
Abstract
Background:
Upper-extremity limb loss has been associated with serious psychological sequelae. Despite advancements in surgical procedures and prostheses for upper limb amputees, it is critical to recognize the psychosocial component of these patients’ care. Although the role of psychological factors in outcomes is increasingly acknowledged, little is known about the prevalence of depression and post-traumatic stress disorder (PTSD) in the civilian population after traumatic upper-extremity amputation.
Methods:
In this retrospective observational single-center study, adult patients evaluated for traumatic upper limb amputations from 2016 to 2019 completed the Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire, Visual Analogue Scale, the Center for Epidemiologic Studies Depression Scale, and the Primary Care PTSD Screen during visits. All data underwent descriptive statistical analysis.
Results:
Thirty-nine adult patients treated for upper-extremity traumatic amputation completed patient-reported outcomes (PROs) questionnaires. The median final follow-up time for our cohort was 17 months from amputation. Twenty patients (51%) screened positive for depression and 27 (69%) for PTSD during follow-up. The median time from amputation to first positive screening was 6.5 months for depression and 10 months for PTSD. The physical component score of Veterans RAND 12-Item Health Survey (VR-12) was significantly worse for patients with depression. The Median DASH and mental component score of VR-12 were significantly worse for patients with PTSD.
Conclusion:
Upper-extremity limb loss has a significant impact on mental health, which in turn affects PROs. The high prevalence of depression and PTSD in traumatic upper-extremity amputees underscores the necessity for screening and multidisciplinary treatment.
Introduction
Upper-extremity traumatic amputations constitute some of the most disabling injuries treated by orthopedic and upper-extremity surgeons. Although the surgical care of upper-extremity traumatic amputation is continually improving and has seen some significant advances in recent years, from targeted muscle reinnervation (TMR) and regenerative peripheral nerve interface for neuroma prevention to ever-more sophisticated myoelectric prostheses,1-3 the importance of psychological recovery is increasingly being recognized as affecting patient-reported outcomes (PROs) and meaningful functional outcomes such as return to work. Depression and post-traumatic stress disorder (PTSD) are two well-known psychiatric conditions commonly afflicting the orthopedic trauma population, with up to one-third of patients being affected. 4 A fairly high prevalence has been reported in the military population, with 21.2% of military patients with combat-related upper-extremity amputations experiencing PTSD and between 6% and 36% of patients experiencing depression, depending on the criteria used. 5 Orthopedic injuries to the upper extremities in general have been associated with greater disability and impact on quality of life than other areas of the musculoskeletal system, especially when the dominant arm is involved. 6 There is a growing awareness that psychological factors play a key role in the disability that results from orthopedic injuries, and 1 meta-analysis suggests that psychosocial factors are more closely associated with disability than are physical measures of impairment in the upper extremity. 7 Depression and PTSD in particular have been associated with a decreased rate of returning to work and therefore functional reinsertion into society. 8 Traumatic amputations often affect patients who are otherwise healthy, such as young adult men who do not routinely interact with the medical field. 9 The surgeon treating these patients may be the first medical provider to be involved in their care and the only provider following them in the long-term. 10 It is therefore of utmost importance that surgeons recognize associated psychiatric comorbidities in this patient population to facilitate proper referral and treatment. Previous studies have reported on the prevalence of depression and PTSD in the military and civilian polytrauma patients, peripheral nerve injuries, brachial plexus injuries, and complex hand injuries.11-13 However, little has been reported regarding the prevalence of depression and PTSD following upper-extremity amputation in the civilian population. 10
The purpose of this study is to evaluate the prevalence of depression and PTSD in adult civilian patients with upper-extremity traumatic amputations. Armed with a better understanding of the psychologic comorbidities after such injuries, clinicians can better screen, treat, and refer patients.
Materials and Methods
Following institutional review board approval, patients sustaining a traumatic upper-extremity amputation were identified through 10th revision of the International Statistical Classification of Diseases and Current Procedural Terminology codes for major limb amputation since the inception of our dedicated upper-extremity amputation clinic in 2016. All adult patients >18 years of age with traumatic upper-extremity amputations requiring surgery from 2016 to 2019 were included; patients <18 years of age, amputations secondary to medical conditions, and patients with a previous history of either depression or PTSD and/or preinjury use of antidepressant medications were excluded.
