
Abstract
Since the 1980s, increased utilization of medical radiology, primarily computed tomography, has doubled medically sourced radiation exposures. Ensuing fear-mongering media headlines of iatrogenic cancers from these essential medical diagnostic tools has led the public and medical professionals alike to display escalating radiophobia. Problematically, several campaigns including Image Gently, Image Wisely, and facets of Choosing Wisely propagate fears of all medical radiation, which is necessary for the delivery of effective and efficient health care. Since there are no sound data supporting the alleged risks from low-dose radiation and since there is abundant evidence of health benefits from low-doses, these imaging campaigns seem misguided. Further, thresholds for cancer are 100 to 1000-fold greater than X-rays, which are within the realm of natural background radiation where no harm has ever been validated. Here, we focus on radiographic imaging for use in spinal rehabilitation by manual therapists, chiropractors, and physiotherapists as spinal X-rays represent the lowest levels of radiation imaging and are critical in the diagnosis and management of spine-related disorders. Using a case example of a chiropractic association adopting “Choosing Wisely,” we argue that these campaigns only fuel the pervasive radiophobia and continue to constrain medical professionals, attempting to deliver quality care to patients.
Keywords
Introduction
Since the advent of computed tomography (CT) imaging in the 1970s, medical utilization of this technology has skyrocketed, so much so that medical radiation has nearly doubled in its exposure profile to the general population. 1 In fact, according to the National Council on Radiation Protection and Measurements (NCRP) Report 160, the average ionizing radiation exposure to the general US population has increased from 3.6 mSv in the 1980s (15% of all exposures) to 6.2 mSv in 2006 (48% of all exposures). 1,2 This has largely been due to CT imaging, followed by nuclear cardiology procedures (Table 1). Conventional radiography is about 11% of medical exposures, 1 and these doses represent an order of magnitude less than CT scans (1-3 mGy vs ∼10-30 mGy; Figure 1). 3
Source and Percentage of Medical Radiation to the US Population (NCRP 160). 1

Abbreviations: CT, computed tomography; NCRP, National Council on Radiation Protection and Measurements.

Estimated radiation doses (mGy) from typical medical diagnostic procedures. A full-spine radiographic series would deliver about 2 to 3 mGy, a typical single CT delivers about 10 mGy. 3 Note: CT doses are shown for multiple scans. CT indicates computed tomography.
Despite CT imaging being the main culprit for this near doubling of radiation exposure from medical imaging, in the past decade, radiation reduction campaigns have targeted any and all radiological imaging. These radiation campaigns have been launched largely because of the NCRP Report 160 and include “Image Gently” for children, 4 “Image Wisely” for adults, 5 and aspects of “Choosing Wisely” 6 which creates dedicated lists of “questionable” or “unnecessary” tests, treatments, and procedures for various medical specialties. Irrespective that conventional radiography is one of the smallest medical sources of exposures for patients (as opposed to CT imaging), the movement of radiophobia created and propagated by these campaigns is far and wide and presents challenges to those in the spinal rehabilitation sector utilizing radiography to assess and treat patients with spine ailments and deformities. 7
In conflict with the “limiting” radiation campaigns is the fact that X-ray-guided treatment for the management of spinal disorders is commonplace in spine deformity evaluation and surgical interventions such as for those with spinal stenosis 8 or osteoarthritis, 8 or those with spine abnormalities such as cervical kyphosis 9 or scoliosis. 10 Nonsurgical spine correction/rehabilitation approaches have also evolved and have an expanding evidence base where radiography is intimately connected to procedure approaches (techniques) and patient outcomes. 11 -26 In some cases, a substantial amount of high-quality evidence from randomized controlled clinical trials (RCTs) with long-term follow-up exists establishing that radiography-guided patient-specific interventions improves outcomes compared to standard/generic interventions not guided by a patient’s specific radiographic spine findings. One example of this is the Chiropractic BioPhysics (CBP) technique combined with multimodal rehabilitation procedures for reducing forward head translation, 11 -16 increasing cervical lordosis, 11 -16 and increasing lumbar lordosis 17 -19 as assessed by spine radiography. Additionally, RCTs provide evidence for spine correction from physiotherapy back extension exercise programs to reduce thoracic hyperkyphosis, 20 -22 as well as physiotherapeutic scoliosis-specific exercise programs (eg, Schroth methods) for reducing scoliosis spinal curvature. 23 -26
Clinically weaker evidence (from case control, case studies/series) exists supporting the effectiveness of many other nonsurgical generalized spine rehabilitation approaches, for example various methods to reduce forward head translation, 27 -30 thoracic hyperkyphosis, 31 -36 scoliosis, 37 -40 pseudo-scoliosis, 41,42 spondylolisthesis, 43 and methods to increase thoracic hypokyphosis. 44,45 There are in fact many spine and posture rehabilitation approaches that use spinal X-rays for the diagnosis and screening of biomechanical parameters essential in guiding patient-centered, spine-specific rehabilitation approaches to reduce various spine displacement or subluxation types 46 in the effort to enhance patient outcomes.
