
Abstract
Despite the high prevalence of weight bias among fitness professionals, few resources are currently available to educate fitness professionals about weight bias and no systematic review of weight bias interventions has been conducted among this population. This paper therefore reviewed extant weight bias interventions for fitness professionals to inform future weight bias-reduction initiatives. Seven reports comprising six studies were identified from inception until April 2024. Findings showed small to large improvements in explicit weight bias, particularly on the weight control/blame component. No improvements were observed in implicit weight bias. The results show an urgent need to bridge the gap between the resources currently available in the fitness industry and those developed by the scientific community and to develop novel multifaceted interventions that draw from multiple theories of attitude and behavior change to effectively tackle weight bias among fitness professionals.
Keywords
Introduction
Weight bias (i.e., negative attitudes toward, and beliefs about, others because of their weight or size; Alberga et al., 2016; Puhl & Brownell, 2013) is highly prevalent across the globe and represents a significant public health and social justice issue (Nutter et al., 2018; Puhl et al., 2021). Research shows that weight bias harms individuals’ physical and psychological health and well-being. For example, individuals who experience weight stigma are more likely to report poor body image and body dissatisfaction, low self-esteem, feelings of worthlessness and loneliness, anxiety and depression, suicidal thoughts and acts, maladaptive eating patterns, avoidance of physical activity, and avoidance of medical care and worse care (Bombak, 2015; Sonneville et al., 2024; Zhu et al., 2022). Despite its detrimental impact, research shows a high prevalence of weight bias and weight stigma across a wide range of domains, including the workplace, healthcare facilities, educational institutions, mass media, and among fitness professionals working in the fitness industry (Côté & Bégin, 2020; Panza et al., 2018; Puhl et al., 2021; Zacher & Von Hippel, 2022).
Fitness Professionals: Definitions and Overview of the Industry
The term “fitness professional” inconsistently includes a broad range of occupations and generally refers to any person whose role is the prescription of movement or exercise. Within that broad range, fitness trainers, personal trainers, and gym instructors have received limited research attention, in part because unlike physical education (PE) teachers, physiotherapists, and sports coaches, they practise mainly within the private sector and are primarily driven by commercial interests (De Lyon et al., 2017). The education pathways for fitness professionals vary significantly, and despite a few crossovers with the healthcare industry (e.g., physiotherapy), they are also vastly different from the education and qualification requirements of health professionals.
For example, the minimum qualification requirements for a fitness instructor in the United Kingdom are equivalent to five GCSEs 1 graded A*–C/9–4 (Lloyd & Payne, 2013), and education for fitness professionals can vary from one to three years of study in higher-level education institutions to 2–12 weeks of training taken prior to employment (Lloyd, 2008). Similarly, in the United States, there are no legal education requirements to be a fitness instructor or personal trainer, although a high school diploma is often required to work in the fitness industry (Akerson, 2014; Melton et al., 2008; Thompson, 2023; Tomko, 2019). More advanced education pathways vary significantly from shorter certifications that can be completed in days or weeks to longer specialization courses and higher education degrees (Tomko, 2019).
These differences are important to consider, as fitness trainers, personal trainers, and gym instructors operate in largely unregulated spaces dominated by the beauty and diet industries. For example, gymnasiums, or gyms, as well as other similar spaces for physical activity and exercise, are environments where bodies are typically on display, thus increasing appearance comparisons and self-objectification (Prichard & Tiggemann, 2008). Further, the motivations of both fitness professionals and the people who attend these spaces are often extrinsic, specifically, appearance based (O’Hara et al., 2014). Given that fitness professionals differ from healthcare professionals with regard to education, qualifications, and work roles (De Lyon et al., 2017; Lloyd & Payne, 2013), it is important to explore which intervention approaches are most effective for this unique group, such that more specific recommendations can be made for future interventions.
Although the public health sector and fitness industry have remarked on the role of fitness professionals as a health promotion asset (Lloyd & Payne, 2013; Thompson, 2023), there is currently mistrust and lack of confidence among healthcare professionals, given that very little is known about fitness professionals’ qualifications and capacity to effectively contribute to the healthcare sector (De Lyon et al., 2017). Fitness professionals routinely act as teachers, trainers, counselors, coaches, and nutritionists (McKean et al., 2015; Melton et al., 2021; Mitchell et al., 2021; Sass et al., 2007). Importantly, fitness professionals often work with diverse population groups, including individuals with specific health-related needs such as people with eating disorders, diabetes, and other concerns (De Lyon et al., 2017). Although many countries and organizations provide a scope of practise for fitness professionals aiming to work with such populations, strict regulations regarding taking on additional roles often do not exist (Melton et al., 2021; Mitchell et al., 2021).