At each clinic visit, patients were asked to complete the Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire, Visual Analogue Scale for Pain (VAS), Center for Epidemiologic Studies Depression Scale (CES-D), and the Primary Care PTSD Screen (PC-PTSD). Secondary data obtained from medical records included age (years), sex (male or female), mechanism of injury (crush, avulsion, sharp, or blast), hand dominance (dominant or nondominant), side of injury (left or right), and medication use (narcotics [yes, no], Neurontin [yes, no], Lyrica [yes, no]). Study data were collected and managed using REDCap (Research Electronic Data Capture) electronic data capture tools hosted at OrthoCarolina. All data underwent descriptive statistical analysis using SAS version 9.4 (SAS Institute, Cary, North Carolina; http://www.sas.com/software/sas9). Standard descriptive statistics were reported, including measures of central tendency, variance, as well as frequencies and proportions. For bivariate analyses, χ2 or Fisher exact tests were used for categorical data to determine statistical differences. Student t test was used to compare normally distributed interval or continuous variables, and the Wilcoxon rank-sum test was used for nonparametric data.
Patients were determined to screen positive for depression or PTSD based on the results of the CES-D and PC-PTSD scales, respectively. Bivariate analysis was performed to identify variables that are associated with the prevalence of these conditions.
Results
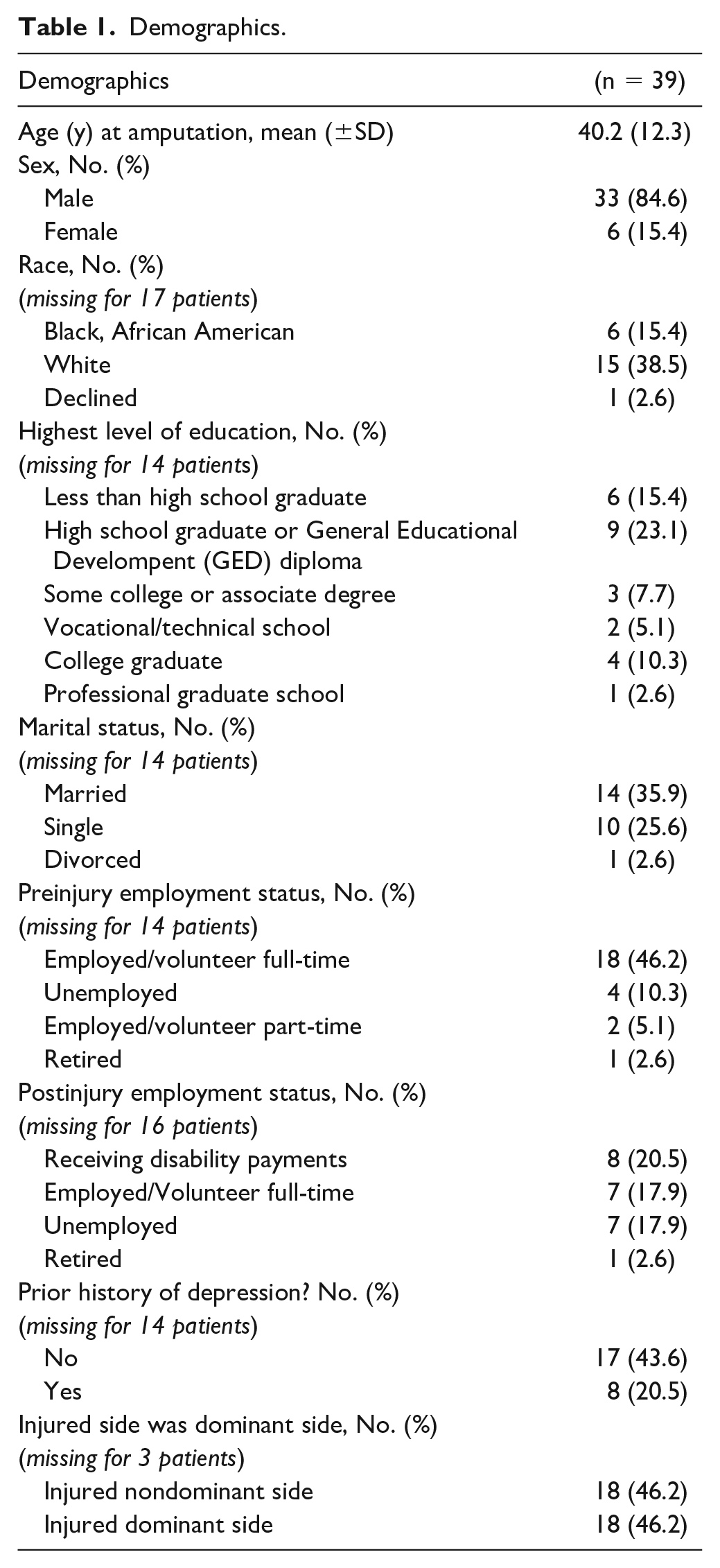
Between 2016 and 2019, 39 patients identified through our dedicated upper-extremity amputee clinic underwent surgical intervention for traumatic upper-extremity amputation and met all other inclusion criteria. There were no inclusion criteria beyond being aged >18 years and having sustained a traumatic upper-extremity amputation. Amputations for medical reasons (eg, infection, necrosis) were excluded. The median time from amputation to final follow-up was 17 months. Patient demographics are summarized in Table 1. In this cohort, the mean age at the time of amputation was 40.2 years (18-69 years), and 33 (84.6%) patients were men. The injured side was the dominant side in 46.5% (n = 18) of patients. Amputations were at the level of the hand in 53.8% (n = 21), transradial in 33.3% (n = 13), and transhumeral in 12.8% (n = 5) of cases. Sixty-seven percent (26 of 39) were workers’ compensation (WC) cases. In all, 38.5% (n = 15) had a TMR procedure and 25.6% (n = 10) had a Starfish procedure.