Recently, there has been mounting pressures to reduce the use of radiography in the assessment of patients with spine problems. 47,48 Specifically, within the chiropractic profession, “chiropractic guidelines” have emerged which emulate medical pharmacologic-based practice low back pain guidelines (ie, Jenkins et al 47 ; Bussiéres et al 49 ) which recommend no initial X-rays for patients presenting with uncomplicated acute low back pain (ALBP) with the exception of “red flags” (serious conditions including tumor, infection, fracture, cauda equina syndrome, etc). 50 Of interest, we agree that limiting radiography is a reasonable practice in the setting of “standard medical” pharmacologic evaluation as the prescription of medicines, bed rest, limiting activity, general stretching, and so on do not require knowing the exact spine alignment of a specific patient. Although the rationale for spine radiography limiting recommendations are multipronged (cost, psycho-social, etc), the main underlaying theme is to “protect” the patient from radiation exposures.
The trend of spine radiography limiting campaigns and guidelines in spine rehabilitation settings is of concern for several reasons. First, the percentage of ALBP patients in clinical practice is likely small versus those presenting with either chronic LBP or an acute flare up of recurrent LBP (ie, type of chronic LBP—most cases). 51 Likewise, many patients presenting with ALBP also present with various other spinal disorders other than low back complaints (eg, low back and neck issues). 52 Thus, we question why ALBP guidelines are pushed so heavily on clinicians when these represent a minority of patients encountered in clinical practice. Second, these guidelines invariably get generalized and become promulgated for all patients rather than for patients presenting exclusively with ALBP for which they were intended. 48 Further, X-ray restrictive guidelines assume that all chiropractors and manual therapists practice techniques using generalized, multilevel gross spinal manipulation, which most RCTs on back pain utilize. 53 This assumption is inappropriate since vertebra-specific spinal adjusting procedures are taught in chiropractic college curricula. X-ray restrictive guidelines and their supporters often ignore or dismiss the scientific evidence supporting structural-based spine care. 54 -56 Thus, the universal pressure to restrict X-ray use in spinal rehabilitation goes against the evidence-based practice of many patient-centered, spine-specific, biomechanical treatment approaches that are readily available, taught in graduate and postgraduate education, and practiced by a significant number of clinicians. 11 -45
The most critical factor underpinning the creation of X-ray restrictive guidelines is the push to reduce radiation exposures due to carcinogenic concerns. 47 -49 We will discuss how this long-held assumption of carcinogenic risks from low-dose X-ray exposures is based on invalidated science. We have chosen scoliosis of the spine as a clinical example to discuss the radiation exposure to such patients. Scoliosis patients represent a unique cohort as it is accepted, even in restrictive X-ray guidelines, that these patients will receive repeated imaging (and radiation exposures) over the course of their treatment and management.
We will discuss the use of X-rays in the treatment of scoliosis including number of total X-rays and estimated total exposures, the evolution of medical radiation restriction campaigns, the fact that the threshold dose for radiogenic cancer is 100 to 1000 times greater than medical X-rays, discuss how studies on imaging-induced cancers are either false or misrepresented, briefly review important studies of low-dose radiation exposures showing evidence of health benefit—not harm, discuss how the innate adaptive protection systems prevent, repair, or remove DNA damage to avert cancers, and finally, demonstrate the cascading effects of “Image Wisely” campaigns using a recent case example of a chiropractic association that participates in the “Choosing Wisely” campaign. 48
Radiography for Scoliosis of the Spine
Scoliosis of the spine is a curvature representing a lateral bending of the spine with simultaneous segmental torsional rotation with lateral translation offset from midline in the coronal plane. Generally, a curvature measuring 10° or greater on an anteroposterior (AP) or posteroanterior radiographic view as quantified using the Cobb angle of measurement signifies definitive diagnosis (Figure 2). 57

First: Cobb angle of measurement; second to fourth: AP radiographs showing an initial 48° scoliosis (T5-L1) in a 14-year old female which reduced to 13° with the patient wearing a rigid corrective brace; after 3 months, a 19° reduction occurred as a follow-up, out-of-brace image showed a 29° curvature as measured from the same vertebral levels as the initial. This patient is still under treatment by the first author. AP indicates anteroposterior.
