
Abstract
Human papillomavirus (HPV) is the most common sexually transmitted infection worldwide, impacting both males and females. In men, HPV causes genital warts, more than 90% of anal cancers, and 60% of oropharyngeal cancers. Given that one in three men are infected with HPV worldwide, there is a pressing need for enhanced public health strategies focusing on prevention. This comprehensive narrative review presents an overview of HPV in men, key risk factors, and primary prevention in men. The most effective preventive measure for HPV in males is vaccination. Males at high risk for HPV include those who smoke, have human immunodeficiency virus, consume alcohol, engage with multiple sexual partners, fail to use barrier methods, and are unvaccinated. HPV vaccinations prevent most HPV-associated diseases; however, numerous barriers to vaccine uptake remain, including misconceptions that men do not benefit from vaccination, safety concerns, limited accessibility, and inconsistent vaccine recommendations.
Introduction
Human papillomavirus (HPV) is the most common sexually transmitted infection (STI) worldwide, affecting both males and females (Dunne & Park, 2013). It is the most commonly reported STI in the United States, with about half of U.S. men infected with HPV at any one time (Giuliano et al., 2008, 2010).
Although public awareness often centers on HPV’s impact on women and cervical cancer, it is crucial to recognize that men are susceptible to HPV-related health issues and play a pivotal role in viral transmission to their sexual partners. Evidence identifies infection with high-risk, oncogenic HPV subtypes as a key factor in several malignancies and their precursor lesions in men (Giuliano et al., 2010; Palefsky, 2007), highlighting the urgent need for an increased awareness of the impact of HPV in men. Evidence suggests that high-risk HPV compromises male fertility by adversely affecting sperm integrity and viability (Boeri et al., 2019; Olivera et al., 2024).
While the epidemiology and impact of HPV in women have been extensively studied, the literature on HPV and its impact on men remain limited. This disparity may be due to the historically lower inclusion of males in HPV-related research and prevention programs, and the higher incidence of HPV-associated morbidity and mortality in women (Garolla et al., 2023). However, the health burden of HPV among men underscores that prevention efforts should include men.
This narrative review presents an overview of HPV in men, key risk factors, and the importance of primary prevention in men. Since there are no established screening strategies for HPV in men, an increased awareness of the consequences of HPV infection in men, an understanding of key risk factors, and HPV vaccination can guide primary prevention strategies to reduce the burden of HPV-associated disease.
Methods
A narrative literature review follows a nonsystematic review approach to present a broad overview and the latest insights on a topic (Baumeister & Leary, 1997). Unlike systematic reviews, which focus on narrowly defined questions (Ferrari, 2015; Gregory & Denniss, 2018), narrative reviews are well-suited for exploring expansive topics. Narrative reviews serve as a valuable tool for concisely distilling complex information, making them particularly useful for examining comprehensive subjects such as HPV prevention in men (Green et al., 2006; Greenhalgh et al., 2018).
To structure this review, two authors (MSL and MH) independently conducted a literature search, using the MeSH terms “human papillomavirus,” “prevention and control,” “primary prevention,” and “men” to formulate an initial draft outline. After developing their respective outlines, they compared findings and collaborated to refine a final version.
The finalized outline guided searches on PubMed and Google Scholar for English-language publications covering HPV epidemiology, pathophysiology, risk factors, clinical manifestations, and primary prevention, focusing on male populations. The retrieved articles were assessed for relevance, and the bibliographies of selected studies were reviewed for additional supporting literature and data sources. Preference was given to original research, official guidelines, and high-quality comprehensive reviews. When applicable, governmental websites such as the Centers for Disease Control and Prevention (CDC), the National Institutes of Health, and other authoritative sources were utilized for epidemiological and statistical data.
The sources reviewed included the following: guidelines, consensus documents, original research articles, review articles, government-sponsored websites, and additional sources such as case studies, pharmaceutical websites, university and hospital-affiliated websites, and websites from national health organizations.
To enhance the credibility and methodological rigor of this review, the authors applied the Scale for the Assessment of Narrative Review Articles (SANRA), a critical appraisal tool designed to evaluate narrative literature reviews. SANRA assesses six key components: (1) justification of the review’s relevance, (2) clear articulation of its objectives, (3) thorough description of the literature search strategy, (4) targeted and appropriate referencing, (5) sound scientific reasoning, and (6) comprehensive presentation of relevant data and conclusions (Baethge et al., 2019).
