
Abstract
Postural alignment is a critical determinant of health status. Its degradation is associated with deformity-caused and compensation-related back pain, neurologic involvement, osteoarthritic development, as well as disability and reduced quality of life. Radiography remains the most efficient method of evaluating standard sagittal and coronal spine and pelvic metrics that are used to plan surgical and nonsurgical treatment strategies. Many current spine guidelines dissuade the use of initial screening X-rays and some chiropractic guidelines condemn repeat imaging to assess progress from treatment regimens; these are anti-scientific viewpoints that ignore alternate viewpoints and evidence. Current understanding of the relationship between different spinopelvic parameters are essential to plan biomechanically appropriate interventions that are patient-specific. There are radiographically measured parameter thresholds critically related to several spinal disorders and positive patient outcomes. Current guidelines must include a caveat for contemporary biomechanical evaluation and its consequent specific treatments and should recommend routine radiographic imaging for spine patients undergoing corrective rehabilitative interventions. The failure to radiographically diagnose spinal deformity is argued to be negligence in many cases. The prime obstacle to routine X-ray imaging lies with the presumed threat of cancer, however, this is dogma; we summarize the main evidence from recent publications why this is so.
Introduction
Many guidelines for low back and neck pain recommend delayed imaging and dissuade practitioners from taking initial radiographs of their patients.1–4 This is particularly emphasized for patients presenting with new or acute spine pain, and some guidelines go as far as dissuading repeat imaging for assessing response to treatment (eg, ACA Choosing Wisely 5 ).5–8
A reality in spine care is that most patients have recurrent spine problems. Investigations have shown the majority of patients who have a first episode of low back pain (LBP) will go on to have more than one episode. 9 Several studies have determined that about a third of patients experiencing an acute LBP episode progress along a trajectory towards developing chronic LBP.10,11 Some estimates have been as high as 75% of patients being shown to suffer from their pain 1 year after a LBP episode. 12 The reality is that in clinical practice, the presenting patient is not reporting a first time incidence of LBP, but more likely a recurrent episode or exacerbation indicative of the common waxing and waning of an original back problem. 13
Chronic back pain has direct links to spine deformity and altered alignment.14–16 Several systematic reviews have unravelled the association and causative effects of biomechanical structural misalignments and their relationships to chronic LBP. For example, loss of lumbar lordosis and spondylolisthesis have both been shown to have direct biomechanical relationships to LBP.14–16 Importantly, these ‘biomechanical diagnoses’ are essential to uncover via radiography, and with modern spine rehabilitation methods, these conditions and others are treatable. In fact, the spine literature has provided an abundance of evidence clearly showing the close relationship between spine deformities (ie, subluxation displacements) with pain, disability and poor health-related quality of life measures.14–19
The spine literature has greatly advanced in the last 20 years. There are now well-established spine parameter thresholds that serve as treatment targets or structural goals of care.20–23 Surgeons who perform spine fusions use various radiography-measured biomechanical spinal parameters, and then follow best-practice guidelines to achieve improved spine and postural displacement positions within certain thresholds in order to prevent poor post-surgical outcomes. Accordingly, non-surgical musculoskeletal health care providers (eg, chiropractors, physiotherapists, etc.) also treat various spine deformities, and importantly treat patients who, without successful treatment, may regress to the point of becoming a surgical spine patient. With the evolution in both the understanding of the interrelationships between spine and pelvis parameters and how these are related to spine function and patient health, it is imperative to perform full-spine radiography to evaluate these relationships in the planning of contemporary spine-altering treatment regimens.
Several factions of spine care specialists, including surgeons, chiropractors and physiotherapists who specialize in spine altering treatments, universally stress the necessity and encourage initial biomechanical parameter assessment via radiographic screening.24–29 Thus, we argue that it is ethical to routinely image the spine in the initial assessment of spine patients as there are a multitude of benefits vs no risks. Herein, we outline why the traditional view of radiogenic cancer risk is outdated, dogmatic and not supported by the literature. We describe how this misinformation serves to perpetuate unnecessary fear and is a major obstacle to the universal acceptance of routine radiographic imaging in practice. Second, we outline how routine X-ray imaging of the spine leads to a multitude of benefits which include: 1. Biomechanical diagnosis (ie, by using contemporary metrics); 2. Avoiding delayed or outright missed diagnoses; 3. Making timely referrals to appropriate specialists; 4. Cost savings by avoiding unnecessary costly advanced imaging (eg, MRI); 5. Satisfying the patient.