Weight Bias in the Fitness Industry
Fitness and movement settings are especially saturated with weight bias, and research consistently shows high implicit and explicit weight biases among fitness professionals (e.g., gym and fitness instructors, personal trainers; Panza et al., 2018; Zaroubi et al., 2021). Implicit weight bias refers to the unconscious attitudes or stereotypes fitness professionals may hold toward individuals in larger bodies, which can subtly influence their behaviors and judgments without their awareness (Robertson & Vohora, 2008). For example, a fitness professional might unconsciously assume that a larger client is less motivated, leading to less enthusiastic encouragement during workouts. Explicit weight bias, on the other hand, encompasses the conscious beliefs and attitudes that are deliberately expressed (Zaroubi et al., 2021). This can manifest in overt actions or comments, such as a trainer directly telling a client that they need to lose weight to be fit, or preferentially selecting leaner clients for advanced fitness classes.
The elevated levels of weight bias observed among fitness professionals can be attributed to a confluence of factors deeply ingrained in the industry's ethos. Traditional fitness education often emphasizes weight-centric paradigms, with a primary focus on weight management and aesthetics (Puhl & Wharton, 2007). This weight-centric approach not only perpetuates societal appearance norms and health inequities but also reinforces the prevalent misconception that body weight directly correlates with health (Rich & Mansfield, 2019; Tylka et al., 2014). Fitness professionals, whose qualifications are predominantly centred around these perspectives, may inadvertently internalize and perpetuate weight bias (Zaroubi et al., 2021). Indeed, studies have found that fitness professionals’ weight biases get stronger as they continue their education (Zaroubi et al., 2021) and spend more time in the industry (Whitehead, 2016).
The idealization of thinness in fitness spaces and among fitness professionals can create an unwelcoming atmosphere for individuals with larger body sizes, discouraging fat people from accessing, feeling comfortable in, and benefitting from these spaces (Argüelles et al., 2022; Flint & Reale, 2018; Thedinga et al., 2021). Please note that the term “fat people” has been used intentionally here instead of “individuals with overweight” or “individuals with obesity” as a way of reclaiming the terminology around fat bodies and reducing the stigmatizing associations with medical terms, such as “obesity.” Where “overweight” or “obesity” is mentioned hereafter as part of a study's findings, these terms are presented in quotation marks to acknowledge their stigmatizing connotation. It should be acknowledged that people differ in how they choose to describe their own bodies and some individuals may prefer to use other terminology (e.g., “higher weight,” “plus-size”). For a further discussion and review about the preferred terminology around weight, see Meadows and Danielsdottir (2016). In line with the above rationale, the term “fat” will be used throughout the remainder of this paper.
For example, fitness professionals who hold high levels of weight bias toward fat people are more likely to perceive fat people as uneducated, lazy, and lacking willpower, and therefore ultimately responsible for their fatness (Greenleaf et al., 2019; Meadows & Bombak, 2019). Further, they are less likely to consider and discuss risks associated with weight loss, and more likely to perceive weight loss as straightforward and achievable for everyone, rather than it being a function of biological, social, and environmental factors (Zaroubi et al., 2021). In addition to this, gyms and other fitness environments often provide additional barriers for individuals living in larger bodies, such as limited equipment options and implicit or explicit stigmatizing messaging in marketing and advertising materials (Argüelles et al., 2022; Myre et al., 2021). This, in turn, reduces the likelihood of fat people engaging in physical activities and benefiting from the positive effects of regular exercise (Harjunen, 2019; Schvey et al., 2017).
Findings from Previous Reviews on Weight Bias Interventions
Although a handful of previous reviews on weight bias interventions have included fitness professionals (Alberga et al., 2016; Moore et al., 2022), no reviews have been conducted specifically on this population, thus limiting conclusions and recommendations for this setting. For example, a systematic review by Alberga et al. (2016) including 17 studies of healthcare professionals, only included two studies that targeted fitness professionals, specifically, kinesiology students (Rukavina et al., 2008, 2010; these studies have also been included in the current review). Among all the included interventions, they identified four distinct approaches to weight bias reduction: (1) education about weight bias, stigma, and discrimination; (2) empathy-evoking activities; (3) self-awareness and reflection of one's own attitudes; and (4) influence of leaders and peers to change people's minds. However, the authors reported inconclusive evidence regarding the effectiveness of each approach (Alberga et al., 2016). An in-depth analysis is provided as part of this systematic review.
Similarly, Moore et al. (2022) conducted a systematic review and meta-analysis among healthcare professionals (e.g., healthcare workers, nurses, doctors) including 16 studies, only two of which targeted students in a subject area related to fitness and/or sports education (Jones & Forhan, 2021; Wijayatunga et al., 2019). The authors concluded that interventions targeting students are the most common and education on causality (i.e., what causes weight gain) and controllability (i.e., an individual's control over their weight) remains the most used approach to reducing weight bias attitudes (Moore et al., 2022).