Demographics.
During the follow-up period, 51% (n = 20) of patients screened positive for depression according to their CES-D/CES-D–Revised score, and 69% (n = 27) of patients screened positive for PTSD.
The median (interquartile range [IQR]) time from amputation to first positive depression screen in the office was 6.5 (2-17) months. The median (IQR) time from amputation to first positive PTSD screening in the office was 10 (2-25) months.
Among patients with a transradial amputation, 69.2% (n = 9) screened positive for depression, and 84.6% (n = 11) screened positive for PTSD. Among patients with a partial hand amputation, 47.6% (n = 10) screened positive for depression, and 66.7% (n = 14) screened positive for PTSD. These results were not statistically significant. Workers’ compensation status was significantly correlated with depression (P = .019) but not PTSD (P = 0.486), although the results trended in that direction (Table 2).
PTSD/Depression Stratified by Worker’s Compensation.
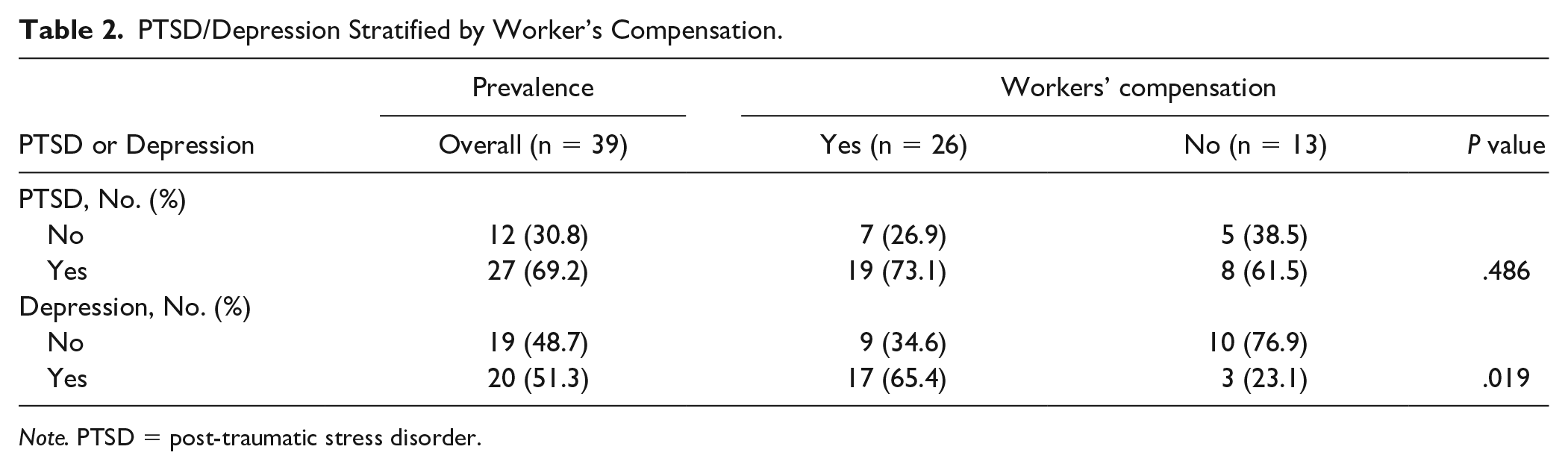
Note. PTSD = post-traumatic stress disorder.