Part I. Radiation Fear-Mongering and Cancer Risk Misinformation
Many recent chiropractic guidelines and opinion commentaries have reiterated the disuse of routine X-ray imaging for the initial assessment of LBP patients as well as the re-assessment of patients following care.4–8 The perceived risk stems from the ionizing radiation, presumed to be associated with the potential of inducing future cancers. 30 There are, however, scientific flaws and logical misrepresentations associated with this traditional and long-held perception.
Recent evidence has come to light showing that the critical events leading to the eventual adoption of a linear-no-threshold (LNT) model of cancer risk assessment was attributed to poor study design and unethical scientific misconduct by Hermann Muller, the Nobel prize winning geneticist. 31 Historical documents reveal that leading up to his famous Nobel lecture advocating for the use of the LNT model for radiation risk assessment, he was conflicted between the smooth path forward ensuring his continued funding from the Rockefeller Foundation vs his ethical obligations to the scientific community to expose possible scientific misconduct of recent studies that supported the LNT by entities involved in the granting of the funding he was receiving. 32 In a series of papers, Calabrese et al prove that Muller misled the scientific community in his famous Nobel Prize lecture, that represented a monumental event leading to the world-wide adoption of the LNT radiation risk assessment model. 33
The LNT model is more of a convenience model than a scientifically accurate model of radiation exposure.34,35 LNT theory assumes that high-dose radiation exposures and the corresponding physiological effects are related linearly; from high exposure down to zero exposure. Belief in the LNT theory assumes that all ionizing radiation is harmful (carcinogenic), and that it is also cumulative (dose additivity). 36 Problematically, neither assumptions are true. First, there exists no data supporting low radiation doses (<200 mrem) causes cancer. In fact, there are hundreds of studies that show the opposite. 37 In fact, the LNT is not supported by modern radiation biology. 38 Ironically, the LNT projects radiation damage down to the smallest exposure approaching the zero exposure, but the model is unrealistic as a zero-exposure environment does not exist. 39 All humans are constantly bombarded with radiation from many sources on a daily basis including background radiation.
Background radiation mostly comes from terrestrial and cosmic sources and no human can escape this exposure. If the LNT was an accurate model of cancer risk, then humans exposed to greater amounts of background radiation would have higher cancer and mortality rates, however, the reverse is true. David et al, for example, showed that there is a positive linear relationship between greater background radiation levels and increased life expectancy, and a negative linear relationship between greater background radiation levels and less cancer death rates, for both males and females. 40 Importantly, this study used data from 320 million people from 3139 counties in the US. They showed that life expectancy, considered the most integrative index of human health, was about 2.5 years longer for people living in higher background vs lower background radiation levels (>180 vs < 100 mrem/yr, p < .005). 40
The second assumption of the LNT, that all radiation exposure is additive is also false; in fact, if it were true, all people exposed to daily background radiation would eventually die from its accumulation and additive effects. The phenomenon of radiation hormesis is an alternate model of radiation exposure that graphically illustrates radiation exposures as having a ‘U’ shape. Low-dose radiation, but more than zero, has the most beneficial effects on physiology as opposed to both lower amounts and higher amounts. In other words, there is an optimal amount of radiation exposure that has been found to stimulate the body’s adaptive protection systems to repair any DNA damage caused.41–43 Lobrich et al 44 determined that DNA double-strand breaks (DSBs) occurs in humans after receiving a CT scan. The DSBs were seen to be self-repaired between 5-24 hours after the scan, and importantly, the body’s innate repair mechanisms repaired more than the original damage caused by the scan. In other words, the final DNA DSB count was less than the initial count prior to the scan. 44 It is now understood that the application of low-dose radiation can have positive effects on human health and can be used in the treatment of many human ailments, 45 as well as its demonstration of increased longevity as previously discussed. 40
A final consideration for this review is that compared to the very small amounts of radiation experienced from spinal X-rays, the fact is, our own body’s metabolism produces the greatest threat to our cells every day. Our metabolism produces endogenous reactive oxygen species (ROS) and hydrogen peroxide (H2O2) from aerobic metabolism46–48 (ie, breathing air) and incredibly, produces about 200 million times greater genetic damage than background radiation. 31 The radiation dose from plain film spinal X-rays are approximated to be within the range of background radiation levels that fluctuate depending on geographic region. Our adaptive repair systems, however, are so efficient that 99.99999% of the oxidative damage gets repaired. 31 Therefore, it is argued that the body’s repair mechanisms have evolved to not only repair radiation damage from minute sources, such as background radiation (or occasional X-rays), but rather to protect us from the unavoidable, endogenous damage from normal metabolism. 31 As we have previously argued, this point alone deems radiogenic cancer risks from spinal X-rays completely irrelevant 49 ; why don’t restrictive imaging guidelines warn people of the cancer risks of breathing air?
