, the College announced amendments to their Professional Conduct Handbook that revoked X-ray rights for routine/repeat assessment and management of patients with spine disorders. Here, we highlight current and historical evidence that substantiates that X-rays are not a public health threat. We also point out critical and insurmountable flaws in the single paper used to support irrational and unscientific policy that discriminates against chiropractors who practice certain forms of evidence-based X-ray-guided methods.
Introduction
Radiographic analysis is not only the first choice in imaging of the spine in all forms of clinical healthcare practice but it is the gold standard for the examination of patients presenting with spinal disorders.1-10 In this context, X-rays can provide critical and immediate information to guide treatment decisions regarding further imaging (e.g., MRI), referral (e.g., surgical consult), indications for co-management (rheumatologist and pain specialist), to rule out or confirm a definitive diagnosis, help provide a timely diagnosis, ease the anxiety of the patient, and satisfy the doctors liability concerns.11-13 In the current era of value-based healthcare, 14 routine initial X-ray screening is, in fact, encouraged as it reduces costs associated with more advanced imaging (i.e., CT and MRI). 15 Last, the evaluation of biomechanical relationships of the spine and pelvis have direct consequences on patient pain, disability, quality of life, and spinal function, and patient outcomes can be altered with evidence-based spine rehabilitation procedures utilized by many manual therapists including doctors of chiropractic.4,8,9,12,13
Within the profession of chiropractic, there has been recent controversy over X-ray use in clinical practice. For example, in 2017, the American Chiropractic Association (ACA) released a statement that it had joined the Choosing Wisely initiative and listed 5 practices that were discouraged. 16 The first two points were associated with X-ray use: specifically, (1) to not X-ray a patient presenting with acute low back pain within the first 6 weeks of onset, and (2) to not X-ray a patient to assess response to treatment. Despite the fact that the ACA’s listed items are not supported by any valid or discipline-specific evidence,17,18 the promoted discouragement of X-ray use through the Choosing Wisely program has led to far-reaching and cascading consequences including the use of this list by insurance companies to deny reimbursement to practicing chiropractors using X-rays to diagnose and assess their patients.17,18
Further examples of controversy over X-ray use in chiropractic include a debate between affiliates of Chiropractic Biophysics NonProfit and Anderson, Kawchuk and members of the Research Council of the World Federation of Chiropractic.19-21 The “scoping review” by Jenkins et al 22 for X-ray use in chiropractic that was heavily criticized, 13 as well as most recently, a controversial “rapid review” on X-ray utility in chiropractic concluding there was no evidence for routine or repeat X-ray imaging in chiropractic practice beyond suspected “red flags” (i.e., serious medical conditions including cancer, infection, fracture, etc.). 23 This last review attempted to assess the chiropractic literature from the inception of multiple databases to November 2019, but only included 9 papers in their final analysis and none dated from the last 15 years! 23
It is precisely this last article mentioned that underpins recent events regarding the College of Chiropractors of British Columbia (CCBC) to make sweeping policy changes to restrict chiropractors from taking X-rays practicing within the jurisdiction of the Province of British Columbia (BC), Canada. Legal adoption of this CCBC policy change would mean BC chiropractors have lost their full X-ray rights for use for treatment assessment and evaluation of spine disorders unless used strictly for the purpose of examining “red flags” only. 24 So-called “red flag only” guidelines for the chiropractic profession have been heavily criticized as they rely virtually exclusively on data from allopathic medical practice (pharmacologic practice), they ignore the plethora of spine literature correlating spine alignment with health outcomes, they ignore the high-quality and evolving evidence for approaches validating spine-altering methods, they ignore studies showing high rates of bony anomalies/pathologies that may alter treatment approach, and they discriminate against chiropractors that practice alternative forms of evidence-based practice that utilize initial and repeat spine X-rays.13,25
This article addresses the peculiar events that have rapidly occurred which seem to be motivated by misguided opinion and political policy over science. First, we highlight recent reviews substantiating diagnostic X-rays as harmless to public health as well as historical evidence about the pseudo-science surrounding the adoption of the linear no-threshold (LNT) model that underpins all radiation risk assessment. We discuss the many criticisms of BEIR VII that is proclaimed to be the primordial LNT support document as well as low-dose radiation as an effective treatment for human diseases. Next, we discuss critical and insurmountable flaws in the contracted “rapid” review 23 invalidating the CCBCs X-ray policy changes. We point out the complete lack of transparency of the CCBC and highlight the Colleges’ failure to perform its role of “protecting the public” by speedily adopting unscientific and unethical policy based on a single flawed manuscript. Finally, we discuss how radiophobia has escalated and culminated into poor policy that neglects consideration of the bulk of existing science.
X-Rays Are Not a Public Health Threat
The first and foremost criterion that precludes definitive action toward dissuading, or in this case radical policy change to outright revoke, full X-ray rights is having belief in the conjecture that “X-rays cause cancer.” Today, this notion is understood to be false. For all intents and purposes, low-dose radiation in the amounts given from X-rays (and CT scans) offers no threat to public health as they have never been shown to cause harm and in fact, have only been shown to enhance health (aka radiation hormesis26-28). Here, we briefly summarize the main findings from several recent studies, we show that the traditional events and science leading to the adoption and acceptance of the LNT model was based on pseudo-science, we present the multiple fundamental flaws which invalidate the use of the US National Academy of Sciences Biological Effects of Ionizing Radiation report (BEIR VII) for use in radiation risk assessment from X-rays, and discuss low-dose radiation as a successful treatment for human diseases.
Contemporary Reviews Show No Harm from Low-Dose Radiation/X-rays
Schultz et al performed a quantitative assessment on the methodologic quality of studies that had evaluated cancer risk from low-dose sources (i.e., X-ray and gamma radiation exposures less than 200 mSv) to determine the evidentiary strength supporting or refuting a causal relationship between low-dose radiation and cancer. 29 The authors state that concerns exist that medical radiation from X-rays (CT scans) will cause thousands of malignancies, and that if this premise is false, the fears from patients and doctors leading to X-ray avoidance would be unfounded.
In their analysis, from an initial 4382 located studies between the years 1975–2017, 62 met all the inclusion/exclusion criteria. From these, 25 studies were deemed to be of high-quality, and importantly, 21/25 did not support cancer induction by low-dose radiation (p = .0003). Thus, fears from X-rays were determined to be unfounded; indeed, the authors stated
29
: A clear preponderance of articles with higher quality methods found no increased risk of cancer from low-dose radiation. The evidence suggests that exposure to multiple CT scans and other sources of low-dose radiation with a cumulative dose up to 100 mSv (approximately 10 scans), and possibly as high as 200 mSv (approximately 20 scans), does not increase cancer risk. (p. 3)
Vaiserman et al performed a recent literature review to assess the validity of the LNT model of radiation damage, the basis of current regulation. 30 They reviewed medical occupational exposures including radiologists and technologists, radiation workers, nuclear workers, nuclear weapons test participants, radiation-based medical procedure participants who received diagnostic imaging and low-dose radiotherapy, environmental background radiation, residential radon exposure, and nuclear powerplant accidents including exposures given to residents exposed from the incidents at Three-Mile Island (1979), Chernobyl (1986), and Fukushima (2011).31-39 They also included the comprehensive reviews from the joint report of the French Academy of Sciences and French Academy of Medicine (2005), 40 BEIR VII (2006), 41 and the United Nations Scientific Committee on Atomic Radiation (UNSCEAR) report (2016). 42
Overall Cancer Mortality in Cohorts Occupationally Exposed to Radiation (Adapted from Vaiserman 30 ).
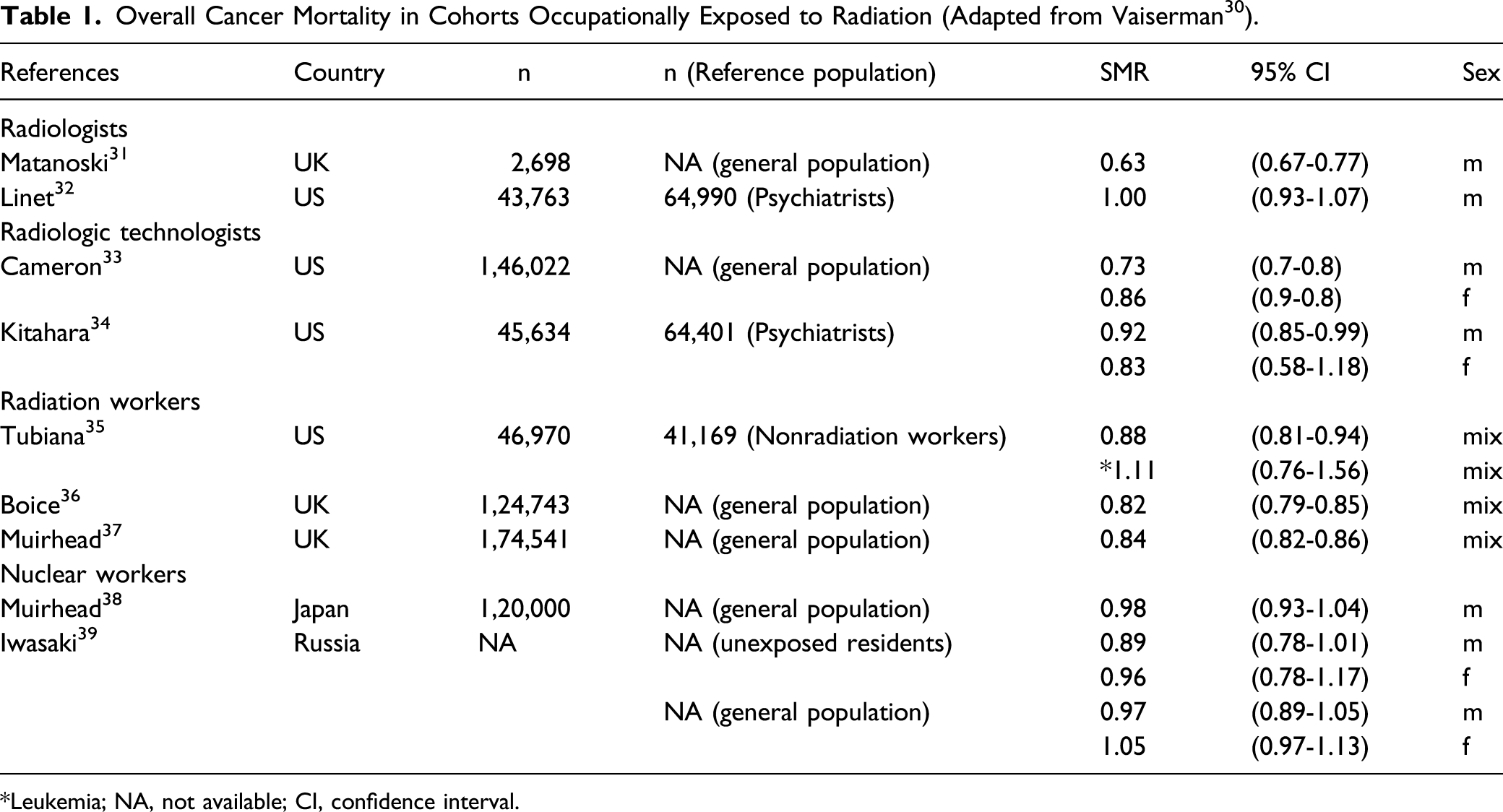
*Leukemia; NA, not available; CI, confidence interval.