Although the focus of scoliosis research has centered around the treatment of children and adolescents, scoliosis can affect patients of any age. Patients with scoliosis receive repeated spinal X-rays during the management of the disorder, which may include “watchful waiting” (no treatment), spinal exercise programs, back braces (Figure 2), spinal traction, and/or eventual surgery. 58 Scoliosis is a major concern for young patients as it may progress during growth and if severe, leads to compromise of the pulmonary and cardiac organs. This is why surgery has long been a mainstay for treating progressive scoliosis deformity and also why there are expanding evidence-based nonsurgical approaches for this disorder. 59
Specific to scoliosis, studies have documented the number of spinal radiographs as ranging from 10 to 25 images, 60 -62 to as many as 40 to 50 images over several years. 63 The more severe the spinal curve, the greater the number of X-rays received during treatment and follow-up. 63 The amount of radiation required for a quality spinal image depends both upon the region to be examined as well as the relative size of the patient. For an AP thoracic spinal image, the absorbed dose ranges from about 0.5 to 1 mGy for a pediatric patient to an adolescent, though these estimates may fluctuate due to the patient thickness and the performance of the X-ray machine.
Hence, the total estimated cumulative dose a typical scoliosis patient may receive over several years, ranges from about 10 to 50 mGy. 59 The concept of cumulative dose is of interest to those employed in radiation protection, as it is based on the presumption that radiation damaged cells accumulate rather than being repaired or removed and replaced. This leads to the linear no-threshold (LNT) dose–response model of radiation-induced mutations (which leads to cancer) in application of risk assessment from low doses. 7,54,59
The Evolution of Medical Radiation Restriction Campaigns
The Image Gently Alliance 4 began as a committee within the Society for Pediatric Radiology in late 2006. It is a coalition of health-care organizations “dedicated to providing safe, high quality pediatric imaging worldwide.” The Society for Pediatric Radiology worked with sister societies including the American College of Radiology (ACR), the American Society of Radiologic Technologists (ASRT), and the American Association of Physicists in Medicine (AAPM) to form “the Writers Group.” The concept of the Alliance was created and the “Image Gently” campaign was launched in 2007 to raise awareness in the imaging community to reduce radiation doses when imaging children.
The Image Wisely Alliance 5 initiated with the creation of the Joint Task Force on Adult Radiation Protection formed by the ACR and the Radiological Society of North America. This task force was to address concerns over the apparent surge of public exposure to ionizing radiation from medical imaging. After collaborating with the AAPM and the ASRT, borne was the “Image Wisely” campaign (2009) with its objective of “lowering the amount of radiation used in medically necessary imaging studies and eliminating unnecessary procedures.” This campaign offers information to radiologists, medical physicists, other imaging practitioners, and patients; it also encourages members to sign a pledge (Figure 3).
Pledge to be abided for referring practitioners and imaging professionals who want to join the “Image Wisely” campaign. 5
Another campaign, “Choosing Wisely” 6 is a US-based health education campaign spearheaded by the American Board of Internal Medicine (ABIM) and was launched in 2012. To participate in Choosing Wisely an interested society must develop a list of 5 to 10 tests, treatments, or procedures that are perceived as commonly overutilized within their healthcare field. Then, the Choosing Wisely initiative publishes this list on its website and shares it with its members. The participating society is encouraged to publicize this list to its members and to the public. The campaign has been criticized as its motive is for cost savings and not for enhanced patient care, as well as the creation of specific medical specialty lists are often formed by society executive without including input from their members. Another grave criticism is that it is feared that third party payers will perceive these lists as evidence or actual guidelines and use it to deny reimbursement for various medical tests and procedures despite the Choosing Wisely website explicitly stating: “Choosing Wisely recommendations should not be used to establish coverage decisions or exclusions.” 6
Recommendations against “unnecessary” radiological imaging are included in several of the various discipline-specific recommendation lists. As of April 2018, there were 552 recommendations distributed on lists for more than 80 medical society partners. The Choosing Wisely initiative has also motivated other nations to entertain implementing similar programs in their respective countries. Although these lists contain many logical and cost-effective suggestions, it is the ones concerning the avoidance of medical diagnostic radiation that we are concerned with.