Two authors (MH and MSL) conducted a final evaluation to ensure that the review met the SANRA criteria and maintained a high level of quality.
HPV Overview
HPV is a double-stranded DNA virus with more than 225 identified types, of which about 40 types can infect the mucosal epithelium (Meites et al., 2021). Virologists organize HPV types through standardized genotyping and divide infectious HPV into two groups: low-risk types, like HPV 6 and 11, which can cause skin, anal, and genital warts, and high-risk types (oncogenic), such as HPV 16 and 18, which are strongly linked to cancers of the throat, and genital areas (Chan et al., 2019). In addition to 16 and 18, other high-risk strains, including types 31, 33, 35, 39, 45, 51, 52, 56, 58, and 59, are also implicated in anogenital and oropharyngeal cancers (National Cancer Institute, n.d.). Table 1 summarizes the link between HPV subtype and clinical manifestation.
Consequences of HPV Infection and Associated Subtype.
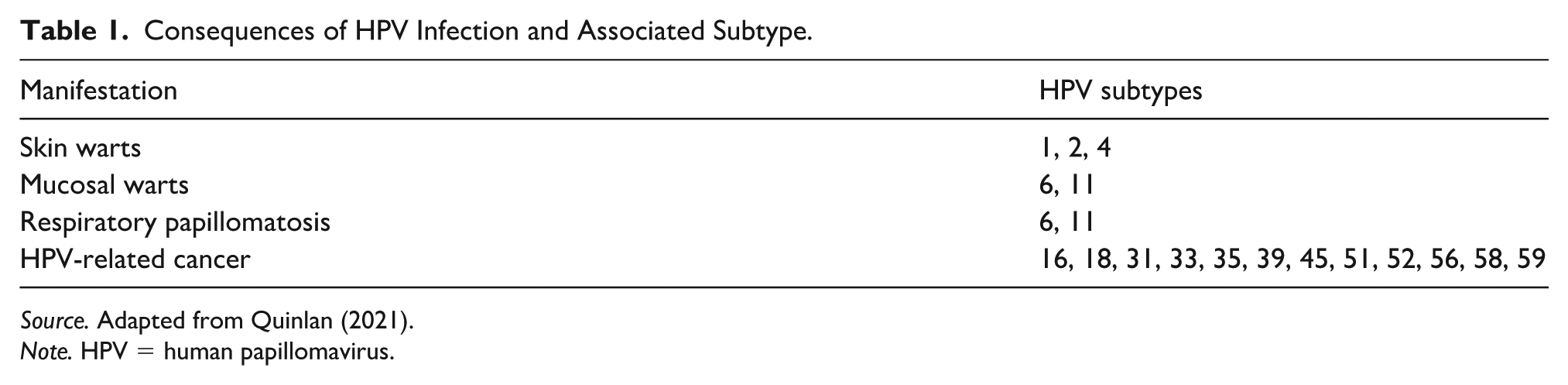
Source. Adapted from Quinlan (2021).
Note. HPV = human papillomavirus.
Men usually contract HPV sexually during vaginal, anal, or oral sex, with a transmission rate of about 65% from an infected individual to a susceptible sexual partner (Anic & Giuliano, 2011). Transmission often occurs unknowingly because most infections are asymptomatic, making it challenging to identify and control the spread of HPV. Nonsexual transmission pathways, such as skin-to-skin contact, can occur. HPV DNA has also been found in semen, sperm cells, various regions of the male reproductive tract, ovaries, and endometrium, indicating that HPV may be transmitted during fertilization or shortly after fertilization (Oyouni, 2023).
HPV in Men
HPV can infect the penis, scrotum, anus, mouth, and throat, specifically the oropharynx. Genital warts are the most common clinical manifestation of HPV in men (Scheurer et al., 2005), with about 1% of sexually active adults in the United States infected at any given time (Illinois Department of Public Health, 2025). Lifetime HPV prevalence is reported as 85% in women and 91% in men who have had at least one sex partner (Chesson et al., 2014).