Synopsis of the Failure of the ALARA Radiation Protection Principle. 43

In another recent review, it was summarized why the long-held notion of X-ray carcinogenicity is not a valid argument. 56 It was shown the LNT is not valid for low-dose radiation exposures (including X-rays) as the Life Span Study (LSS) data, which is considered the main evidential support, shows a hormetic dose-response curve (non-linear)57,58; the BEIR VII has been heavily criticized for having both faulty assumptions and analyses.59-62 The original adoption of the LNT was based on faulty data and dubious agenda,63-68 and that the LNT has evolved to become more political than scientific.69,70 It was argued that the ALARA concept is obsolete as it relies on the invalid LNT model. 56 It was also illustrated that exposure levels shown to be carcinogenic have thresholds that are very high, for example, from the data presented from Doss (700 mGy)57,58 as well as Cuttler (1100 mGy). 71 This last argument is of critical importance as it illustrates that X-ray exposures represent an infinitesimal fraction of the threshold for potential cancer induction. Cuttler also noted that, even in those exposed to above 1100 mGy from the atomic bomb, only .5% developed leukemia which he noted was “very surprising.” 71
Oakley and Harrison 56 also argue that low-dose ionizing radiation (LDIR) upregulates the adaptive protection systems of the body that repair any damage done by X-rays,72-75 and that an X-ray would only equate to about one-millionth of the endogenous damage from breathing air on a daily basis. Also, LDIR treatments are based on the physiological response of the body and have been used to treat a variety of human ailments including inflammatory and neurodegenerative conditions, infections, and cancers.75-77 It was argued the total collective dose (TCD) concept is invalid for LDIR due to the adaptive response mechanisms, as any DNA damage resulting from each exposure event (X-ray) would be mitigated prior to any subsequent exposure. It was also discussed that aged cohort studies purveying radiogenic cancers from prior X-rays are not generalizable to the wider population due to cohorts who were imaged in their youth having increased incidence of anomalies and other predisposing factors and, thus, increased susceptibilities to cancers.78,79
It has recently been pointed out that the Radiation Effects Research Foundation (RERF) has recently been incorporating non-radiation factors into consideration for cancer incidence in the LSS cohort survivor data which has led to obvious suspicions about the merit of previous studies published by RERF that did not previously account for other such risk factors. 80 Indeed, cancer is understood to be a multifactorial disease process. In assessing two recent RERF studies (Sakata et al 81 ; Grant et al 82 ), Pennington found the LSS cohort input data and modeling had “extensive deficiencies and defects” and that “a best estimate of radiation-only cancers within the LSS cohort’s large population using current cancer risk factors for the Japanese population offers a strong indication that A-bomb-blast LDIR could not produce such cancers.” 80 He also questioned how the RERF “continues to find and assert that bomb-blast LDIR remains a distinguishable source of radiogenic cancer” when it was concluded that the “LDIR radiogenic cancer model is highly implausible if not improbable.” 80
A recent review by Ricci and Tharmalingam investigated the validity of LNT interpolations from high-dose atomic bomb data to the use for risk assessment at low-dose levels. 83 Noting that LNT cancer risk modeling generally excludes co-exposures to chemicals, dietary, and socio-economic cancer risk factors, LNT radiation modeling always and incorrectly predicts cancers as solely attributed to ionizing radiation exposures. They point out that for the linear interpolation to be correct, there would have to be exact similar biological mechanisms that lead to cancer from high and low doses of radiation; however, this cannot be correct as both biological and epidemiological data show non-linearity and thresholds. They also show that the use of the LNT suffers from misspecification errors, multiple testing, and other biases and “its use by regulatory agencies conflates vague assertions of scientific causation, by conjecturing the LNT, for administrative ease of use.” 83
Recently, a task group was organized by the Society of Nuclear Medicine and Molecular Imaging to assess the validity of the LNT, its use in risk assessment and radiation protection, and the risk of cancers from low-dose radiation exposures. 84 The task group concluded “the evidence does not support the use of LNT either for risk assessment or radiation protection in the low-dose and dose-rate region” and that it is “actually refuted by published epidemiology and radiation biology.” 84 They found the LNT was not supported by any evidence for use in the low-dose and dose-rate region.
Pseudo-Science led to the Adoption of the LNT Model
The assessment of all radiation risks is through application of the LNT model. Soon after its first adoption in 1956, all the major regulatory agencies (e.g., NAS BEIR, National Council on Radiation and Protection [NCRP], and International Commission on Radiological Protection [ICRP]) used the LNT as the foundation for risk assessment from radiation exposures. The LNT implies that all radiation is harmful and also cumulative; in fact, it asserts that no radiation is without risk. 58 The LNT model is a simple model of linear extrapolation from data at high radiation exposures down to the zero dose. As will be explained, this model seems to be more about politics than science.69,70 Despite the exponential emergence of data against the legitimacy for the use of LNT for low-dose exposures such as from X-rays and CT scans, these agencies continue to endorse the LNT.
Surprisingly, there have been new revelations about the dubious origins of the LNT.63-68 The origins of the LNT model have recently been shown to have been surrounded by actions of scientific fraud and misconduct.63-68 The linearity concept without a threshold for mutation induction by radiation exposure came from Hermann J. Muller’s original fruit fly experiments and the historic 1927 publication in Science. 85 Muller produced transgenerational phenotypical changes using very high radiation doses. He claimed they were gene mutations, though decades later these were shown to be gene deletions and other chromosomal rearrangements. 67 Thus, at that time, the radiation research genetics field was misdirected for decades based on Muller’s false claims of producing gene mutations. It is also noted that his 1927 Science publication presented no data and was not peer reviewed. 64 It appears he avoided peer review to claim primacy for discovering gene mutation that did lead him to receive the Nobel Prize for physiology or medicine in 1946 for “the discovery of the production of mutations by means of X-ray irradiation.” 86
Calabrese revealed historical documentation that legitimate scientific evidence that directly opposed Muller’s LNT theory work was deliberately suppressed by the Nobel Laureate on his way to winning the 1946 Nobel Prize. 68 Muller who gave his Nobel Prize Lecture on December 12, 1946, knew of high-quality data from a study by Casperi and Stern 87 using low-dose radiation exposure that clearly showed a threshold and refuted the low-dose linearity concept that Muller endorsed. After Muller was asked for feedback, documented in a letter back to Stern dated November 12, 1946 (1 month prior to his Nobel lecture), Muller indicated “he received the manuscript, scanned through the entire document, saw its significance, knew that the findings were refuting the low-dose linearity concept, that the study was done by Caspari, whom he viewed as a very competent person, so he couldn’t challenge the findings.” 68 Regardless, in his Nobel lecture Muller stated that there was “no escape from the conclusion that there is no threshold.” 68
In 1957, extending on the work from Muller, Lewis published an important paper in Science generalizing the linear relationship from germ cells to somatic cells applying it to cancer. 88 This inspired the NCRP in 1960 to adopt the LNT for cancer risk assessment. As Calabrese explains, “It was this sequence of events that propelled the LNT cancer risk assessment model into the public health arena, transforming the fields of environmental health, food safety, radiation health, and occupational health.” 63 At this point, like dominos, “many other national advisory committees did copycat acceptances, and linearity became a done deal. The tide was turned. It was a paradigm shift within a very short time period.” 68 To this day, the international and national radiation advisory agencies continue to endorse the LNT model for risk assessment.
Prior to the paradigm shift to the LNT model, there was a threshold model for which many argue that the early radiologist data 89 shows that the first recommended dose limit of 0.2 R per day (approximately 70 rad or 700 mGy per year) adopted by the ICRP in 1934 represents a safe dose limit that should be re-adopted. 33 Cardarelli and Ulsh argue that abandonment of the LNT model for low-dose radiation risk assessment by incorporating contemporary science into the regulatory processes could succeed to ensure that science would underpin decision making, that the public be educated on the lack of risks from low-dose radiation exposures, and to “harmonize government policies with the rest of the radiation scientific community.” 90
BEIR VII Is Continually Endorsed as Primordial LNT Proof Despite Having Critical Flaws
LNT advocates always rely on the BEIR VII as the pinnacle of scientific consensus or proof of legitimacy of the linearity single hit theory that underpins all radiation risk assessment. Here, we discuss the many criticisms of BEIR VII that invalidate its use for risk assessment from X-rays.