The American Chiropractic Association (ACA), for example, in association with the ABIM published a list of 5 practices to question regarding chiropractic services 48 ; 2 of these items include avoiding X-rays (1. “In the absence of red flags, do not obtain spinal imaging [X-rays] for patients with acute low-back pain during the six weeks after the onset of pain”; 2. “Do not perform repeat spinal imaging to monitor patients’ progress”). We will use the ACA adoption of Choosing Wisely as our case study of how this has unnecessarily created problems within the chiropractic profession.
Carcinogenic Radiation Dose Threshold Is 100 to 1000 Times Greater Than Medical X-Rays
Vaiserman et al 64 argue the most accurate information on health effects from low-dose radiation exposures are from studies on medical/technical personnel who were occupationally exposed. In the early part of the last century, prior to 1920, there were increased cancers in radiologists, radiologic technologists, radiation, and nuclear workers; however, this trend disappears after 1920, 65,66 when the first radiation limits were set in place at 0.2 R/d, which corresponds to about 500 mGy/year. Some argue that current standards are very over-restrictive and that the historical standard was sufficient. 64,67
The traditional data set used to support the linear no-threshold model used for risk assessment from radiation is the Nagasaki and Hiroshima atomic bomb survivor data, a part of the Life Span Study (LSS). 68 A recent analysis of these data (2012) has shown a departure from the linear dose–response assumption. 69 Doss points to the fact the data shows no negative health effects up to the dose of 700 mGy. 70 Another analysis (2019) of this same cohort shows an even higher dose threshold for leukemia at 1100 mGy (Figure 4), where it was pointed out that only 0.5% of the 10 000 residents who received a dose above 3000 mGy developed leukemia. 71,72 These data suggest that the human threshold for radiation exposure is quite high; carcinogenic exposures are 100 to 1000 times greater than that given by medical X-rays.

Evidence of Spinal Imaging–Induced Cancer Is Either False or Misrepresented
Chiropractic and other physical medicine professionals have been treating scoliosis patients for more than a century, and they have been using radiographic imaging to diagnose, monitor the progression of deformity, and assess treatment effect (ie, “stabilization” or reduction in curve).
59
Epidemiological studies have been carried out over the years to estimate the risk of cancer due to these low radiation exposures,
60,61,73,74
but these are based on the LNT model that has yet to be validated for low-dose radiation exposures.
7,59,75
-80
Further, the LNT model is not meant to be used for this purpose as the ICRP states: it is not appropriate for the purpose of public health planning, to calculate the hypothetical number of cases of cancer or heritable disease that may be associated with very small doses received by large numbers of people over very long periods of time.
81
Studies of Low-Dose Radiation Exposures Show Evidence of Health Benefit, Not Harm
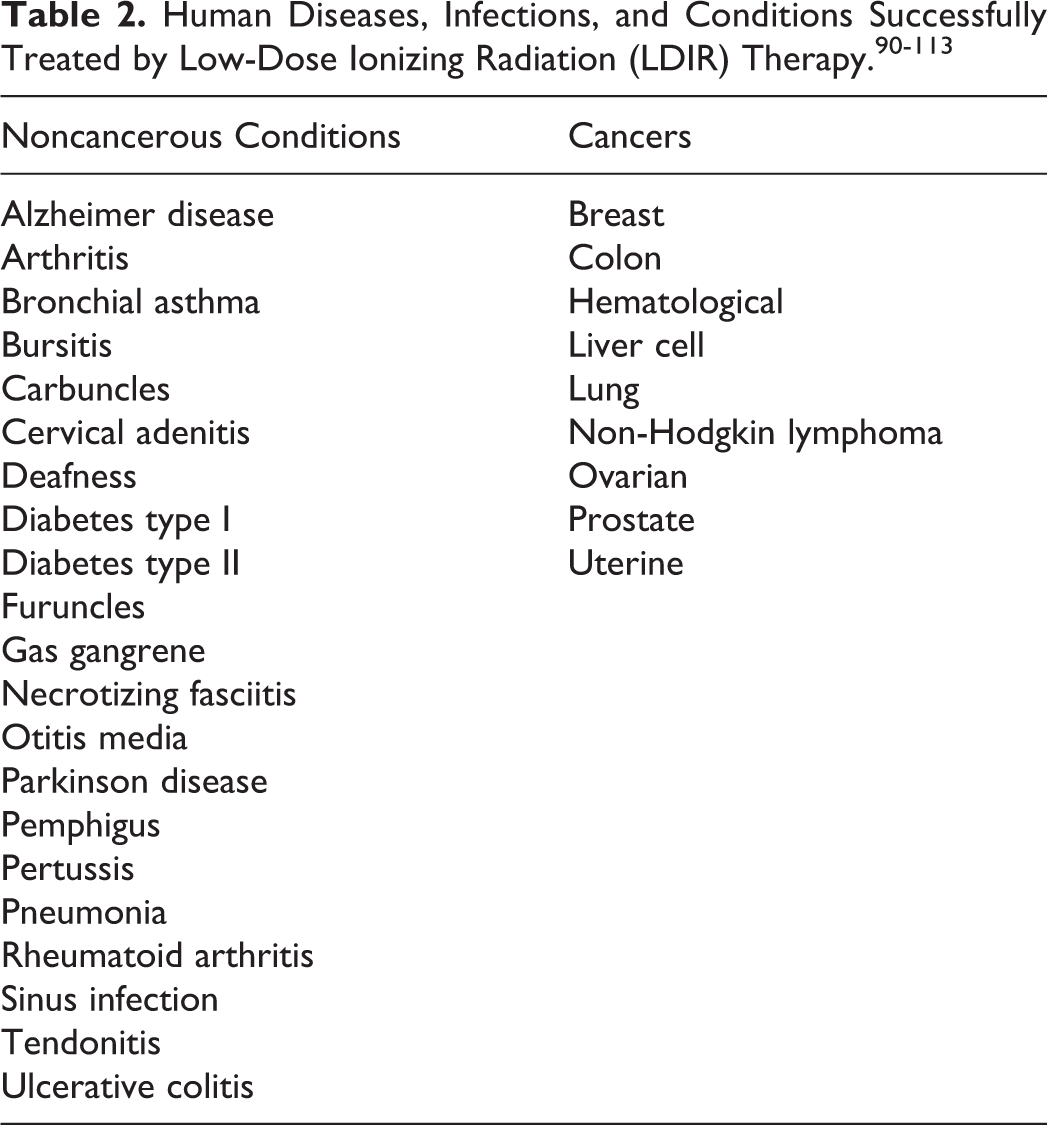