Genital warts are small, rough lumps that can be flat, raised, or cauliflower-shaped and may be painful, itchy or bleed, and can take a psychological toll. Warts usually appear on the penis, scrotum, or in the anal region, but can occur in or around the mouth or lips. Low-risk HPV types 6 and 11 cause about 90% of genital warts (Brown et al., 1999; Temple et al., 2025). HPV types 6 and 11 are also strongly associated with recurrent respiratory papillomatosis, a rare disease affecting the respiratory tract (Katsenos & Becker, 2011).
HPV-associated cancer is the most serious HPV-related health concern. High-risk, oncogenic HPV subtypes typically remain asymptomatic in both men and women. Long-term infections in women (often lasting many years) with oncogenic HPV strains are responsible for nearly all cases of cervical cancer. While most HPV infections spontaneously resolve within one to two years, approximately 10% to 20% of infected men fail to clear the virus and experience persistent infections. Risk factors for failing to clear HPV include HIV (Swase et al., 2025), immunosuppression, older age, and smoking. In men, chronic infections play a significant role in anal cancer, oropharyngeal squamous cell carcinoma (Scott-Wittenborn & Fakhry, 2021), and penile cancer. In the United States, about 16,000 men develop HPV-associated cancers annually (Rosado et al., 2023).
Oropharyngeal cancer is the most common and the leading cause of HPV-associated cancer death in men, followed by anal cancer (Senkomago et al., 2019). Most oral and anal HPV-associated cancers are caused by HPV subtypes 16 and 18. Penile cancer is a less common but serious condition and is also linked to persistent HPV infections. HPV-associated cancers in men are increasing (CDC, 2018a), underscoring the importance of preventive measures. Table 2 summarizes the annual HPV-attributable male cancer cases in the United States.
Estimated Annual HPV-Attributable Cancer Cases in Men.

Source. CDC Cancer. Cancers linked with HPV each year (Rosado et al., 2023). Accessed March 19, 2025.
Note. HPV = human papillomavirus.
Unlike penile and anal cancer, HPV-associated oropharyngeal cancer lacks a well-defined precursor lesion (Kreimer & Chaturvedi, 2011). While some patients may develop dysplastic lesions, these are rarely visible, making it difficult to identify a precancerous lesion and intervene early. Symptoms, including sore throat, hoarseness, difficulty swallowing, or neck mass, appear late. However, HPV-positive cases of oropharyngeal cancer tend to have a better prognosis than HPV-negative tumors (Ang et al., 2010). Natural history of HPV-associated anal cancer is similar to HPV-associated cervical cancer in women, progressing from a persistent infection to dysplasia, anal squamous intra-epithelial lesions, and ultimately to cancer (Chang et al., 2004). Although anal HPV infections share similarities with cervical HPV infection, their natural history, including the progression to intra-epithelial neoplasia and cancer, remains incompletely understood (Moscicki et al., 2006, 2012). Further investigation is needed to elucidate the factors influencing HPV transmission between sexual partners and assess the impact of HPV vaccination in women on HPV-related disease in men (Palefsky, 2007).
In men, penile HPV infections can persist without causing active disease or obvious symptoms (latent infection), or progress to subclinical or clinical disease. Approximately 60% of invasive penile carcinomas are attributable to HPV, with HPV subtypes 16 and 18 the most frequently detected genotypes in penile tumors (Rosado et al., 2023).
HPV Vaccination
HPV vaccination has emerged as a crucial primary prevention strategy against HPV-related cancers and other diseases caused by HPV in both women and men. The value of vaccination as a prevention tool is emphasized in guidelines published by the World Health Organization (WHO) and the U.S. Centers for Disease Control and Prevention (CDC) (Meites et al., 2019). Initially developed to address cervical cancer, the HPV vaccine also yields significant benefits for males by preventing genital warts and HPV-associated cancers of the oropharynx, anus, and penis (Meites et al., 2019). While vaccination remains the most effective preventive measure against HPV infections and related health issues in men, global vaccination coverage for males is only 4% (Rosado et al., 2023).