Sutou recently summarized 5 main flaws of the BEIR report that relies heavily on the LSS data. 62 First, the dose-response curve of leukemia is linear quadratic (i.e., non-linear), but because there was no statistical difference between a linear and linear-quadratic model, the BEIR committee adopted the linear model. As Sutou states, “this forced logic is unacceptable.” 62 Second, the highest dose in the BEIR reports (Figure 4) is 2 Gy, but excess relative risk (ERR) typically shows a downward turn of exposures greater than 2 Gy since individuals highly exposed would die prior to any cancer development. Therefore, “concealing a downturn by limiting doses up to 2 Gy… is successful in giving the impression of linearity.” 62 Third, the BEIR committee performed a statistical trick by combining all data points less than 100 mGy into 1 point, which again, conceals evidence of non-linearity. Fourth, the BEIR committee assumed a zero-exposure in the not-in-the-city (NIC) controls of the LSS data; however, they were also exposed to residual radiation from black rain occurring for a few hours, 45 minutes after the detonation over Hiroshima. 62 Sutou shows that a re-analysis accounting for the NIC exposures shows a threshold and hormetic dose response (i.e., non-linearity). Fifth, the BEIR report ignores the adaptive protection mechanisms “acquired through the evolution processes of billions of years” 62 that innately attempt to mitigate DNA damage.72-75 Sutou concludes “LNT based on LSS is invalid… Indeed, A-bomb survivors live longer and get cancer less frequently… It is high time to admit beneficial effects of radiation hormesis and to establish a new paradigm for LDR [low-dose radiation] regulation.” 62
Siegel et al point to the limited literature included in the BEIR VII report, particularly the reliance on use of in vitro data that do not support the LNT. Importantly, they point to the fact that in vitro data cannot be used as proof of carcinogenesis for intact organisms. 61 Siegel et al shows the BEIR report acknowledges epidemiological data linking cancer induction from low-dose radiation exposures is lacking, but then places major emphasis on a single study by Lloyd et al. 91 This study is a collaborative effort from 6 laboratories that counted chromosomal alterations (dicentric chromosomes) in human lymphocytes induced in vitro resulting from radiation exposures in the range of 0–300 mGy. First, it is interesting that the BEIR report omitted the zero-dose data point that showed a value of 0.17 dicentrics per 100 cells. Importantly, Lloyd et al found the dicentrics per 100 cells to be .11, .12, and .11 for exposures of 3, 6, and 10 mGy. 91 This damage rate is less than the zero-dose control and unequivocally demonstrates non-linearity (hormesis).
Even at the higher exposure doses of 20, 30, and 50 mGy, they remain relatively plateaued at 0.19, 0.24, and 0.24 dicentrics per 100 cells. Only the 300 mGy, the highest exposure dose in the study showed significantly increased damage at 1.28 dicentrics per cell. 91 Siegel et al state “Linearity at the low doses does not exist (in this case 2-50 mGy and likely beyond, somewhere between 50 and 300 mGy); rather, it is forced by the high-dose extrapolation of the LNT model.” 53 Although the BEIR report claims that “a linear relationship between low-linear energy transfer dose and chromosomal mutation down to around 20 mGy” exists, 41 Seigel et al points out that the Lloyd et al data do not support this statement. Further, and most importantly, “BEIR’s assertion that the link between initiation and clinical cancer had been ‘established’ is unsupportable” as “Such studies (in vitro studies) can only suggest mechanisms of cancer initiation; they cannot by themselves provide evidence of clinical cancer development in whole organisms.” 61 Siegel et al call for the establishment of a new BEIR VIII committee to “critically reassess the validity, and use, of LNT and its derived policies.” 61
In another BEIR critique, Doss reminds us that the recent updates to the LSS by Ozasa et al, 92 and Grant et al, 82 show non-linearity and therefore, “the main epidemiological evidence quoted in the BEIR VII report no longer supports the LNT model.” 60 Doss also states that although many commonly argue that because innate repair mechanisms are less than perfect, a threshold is not plausible (e.g., Duncan et al 93 ); however, when one considers the large amount of endogenous DNA damage, low-dose radiation would result in upregulation of the adaptive repair mechanisms so that overall, there would be less DNA damage. Thus, there would in fact be a reduced overall DNA damage and mutations as has been observed in mice. 94 Doss states “even though DNA repair mechanism is imperfect, there would be reduction of overall DNA damage after low radiation exposures.” 60
In a detailed analysis, Calabrese and O’Connor demonstrate more critical flaws in the BEIR VII report. 59 They note that some BEIR reports have disagreed with other BEIR reports, noting that “lifetime excess cancer risks” increased an order of magnitude from BEIR III to the BEIR V. This was from the committee choosing to switch from using a linear-quadratic risk model to a linear risk model (e.g., 42 vs 660 cancer deaths projected from an exposure of 100 mGy between the different reports). BEIR VII uses a combination of the 2 risk models. Regarding this changing of risk model use, Calabrese and O’Connor state “While the underlying scientific data reviewed by these committees had obviously been updated, there was and is nothing in the published literature indicating that the risks from ionizing radiation are an order of magnitude greater than previously thought.” 59
It is known that the BEIR committee examined data from many sources, but often data showing hormesis or threshold were excluded. For example, environmental studies show that residents living in unusually high background radiation exposures, those near nuclear reactor plants and those exposed to fallout from nuclear accidents (apart from increased thyroid cancers) show no evidence of increased cancers. The BEIR committee considered these types of studies to be of little use due to being “descriptive in nature” and “ecological in design.” 59 Occupationally exposed workers involving nuclear powerplant workers (Cardis et al 95 ) initially showed an increased mortality risk for all cancers except leukemia; however, excluding invalid data involving one Canadian test site showed no increased cancer risk but, in fact, also showed an overall decreased risk of both all causes and cancers for nuclear workers versus expected. 96 The BEIR report does acknowledge this trend but attributes it to the “healthy worker effect” and “unknown differences” between nuclear workers and general public and excludes the data for “not being suitable.” 59
The BEIR VII report almost completely relies on the data from the LSS cohort, and in doing so, they create risk models for calculating the risks of cancer. It is noted that an ERR model and an “excess absolute risk” (EAR) model was used by BEIR but resulted in great incongruence between the two. The “lifetime attributable risk” (LAR) model which is the difference in the rate of a condition between an exposed to unexposed population is used to estimate the probability of developing a premature cancer over a lifetime while accounting for the age of exposure, latency period, and the dose and dose rate effectiveness factor. It is pointed out that when the LAR is based on ERR versus EAR, significantly different risk estimates arise, even differing by a factor of 10. 59 Calabrese and O’Connor argue that ideally all estimates should be identical and be within 1-2 standard deviations of each other—but the BEIR estimates are not. Further, the BEIR committee assigned weighting factors, and it is pointed out that the weighted mean risk coefficient factor from the included data was 0.05/Gy 59 ; however, “the BEIR VII Committee chose a value of ERR = 0.86/Gy, which is 17 times larger than the weighted mean from all nine medical studies” (that the report included). 59 Notably, the BEIR report 41 itself even states “because of the various sources of uncertainty it is important to regard specific estimates of LAR with a healthy skepticism…” (p. 278).
One final critique worthy of mention by Calabrese and O’Connor 59 was the use of the dose and dose rate effectiveness factor (DDREF). This is a factor built into the BEIR estimation of radiation risks that modifies or reduces the dose-risk relationship as estimated by the model to specifically account for the level of dose/dose rate for which the radiation dose was exposed to a population. Importantly, the BEIR committee assigned a value of 2 for the DDREF; however, as Calabrese and O’Connor state “use of any value of the DDREF greater than 1 essentially converts the LNT into a linear-quadratic or biphasic model, and provides a means of modifying the linear model without officially abandoning the LNT hypothesis.” In the end, Calabrese and O’Connor conclude: “Collectively, the uncertainties in the derivation of the BEIR VII risk estimates, and the intrinsic speculative nature of the risk estimates themselves, cause predictions of cancers and cancer deaths to be more hypothetical than real in populations exposed to medical imaging.” 59
Low-Dose Ionizing Radiation Is an Effective Treatment for Human Illnesses

There has been a recent re-emergence of interest for LDIR treatment for human disease as seen in recent case reports and a pilot trial.114-119 In fact, there is much hope for LDIR therapy to prove effective for conditions that have no successful treatment approach such as for Alzheimer’s disease.
119
It must be stated that although the mechanisms for the therapeutic benefits of LDIR are not fully elucidated, it is understood that LDIR upregulates the innate adaptive protection systems (Figure 1).72-74 Generally, any initial damage caused by radiation exposures will be prevented, repaired and/or removed by very efficient biological systems that results in a net decrease in DNA damage; an increase in health benefit. Thus, knowledge of the innate adaptive protection systems and how they can be stimulated to treat disease at radiation doses far above those from spine X-rays should serve as enough evidence to abandon the notion of low-dose carcinogenicity fears from X-rays. The adaptive response systems very efficiently prevent, repair, or remove virtually all DNA alterations.
74

As discussed, the underpinnings of all X-ray restriction stem from the traditional notion of carcinogenesis of low-dose radiation exposures that does not exist. Thus, if the fundamental carcinogenesis conjecture surrounding X-ray utilization is eliminated, what is left to be of concern for the taking of innocuous X-rays? Next, we overview the great deficiencies of the recent review paper contracted to Côté (Corso et al 23 ).
Methodological Deficiencies Invalidate the Contracted Côté Paper
Here, we point out critical and insurmountable flaws in the single paper by Corso et al 23 used to support the irrational, unscientific policy change by the CCBC that discriminates against chiropractors that practice alternative forms of evidence-based practice that utilize initial and repeat X-rays for the analysis and treatment of spinal disorders outside of the exclusive use for screening for “red flags.”