A more recent scoping review of interventions to reduce weight bias among health and fitness professionals (De Paolis et al., 2023) identified 11 studies, only three of which targeted fitness professionals. The last search for this review was conducted in June 2022. Similar to previous reviews, De Paolis et al. (2023) found that interventions in education settings focusing on the uncontrollable causes of “obesity” were found to reduce the blame component of explicit weight bias, while those targeting weight bias through group discussions and reflective activities improved students’ awareness of their biases and provided opportunities for reflection on instances of bias within practical settings. Although Moore et al. (2022) reported improvements in the quality of papers published in this field, notable methodological weaknesses remain, namely a lack of long-term follow-up, high attrition, variability in the quality of measures used, and the absence of validated benchmarks of clinical significance (Alberga et al., 2016; De Paolis et al., 2023; Lee et al., 2014).
The Current Review
While the detrimental impact of weight bias and stigma in the fitness industry is widely recognized, there exists a notable gap in our understanding of effective interventions for mitigating these issues among fitness professionals. To our knowledge, no systematic review has specifically focused on the unique challenges and requirements of fitness professionals. Additionally, there is a strong argument to avoid segregating fitness professionals operating in gyms, health clubs, and other private spaces and to stop combining this group with professionals working in the healthcare sector. This review addresses this gap by: (1) identifying existing interventions that aim to reduce implicit and explicit weight biases among fitness professionals; (2) describing and evaluating the characteristics of these interventions that influence their effectiveness in reducing weight bias and related outcomes; and (3) providing recommendations to guide future research and intervention development targeting implicit and explicit weight biases among fitness professionals.
Methods
This systematic review was conducted in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement (Page et al., 2021) and was preregistered on PROSPERO (ref no. CRD42023467272) prior to commencement (3 October 2023). In line with calls for a “fat epistemology” (Cooper, 2016; Pausé, 2012, 2020) that centres the voices and experiences of fat people in any research conducted on the study of fatness, the fat body, and the fat experience (Manokaran et al., 2021), this review was conducted with three authors who identify as fat (BS, JS, PD). The authorship team further comprises researchers, fitness professionals, and activists who have body positivity and fat liberation activism experience (BS, PD); research expertise in body image and weight bias and the intersection between body image, weight bias, and movement (AT, EM, GW, JS, PD); experience of working in the fitness industry (BS, JS); public health and clinical nutrition expertise focusing on the Health at Every Size® (HAES®) framework and nondiet approaches (AT); and extensive knowledge and expertise in conducting systematic reviews (AT, EM, GW, JS, PD).
Data Sources and Search Strategy
Four strategies were used to identify studies for inclusion. First, we conducted a systematic computerized search for papers published from inception until 29 April 2024 using the following bibliographic databases: PsycINFO, PsycARTICLES, CINAHL Plus, AMED, MEDLINE, ERIC, SPORTDiscus (all accessed via EBSCO), ProQuest (dissertations and theses), and the Cochrane Central Register of Controlled Trials. Boolean combinations, alternative spellings, and abbreviations of the following search terms were used: (1) terms related to the target population (e.g., “fitness professional,” “personal trainer”); (2) terms related to the intervention (e.g., “randomized controlled trial,” “psychoeducation”); (3) terms related to bias (e.g., “bias,” “stigma”); and (4) terms related to body weight and size (e.g., “BMI,” “weight”). Second, backward citation searching was conducted to identify additional studies that met inclusion criteria, which was done by checking the reference lists of the included and excluded studies. Third, we reviewed “grey literature” (e.g., conference abstracts, dissertations) and searched for unpublished studies uploaded to PsyArXiv, SportRxiv, or registered on ClinicalTrials.gov. Finally, we invited authors from body image and fitness communities to provide studies via a mailing list. No date limits were used; however, searches were restricted to evaluations conducted in English (see Table S1, Supplementary Materials).
Study Eligibility Criteria
Studies were included if they: (1) evaluated interventions that specifically aimed to reduce implicit and/or explicit weight biases or related constructs (e.g., fat phobia, weight stigma, and antifat prejudice) among fitness professionals and (2) included an assessment of implicit or explicit weight bias or a related construct at baseline and postintervention (e.g., Anti-Fat Attitude Test [AFAT], Implicit Weight Bias Association Test [IAT], and Fat Phobia Scale). The term “fitness professional” encompassed any person who is teaching or instructing members of the public or general population (or specific target demographic, such as children or the elderly) to engage in movement for the purpose of well-being, leisure, or to promote an active lifestyle (e.g., gym and fitness instructors, personal trainers, PE teachers, sports coaches). This excluded people working solely with professional or elite athletes (e.g., high performance coaches). Studies were excluded if they did not target fitness professionals or combined data from fitness professionals with data from healthcare professionals or other participant groups (e.g., nurses, doctors).