Part II: Neglecting Spinal X-Rays is Negligence – Advantages of Routine Imaging
Just as surgeons make better treatment choices based on biomechanical relationships between X-ray based spinal parameters, so too do spine rehabilitation practitioners. Le Huec and Roussouly, for example, state: “Spinal imbalance should be taken into consideration before initiation of any kind of treatment including conservative or surgical procedures.” 26
Despite many anti-imaging proponents claiming a lack of evidence to support X-ray-based non-surgical rehabilitation approaches,5–8 there is in fact an overwhelming literature base supporting spine-altering approaches in the sagittal plane for the cervical spine,50–65 thoracic spine66–74 and lumbar spine,74–81 and for the coronal plane in non-scoliotic spine deformities in the cervical spine, 82 thoraco-lumbo-pelvic region 83 and for scoliotic spine deformities.84–87 Further, one can argue that even non-spine altering approaches, such as spinal manipulative therapy (SMT), can be better planned for a specific patient with their unique spinal deviations and other X-ray diagnoses (degenerative changes, anomalies etc.) taken into consideration; occasionally these SMT methods are known to produce improvements in radiological outcomes on post intervention analysis. 62
The advantages of routine X-ray imaging in spine care include: 1. Biomechanical diagnosis (ie, by using X-ray metrics). 2. Avoiding delayed or outright missed diagnoses. 3. Making timely referrals to appropriate specialists. 4. Cost savings by avoiding unnecessary costly advanced imaging (eg, MRI). 5. Satisfying the patient. Here we consider each.
Biomechanical Diagnosis (ie, by Using X-Ray Metrics)
Traditional pain diagnoses do not help to dictate successful treatment approaches. For example, ‘low back pain,’ ‘sciatica,’ or ‘radiculopathy’ diagnoses are common but do not translate into identifying cause or best treatment options. Alternatively, diagnoses such as ‘lumbar spine hypolordosis,’ ‘thoracic spine hyperkyphosis,’ or ‘cervical kyphosis’ do translate into cause and effect; that is, can direct treatment selection unique to the patient. Each of these biomechanical diagnoses can be quantified and then be targeted with patient-specific treatment to improve the respective spine displacement or deformity.