Radiophobia created from medical radiation restriction campaigns discourage use of low-dose ionizing radiation (LDIR) for use as actual treatment (by exposure) and research of so-called “radiotherapy.”
90
This is not entirely the fault of the practitioner/radiologist, as the medical educational system is devoid of information on the many applications of LDIR in medicine. As Cuttler notes: It appears to be unacceptable for physicians to learn about or use LDIR therapy…. Physicians are not taught the experience of the past 120 years that low doses of radiation stimulate the (body’s innate) protective systems, including the immune system, which involve more than 150 genes.90(p5)
Other evidence on health benefits from low-dose radiation exposures comes from the reanalysis of the Canadian breast cancer fluoroscopy study data, 115 where Cuttler and Pollycove demonstrated females treated for tuberculosis up to 300 mGy had a third less breast cancer than background incidence. 116 Tubiana et al showed cancer incidence for secondary malignant neoplasms in those who were previously treated by high-dose radiation up to 0.5 Gy (500 mGy) for childhood cancers had fewer secondary cancers than expected. 117 Hwang et al showed that residents living in buildings contaminated with Cobalt-60, showed 30% less cancers than expected with total exposures estimated at 0.048 Gy (48 mGy). 118
Another essential consideration for health effects due to low-dose exposures comes from inescapable background exposures. For example, the cancer incidence is lower for people living at higher altitudes (eg, Colorado vs sea-level). This decrease has been attributed to the higher radiation level, due to cosmic sources. 119,120 Radon exposure from the ground also has great fluctuations, and Cohen determined that residents living in the counties with the highest radon levels had the least lung cancer rates. 121 -123 There are many global regions that show surprisingly very high background radiation levels including Ramsar (Iran), Guarapari (Brazil), Karunagappally (India), Arkaroola (Australia), and Yangjiang (China). Residents of Ramsar, Iran, receive annual exposures of up to about 260 mGy, which is 80 times the world average. 124 Most importantly, there have never been any reports of radiogenic adverse health effects to residents living in these super high background radiation levels anywhere in the world 78,125 -127 ; in fact, the residents in such areas have been shown to have a greater adaptive response than controls. 128
Innate Adaptive Systems Prevent, Repair, or Remove DNA Damage to Prevent Cancers
As discussed, an abundance of good evidence points to low doses of radiation as having biopositive or healthful effects on the body, leading to fewer cancers—not more. Therefore, the question is: How can low-dose radiation exposures decrease cancers? The answer lays in the body’s incredibly effective innate adaptive protection systems (aka “DNA damage-control biosystem”; Figure 5). 129 -133 Pollycove and Feinendegen 129 have illustrated that about one million natural DNA alterations occurring per cell, per day are remediated, resulting in only about 1 mutation after the body’s innate damage control biosystem performs its very efficient repair and removal processes.