The first-generation HPV vaccines, a bivalent vaccine (Cervarix), and a quadrivalent vaccine (Gardasil) were introduced in the mid-2000s. Cervarix targets HPV types 16 and 18, which are responsible for approximately 70% of cervical cancers (Monie et al., 2008), while Gardasil also covers HPV types 6 and 11, which cause most genital warts. The subsequent development of the nonavalent vaccine (Gardasil 9) extended protection by including five additional high-risk, oncogenic HPV types (31, 33, 45, 52, and 58), broadening its preventive scope (Joura et al., 2015). The nine subtypes covered by the vaccine are associated with the majority of anal cancer, throat cancer, and genital warts. While originally approved for cervical cancer prevention, in 2020, the FDA expanded the HPV vaccine’s approval to include anal cancer, oropharyngeal cancer, and other head and neck cancers (Merck, 2020). Recent data presented at the American Society of Clinical Oncology showed that the vaccine reduced the risk of all HPV-associated cancers in men by about 50% (Orr, 2024).
HPV vaccines consist of virus-like particles (VLPs) made from the L1 protein of the HPV capsid. These VLPs mimic the native structure of the virus without containing its DNA, enabling the induction of high titers of neutralizing antibodies without causing an actual infection (Akuzum et al., 2018). These antibodies prevent the virus from entering epithelial cells, reducing the risk of infection and subsequent HPV-related diseases. Immunogenicity is well documented and consistently exceeds the antibody response from natural infection (Andijani & Alsalhi, 2024).
While initially targeted at females, extensive clinical trials confirm the HPV vaccine’s effectiveness in men. For instance, studies in adolescent and young adult males demonstrate about 90% efficacy in preventing external genital lesions and precancerous anal lesions associated with the vaccine-covered HPV types (Rosado et al., 2023). This is especially important for men who have sex with men, a group at elevated risk for anal cancer. The durable immune response in males further supports its effectiveness and administering the vaccine before exposure to HPV can prevent most HPV-associated disease (Rosado et al., 2023). Rising rates of HPV-associated oropharyngeal and anal cancers in men underscore the importance of primary prevention through vaccination.
HPV vaccines have an excellent safety record, with postmarketing surveillance and large-scale studies confirming that serious adverse events are rare (Phillips et al., 2018). The most common side effects include local injection-site reactions and transient systemic symptoms like low-grade fever, which are generally mild and self-limiting (Yousefi et al., 2022). The CDC and Advisory Committee on Immunization Practices recommend routine vaccination for boys and girls at ages 11 to 12 years (with the option to start as early as 9 years). A two-dose schedule is recommended for those initiating vaccination before age 15, while a three-dose series is advised for older or immunocompromised individuals. Although the CDC recommends that everyone up to age 26 get the HPV vaccine, it is more effective when given before puberty. While most sexually active men have been exposed to HPV, unvaccinated men aged 27 to 45 years may still benefit from vaccination since it may cover HPV subtypes different from the ones they were exposed to (CDC, 2024a).
Studies demonstrate good immunogenicity after a single shot (Montroy et al., 2024; Waheed et al., 2023). In a 2022 position article, the WHO (2022a) stated that a single-dose schedule could provide similar efficacy and durability of protection to a two-dose schedule. Consequently, WHO recommends an off-label single-dose schedule for boys aged 9 to 20 years and two doses with a 6-month interval after age 21. A single-dose option is less costly, less resource intensive, easier to administer, and in countries with limited resources it frees up resources for other health priorities. Immunocompromised individuals should receive at least two doses and, when possible, three doses (WHO, 2022b).
Despite overwhelming evidence supporting the vaccine’s safety and efficacy, vaccine hesitancy remains partly due to misconceptions that HPV is solely a women’s issue, which diminishes its perceived benefits for males. In the United States, with coverage defined as one or more shots, uptake was about 35% among males 19 to 26 years, compared to almost 60% among females (CDC, 2022). Few studies examine HPV vaccine barriers specific to men (Siu et al., 2019), but a major impediment is the lack of a recommendation from and/or discussions with a healthcare provider (Grandahl & Nevéus, 2021). A healthcare provider’s unequivocal recommendation can motivate parents to have their sons vaccinated (Grandahl & Nevéus, 2021). In fact, parents often cite a physician’s failure to recommend HPV vaccination as the reason for not vaccinating their child (Attia et al., 2018), and these recommendations should become routine for males. Since many young males do not have a primary care physician or only seek episodic care (Mansfield et al., 2005), involving school nurses and school-based clinics offers an opportunity to improve HPV vaccine uptake (Attia et al., 2018; Grandahl et al., 2016).