Study Selection and Data Extraction
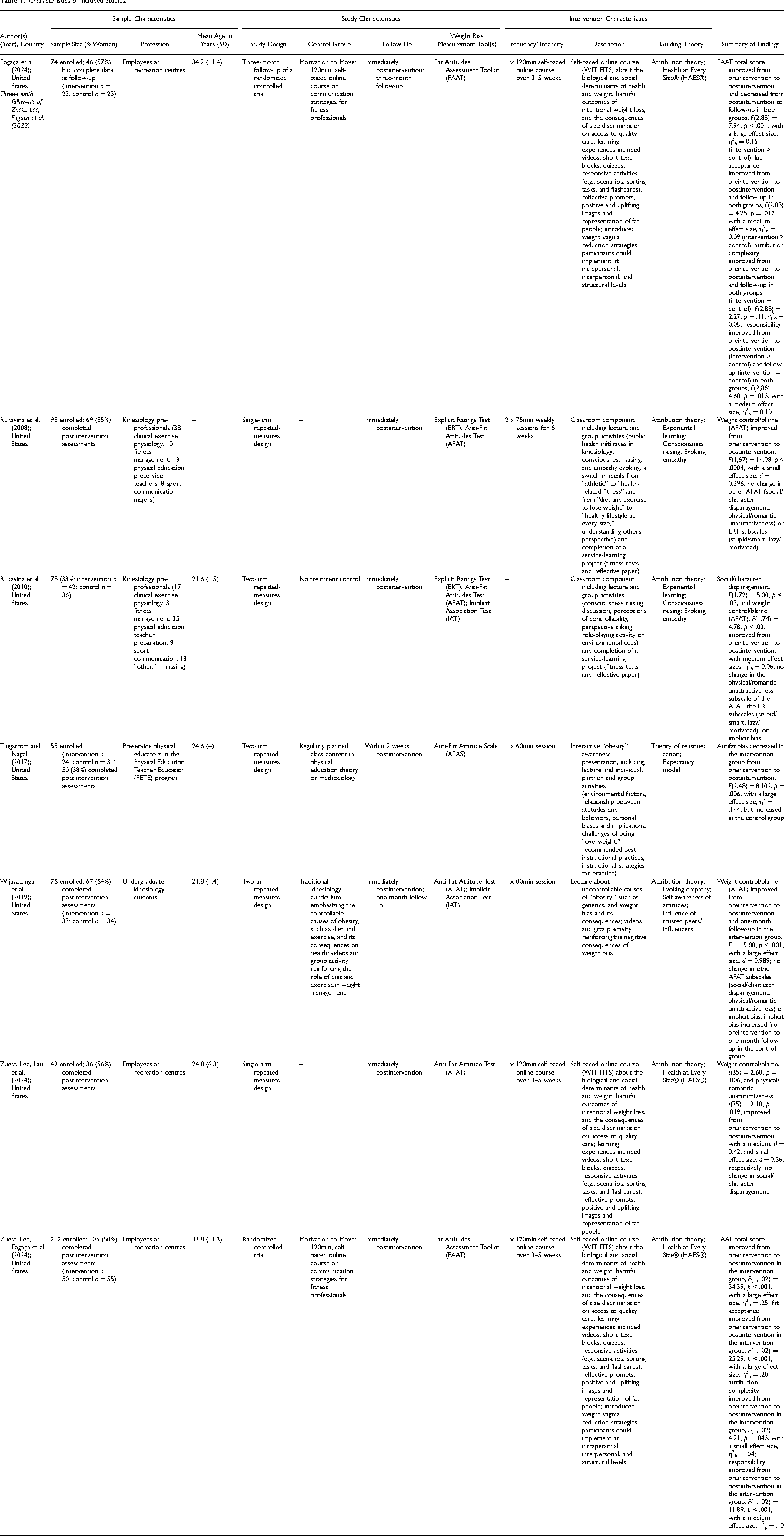
The lead author screened titles and abstracts of the retrieved papers against the above inclusion and exclusion criteria, with support from the second author. Duplicates and irrelevant papers were removed. Any disagreements in selecting the final papers for inclusion were resolved through discussion of uncertainties and clarifying eligibility criteria. Data extraction was completed by the first and second authors who cross-checked each other's extraction (see Table 1). For studies that described statistically significant outcomes, a p < .05 was considered significant.
Characteristics of Included Studies.