Patient-reported outcomes are summarized in Tables 3 and 4. The VAS (median) was 4.6, and the total DASH (mean) was 44.2 for the entire patient cohort.
PROs at Initial Visit Stratified by Depression.
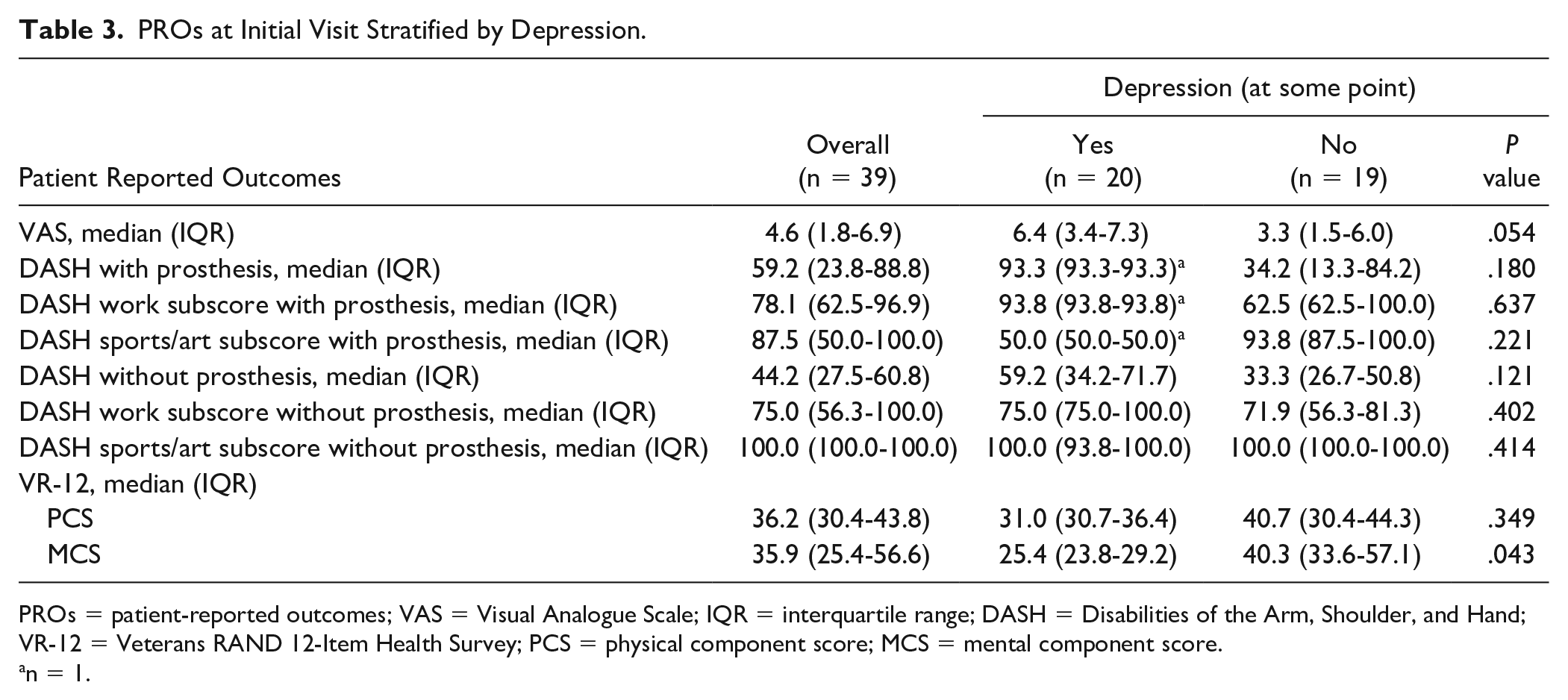
PROs = patient-reported outcomes; VAS = Visual Analogue Scale; IQR = interquartile range; DASH = Disabilities of the Arm, Shoulder, and Hand; VR-12 = Veterans RAND 12-Item Health Survey; PCS = physical component score; MCS = mental component score.
n = 1.
PROs at Initial Visit Stratified by PTSD.