Dental visits also offer opportunities to educate and recommend the HPV vaccine, particularly for adolescents and young adults who may not otherwise receive information from other healthcare providers (Walker et al., 2019). Dentists can enlist parents by emphasizing the safety and efficacy of the vaccine and framing it as a male cancer-prevention measure (Lipsky et al., 2025).
For recommendations to be effective, health professionals need sufficient knowledge, training, and confidence about HPV-related cancer to address concerns about HPV infection and vaccination (McRee et al., 2014). Correcting misinformation that HPV is not just a female disease (Tatar et al., 2017) that vaccination promotes promiscuity, and alleviating concerns about side effects and safety also contribute to higher uptake. Additional barriers include cost and access issues, and cultural stigma surrounding sexually transmitted infections (Grandahl & Nevéus, 2021). Addressing these challenges requires public health initiatives focused on education and clear communication. Evidence indicates that when healthcare providers deliver strong, informed recommendations, acceptance rates improve significantly (Oh et al., 2021). Table 3 summarizes barriers and possible solutions to vaccination.
Summary of Barriers to HPV Vaccination and Possible Solutions.

Source. Adapted from Attia et al. (2018); Grandahl and Nevéus (2021).
Note. HPV = human papillomavirus.
Key Risk Factors
Sexual Risk Behaviors and HPV in Men
Table 4 summarizes the key risk factors discussed in this section. Risk factors for HPV transmission include multiple sexual partners, unprotected sex, an early sexual debut, the absence of circumcision, and smoking (Rodríguez-Álvarez et al., 2018). The HPV vaccine offers durable effectiveness, immunogenicity, and safety with almost no breakthrough disease. However, the vaccine does not protect against all pathogenic HPV subtypes and primary prevention strategies such as condoms, dental dams and counseling about risk factors should be part of HPV prevention.
Risk Factors for HPV Infection and Persistence.

Source. Adapted from Rodríguez-Álvarez et al. (2018); Saunders et al. (2017); Szabo and Saha (2015); Wang et al. (2025).
Note. HPV = human papillomavirus.
While condoms significantly reduce the transmission of several STIs, they only offer partial protection against HPV. Even when used correctly, HPV can infect areas not covered by a condom and by skin-to-skin contact skin before placing the condom (Ames, 2024). Nonetheless, the risk of HPV acquisition is about twofold lower among nonmonogamous men, and consistent condom use reduces the overall risk of HPV transmission and the duration of HPV infections among high-risk men (Pierce Campbell et al., 2013). Moreover, condoms reduce the risk of infections with subtypes not covered by the vaccine.
Men who have sex with men are 16 to 17 times more likely to develop anal cancer due to higher rates of HPV infection and persistent infection (Saunders et al., 2017). Receptive anal sex increases the likelihood of HPV transmission and the risk of HPV-associated anal cancer. Barrier methods lower the risk of HPV infection and co-infection with HIV. HIV weakens the immune system, impairing the body’s ability to clear HPV infections increasing the risk of persistent infection and progression for HPV-related anal and oropharyngeal cancer in men (Clarke et al., 2022). It is important to counsel patients that condoms and dental dams reduce this risk regardless of vaccine status.
Oral sex is a key risk factor for HPV-associated oropharyngeal cancers (D’Souza et al., 2009; Wierzbicka et al., 2023). Unfortunately, many adolescent and adult patients perceive oral sex as risk-free and fail to use barrier protection because they do not understand the risks and the types of protection available (Saini et al., 2010; Strome et al., 2022). In addition to condoms, dental dams are an underutilized barrier method that offers some protection during oral-vaginal and oral-anal sex (Gutierrez et al., 2022). These are a single-use, rubber-based sheet (or latex square barrier) used to cover the vaginal or anal orifices to prevent direct contact between the mouth and the anus or vagina. Most research on dental dams focuses on women, and there are little data about their effectiveness in men.