Quality Assessment
The quality of included studies was assessed using the Quality Assessment Tool for Quantitative Studies, developed by the Effective Public Health Practice Project (EPHPP; Thomas et al., 2004). The EPHPP allows for the assessment of publications across a wide range of health topics and various study designs (Jackson & Waters, 2005) and has proven to have fair interrater agreement for separate domains and excellent agreement for overall grade (Armijo-Olivo et al., 2012). The EPHPP provides an overall methodological quality rating of “strong” (no weak component ratings), “moderate” (one weak component rating), or “weak” (two or more weak component ratings), based on: (1) selection bias; (2) study design; (3) confounders; (4) blinding; (5) data collection methods; and (6) withdrawals and dropouts. The first and second authors independently assessed all studies. Cohen's kappa (Cohen, 1960) was calculated to determine interrater reliability, showing good agreement between subscale scores (88.1%; κ = 0.821, p < .001) and moderate agreement between total scores (85.7%; κ = 0.588, p = .088). Discrepancies were minor and were resolved through discussion.
Results
Paper Selection
The searches produced a total of 674 titles across databases, registers, and calls for papers. After removing 258 duplicates, the remaining 416 records went through a title and abstract screening for eligibility, of which 13 papers were sought for retrieval. One paper could not be accessed, and 12 papers were screened based on the full text. Of these, three papers did not target fitness professionals and two did not describe a weight bias intervention. The final sample comprised seven reports describing findings from six studies (see Figure 1).
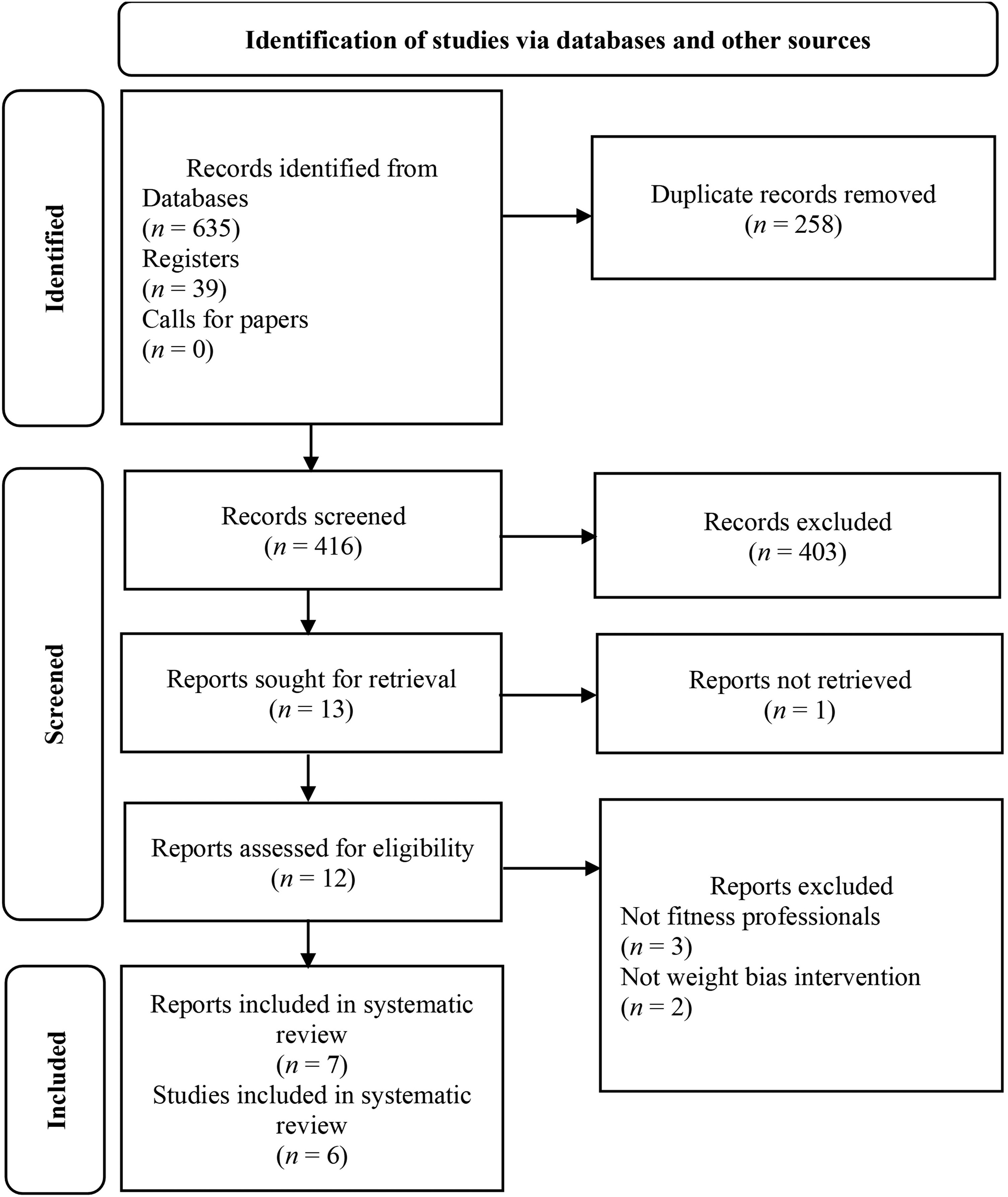
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart of study selection.