Rationale for Review
Aside from the radiation fear from X-rays as discussed, the rationale for this review is unfounded. In the introduction, Corso et al 23 cite Mizrahi et al 120 to argue that the rate of X-ray use by “chiropractors and podiatrists increased by 14.4% between 2003 and 2015.” 23 They go on to state: “this occurred despite the publication of several evidence-based clinical practice guidelines and clinical prediction rules to assist chiropractors in determining the indication for spine radiographs to assist with diagnosing a pathology.” 23 For this statement, they readily show their bias by not even considering X-ray use for biomechanical assessment and reference five citations,121-125 problematically 3 of the 5 citations were published after 2015121-123—a “time-machine oversight.” 126 Of the 2 citations prior to 2015,124,125 one was exclusively for cervical spine trauma. 125 The only citation that supports Corso’s rationale is the 2008 Bussieres et al radiographic guidelines, 124 though these have been criticized as being recycled allopathic medical care guidelines (i.e., for the practice of general medicine)17,18,25 that are declared to be modeled after the UK Royal College of Radiologists “Referral guidelines for imaging” 127 (i.e., red flag guidelines) where one of the stated purposes of the “chiropractic guideline” is for use in the hospital emergency room (i.e., medical practice). 124 The Bussieres guideline has been heavily criticized for not including chiropractic-specific X-ray uses17,18,25 (e.g., screening for anomalies and/or pathologies that alter manipulative techniques) or for biomechanical analysis which is indeed the universally accepted standard for investigating the integrity of the spine structure and function throughout the spine care literature.1-10,12,13,25,128-135
X-ray based Chiropractic Technique Systems. 136

Abbreviations: NUCCA, National Upper Cervical Chiropractic Association; SONAR, Spinal Orthopedic Neurological Advancement and Research.
In several recent publications, evidence-based X-ray-guided treatment by chiropractors and other manual therapists have been summarized.4,8,9,12,13,17,21,25,137-139 It needs to be noted that the evidence-base for the manual therapy sciences in general is lacking, 140 and that chiropractors use a broad and diverse range of patient treatments, whether specifically studied by chiropractors or other healthcare specialties (This is important to note as we discuss later, the Corso paper inclusion criteria only included studies where treatment was exclusively “done by chiropractors” which automatically excluded 100s of otherwise eligible studies). In brief, for spine radiographic assessment and outcomes, there exists the highest quality evidence (RCTs) for methods shown to decrease forward head posture,141-149 increase cervical lordosis,141,142,144–151 decrease thoracic hyperkyphosis,152-160 increase lumbar lordosis,137,161-163 and decrease/stabilize scoliosis deformities.164-168 It is noted that although some of the RCTs assessing thoracic hyperkyphosis used surface contour instead of imaging, imaging is the most appropriate method to assess the exact type or cause of kyphosis (fracture, postural, senile, congenital, Scheuermann’s, etc.) as well as the segmental location of any deformity. Furthermore, regarding these spine displacements with RCT evidence, chiropractors are intimately trained in the evaluation of these, are intimately trained in these specific treatment protocols and interventions used, and chiropractors are legally licensed in the clinical application of these protocols and practices.
There are also multiple non-randomized clinical control trials (nRCTs) and hundreds of case reports/series showing X-ray-guided chiropractic treatment leads to positive patient outcomes. 169 Several recent case reports/series document the improvement in several different spine displacement patterns (i.e., spinal deformities/subluxation patterns170-175) that are only precisely diagnosed and quantified by radiography including reduction of anterior whole-spine sagittal balance,176,177 reduction of cervical pseudo-scoliosis,178-180 reduction of lumbar pseudo-scoliosis,181,182 improving thoracic hypokyphosis (straight back syndrome),183-185 reduction of thoracolumbar kyphosis, 186 correcting lumbar kyphosis (flat back syndrome), 187 reduction of lumbar hyperlordosis and pelvic tilt, 188 reduction of cervical spondylolisthesis,189,190 and reduction of lumbar spondylolisthesis.191-193
As illustrated, even prior to critically debunking the Corso review, it can be seen that the rationale for inquiry is based on misplaced bias. There is an underlying assumption that X-ray-guided chiropractic techniques and practices are not “evidence-based” methods and that the chiropractors who do utilize radiography outside of allopathic “red flag” use are practicing negligence and are a public health threat. As will be illustrated, this is farthest from reality.
Selection of “Rapid Review”
The contracted review (Corso et al 23 ) was initially registered with the PROSPERO (International prospective register of systematic reviews) on November 12, 2019, and the “start date” was listed as November 4, 2019. 194 In its filing under the section “Type and method of review,” it was listed as a “systematic review” (SR). The completed manuscript was submitted to the journal Chiropractic & Manual Therapies on March 31, 2020, accepted on May 24, 2020, and published online on July 9, 2020. 23
According to the PROSPERO website, planned prospective reviews may be considered prospective until the point of data extraction from included studies. This means that most of the work on the Corso manuscript occurred over the course of less than 5 months. Considering the average SR takes 6 months to 2 years for completion, 195 this project was performed remarkably quick. Also noted is that despite being registered as an “SR,” the final published review was actually a “rapid review” (RR). According to Tricco et al, a RR is “a form of knowledge synthesis in which components of the systematic review process are simplified or omitted to produce information in a timely manner.” 196 For such an established aspect of clinical practice (taking X-rays), it is questioned why a RR was performed and not a standard SR (which was officially registered but not actually performed). What was the urgency to evaluate a common practice that has existed for decades and specifically been practiced without public health concern for 87 years in BC, Canada? 197 As mentioned previously, at least 23 chiropractic technique systems and many other rehabilitation practices are X-ray-guided. 136
In a review of RR methods, 50 different methodological approaches were identified. 196 In other words, RRs are abstruse as there is no consensus to their make-up. Interestingly, the main unifying theme of RRs is that they are performed with significant and purposeful methodological “shortcuts” as compared to the standard SR. 196 In actuality, a RR allows the investigator to introduce bias by electing which procedures to eliminate in order to expediate the process. The methods naturally become vulnerable to vast criticism for being “shotty” or “suspect” depending on the intent of the study. Because no universal definition for RR methodology exists 195 (i.e., remains underdeveloped), many experts question their validity.198,199
As we will show with the Corso study, 23 the inferences from this RR are as what all RRs are understood to be; that is, “their scope is limited.” 199 In fact, RRs should be read with a cautious interpretation of findings as there are “gaps in transparency and knowledge about the trustworthiness of rapid reviews.” 195 Indeed, RRs have been found to be incongruent with standard SRs. 196 We question what time-sensitive demand could have made the authors choose a RR on the utilization of X-ray by chiropractors in British Columbia, Canada, that again, we note, has been competently practiced without prior public health concern for 87 years?
Inappropriate Referencing of WHO Guidelines
Corso et al cite the World Health Organization’s overview of RR uses. 200 According to this report, “Policy-makers require valid evidence to support time-sensitive decisions regarding the coverage, quality, efficiency and equity of health systems” and that “There is also a need for capacity strengthening in low- and middle-income countries in the field of evidence synthesis and rapid reviews more specifically.” Thus, it seems the purpose of a RR as described by the WHO appears to be in situations where a “time-sensitive” matter is at hand and/or when decisions need to be made by low- and middle-income countries (where a proper systematic review of the literature may not be feasible) for which Canada is definitively not.
The WHO document is also specifically designed for a “new” diagnostic test, but X-rays are the gold standard for evaluation of spinal disorders and have been used for this purpose for over 100 years! According to the WHO report, a SR would be a standard necessary to properly assess healthcare policy; therefore, as stated in the WHO report: “generally accepted standards for study selection, data abstraction, and quality assessment for systematic reviews” is to “use two or more reviewers, working independently, to screen and select studies.” The lead author (Corso) was responsible to identify and screen all eligible articles. 23 The authors validated the quality of screening by this single author by randomly screening only ten percent of all eligible articles by a second investigator. The decision to use only one reviewer (Corso) introduced potential bias in the study design and goes against the recommendations made by the WHO. 200
Eliminating Valid Studies If Not “Performed by Chiropractor”
One of the most condemning flaws of the Corso et al review is the inclusion criteria being “studies of patients presenting to chiropractors who received spinal radiographs of the cervical, thoracic or lumbar spine region, in the absence of red flags.” Knowing that literature of the manual therapy sciences is lacking 140 and that in particular, chiropractic specific literature is limited, 201 setting this inclusion criteria to be strictly studies “done by chiropractors” automatically excludes hundreds if not thousands of otherwise relevant studies where the interventions are part of a practicing chiropractors legally licensed armamentarium!