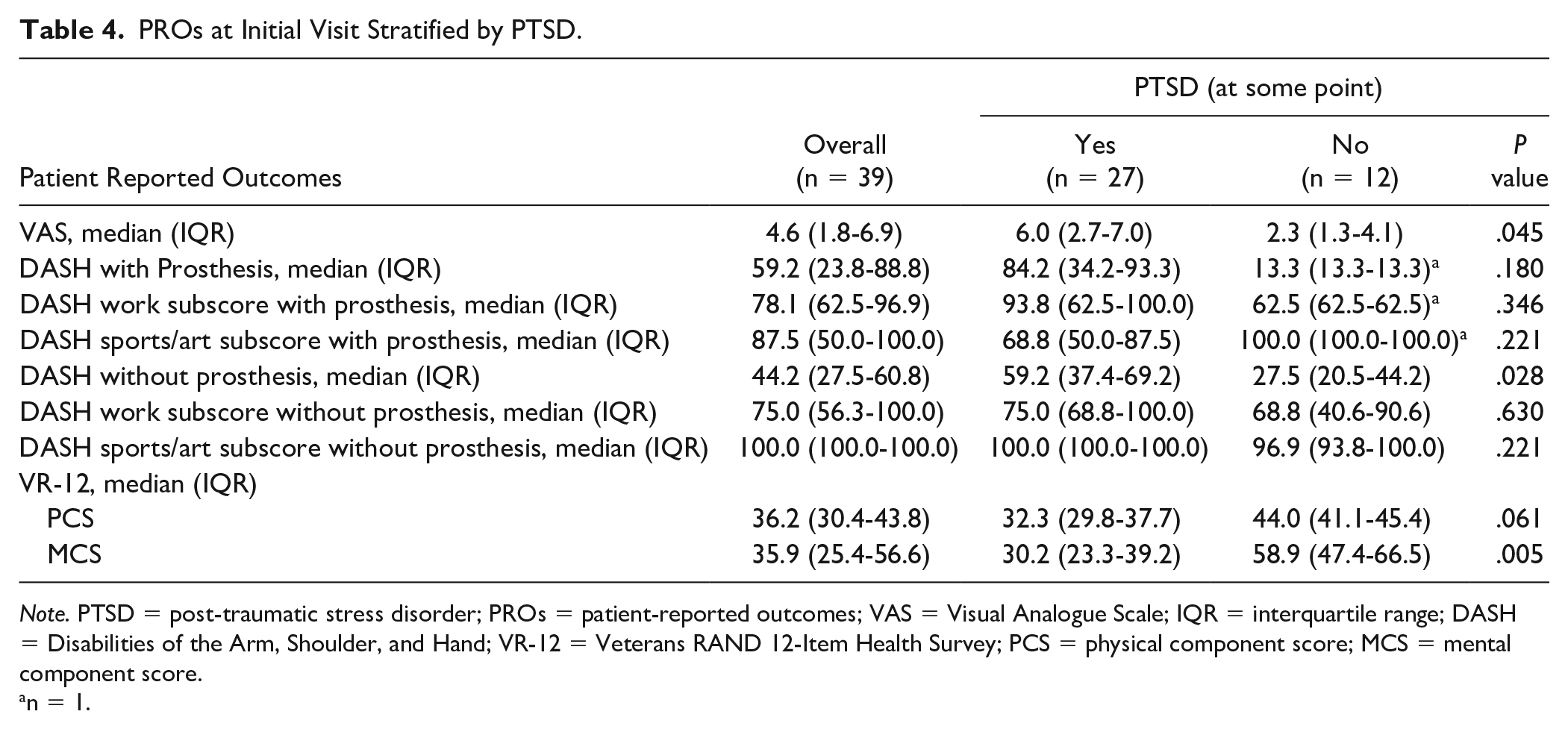
Note. PTSD = post-traumatic stress disorder; PROs = patient-reported outcomes; VAS = Visual Analogue Scale; IQR = interquartile range; DASH = Disabilities of the Arm, Shoulder, and Hand; VR-12 = Veterans RAND 12-Item Health Survey; PCS = physical component score; MCS = mental component score.
n = 1.
When comparing PROs of patients who had scored positive for depression with those who had not in Table 3, there was a statistically significant difference in the mental component of the Veterans RAND 12-Item Health Survey (VR-12) of 25.4 versus 40.3 (P = .0043) and a nonstatistically significant trend toward worse VAS of 6.4 versus 3.3 (P = .054), DASH of 59.2 versus 33.3 (P = .121), and the physical component score (PCS) of VR-12 of 31 versus 40 (P = .349).