Male Circumcision and HPV
Smith et al. (2021) found that male circumcision reduced the risk of Kenyan men acquiring HPV. Several other studies and a meta-analysis demonstrate that circumcised men have a lower prevalence of HPV infections compared with uncircumcised men (Auvert et al., 2009; Hebnes et al., 2021; Tobian et al., 2009; Zhu et al., 2017). One reason may be that the foreskin provides a moist environment, ideal for HPV to persist and multiply. Circumcision also reduces the surface area where the virus can establish an infection and the nonkeratinized foreskin mucosa is more susceptible to HPV infections (Zhu et al., 2017). However, the literature on HPV and circumcision is inconsistent, and not all studies show a benefit (Albero et al., 2013). Apart from preventing HPV acquisition, the foreskin can be a reservoir for HPV, and circumcision may reduce transmission and enhance viral clearance (Shapiro et al., 2023). Eliminating persistent infection is particularly relevant for high-risk HPV strains linked to cancer development.
In regions with high HPV prevalence and limited access to vaccination, circumcision may serve as a supplementary public health measure and help lower the burden of HPV-related cancers (Zhu et al., 2017). Circumcision is also associated with a lower risk of other sexually transmitted infections including HIV (Tobian et al., 2010). HIV often coexists with HPV and the immune response triggered by HIV, and other sexually transmitted diseases may influence HPV persistence and progression. Despite this, circumcision alone does not provide complete protection against HPV and should not be viewed as a replacement for vaccination and safe sexual practices. Practitioners should be aware that many ethicists and organizations oppose circumcision on ethical grounds and that the American Academy of Pediatrics, the American Academy of Family Practice, and the CDC do not believe the health benefits warrant routine circumcision for all males (American Academy of Pediatrics Task Force on Circumcision, 2012a; American Academy of Pediatrics Task Force on Circumcision, 2012b; Collier, 2012; Omole et al., 2021; Svoboda et al., 2016).
Alcohol and HPV
Alcohol consumption is consistently linked to elevated high-risk sexual behaviors across diverse populations. Heavy or binge drinking impairs judgment and reduces inhibitions, increasing the likelihood of unprotected sex, multiple sexual partners, and other risky behaviors that facilitate the transmission of STIs, including HPV (Llamosas-Falcón et al., 2023). In college settings, for example, alcohol-related sexual encounters are prevalent, with many students reporting unprotected intercourse following alcohol use. Data from the Youth Risk Behavior Surveillance System further indicate that a substantial proportion of high school students engage in sexual activity after drinking, often accompanied by reduced condom use (CDC, 2018b). Reduced condom use directly increases the likelihood of HPV transmission by removing an important layer of protection.
In addition to its role in facilitating risky sexual encounters, alcohol consumption also undermines adherence to HPV prevention measures (Havelka et al., 2024). Timely and complete HPV vaccination is critical for preventing HPV infection and its sequelae, such as cervical, penile, anal, and oropharyngeal cancers. Excessive alcohol use is associated with less use of preventive healthcare services, including fewer routine health visits and a lower likelihood of completing multidose vaccine schedules (Green et al., 2010). This diminished healthcare engagement creates significant barriers to both initiation and completion of the HPV vaccine series, undermining its effectiveness in reducing HPV-related disease burden.
Gender differences further complicate this scenario. Men generally report higher levels of alcohol intake (White, 2020) and tend to engage in a greater number of casual sexual encounters, which elevate their risk of HPV acquisition and transmission. Women, despite consuming less alcohol on average, often face challenges in negotiating condom use when under the influence, potentially placing them at increased risk for HPV infection. These gender-specific dynamics underscore the need for interventions tailored to both sexes.
Beyond behavior, alcohol also exerts biological effects. It weakens host immune defenses against viral infections (Szabo & Saha, 2015). Schabath and colleagues (2015) found that heavy alcohol intake was associated with increased risk for persistent HPV infections among men, after controlling for confounders such as sexual behavior and smoking. This suggests that alcohol has an independent adverse impact on HPV outcomes.