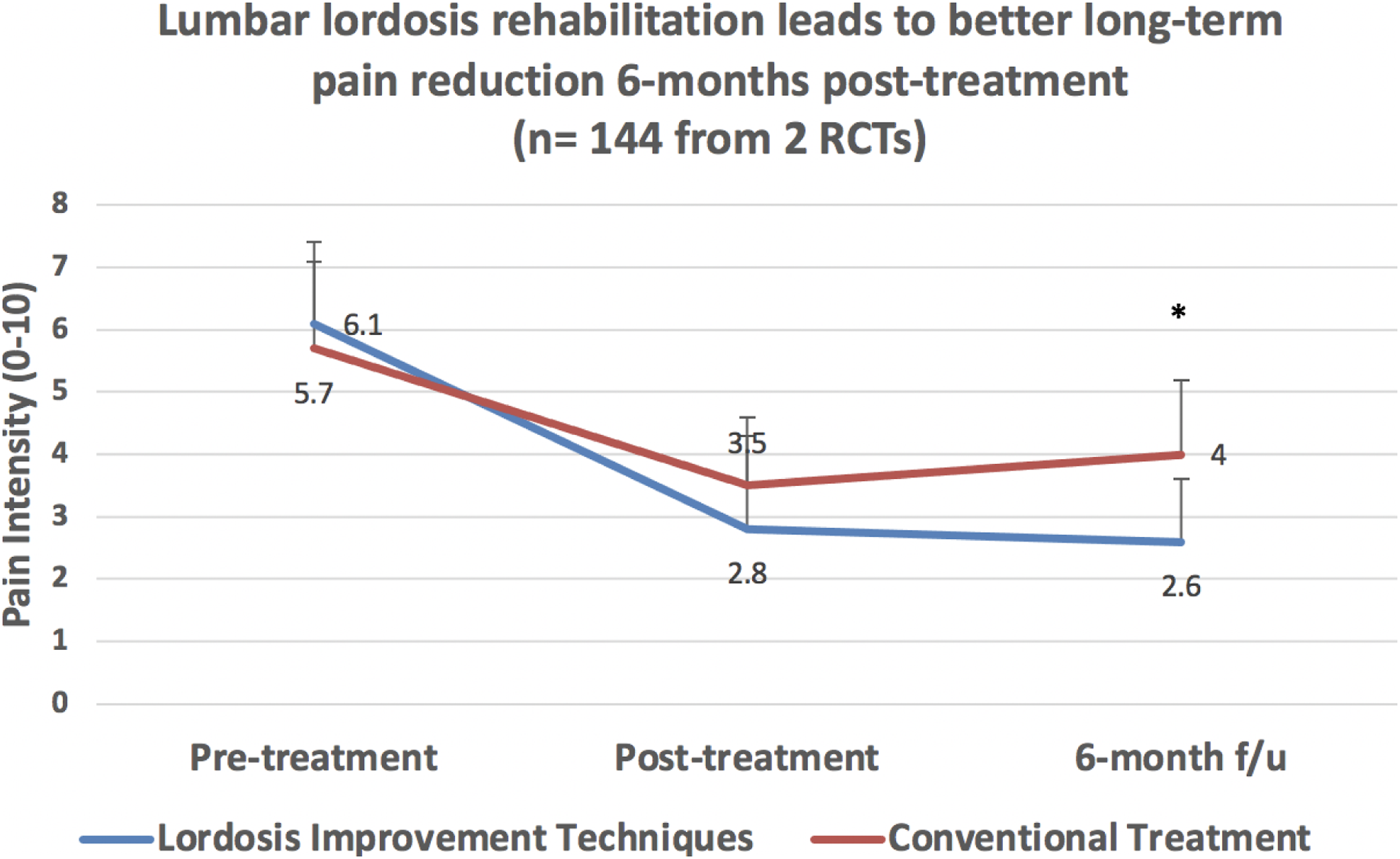
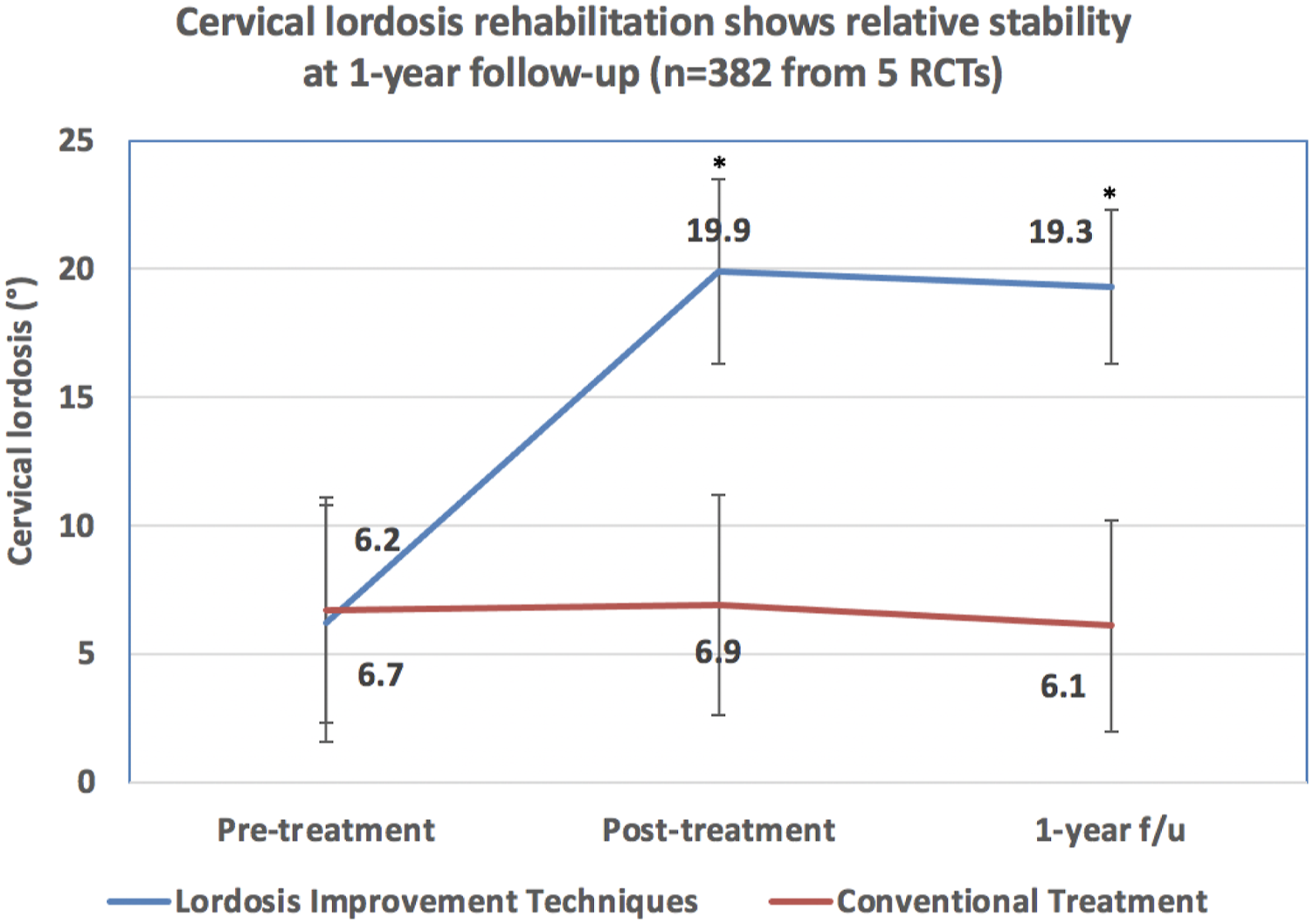
An illustration of the tragic flaw of strictly requiring “chiropractic patients” involves the exclusion of multiple recent RCTs from the Chiropractic BioPhysics (CBP) and related groups,141-150,161-163 which, of course, represents the highest level of scientific evidence. Several high-quality RCTs show that X-ray-guided structural rehabilitation procedures (which were invented by and are routinely practiced by a significant faction of chiropractors) definitively leads to improvement of spine alignment as measured from X-rays and most importantly, superior long-term patient outcomes (Figures 2-5).4,137-139,141-150,161-163,202 The inclusion of even one of these RCTs would have reversed the conclusion of the review; in fact, these RCTs alone refute their findings of no clinical utility of X-rays as the RCT is level 1 evidence versus the Corso et al
23
rapid review (i.e., deficient review) which we believe, should be considered level 5 evidence equivalent to expert opinion. Data from 2 RCTs demonstrates patients receiving lumbar extension traction as well as conventional treatments have lordosis improvements that are sustained for 6 months after stopping treatment versus the lumbar curve in comparative groups (controls) remain unaffected by conventoinal treatments (weighted averages from 2 RCTs161,162). *Indicates a significant group difference as specified in each of the 2 trials; brackets represent weighted standard deviation. Data from 2 RCTs demonstrate patients achieving lumbar lordosis improvement (via extension traction) as well as conventional treatments have pain reductions that are sustained for 6 months after stopping treatment versus comparative groups (controls not achieving lordosis improvement) who show a regression (increase) of pain intensity toward baseline after stopping treatment (weighted averages from 2 RCTs161,162). *Indicates a significant group difference as specified in each of the 2 trials; brackets represent weighted standard deviation. Data from 5 RCTs demonstrates patients receiving cervical extension traction as well as conventional treatments have lordosis improvements that are sustained for 1 year after stopping treatment versus the cervical curve of comparative groups (controls) remain unaffected by conventional treatments (weighted averages from 5 RCTs141,142,144,147,149). *Indicates a significant group difference as specified in each of the 5 trials; brackets represent weighted standard deviation. Data from 5 RCTs demonstrate patients achieving cervical lordosis improvement (via extension traction) as well as conventional treatments have pain reductions that are sustained for 1 year after stopping treatment versus comparative groups (controls not achieving lordosis improvement) who show a regression (increase) of pain intensity toward baseline after stopping treatment (weighted averages from 5 RCTs142-144,147,149). *Indicates a significant group difference as specified in each of the 5 trials; brackets represent weighted standard deviation.

Missed and Excluded Reliability Studies
Of the 8 total studies included in their review pertaining to the reliability of X-rays, 6 of the 8 were from the CBP chiropractic group.203-208 Surprisingly, Corso et al missed 8 other papers on reliability/repeatability of X-ray mensuration procedures also published by the CBP authors.209-216 Further, although they included a chiropractic clinical outcome study by Plaugher, et al 217 on the Gonstead analysis system, they missed a reliability study on same system for the pelvis by the same author 218 as well as they missed the study by Burk, again on the same Gonstead analysis system. 219
Surprisingly, a 1997 study published in Spine by Côté et al, the co-author contracted to perform the manuscript in question, found, “Measuring the magnitude of the sagittal curve from C2 to C7 had excellent interexaminer agreement, with an intraclass correlation coefficient of 0.96 (95% confidence interval, 0.88-0.98) and an interexaminer error of 8.3 degrees.” 220 Oddly, this study was not included by Corso et al. 23
Additionally, we found 12 other articles that included analysis of reliability of X-ray mensuration procedures, published by chiropractors and missed by Corso et al.221-232 This makes 23 missed papers, that should have been included according to their own inclusion criteria that limited papers to being published by chiropractors. This is very concerning considering these are more papers than they included in their review. 23 We believe these citations alone would have altered their findings regarding reliability/validity of X-ray mensuration analysis.