Redundant and effect adaptive response system very efficiently prevents, repairs, and removes virtually all DNA alterations. 129
It is important to realize that radiation is ubiquitous and humans are constantly exposed to it from many sources including radon from the ground, buildings, rocks, cosmic sources, foods, our own bodies (Potassium-40), and so on. 134,135 Background radiation levels were also much higher hundreds of years ago (at least 10x higher). 134 Thus, the human body has adapted to handle radiation and other toxic agents that induce genetic damage. The most harmful source of DNA damage, in fact, is endogenous processes such as breathing air and normal metabolism. 126, 132 -134 Specifically, it is the leakage of free radicals (reactive oxygen species) from mitochondrial metabolism of oxygen that produce DNA alterations, 90,129,136 -138 and “aging, mortality, and cancer are associated with stem cell accumulation of permanent alterations of DNA, that is, the accumulation of mutations.” 90 Surprisingly, every hour, every cell in the body endures about 8000 DNA-modifying events—and this is independent of any radiation! 139
Traditionally viewed as a rare event, 140 DNA repair enzymes are a central function of living cells. 141 Our body’s efficient adaptive protection systems have both hierarchical layering of protection as well as redundancy functioning at the molecular, cellular, organ, and systemic levels. Although very high levels of radiation exposures certainly inhibit these systems, low-doses stimulate them and these involve gene activation, repair enzyme synthesis, protein synthesis, stress-response protein production, activation of membrane receptors, detoxification of free radicals, proliferation of thymocytes and splenocytes, and overall stimulation of the immune system and repair of DNA. 142 As discussed, the threshold dividing biopositive from bionegative health effects can be quite high (eg, 1100 mGy 71,72,90 ).
It is only with an appreciation of the body’s innate DNA damage control biosystem that one can fathom the dual adaptive system expression to low-dose versus high-dose exposures, that is, radiation hormesis. 143 Radiation hormesis is definitively a real phenomenon, more realistically describes the health benefits observed at low-dose exposures, and as mentioned also more realistically fits the LSS data that underpin the validity of the LNT concept. Linear no-threshold ideology suggests for each mutation, there is a linear increase in cancer incidence, except as Pollycove argues, this argument “focuses on the negligible number of mutations produced by radiation.” 144 Endogenous DNA assault (from breathing air) outnumbers the possible immediate radiation-induced damage to a cell by an X-ray by a million-fold. 7 Thus, it is factually preposterous to have radiophobic cancer concerns from medical X-rays after considering the daily burden of endogenous DNA damage.
Cascading Effects of Image Wisely Campaigns
In health care, the cascading effects of these image wisely campaigns are far-reaching and have political and social consequences to procedural interventions and reimbursement perspectives. For example, based on the ABIM’s Choosing Wisely initiative, in 2017, the ACA chiropractic association developed a position statement for its professional and consumer stakeholders called “Five Things Physicians and Patients Should Question.” 48 Although the ACA position provided an exception for chiropractors using radiographic imaging for the long-term management of “idiopathic scoliosis” disorders, their public policy is uncertain for other types of scoliosis (congenital, neuromuscular, de-novo, etc). Furthermore, the ACA 48 and other choosing wisely supporters 47,48,55 propagate inaccurate claims regarding the nature of spine alignment disorders and have created fear-mongering for radiation exposure from imaging. Specifically, the ACA 48 statement under point #2 not to take X-rays to monitor progress: “There is currently no data available to support a relationship between changes in alignment or other structural characteristics [of the spine] and patient improvement,” is quite false and contradicted by many types of quality publications including many RCTs. 11 -19
The reality of these imaging policies is that they deter/inhibit patients from receiving necessary spine imaging to aid in a proper diagnosis for their condition and they constrain the treating chiropractor or spine specialist from providing proven spine corrective care treatment approaches. Specifically, many patients with scoliosis have both short- and long-term back pain and related disabilities. Well-done studies have identified that key spine alignment alterations as determined and quantified on spine radiographs correlate to back pain, disability, and progression of deformity in scoliosis and generalized chronic low back pain patients. 145 -148 Furthermore, in specific types of scoliosis such as adult onset, alterations of the spine alignment have been found to be one of the triggers for the initiation of the scoliotic deformity itself. 149
Several well done RCTs have identified that patients who receive specific rehabilitation interventions designed precisely from their altered alignment on spine radiographs fare better in terms of long-term improved back pain, disability, spine function, and other important variables. 11 -19,24,25 Thus, a major ramification of these “well-meaning” imaging campaigns is the stifling of conflicting data and the potential stifling of radiographic patient-specific spine rehabilitation care programs known to aid in patient health outcomes for both scoliosis and nonscoliosis populations.