Given alcohol’s combined behavioral and biological influences, integrated public health strategies are essential. Programs aimed at reducing alcohol misuse should incorporate comprehensive sexual health education that emphasizes consistent condom use and the importance of timely HPV vaccination (CDC, 2024b). School-based and community interventions (e.g., brief motivational interviewing) alongside reminder systems for vaccine appointments could mitigate the adverse effects of alcohol on health behaviors. In addition, healthcare providers should screen for risky alcohol use and offer targeted counseling regarding both substance use and safe sexual practices (Moyer & U.S. Preventive Services Task Force, 2013; Savoy et al., 2020). By addressing alcohol consumption within the broader context of HPV prevention, these integrated approaches may reduce barriers to vaccination adherence and ultimately lower the risk of HPV-related diseases.
Smoking and HPV
Giuliano et al. (2002) first demonstrated that smoking increases the persistence of oncogenic HPV infection. Subsequent studies found that smoking prolongs cervical HPV infection and increases the risk for cervical dysplasia, the progression of dysplasia to cervical intra-epithelial neoplasia and, ultimately invasive carcinoma (Koshiol et al., 2006; Minkoff et al., 2004; Sellors et al., 2003; Sellors et al., 2000). However, less is known about how smoking influences HPV infection in men.
In 2020, about one-third of men worldwide and 13.1% in the United States smoked (CDC, 2024c; WHO, 2023). Given the prevalence and consequences of HPV in men, it is important to understand the impact of smoking on the natural history of HPV infections. Smoking could influence HPV infection by inhibiting local immune function, stimulating cellular proliferation and turnover, upregulating inflammation, or damaging DNA (Schabath et al., 2012). The HPV infection in men study found that current smoking was associated with an increased risk of low-risk and oncogenic HPV infection. This association was strongest for men with fewer lifetime female sexual partners (Schabath et al., 2012). Current smokers also had a higher prevalence, persistence, and incidence of anal HPV compared with never smokers (Umutoni et al., 2022). A literature review further linked smoking to an increased risk of head and neck cancer in the presence of HPV infection (Sinha et al., 2012). Together, these findings, along with the biological plausibility that smoking can promote infection, persistence, and the carcinogenetic effect of HPV, suggest that smoking cessation should be considered a primary prevention strategy for HPV infection.
Review Limitations
In a nonsystematic review, there is the possibility of selection bias when choosing articles, and some critical studies might have been missed. In addition, the rigorous evaluation of the included evidence was not conducted systematically. Despite these shortcomings, it is essential to acknowledge that narrative reviews remain valuable for condensing and integrating extensive information on a wide-ranging subject.
Conclusion
HPV prevention in men is essential for reducing the burden of genital warts, as well as penile, anal, and oropharyngeal cancers. Despite the availability of effective vaccines, awareness and uptake remain low, highlighting the need for increased education and access to prevention strategies.
Key takeaways emphasize vaccination as the most effective prevention tool, alongside safe sexual practices, targeted screening for high-risk groups, counseling about risk factors, and the role of healthcare providers in early detection and education.
A coordinated effort is needed to expand vaccination, improve awareness, and integrate HPV prevention into routine health care. By prioritizing these measures, we can significantly reduce HPV-related diseases in men and improve public health outcomes.
Footnotes
Acknowledgements
The authors thank the Clinical Outcomes Research and Education Center at Roseman University of Health Sciences College of Dental Medicine for their kind support.
Ethical Approval
Not applicable.
Consent to participate
Not applicable.
Author Contributions
Conceptualization—Man Hung, Martin S. Lipsky.
Methodology—Man Hung, Martin S. Lipsky.
Software—Man Hung.
Validation—Man Hung.
Formal analysis—Man Hung, Martin S. Lipsky.
Investigation—Man Hung, Martin S. Lipsky, Bayler Gunnell, Justin Nguyen, Samantha Lee, Geo Wolfe.
Resources—Man Hung.
Data curation—Man Hung, Martin S. Lipsky, Bayler Gunnell, Justin Nguyen, Samantha Lee, Geo Wolfe.
Original draft—Man Hung, Martin S. Lipsky, Bayler Gunnell, Justin Nguyen, Samantha Lee, Geo Wolfe.
Editing—Man Hung, Martin S. Lipsky, Bayler Gunnell, Justin Nguyen, Samantha Lee, Geo Wolfe.
Visualization—Man Hung, Martin S. Lipsky.
Supervision—Man Hung, Martin S. Lipsky.
Project administration—Man Hung, Martin S. Lipsky.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Not applicable.