Many more studies (we reference >130 here) were excluded merely because the reliability study was published by non-chiropractors, although the mensuration analyses are taught in chiropractic school and used by chiropractors on a daily basis (e.g., Cobb method for scoliosis analysis), and published in chiropractic radiography guidelines.170,233-370
Missed and Excluded Clinical Outcome Studies
Only 9 total papers were included in their rapid review; 7 of these papers were investigations on CBP chiropractic technique methods.203-208,371 Additionally, it is unbelievable that the most recent of these included papers was published in 2005 and no studies were included in the evaluation of X-ray utility for the entire chiropractic profession from the last 15 years! 23 An inquiry to the CBP NonProfit website lists over 150 papers published since 2005. 372 This includes spinal modeling studies, the sum of which has been described in recent publications.138,171 The CBP research group has modeled the normal human spine where the cervical curve is a portion of a circle and the thoracic and lumbar spinal curves are portions of ellipses that meet at the thoracolumbar junction at their straightest sections. Importantly, the Harrison normal spinal model has been validated in multiple ways. Simple analysis of alignment data on samples of the normal, asymptomatic population has been done.373-380 Comparison studies between normal samples to symptomatic samples,371,375,380 as well as between normal samples to theoretical ideal models have been done.373,374,376-379 Two studies even showed that pain patients and asymptomatic persons can be successfully identified by discriminant statistical analysis based on spine alignment parameters; that is, the presence of cervical or lumbar hypolordosis375,380 which is consistent with systematic literature reviews and meta-analysis findings from the current literature.7,381,382 These modeling papers373-380 are important for the profession and add great weight to the clinical utility of radiography use in chiropractic and the manual therapies.
Regarding CBP literature, there were also 4 clinical trials “done by chiropractors” also missed by Corso.178,181,383,384 Most importantly, and as mentioned, there were 7 RCTs also not included (excluded by strict inclusion criteria) by Corso.143-145,147,149,150,161-163 The results of these trials demonstrate that patients who receive spine traction methods (invented by chiropractors) based on radiographic measurements (Posterior tangent method invented by Don Harrison, DC) as a part of spine rehabilitation programs show statistically better long-term improvement in pain, disability, and other functional outcomes as well as spinal kinematics and other physiological measures at long-term follow-up with improvement in radiographically measured spine alignment. The RCTs met all the inclusion criteria of the authors, except that the care was provided at a physiotherapy department by physiotherapists despite the fact that many of the trials were co-designed and co-authored by a chiropractor.143-145,147,150
Non-surgical management of spinal deformities (e.g., scoliosis and thoracic hyperkyhosis) are also within the scope of practice of Doctors of Chiropractic. Three studies were missed by Corso et al that were conducted by chiropractors in chiropractic settings and published in “chiropractic” journals for treatment of scoliosis.385-387 The bulk of research on the conservative approach to the management of scoliosis/hyperkyphosis has been performed by and published from other disciplines (Physical Medicine and Rehabilitation, Physical Therapy and Physiotherapy).152-160,164-168 These studies report on treatment methods commonly used in chiropractic practice, including exercises and the provision of thoracolumbosacral orthoses (TLSOs). Results across these disciplines show that scoliosis specific exercises with and without bracing is effective in the management of scoliosis,164-168,388-409 as well as the sagittal spine deformity of thoracic hyperkyphosis.152-160,410,411
Failure to Include Upper Cervical, Full-Spine, Pelvis, and Leg Length Inequality
Chiropractors have utilized unique X-ray views of the joints of the spine and pelvis for over 100 years, including upper cervical specific views, full-spine views, pelvic views, and views specific for evaluation of leg length inequality (LLI) (e.g., femoral head view or modified Risser-Ferguson view). All these chiropractic specific views and their analyses are presented in the ICA X-ray guidelines. 170 Importantly, the Corso et al review did not consider these unique X-ray views or their treatment by chiropractors as their search strategy only included the terms “cervical,” “thoracic,” and “lumbar” spine. 23
It is widely known that many specialty chiropractic techniques utilize upper cervical X-ray views including Atlas Orthogonality (AO), Blair, Grostic, NUCCA, Kale, Toggle recoil, and others (Table 4). Dedicated upper cervical chiropractic X-ray views are unique to chiropractic are not typically performed within allopathic medicine, and these include the anterior-posterior (AP) open mouth, nasium, vertex, base posterior, and Blair protracto views.170,412 Regarding these views, there are both reliability studies224,225,227,228,230,232 and clinical outcome studies.224,413-424 Again, these studies should have been included by Corso et al. 23
Regarding full spine X-ray analysis, many technique systems in chiropractic utilize the AP or posterior-anterior (PA) full spine radiographic view routinely such as Gonstead technique. This is also the standard radiographic view throughout all healthcare for the analysis of scoliosis. Regarding the lateral full-spine radiograph, it is well known that the full spine view is the standard for biomechanical assessment1-3,130-132,170,171 and much information can be gained such as:
170
A global view of the sagittal balance of C1, T1, T12, and S1; An evaluation of forward/backward head translation; An evaluation of forward/backward ribcage posture; An evaluation of sagittal posture (from the postural examination) and spinal coupling on the radiograph; An evaluation of cervical lordosis; An evaluation of thoracic kyphosis; An evaluation of lumbar lordosis; An evaluation of pelvic tilt; An evaluation of pelvic morphology; An evaluation of any retro- or spondylolisthesis; An evaluation of spinal degeneration (vertebrae, discs, and spinal ligaments); Spinal canal dimensions; and A number of other anomalies, fractures, and instabilities.
The pelvic X-ray view is a popular view for some chiropractic approaches including the Gonstead system. 218 Many pelvic and sacral listings (i.e., thrust vector trajectories) can be determined as well as insight into pelvic anomalies and pathologies that may alter treatment approaches. Radiographic screening for suspected LLI is also a common practice by chiropractors. An LLI can induce full-spine postural adaptations425,426 and be implicated in the pathogenesis of spinal disorders.427,428 Again, there are reliability studies on radiographically measuring LLI252,262,280,324,328,329,345,354,366 and outcome studies on use of shoe lifts for treatment of LLI.252,261,269,272,275,297,304 These should have been considered by Corso et al. 23
Failure to Include Studies on Anomalies/Pathologies that Alter Manipulative Treatment
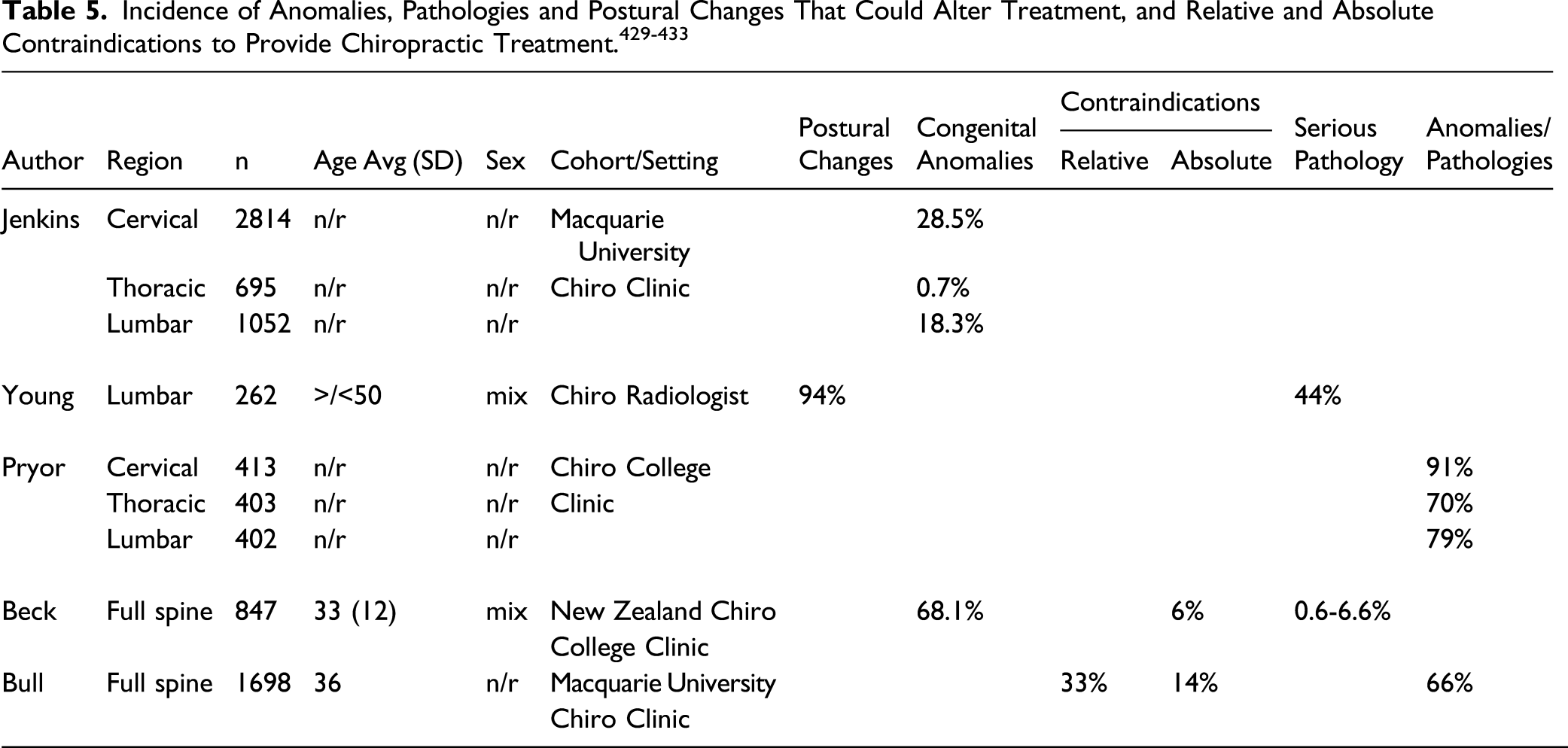
In other studies, it was determined that in a population of almost 11,000 so-called “healthy” air force recruits, 97% had pathological findings. 434 Another study determined that the average number of radiographic anomalies, degenerative changes, and deviations of posture was 3.5 per screened person. 435 This latter study was performed on healthy air force candidates, and the authors stated “Since the population is highly selected, the figures we present may be minimum numbers in a western industrialized society.” 435
These types of studies are of critical importance for chiropractors and the implications of how different radiographic anomalies and pathologies play into how they alter spine manipulative approaches is an understudied area. Anecdotally, these types of radiographic findings are important and have implications to patient care and outcomes.