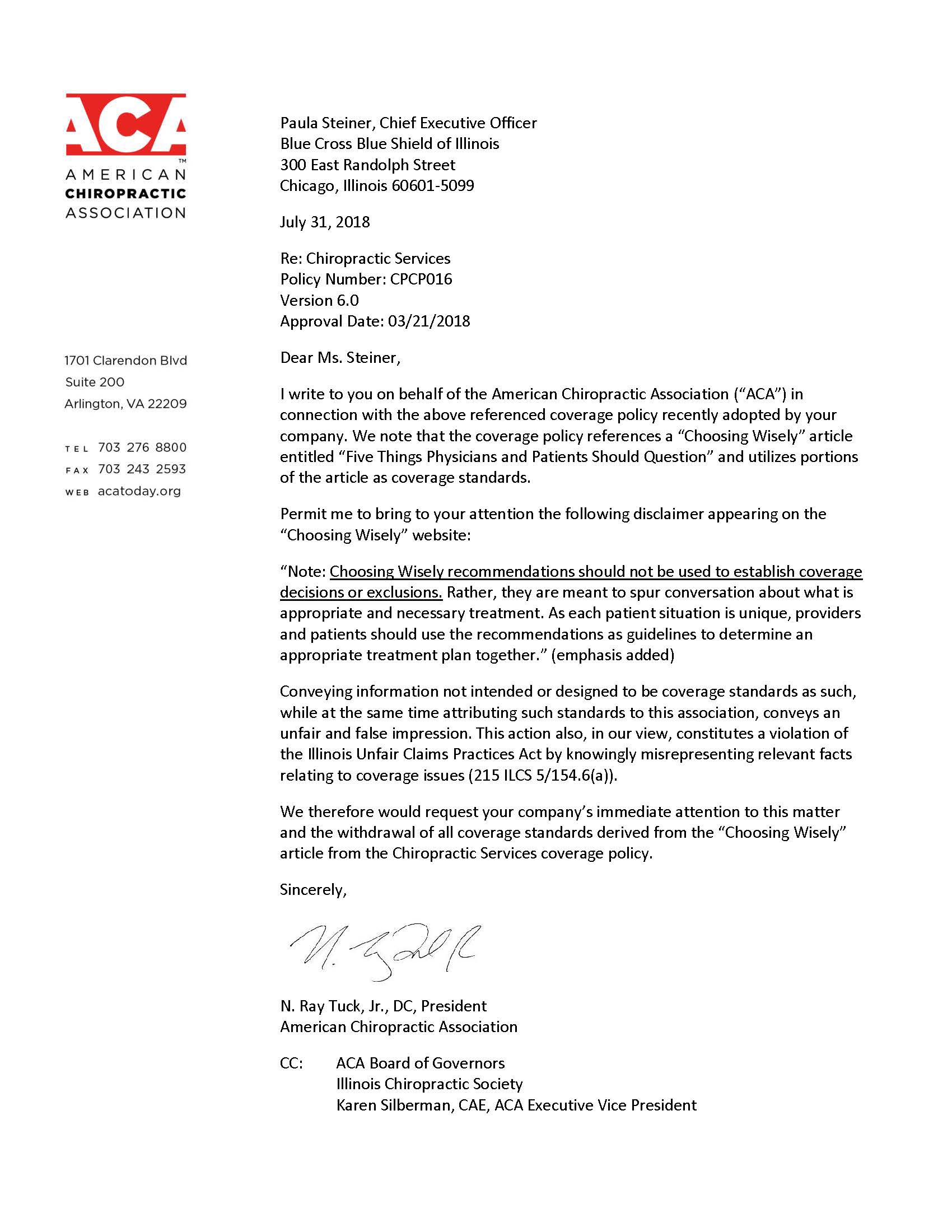
Finally, and perhaps tragically, the ACA’s adoption of the Choosing Wisely initiative led to some insurance companies including Blue Cross Blue Shield (BCBS) to routinely assign non-reimbursement for types of X-ray imaging claims as part of its “chiropractic services policy.” 150,151 This led to a back-peddling of the ACA as the president, NR Tuck formally requested CEO Pauline Steiner of BCBS to “withdrawal of all coverage standards derived from the “Choosing Wisely” article from the Chiropractic Services coverage policy.” 151
Ironically, the ACA released a statement to its members stating: “Should a chiropractic service be denied based specifically on the (Choosing Wisely) recommendations, ACA urges doctors to contact us immediately.” 152
Perhaps fundamentally flawed from the outset, the ACA’s list was created by an internal committee and did not involve essential stakeholders including practicing chiropractors, chiropractic state associations, chiropractic technique groups, and so on. Further, as stated under the rationale for the anti-imaging points 1 and 2, the ACA acknowledges that recommendations 1 and 2 are “performance measures” approved by Centers for Medicare and Medicaid Services for the 2017 Spine IQ Qualified Clinical Data Registry for Conservative Spine Care. 48 It should be mentioned that the ACA’s Senior Scientific Advisor, C. Goertz is also the CEO of Spine IQ, which partially aims to “define quality” in spine care delivery. 153 Since points 1 and 2 of the ACA’s interpretation of Choosing Wisely are anti X-ray use 48 and stem from a corporate entity’s (Spine IQ, IA, USA) attempt to define “good” clinical performance measures; this logically indicates that no or reduced imaging of a patient’s spine will be represented as the future standard for which chiropractic clinicians will be judged against. Problematically, as previously stated, this “good performance standard” is in direct opposition to considerable evidence 53,54,56, 154,155 and represents only one side of a controversial topic. 55,155 Problematically, this is one of the main critiques of the Choosing Wisely campaigns as “the motives of professional societies with Choosing Wisely lists has been questioned.” 156 Since the launching of the ACA’s Choosing Wisely campaign, over 30 chiropractic groups, technique organizations, state and national associations, foundations, colleges, and universities have formally rejected the ACA’s Choosing Wisely list 157 (Table 3).

To this day, the ACA’s Tuck and Goertz continue to publish blogs to the association’s website to rationalize the Choosing Wisely list and repeatedly emphasize: “Choosing Wisely lists are not guidelines, clinical care mandates, “never lists” or payor policies.” 158 In health care today, we agree that redundant and unnecessary tests and procedures should be minimized, however, to ignore a faction of an entire profession’s practice and ignore a plethora of high-quality evidence is contradictory to supporting best practices, confuses the public and divides the profession. Outside of important biomechanical spinopelvic parameters to assess for treatment, there are serious considerations in support of mandating X-rays for all patients presenting to chiropractors prior to receiving treatment. 159