Characteristics of the Included Studies
A total of seven publications comprising six studies (single-arm repeated-measures n = 2, double-arm repeated-measures n = 3, randomized controlled trial n = 1) were included in this review. The double-arm studies used regular class content as the control condition (n = 2) or a control group from a different course (n = 1), while the randomized controlled trial used an active control condition (motivation techniques to promote physical activity). All studies were conducted in the United States with adult participants. Except for Fogaça et al. (2024), Zuest, Lee, Lau et al. (2024), and Zuest, Lee, Fogaça et al. (2023) whose participant samples comprised employees at recreation centres, the remaining four studies were conducted with kinesiology students or pre-professionals in different majors (e.g., clinical exercise physiology, fitness management, preservice PE teachers, sports communication). Sample sizes ranged from 42 to 105 participants.
Interventions ranged in delivery and length, with two papers detailing interventions comprising 12, 75-min sessions delivered over six weeks; two papers detailing single-session interventions ranging from 60 to 80 min in length; and three papers describing a 120-min online self-paced course. All interventions were delivered by experts. The content of the interventions for most studies targeted weight stigma toward adults, while Tingstrom and Nagel (2017) tailored the messaging for weight stigma toward children, given their intervention was aimed toward preservice PE school teachers. Most studies used attribution theory and empathy evoking as guiding theories. Other theories included consciousness raising, experiential learning, the theory of reasoned action, the expectancy model, self-awareness, influence of trusted peers/influencers, and HAES®. Regarding measures used to assess weight bias, the AFAT was the most frequently used scale, followed by the Fat Attitudes Assessment Toolkit (FAAT), Anti-Fat Attitude Scale (AFAS), Explicit Ratings Test (ERT), and the IAT. Only two studies included a follow-up assessment (one month, Wijayatunga et al., 2019; three months, Fogaça et al., 2024).
Study Quality
Six papers comprising five studies were rated as “weak” and one study was rated as “moderate” quality (Wijayatunga et al., 2019; see Table S2, Supplementary Materials). Studies were generally rated weak on selection bias (sample was not representative of the target population), confounders (studies did not control for relevant confounders in their analyses), and withdrawal and dropouts (low intervention and survey adherence and completion rates).
Study Findings
Explicit Weight Bias
The findings across the six studies consistently showed small to large improvements in explicit weight bias, specifically on the weight control/blame subscale of the AFAT from preintervention to postintervention (Rukavina et al., 2008, 2010; Wijayatunga et al., 2019; Zuest, Lee, Lau et al., 2024) and at one-month follow-up (Wijayatunga et al., 2019). Zuest, Lee, Fogaça et al. (2024) further observed improvements in fat acceptance, attribution complexity, and responsibility scores in the intervention condition, as measured by the FAAT at postintervention; however, improvements were only maintained in FAAT total scores and fat acceptance at three months (Fogaça et al., 2024). Further, both the intervention and control groups experienced improvements in fat attitudes from preintervention to postintervention, which dropped at three months, although attitudes diminished less in the intervention group, compared to the control group (Fogaça et al., 2024). Additionally, one study found an improvement in explicit weight bias from preintervention to postintervention measured using the AFAS (Tingstrom & Nagel, 2017). Findings were mixed regarding the other subscales of the AFAT. Zuest, Lee, Lau et al. (2024) found a small improvement in the physical/romantic unattractiveness subscale, and only one study observed a medium improvement on the social/character disparagement subscale of the AFAT following the intervention (Rukavina et al., 2010). No changes were observed on any of the ERT subscales (i.e., stupid/smart, lazy/motivated) following the interventions (Rukavina et al., 2008, 2010).
Implicit Weight Bias
No significant changes were observed in fitness professionals’ implicit weight bias. Notably, Tingstrom and Nagel (2017) and Wijayatunga et al. (2019) observed an increase in implicit weight bias among the control condition (regularly planned class content), suggesting that the standard curriculum itself can increase bias when no intervention is administered.
Discussion
To date, no systematic review has been conducted exclusively on fitness professionals to explore existing weight bias interventions among this population. Seven papers comprising six unique studies were identified in the current review. Explicit weight bias, particularly on the weight control/blame subscale of the AFAT, showed consistent small to large improvements postintervention and at one-month follow-up. However, mixed results were observed regarding other AFAT subscales, and no changes were noted when weight bias was assessed using the ERT. Moreover, no significant changes were observed in fitness professionals’ implicit weight bias, though control conditions showed increased bias from preintervention to postintervention, highlighting the potential bias reinforcement of standard curricula. This finding is in line with previous literature showing that the longer fitness professionals are in education or working in the fitness industry, the more biases they hold toward fatness and fat people (Whitehead, 2016; Zaroubi et al., 2021). Alternatively, it may be that the interventions increased social desirability to not report antifat attitudes or were insufficient to reduce implicit biases, even though explicit biases decreased. However, this needs to be substantiated in future research.