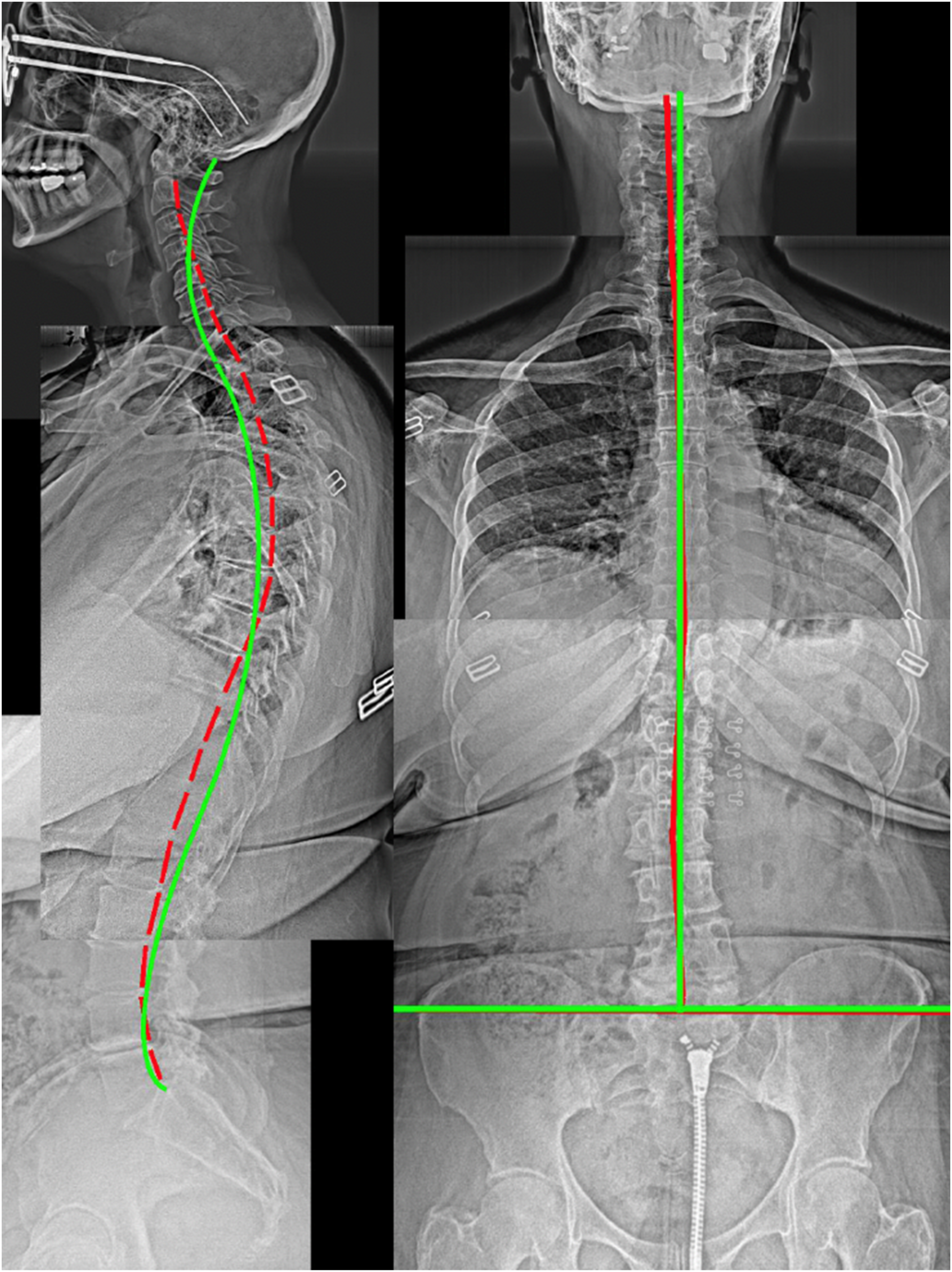
We emphasize the use of biomechanical diagnoses by presenting 5 consecutive patients from the first author’s spine clinic. Figures 1-5 illustrate how each individual can be diagnosed with specific biomechanical subluxation/displacement patterns that correlate to each respective patient’s symptoms and functional abilities, and although not presented here, each were treated with patient-specific approaches based on their unique spine patterns. After inspecting Figures 1-5, it becomes clear that patients can be quickly diagnosed biomechanically, either to have or not have particular biomechanical relationships in their neutral standing position. Clinically, this essential biomechanical information can only be efficiently attained via the mensuration of standing X-rays that range from the base of the skull down to the femur heads.