When comparing PROs of patients who had scored positive for PTSD with those who had not in Table 4, there was a statistically significant difference in median DASH score (59.2 vs 27.3, P = .028) and VR-12 mental component score (30.2 vs 58.9, P = .05). The difference in VR-12 PCS (32.3 vs 44) did not reach statistical significance (P = .061).
Discussion
Depression and PTSD are serious psychiatric diagnoses that significantly impact patients’ quality of life, likelihood of returning to work, and overall function. There are few previous data on the prevalence of these conditions in civilian patients with operatively treated upper-extremity traumatic amputations. In this study, we report on the prevalence of depression and PTSD in a homogeneous civilian population of surgically managed patients with upper-extremity amputations secondary to trauma.
In our cohort, there appears to be a high prevalence of these 2 conditions, with almost half screening positive for depression at some point in their postoperative clinical care and two-thirds of patients screening positive for PTSD. These rates were higher in more proximal-level amputees. There is also a significantly higher rate of depression in patients with a WC status. The first instance of positive screening for either depression or PTSD does not appear to cluster around a particular time point, with our data showing wide variability in time to psychiatric diagnosis. These results argue for continuous monitoring over time in all patients.
Diagnostic criteria for depression are derived from the Diagnostic and Statistical Manual of Mental Disorders (DSM) and typically combine a depressed mood with loss of pleasure or interest (anhedonia) and a number of behavioral changes and functional impairment in sleep, appetite, energy levels, and cognitive domains such as concentration. The PTSD is a disorder that may develop after exposure to trauma, defined in DSM-5 as “actual or threatened death, serious injury, or sexual violence.” The PTSD symptoms may include reexperiencing, numbing, hyperarousal, and avoidance.
A previous study of the psychological well-being of patients with upper-extremity limb loss which included both traumatic and nontraumatic etiologies found a comparable prevalence of depression (54.8%) but a significantly lower rate of PTSD (23.6%). 14 This difference may highlight the fact that although traumatic and atraumatic amputees can appear similar from a functional standpoint, their needs may differ when trying to optimize their overall rehabilitation. In addition, the aforementioned study found a higher rate of depression and PTSD in patients with partial hand amputations compared with more proximal levels of limb loss, which was not the case in our population.
Our study has several limitations. First, the sample remains relatively small (N = 39), although this remains a relatively large study within the existing literature of surgically managed civilian traumatic upper-extremity amputations. Nonetheless, despite the small sample size, the data unambiguously reveal that this population is at high risk of psychiatric comorbidities. The second limitation is that depression and PTSD are measured in a binary fashion and reported as being present at any time point throughout the patients’ follow-up. It would be interesting and of value to understand how the severity of psychological symptoms varies over time and whether certain interventions such as receiving a prosthesis, undergoing secondary surgery, or receiving psychiatric care has an effect. Third, our study did not establish any clear demographic risk factors for the development of depression or PTSD within our patient population, with the exception of WC status for depression. A larger sample size would be needed to discern statistically significant patterns of risk factors and protective ones. However, given the overall high prevalence, it is likely prudent to assume that all patients with a surgically treated upper-extremity traumatic amputation are at risk and should be screened.
We found the prevalence of depression and PTSD in our cohort of adult civilians with traumatic amputations treated surgically to be higher than previous reports in the military population or in cohorts of patients that included atraumatic amputations for medical conditions. Therefore, surgeons taking care of this patient population need to have a high index of suspicion for significant psychiatric comorbidities. Universal screening of patients in clinic with validated scores for depression and PTSD such as CES-D and PC-PTSD is recommended. In our own center, we have found it beneficial to establish a multidisciplinary clinic environment on a monthly basis for all upper-extremity amputees, with a clinical psychologist, occupational therapist, and prosthetist on site. In addition to facilitating patients’ care, it normalizes their experience and may decrease the stigma associated with psychological suffering. In the future, rather than focusing on the binary presence or absence of a psychiatric diagnosis, recognizing the spectrum of psychological suffering and its impact on recovery will likely benefit virtually all patients after upper-extremity limb loss.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Informed Consent
Informed consent did not need to be obtained from the participants of this study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.C.T. and R.R. declare that they have no conflict of interest. B.L. has received consulting fees from Hanger Clinic. G.G. has received royalties and consulting fees from Biomet and consulting fees from BME, Hanger Clinic, Integra, Restor3d, and Stryker; was a paid presenter or speaker for DePuy, Endo Pharmaceutical, Integra, and Zimmer; and is a member of the American Association for Hand Surgery and American Society for Surgery of the Hand, and is also on the editorial board of Journal of Hand Surgery.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.