Failure to Define “Red Flags”
Despite the fact that Corso et al 23 mentioned the word “red flags” 18 times throughout their review, they failed to specify the precise definition of the term in their paper. This is a critical flaw. For example, all spine guidelines, even “red flag” chiropractic guidelines (e.g., Bussieres et al 124 and Jenkins et al 22 ), allow for the routine and repeat use of X-rays in the diagnosis and monitoring of scoliosis of the spine. Scoliosis is not considered to be a traditional “red flag” per se. So, if Corso et al 23 do not consider scoliosis to be considered in their interpretation of a “red flag” then this just adds to the invalidation of the scope and findings of their review as scoliosis assessment and treatment is a major emphasis in the education of chiropractors and is commonly managed by chiropractors.
Eliminating Valid Studies Based on “Bias”
In the Corso paper, 23 all clinical trials that were located and included in their risk of bias scoring were thrown out due to “risk of bias.” In fact, no clinical trials were considered in their formal assessment of X-ray utility. Several of the trials we argue were of sufficient quality. For example, the Harrison nRCT (2002) 436 documenting X-ray-guided improvement in lumbar curve and pain levels after spinal manipulative therapy and extension traction methods as compared to no changes in spine alignment or pain level in a control group was considered by Corso et al 23 to be at high risk of bias, although in a recent systematic review this same trial was scored a low risk of bias 137 and the results of this initial nRCT were later found to be consistent with the results of RCTs on the topic.161-163
Another Harrison nRCT (2003) 437 was scored similarly to the previous trial and considered as having a high risk of bias (their Table 1). As mentioned, Corso et al missed 4 other CBP trials “done by chiropractors” that should have been included in their analysis.178,181,383,384 Importantly, if one of these trials were included in Corso et al’s final assessment, it would have reversed their conclusions. Corso et al mention that they included a “quality control step” in the critical appraisal of studies; the lead author presented a summary of appraised papers to 4 co-authors who “validated” the outcome of the appraisals. Indeed, the final internal validity rating of the papers was determined through “discussion” (p. 4). 23
It seems despite using a risk of bias scoring system, the actual allocation of uncertainty remained up to the assessor and we argue was conveniently extra critical, particularly when the study was performed by those who hold a pre-existing bias against X-ray use in practice, as we will discuss.
Conclusions Defies Impairment Rating Guidelines
According to the American Medical Association (AMA), “repeat” X-rays are required to be taken at “maximal medical improvement” (MMI) to determine intersegmental vertebral instability for impairment ratings.438,439
According to the fifth edition of the AMA Guidelines to the Evaluation of Permanent Impairment, Chapter 15, The Spine, 438 there are 2 methods to determine permanent impairment of the spine: (1) Diagnosis-Related Estimate (DRE) and (2) Range of Motion (ROM). “The DRE method is the primary method used to evaluate individuals with an injury” (p. 374). 438 The guideline references White and Panjabi 440 and Shaffer 441 to make the statement “Motion of the individual spine segments cannot be determined by a physical examination but is evaluated with flexion extension roentgenograms.” 438 Impairment is rated only when the patient has reached MMI as defined as the “date from which further recovery or deterioration is not anticipated, although over time there may be some expected change” (p. 19). 438
According to the sixth edition of the AMA Guidelines to the Evaluation of Permanent Impairment (AMA Guides) Chapter 17, The Spine and Pelvis, uses Diagnosis Based Impairment (DBI) regional grids. 439 As is the case with the fifth edition, 438 impairment ratings are only to be made when the patient has reached MMI. Four of the five defining variables dictating the Class in which the severity is determined for impairment ratings, including “alteration of motion segment integrity” (AOMSI) require radiographic investigation, again at MMI. 439
Healthcare providers including chiropractors, therefore, cannot perform an impairment rating in accordance with the AMA Guides438,439 without repeat X-rays performed after treatment methods have been exhausted. Assuming initial X-rays were obtained on an injured patient, these “repeat” X-rays are required in the determination of most cases of permanent impairment of the spine, and the CCBCs new policy runs counter to the long-established AMA Guides.
Co-Authors Hold Anti-Imaging Bias
It seems ironic that a review that concludes there is “no evidence” of X-ray utility in the entire chiropractic literature when, as we have indicated this is completely contrary to hundreds of missed studies, is made by at least 2 authors who have known biases against routine X-ray use. Côté has vocalized anti-imaging sentiment at scientific conferences attended by some of the present authors (e.g., verbal exchange during platform presentation question and answer session
441
) and Corso has expressed anti-imaging bias on social media outlets (Figure 6). Notably, a critical validity concern of RRs is “author bias,” and notably, Corso was the sole researcher responsible for the article review using their version of RR methodology. Tweet by the primary author years before conducting review on X-ray utility in chiropractic shows strong bias against X-ray use in practice.
Strong Conclusions Based on Little/Conflicting Evidence
Corso et al 23 stated that “No relevant studies assessed the clinical utility of routine or repeat radiographs (in the absence of red flags) of the cervical, thoracic, and lumbar spine for the functional or structural evaluation of the spine. No studies investigated whether functional or structural findings on repeat radiographs are valid markers of clinically meaningful outcomes.” 23 Despite these claimed findings, the authors draw the conclusion “we found no evidence that use of routine or repeat radiographs… improves clinical outcomes and benefits patients.” and therefore “recommend chiropractors do not use x-rays.” 23 This is not a scientific statement. A basic tenant of evidence synthesis is that one cannot make conclusive statements when the evidence is limited (which in this case is not, just ignored) or when the evidence is inconclusive (which again in this case is not, just ignored). The Corso et al 23 findings are opinion and at odds with scientific reality.
It has already been mentioned that many have questioned the validity of RRs since the methods involve “shortcuts,” and we pointed out that it would be easy for an investigator to adjust the methods to suit an agenda. It is questionable that based on only 9 papers, the authors could draw such a strong conclusion, especially concerning that only two papers addressed the validity of X-ray use, and one of these papers clearly support X-ray use. The McAviney et al 371 paper showed powerful results in conflict with Corso’s conclusions. Within the Corso paper, 23 they did mention McAviney et al 371 found that patients having a neck curve less than 20° had twice the odds of having cervicogenic symptoms. Importantly, McAviney et al 371 also determined that patients having a straightened or reversal of the normal neck curve had 18 times the odds of having cervicogenic symptoms. This latter finding within the included McAviney et al 371 paper was not mentioned by Corso et al. 23 Thus, 50% of the included validity evidence (1 of 2 papers) showed X-rays to be very useful in the assessment of sub-acute and chronic neck pain patients. Conspicuously, Corso et al stated that “these studies provide no evidence of clinical utility.” 23
The volume of literature is much larger than the 9 articles included in the Corso et al analysis. 23 It is our contention that the exclusion of at least the 64 missing studies meeting their own inclusion/exclusion criteria that we mention here,178,181,209-232,373–377,379,380,383–387,390–401,413–424,429,430,432, as well as about 180 studies we also referenced that were excluded based on “not performed by a chiropractor” 143-145,147,149,152-160,233-370,388-411,425-428 would have undoubtedly led to the scientifically accurate conclusion that routine and repeat X-rays are very much an evidence-based practice for chiropractors who specialize and practice various X-ray-guided approaches to spine care.
It is noted that the journal in which they selected to publish their RR has also published many papers with dissenting views of the chiropractic profession in which reviews/commentaries are known for overreaching and generalized conclusions,442-451 and also for which the long-time chief editor has anti-imaging views. 452 Regarding the Corso et al 23 manuscript, several authors of the present paper submitted letters-to-the-editor (LTE) to point out many critical flaws; however, surprisingly, these letters were “peer reviewed” and finally rejected without ever making it to the Corso et al authors. It is noteworthy that some of the current authors who have published multiple previous LTEs453-462 had never previously experienced a journal formally ‘peer reviewing’ an LTE. In the end, the Corso review is pseudo-science and should have failed peer review.
CCBC Rapidly Reviews and Changes the 1934 Policy (Figures 7-9)
Chiropractors in BC have had full and unrestricted use of radiography rights since they were established in 1934.