23
We reiterate here that this approach is definitively an evidence-based form of radiological based assessment and intervention.50–87 A 37-Year Old Concerned About His Posture and Hip Tightness. This Patient was Diagnosed With a Right Thoracic Lean, Right Head Translation, Increased Pelvic Tilt, Increased Sacral Base Angle, Lumbar Hyperlordosis, Thoracic Hyperkyphosis, Anterior Head Translation, and Cervical Hypolordosis. Note for Figures 1-5: Left: Stitched, Lateral Full-Spine Radiograph; Right: Stitched Anterior-Posterior Full-Spine Radiograph; Green line: Ideal Alignment; Red line: Patient Alignment A 32-Year Old Female With Chronic Back Pains (6/10). This Patient was Biomechanically Diagnosed With Scoliosis, Cervical Kyphosis, Thoracic Hypokyphosis, Increased Pelvic Tilt, Increased Sacral Base Angle and Lumbar Hyperlordosis A 46-Year Old Male With Chronic Neck and Back Problems Seeking Relief From Pain. This Patient was Biomechanically Diagnosed With Thoracic Hyperkyphosis, Posterior Thoracic Translation, Anterior Head Translation, Cervical Hypolordosis, and an Anatomical Leg Length Discrepancy An 83-Year Old Female Complained of the Inability to Straighten up was Told by Her Massage Therapist She May Have ‘Scoliosis.’ This Patient was Diagnosed With Severe Scoliosis, Severe Thoracolumbar Kyphosis, Anterior Head Translation, and a Reduced Sacral Base Angle. Note the Right Lateral-Listhesis of L4 on L5 A 64-Year Old Female With Chronic Neck and Back Pains Averaging 8/10. This Patient was Diagnosed With Lumbar Scoliosis, Right Head Translation, Upper Thoracic Hyperkyphosis, Lower Thoracic Lordosis, Anterior Head Translation, and Cervical Hypolordosis



Biomechanical X-Ray Parameter Thresholds Reported in the Literature as Treatment ‘Goals of Care.’

It is important to note that thresholds of spinal deformity for spine surgeons are likely greater than the thresholds for treatment of non-surgical manual therapists. 29 Indeed, patients resorting to surgical consult and subsequent surgery frequently have endured excessive suffering as many consider surgery as a ‘last option’. 29 Therefore, patients presenting with spinal misalignments whom suffer from pain, disability and functional limitations should be considered for non-surgical spinal rehabilitation, as the closer the spine and posture is to ‘ideal,’ the easier it should be to correct it. Logically, treating smaller deformities, if successful, would lead to the prevention of larger deformities and potentially invasive surgeries.
Avoiding Delayed or Outright Missed Diagnoses
The first point, biomechanical diagnosis leads to the second listed benefit of avoiding missed and delayed diagnoses. A spine patient who has not been adequately screened by standing X-rays remains, at least biomechanically, undiagnosed. With appropriate mensuration, virtually all patients will have biomechanical diagnoses from their radiographs (ie, Figures 1-5). As demonstrated in Figures 1-5, it can be logically anticipated that all patients will demonstrate unique biomechanical relationships of the spine and posture based on previous injuries, habits, occupations, etc.
We have determined that in a sample of 100 consecutive chiropractic-seeking patients, full-spine radiography revealed that all patients had clinical information gained from the X-rays that aided in customizing treatment procedures. 109 Further, regarding the diagnosis of specific spine deformities, depending on the thresholds used, large percentages were diagnosed with various spine misalignments associated with pathologies. Only 12% of the sample had an ideal cervical lordosis (between 29-42° measured from C2-7 posterior tangents) where 64% had a cervical neck curve straighter than 22° which correlates to the average value of chronic neck pain subjects. Forty-four percent had an anterior head translation (forward head posture) of greater than 25 mm which correlates with pain and disability. 89 Forty-two percent of the sample had a thoracolumbar offset from the vertical of greater than 25 mm, and 20% had a sagittal vertical axis imbalance greater than 50 mm, constituting adult spinal deformity (ASD). Fifteen percent had a complete cervical kyphosis, associated with an 18x likelihood of experiencing neck pain. 94
Beyond diagnosis on spine patients seeking care for their ailments, studies on healthy populations also show high percentages of abnormal X-ray findings. Studies on military personal, for example, have shown that high percentages of the population have radiographically diagnosable pathologic findings. Hald et al 110 found 97% of 11 000 ‘healthy’ air force recruits had pathologic findings on X-ray. Anderson et al calculated an average of 3.5 radiographically diagnosable anomalies, degenerative changes, and/or deviations of posture per screened person and suggested that due to this population being ‘highly selected’ the number may be much higher in a typical western society population. 111
An important logical point is that those who were previously treated without being X-rayed, and then sought out treatment from a provider who performed X-rays will have been a victim of a delayed diagnosis due to the avoidance of initial X-rays. There is an abundance of examples in the literature featuring previously ‘failed treatment’ as the examination of finally attained X-rays led to a biomechanical diagnosis, which in turn, appropriately led to a specific treatment for that specific biomechanical misalignment.112–117 The final analysis of avoiding initial X-rays is that it leads to ‘black box treatment’ 29 and therefore, spine misalignments that are not diagnosed will not get treated.