The existing evidence base shows that interventions based on attribution theory and raising awareness around weight bias and empathy toward individuals of higher weight have a small impact on the weight controllability component of weight bias. However, little evidence currently exists regarding the effectiveness of weight bias interventions on other components of explicit and implicit weight biases. Moreover, only one study identified in the current review evaluated more positive attitudes toward fatness and fat people, such as acceptance of body and appearance diversity (Casadó-Marín & Gracia-Arnaiz, 2020) or fat acceptance (Cain et al., 2022). Specifically, one study (Fogaça et al., 2024; Zuest, Lee, Fogaça et al., 2023) used the FAAT (Cain et al., 2022), a multidimensional, nonstigmatizing measure of contemporary attitudes toward fatness and fat people. The limited evaluation of multifaceted and positive measures of weight bias is a significant limitation given that little is currently known regarding whether a change in attitudes toward the controllability of weight improves how fitness professionals relate to, and interact with, fat people. For example, the acknowledgment of weight's uncontrollability by fitness professionals could lead to decreased motivation to support fat individuals in their fitness pursuits, highlighting the necessity for research into how this affects interactions and strategies to mitigate negative impacts.
Relatedly, scholars argue that there are drawbacks of empathy approaches, as they may instead evoke concern and pity as a cloaked version of stigma toward, and othering of, fat people (SturtzSreetharan et al., 2022). Most current interventions focus on evoking empathy and/or education about the causality/controllability of “obesity,” thereby medicalizing and pathologizing “obesity” (Ramos Salas et al., 2017), and framing being fat as a struggle that requires sympathy, which can have iatrogenic effects. Previous research has found that although empathy-evoking approaches increase empathy and affective attitudes toward fat people, they may be ineffective at reducing explicit weight bias (fat phobia) and social distance toward fat people (Gloor & Puhl, 2016). Similarly, a systematic review and meta-analysis of weight-bias interventions among adult samples found that interventions based on the dominant paradigms in weight-bias reduction research (i.e., controllability, empathy, and social consensus) performed no better than interventions based on different theoretical models (Lee et al., 2014). This is also evidenced in the current review by the lack of improvement in fitness professionals’ implicit bias following interventions targeting controllability, empathy, or awareness, meaning that most biased attitudes toward weight remained in this population.
To address limitations of existing approaches, novel approaches have recently been proposed that go beyond weight attribution, awareness, and evoking empathy. For example, Ebbeck and Austin (2018) proposed self-compassion for fitness professionals as a tool to create a climate of self-care and care for others, whereby the ultimate goal is to shift the focus in fitness centers from appearance to health and well-being. Moreover, HAES® has been applied as a framework in a wide range of domains to decouple weight and body size from “health” (Dugmore et al., 2020; Hunger et al., 2020; McGregor et al., 2022). However, little application of these frameworks has been seen in weight bias interventions targeted toward fitness professionals. Further, more research is required on how HAES® and self-compassion approaches can be applied to interventions to reduce weight bias among this population and to rigorously test if such approaches are effective in reducing weight bias.
Few resources are currently available for fitness professionals that aim to educate about weight bias and weight stigma, and how to work with fat clients. Of the few that are available, most focus on body image, disordered eating, and exercise behaviors, the causes of weight stigma, and the importance of representation in the fitness industry. For example, in the United Kingdom, Fitness Professionals Against Weight Stigma CIC offers a free self-paced online course on the basics of weight stigma. In the United States and Canada, the Size Inclusive Training Academy© has a fitness specialist qualification and a similar version of this course (A Space for Every Body: Addressing Weight Bias in the Fitness Industry) is offered through the American Council On Exercise®. Besides education around body image and weight bias, this course includes topics on training methodology, form and physiology, equipment and setting considerations, and marketing for fitness professionals. To date, none of these resources have been evaluated with regard to their effectiveness at reducing weight bias among fitness professionals. This shows a gap between what has been designed and trialed in the scientific space and what has been developed and implemented by fitness professionals for their industry. The interventions developed in the applied psychology space need to provide more practical and innovative tools for the industry and the programs currently being offered within the industry would benefit from rigorous scientific testing to assess their efficacy and impact and to establish that they are not causing harm.