197
The Corso et al paper
23
was published online on July 9, 2020, and the CCBC announced to its members that it was reviewing the policy of full X-ray rights one week later on July 15, 2020 (Figure 7). After collecting member and public feedback as of September 8, 2020, it was stated that “A summary of comments will be posted after the consultation period.” (Figure 7)
463
Message from CCBC to its members (August 11, 2020). This notice signified the board was collecting member and public feedback to “anticipated amendments” (“red flag” only X-ray use) between the dates August 11, 2020, to September 8, 2020. This message also indicated the research to support this effort was the Corso et al
23
rapid review. Original “draft amendments” to the Professional Conduct Handbook Part 15 (X-ray use) proposed by CCBC (August 11, 2020). This is the first time X-rays were proposed to be restricted to “red flag” only use since chiropractors were licenced to utilize radiography in British Columbia, Canada, in 1934. This draft amendment was created prior to member/public feedback. Final “approved amendments” instituted by CCBC (February 4, 2021). The new policy strictly revokes X-ray use except for purpose of examining suspected “red flag” conditions. In the announcement on their website, they state “The application of radiography is not without risk and therefore, must be carefully considered.”


As of July, 2021, 6 months after the CCBC instituted radical policy change discriminating against chiropractors who utilize X-rays for reasons other than diagnosing serious medical pathology (i.e., “red flags”), there has been no disclosure of the comments from its members and the public.
24
On a September 25, 2020, “update” the CCBC did acknowledge that they had received over 1000 responses to the proposed changes including themes related to
463
Ensuring that any policy changes more clearly include the clinical judgment of the chiropractor; A request that the College further define “red flags” that a chiropractor may use in determining the need for radiography and what factors are necessary in leading to determining the need for radiographs; o Factors such as a thorough history and examination leading to a determination of the necessity of further testing and/or radiographs. Clarifying the literature/studies that were considered by the independent researchers, and why other studies were not included in the rapid review; and Providing more information about and safety concerns regarding the use of radiography.
As shown, the issues raised in these themed responses are important and to this day have not been addressed. The entire timeline from when the CCBC first informed its members that it was reviewing a well-established and important policy of full radiography rights to revoking these full rights to parallel medical practice “red flag” use was over a period of only 6 months (Figures 7-9).
It is suspect when a governing College makes such rapid and radical policy change to a practice that had been in place for 87 years (1934). Particularly concerning is that the CCBC have not posted the member/public comments, they contracted to an individual with known anti-radiology bias and implemented the “draft amendments” (Figure 8) citing radical restrictions 1 month after the publication of the flawed review that were unchanged (Figure 9) after apparent consideration of over 1000 member/public feedback letters of concern, admittedly most being critical to the proposed policy change. 463
As mentioned, reliability studies are important, and the 8 included studies showed good reliability that provide legitimacy for X-ray use in practice. The validity studies are of utmost importance to address the clinical utility of X-ray use in practice, and regarding these, we question how such a radical and discriminatory policy change could occur so quickly after 87 years and also hinge on only 2 validity papers when one (McAviney et al 371 ) clearly supports X-ray use.
This new CCBC policy, that restricts full X-ray use including for analysis of biomechanical parameters as well as screening for anomalies and pathologies that may alter treatment approach, is clearly neither evidence-based nor ethical. In fact, the new policy may be a threat to public health as spine care patients will unknowingly be limited to subpar clinical investigation (no X-ray for biomechanical assessment) and management (no biomechanical outcome goals—i.e., scoliosis, etc.). Undoubtedly, this may have dire and cascading consequences to countless patients and their clinical outcomes.
Discussion
The many criticisms of the Corso et al 23 rapid review illustrate how flawed methodology results in flawed conclusions. It is suspect that the CCBC contracted an individual to conduct a systematic review on a well-entrenched aspect of chiropractic clinical practice that ended up as an incredibly limited and fatally flawed, “rapid” review with sweeping and generalized conclusions condemning routine/repeat X-ray use. In fact, the conclusion of the Corso et al 23 paper is based on only two validity papers. One of the two validity papers very clearly powerfully supports X-ray utility in clinical practice. It is concerning that the authors of the contracted Côté paper concluded there is “no evidence” for X-ray use in chiropractic (outside of “red flag” screening) when literally dozens of chiropractic-specific papers178,181,209-232,373-380,383-387,390-401,413-424,429,430,432 and 100s of other papers were clearly missed. 143-145,147,149,152-160,233-370,388-411,425-428
The Corso et al 23 statement “We found no evidence that the use of routine or repeat radiographs to assess the function or structure of the spine… improves clinical outcomes and benefits patients” is factually false, it is antithetical to scientific reality, and it is based on a fatally flawed review that was written by biased researchers who hold anti-imaging ideology. It is ironic that Corso et al 23 attempted to assess the “clinical utility” of X-ray use in chiropractic when there is no unequivocal answer to the meaning of clinical utility; in fact, “Clinical utility will always be in the ‘eyes of the beholder,’ and the answer will therefore be different depending on the interests and goals of the stakeholder.” 464 Lesko et al 464 remind us that the evidence of clinical utility will be judged differently by equally qualified peers to the usefulness of the diagnostic (in this case X-rays) as applied to patients to their real-world clinical practice settings.
It is irresponsible that the CCBC, a formal regulatory body made a fundamental policy change so rapidly, basing its decision on a single flawed review, all while acknowledging over 1000 feedback responses were mostly critical of the change. The member and public feedback were obviously not considered as the draft for the policy change released prior to the open feedback period (Figure 8) did not change following public/member feedback (Figure 9); in fact, it was more strictly specified. To this day, the CCBC has not released the content of the 1000+ feedback responses.
Perhaps the most tragic outcome to the policy change that discriminates against chiropractors who practice evidence-based, X-ray-guided methods is the fact it actually discriminates against the healthcare consumer (ie, patient) by not allowing them to make health choices based on education provided within a risk-to-benefit ratio by clinicians. In fact, it is known that certain spinal disorders can predispose affected patients to future undesirable outcomes, including greater injury rates, 465 greater injury severity (e.g., during motor vehicle collisions466-469), development of future pain and disability (e.g., having lumbar hypolordosis 470 ), having lingering pain and disability after a sustained injury (e.g., nonrecovery after whiplash 466 ) and even early mortality (ie, from thoracic hyperkyphosis471-477). Most of these spine deformities have established or evolving evidence for their non-surgical treatment and reduction. It is an honest and ethical practice to screen and inform appropriate patients of the pathognomonic consequences of certain spinal conditions.
As discussed, it is a well-framed and evidence-based practice to routinely assess a patient’s spine and pelvis for biomechanical assessment that is linked to procedural treatment approaches and patient outcomes. In a recent synopsis of the clinical utility of X-rays in chiropractic and the manual therapies,
25
it was determined X-rays are uniquely required by chiropractors and manual therapists specializing in spine-altering techniques and practices for three main purposes: To assess spinopelvic biomechanical parameters; To screen for relative and absolute contraindications to spine care; To re-assess a patient’s progress to some types of spine rehabilitative treatments.
We would add an obvious fourth reason; that is, to rule out “red flags” or serious medical conditions (i.e., malignancy, infection, and fracture) unrelated to spine care that would warrant immediate referral. The recent restriction of X-ray rights by the CCBC increases the liability to the doctor who, in many instances, is now “handcuffed” and forced to treat patients “blindly.”
Discrimination against the consumer of spine care will subject them to limited (in many cases inadequate) clinical investigation and therefore limit management options (e.g., restrict spine-altering options including specific vectored spine adjustments, spine corrective traction, spine corrective bracing, and spine correcting exercises). Patient care planning requires the consideration of patient goals, needs, and values. Indeed, when clinical opinion varies, lawmakers and policy makers must weigh consumer values and desires into policy decisions taking into account therapeutic risks, and in the case of diagnostic ionizing radiation, the risks are shown to be negligible. Full evidence-based practice (EBP), in fact, consists of three separate arms: (1) clinical evidence, (2) practitioner experience, and (3) patient preferences. 478 To not consider practitioner experience or patient preference is to not follow true EBP. The CCBCs new policy change to restrict full radiography use directly opposes modern EBP principles 2 and 3 and is clearly based on only a pre-select “drop” of the actual ocean of scientific evidence available on the topic.
Conclusions
Radiation exposures from X-rays used in the assessment and monitoring of patients receiving particular forms of chiropractic and manual therapy treatments are not a public health threat. These low-dose radiation exposures have not been shown to cause harm; in fact, all recent evidence shows it reduces carcinogenic effects. The rationale to avoid X-rays based on LNT-based mythology is perpetuating radiophobia surrounding carcinogenic fears that will not occur. Outdated misinformation of the dangers of medically warranted X-rays should cease.
The radical policy change by the CCBC to restrict chiropractors in British Columbia, Canada, from utilizing X-rays for biomechanical screening and re-assessment purposes harms the spine care consumer by limiting their choice and discriminates against practitioners who have enjoyed EBP freedom since 1934. The new CCBC X-ray policy restrictions oppose EBP. The CCBC actions in creating this recent policy change are suspect as it is based on a single paper 23 that is proven to be fatally flawed and that over 1000 mostly critical feedback letters were not considered or even released to the members.
Herein, we have cited dozens of chiropractic studies that should have been included in the contracted Côté review 23 and hundreds of others that directly apply to modern, evidence-based, and radiography-guided chiropractic clinical practice. We recommend the CCBC to reverse its unscientific policy regarding the unprecedented restrictions of licenced chiropractors to take X-rays. Public health policy changes based on scientific misinformation through faulty and biased study design are a major threat to the safety and health of the public.
Footnotes
Acknowledgment
We thank Drs Gregory Plaugher, David Beaudoin, Surdeep Dhaliwal, Mark Foullong, Dustin Freund, Brad Gage, Melody Jesson, and Franchesca Lee for their invaluable input. We also thank the reviewers for their feedback.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PAO is a paid consultant for CBP NonProfit; DEH teaches spine rehabilitation methods and sells products related to the treatment of spine deformities.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The APC charge was funded by the International Chiropractor’s Association.