Making Timely Referrals to Appropriate Specialists
Urgent specialist referrals are appropriate when diagnosing certain rare medical conditions (eg, cancers, abdominal aortic aneurisms, etc.). Although anti-radiographic proponents argue that medical referrals based on diagnosing medically urgent ‘red flag’ diagnoses are rare, red flag screening tests are inherently known to have validity concerns (ie, false negative rates), 118 increasing the chances of missing a serious diagnosis and increasing clinician liability. Henschke et al, 119 for example, found a 1% incidence of serious pathology in 1172 consecutive patients. However, an alarming 80% of patients demonstrated ‘red flags,’ and 50% of the patients with serious pathology would have likely been missed without further imaging. Importantly, it was impossible for the physician to differentiate, during the initial consultation, which of the 80% (985/1172) of the sample having red flags actually had the more serious pathologies. 119
Chiropractic-specific studies have shown that so-called ‘rare’ serious pathologies may not be so rare. In regard to malignancies, Beck found an incidence of up to 3.1% in a sample of 847 full-spine patient radiographs (ie, 1 in 32). 120 Importantly, the frequency of malignancies as incidental findings are increasing as cancer rates are continuing to rise, 121 and cancer is a diagnosis that should not be missed. 122 Outside of malignancies, other serious pathologies are possible and have relatively high incidence rates. In the same study by Beck et al, 120 the incidence of fracture was 6.6% (1 in 15), abdominal aortic aneurysm was 0.8% (1 in 125), and atlantoaxial instability was 0.6% (1 in 167). All of these are ‘incidental findings,’ and clinically important pathologies that render physical manual therapies as an absolute contraindication. Professional referral to an appropriate specialist would better serve the patients interest.
Another consideration is that the biomechanical diagnoses obtained via radiography offers the opportunity to identify patients at risk for certain conditions based on spinal misalignments. Adolescent idiopathic scoliosis, for example, is often first noticed by the parent while coincidentally noticing asymmetries in their child’s back. Since scoliosis screening programs are frequently no longer endorsed, scoliosis is often missed. Problematically, larger curves are more difficult to treat, while smaller curves afford a better opportunity for a better outcome if diagnosed early in its development. 123 Other deformities such as thoracic hyperkyphosis, scoliosis, forward lean of the body (sagittal vertical axis), and ASD are associated with balance instability, 124 and patients with instability, particularly older patients, should be triaged for balance rehabilitation to prevent falls, injuries and deaths. 125
The universal proposition for the avoidance of initial X-rays (‘red flag only’ guidelines), are based on the low odds of finding serious pathology (eg, cancer, fracture, etc.). However, most chiropractic guidelines are simply a reiteration of medical physician LBP guidelines which provides guidance on the treatment of back pain mainly by pharmaceutical agents, not imparting manual forces directly onto the spine. Manual therapists, including chiropractors and physiotherapists offer fundamentally different treatments, and logically, should have unique considerations included into discipline-specific guidelines. In this section, we have argued that timely referral to appropriate specialists can be made when definitive information from radiographs are immediately available. As demonstrated, when images are not at hand, much opportunity is lost at the patient’s expense. An inconvenient reality for anti-imaging proponents is the fact that even when manual practitioners abide by X-ray restrictive guidelines, under-referring for X-rays are common. 126 In other words, when ‘red flags’ are present, many times the patient is not referred for imaging; this is very concerning. Initial routine imaging would eliminate this possibility.