Conclusions
It is our opinion that largely due to the release of ICRP’s 2006 Report 160 demonstrating a doubling of medical radiation exposures to the public that a renewed interest and radiophobia was ignited toward any and all medical radiation. Immediately following the release of this report was the launch of the “Image Gently” campaign aimed at reducing radiation exposures to children in 2007 and the “Image Wisely” campaign for adults in 2009. In 2012, the “Choosing Wisely” campaign was initiated that also lists many recommendations throughout many medical specialties toward limiting radiation exposures in medical practice.
The pressure on providers to limit radiation exposures to their patients changes practice triage and has been shown to increase radiation exposures, delay timely medical treatment, and add a heightened risk of liability burden to the practitioner. 160 All of these occurrences are counterproductive to the practice of efficient health care. Our case example of X-rays to scoliosis patients demonstrates that this is clearly an evidence-based practice and that no other imaging is more practical. 59 Further, it has also been demonstrated that low-dose medical radiation, even by repeated spinal imaging of patients over several years, is a safe practice. 59
Despite these imaging campaigns explicitly stating that their recommendations are just that, and not strict guidelines, the enthusiastic endorsement of these campaigns (eg, ACA’s endorsement within chiropractic) has led to the assumption that these are “guidelines” and to the denial of reimbursement claims by chiropractors by insurance companies (eg, BCBS). This case study of the chiropractic profession exemplifies the complete failure of an attempt to achieve the goals of improving patient care by adopting a radiation restriction campaign; rather this has backfired adding needless strain on chiropractic practice and is affecting the ability of patients to receive specific spine care based on radiographic findings.
We propose the elimination of medical radiology restriction campaigns. The efforts are based on the false premise that these methods of imaging are dangerous, when they are not. The body’s innate adaptive protection systems are stimulated; they over-remediate the damage caused by radiation. The immune system is stimulated. Evidence points to reduced cancer incidence from low-dose medical radiology (X-ray, CT scans), not more cancers.
Footnotes
Acknowledgments
The authors thank Niousha Navid Ehsani for feedback on this manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: P.A.O. is a paid research consultant for CBP NonProfit, Inc.; D.E.H. teaches spine rehabilitation methods and sells products to physicians for patient care that require radiography for biomechanical analysis.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funds from CBP NonProfit, Inc.
{kind=link}