Limitations and Future Directions
The findings of this review need to be considered in light of several limitations. In relation to the included literature, most studies showed poor methodological quality, particularly related to study design, selection bias, and confounders, as well as the lack of long-term follow-up assessment and maintenance of target outcomes. Additionally, only two studies were conducted among in-service fitness professionals. As highlighted by previous reviews (Moore et al., 2022), most weight bias interventions are currently targeted toward students and pre-professionals, limiting the conclusions that can be drawn regarding the effectiveness of such interventions among fitness professionals already working in the fitness industry. More research is therefore required to develop and evaluate weight bias interventions among fitness professionals. Finally, although we conducted extensive searches for published and unpublished literature, some studies may have been missed, particularly studies published in languages other than English.
Application to Practice
Weight bias is associated with numerous negative health, social, and economic outcomes. The pervasive weight bias documented among fitness professionals perpetuates health inequities by deterring fat people from accessing fitness spaces and gaining the associated health benefits. Our systematic review shows that weight bias interventions within this population are scarce and have limited effectiveness. Furthermore, there is a notable lack of publicly available resources and those that exist are not evidence-based. Additionally, there is a notable discrepancy in the content of interventions evaluated in the scientific literature and those that are industry-based. Specifically, while published intervention studies focus on education and awareness about weight bias and weight stigma, as well as attitudes toward fat people and fatness, existing programs are more practical in that they offer specific guidance around how to work with people in larger bodies and how fitness professionals can market themselves as weight inclusive. The findings of the current review underscore the critical need for innovative interventions tailored to fitness professionals to mitigate weight bias, promote inclusivity within fitness environments, and reduce health disparities. Specifically, there is a need for novel intervention approaches that are multifaceted and draw from multiple theories of attitude and behavior change (Alberga et al., 2016; Sherf-Dagan et al., 2024), and incorporate theory, learnings from empirical research, and practise to ensure they are useful, feasible, and effective at inducing sustained change in explicit and implicit weight biases.
Moving forward, we propose future research could apply and evaluate the Matrix of Anti-Stigma Interventions outlined by Harwood et al. (2022) in the context of weight bias interventions for fitness professionals. This conceptual framework builds upon prior research by Link (2001) and Corrigan et al. (2001), offering a versatile tool applicable to various stigmas, including weight stigma. Corrigan et al. (2001) delineated three intervention strategies aimed at mitigating stigma: (1) protest, which involves confronting negative representations; (2) contact, which involves facilitating interactions between the public and stigmatized groups; and (3) education, which involves improving understanding of stigmatized issues. Harwood et al. (2022) suggest a fourth category, regulation, to encompass legal approaches moderating discriminatory behavior. Considering the three mechanisms of stigma—direct discrimination, structural discrimination, and self-stigma (Harwood et al., 2022)—the Matrix of Anti-Stigma Interventions integrates these mechanisms with the four intervention strategies. Each cell in the Matrix exemplifies how an intervention strategy can address a specific stigma mechanism, recognizing that interventions may target multiple mechanisms. Most current interventions focus primarily on one intervention strategy (e.g., education) and one mechanism of stigma (e.g., direct discrimination). However, the Matrix highlights that interventions employing a blend of protest, contact, education, and regulation strategies may be most impactful. Indeed, to target the wider structural discrimination of weight bias and weight stigma, interventions should move beyond communicating the harms of labeling and stereotyping fat bodies to provide education about the rights of individuals to be treated fairly and the legislation in place to protect those rights (Harwood et al., 2022; Ramos Salas et al., 2017).
Conclusions
There is a notable gap in the development and provision of effective interventions to reduce weight bias among fitness professionals. The findings of this review show some evidence for reduction in explicit weight bias, particularly on weight control and blame attitudes, but limited evidence for other explicit and implicit weight bias outcomes. A few novel approaches have been suggested, such as self-compassion and HAES®, but such approaches have little application and evaluation. This review also shows a gap between what has been designed and evaluated in the scientific space and what is developed by fitness professionals and available in the industry. There is an urgent need to bridge this gap and to develop novel intervention approaches that are multifaceted and draw from multiple theories of attitude and behavior change to effectively address weight bias and weight stigma among fitness professionals.
Supplemental Material
sj-docx-1-rsj-10.1177_15588661241280200 - Supplemental material for A Systematic Review of Interventions That Aim to Reduce Implicit and Explicit Weight Biases among Fitness Professionals
Supplemental material, sj-docx-1-rsj-10.1177_15588661241280200 for A Systematic Review of Interventions That Aim to Reduce Implicit and Explicit Weight Biases among Fitness Professionals by Jekaterina Schneider, Aline Tinoco, Becky Scott, Gemma L Witcomb, Emily L Matheson and Phillippa C Diedrichs in Recreational Sports Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Vice Chancellor’s Early Career Researcher (VC ECR) Development Award 2023–25, University of the West of England, (grant number USOS1010).
Supplemental Material
Supplemental material for this article is available online.
Correction (December 2024):
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.