Cost Savings by Avoiding Unnecessary Costly Advanced Imaging
Anti-imaging proponents argue that avoiding routine imaging helps to reduce health-care costs.6,7 In certain cases this may be true, but only by a marginal magnitude as plain film imaging is very cost effective and readily available. More importantly, routine plain film imaging leads to a large reduction in health care expenditures as it reduces or eliminates the need for higher cost imaging (eg, MRI, CT etc.). 127 In fact, the implementation of routine initial radiological spine screening would greatly reduce healthcare costs that are associated with more advanced imaging including CT and MRI.
Further, in the larger context of patient management, routine X-ray screening provides immediate and potentially critical information to assist in the guidance for treatment decisions regarding triage for advanced imaging (eg, MRI), for referral (eg, surgical and specialist consultation), prompting indications for co-management (rheumatologist and pain specialist), for ruling out or confirming a definitive diagnosis, for easing the anxiety of the patient, satisfying liability concerns of the practitioner and third party payors, and providing a timely diagnosis.128–130 Perhaps the latter point, providing a timely diagnosis (or non-diagnosis) culminates in the most healthcare savings as it prevents the lingering of patient diagnosis and treatment, and facilitates timely management.
Satisfying the Patient
The 3 arms of modern evidence-based medicine includes best research evidence, clinical expertise as well as patient values and preferences. 131 Unfortunately, patient values and preferences are often ignored in the triage of the patient encounter. 132 It must be pointed out, however, that patients who seek spine care expect a thorough examination that includes radiographic imaging.133–135 The classic Deyo study, for example, determined that 73% of patients expect x-rays for the diagnosis of their spine problem. 134 Jenkins et al 135 determined about half of all patients seeking care for low back pain consider imaging necessary. Satisfying patient needs involves fulfilling their expectations. It is established that patients are already more satisfied with chiropractic care, 136 but they are particularly satisfied when their beliefs are met by receiving radiographic imaging for their spinal problems.137–139
A frequently cited reference used to support the discouragement of routine radiography in LBP management is the Kendrick study.137,138 Ironically, Kendrick et al determined that two-thirds of all the patient radiographs were abnormal and also that 61% of patients who were followed for 9-months remained in pain. Importantly, the back pain patients who received imaging were more satisfied with the (ineffective) care they received. The study also found that patients allocated to a preference group, where the decision to receive lumbar radiography was made by them, achieved clinically significant improved outcomes compared to those randomized to a non-radiography or to a radiography group.137,138
Thus, it seems patients who are radiographically screened and given a certain diagnosis or non-diagnosis are more satisfied with the care they are provided, regardless of treatment effectiveness. Of course, critics would argue that reporting potential non-significant X-ray findings to a patient may lead to detrimental outcomes as the patient may cling to an image finding when it could be a coincidental and benign finding, we argue the onus is on the practitioner to realistically report X-ray results to the patient and its importance or particularly, its lack of importance as it would be unconscionable to not report radiographic findings regardless of the implications.
Discussion
Herein we described how there are no valid data to support use of LNT theory for the low-dose ionizing radiation exposures. Therefore, dose as a surrogate for risk in radiological imaging is not appropriate, and as argued previously, the use of the ‘as low as reasonably achievable ‘ (ALARA) concept in medical imaging is obsolete. 140 Regarding the ALARA concept, Oakley and Harrison 140 have described how the continued application of a false principle unnecessarily constrains healthcare professionals who attempt to deliver high-quality patient care and leads to the reluctance by doctors to order images, leads to a resistance from patients (or their parents) to receive images, leads to subquality images, leads to repeated imaging and increased radiation exposures, stifles use of low-dose radiation research and treatments (low-dose radiation therapy), and continues the endorsement of the ALARA principle. Tragically, it also propagates radiophobia; that is, the ubiquitous fear of X-rays. 30
The LNT model of radiation damage has been thoroughly discredited 141 and remains the universal cancer risk model for political and economic reasons, not for safety reasons. 142 We summarized how the 2 underlying features of LNT concept, linearity and additivity, are not true for the low-dose exposure region. Also, as discussed, breathing air is millions of times more harmful and we are not concerned with this. It is ironic that within literature debates between pro-imaging and anti-imaging proponents (‘red flag’ only use),5–8 the anti-imaging adversaries cannot address legitimate validity concerns over use of the LNT and the current radiobiological evidence that fails to support LNT.143–146
We summarized 5 clinically significant reasons supporting the use of routine imaging by spine care specialists including 1. Biomechanical diagnosis (ie, by using X-ray metrics), 2. Avoiding delayed or outright missed diagnoses, 3. Refer to appropriate specialist, 4. Cost savings by avoiding unnecessary costly advanced imaging (eg, MRI), and 5. Satisfy patient. All of these arguments individually support routine imaging; particularly as there are no radiation risks. Ultimately, we argue that the routine radiographic imaging approach has a risk-benefit profile of all benefit, no risk.
Regarding biomechanical diagnosis and X-ray cut off metrics that are reported in the scientific literature (Table 1), there is often conflicting evidence reported in the literature. For example, the 2018 systematic literature review with meta-analysis by Guo et al 147 reported that there is no difference in radiographically measured cervical lordotic values between patients with chronic neck pain compared to asymptomatic controls. Problematically, this highly cited publication is fraught with a disturbing scientific error. Guo et al 147 inappropriately cited and included the Harrison et al 1996 88 investigation as a case control of asymptomatic vs neck pain patients when in fact this manuscript did not report such data. Guo et al failed to properly identify the Harrison et al 2004 97 investigation as the correct case control to be included in their analysis even though they did include this reference in their asymptomatic data analysis. This gross oversight let to the incorrect conclusion regarding an abnormal reduced cervical lordosis as a significant predictor of neck pain. In contrast, the 2024 systematic review and meta-analysis by Kim et al 148 properly evaluated the 2004 Harrison et al 97 case control investigation in their analysis and found that patients with neck pain have a statistically relevant reduced cervical lordosis on X-ray. Thus, the challenge becomes which lens a clinician and/or researcher chooses to look through when making informed decisions regarding the scientific evidence supporting or refuting radiographic investigation of a patients spine. While there exists evidence to the contrary to that reported herein, the current authors argue that the prevailing literature continues to support the use of spine radiography to analyze, diagnose, and treat patient disorders.149–151
Recently, anti-imaging proponents have published studies concluding that imaging did not result in altering the outcome in patient care.152,153 These studies, however, are setup for imaging to fail from the start; in other words, the main flaw is that the X-rays were not used for the gain of biomechanical information to dictate a patient-specific treatment approach to exactly alter the patients abnormal alignment towards normal. Radiographic imaging does little to alter an approach consistent with gross spinal manipulation. Obviously, as opposed to the misuse of routine imaging152,153 an approach to routine imaging applies to clinicians who offer treatments that alter spine deformities,50–87 and it is time that current spine pain guidelines outline triage pathways that highlight the unique needs of practitioners specializing in spine and posture correcting methods.
Conclusion
Current understanding of the relationship between different spinopelvic parameters are essential to plan biomechanically appropriate interventions that are patient-specific. There are radiographically measured parameter thresholds critically related to several spinal disorders and positive patient outcomes. Current guidelines must include a caveat for contemporary biomechanical evaluation and its consequent specific treatments and should recommend routine radiographic imaging for spine patients undergoing corrective rehabilitative interventions. The failure to radiographically diagnose spinal deformity is argued to be negligence in many cases. The prime obstacle to routine X-ray imaging lies with the presumed threat of cancer, however, this is dogma.
Footnotes
Acknowledgement
We acknowledge the patients who consented to the presentation of their X-rays as used in Figures 1-![]() .
.
Author Contributions
PAO created the first draft of the manuscript; all authors reviewed, edited and consented to the publication of the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funds from CBP NonProfit, Inc.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: P.A.O. is a compensated consultant for Chiropractic BioPhysics, NonProfit, Inc J.W.H. is a compensated researcher for CBP Non-Profit, Inc D.E.H. is the CEO of Chiropractic BioPhysics® (CBP®) and provides post-graduate education to healthcare providers and physicians. Spine rehabilitation devices are distributed through his company. D.E.H. is the president of CBP Non-Profit, Inc, a not-for-profit spine research foundation.