
Abstract
This descriptive, cross-sectional survey study aimed to evaluate the knowledge of human papillomavirus (HPV) infection and vaccination, related diseases, vaccination status, and attitudes toward vaccination among Turkish male health care workers (HCWs). The study was planned between June 20 and 30, 2023. A questionnaire was developed by reviewing similar studies to assess the sociodemographic characteristics, knowledge about HPV, vaccination, and attitudes toward vaccination. A total of 322 volunteers (doctors, male nurses, and other allied health personnel such as cleaning staff, patient carers, and technicians) completed the questionnaire. Participants generally provided accurate answers to questions about HPV but often provided incorrect answers regarding vaccination. In addition, the overall HPV knowledge score was significantly higher among vaccinated participants or those willing to be vaccinated than those who were unvaccinated participants and those who were unwilling to be vaccinated (p < .05). There was a significant and moderately strong relationship between HPV vaccine knowledge level and willingness to be vaccinated. In addition, the relationship between vaccination status and knowledge level was substantial. Factors such as medical position, age, alcohol use, and regular physical activity were more likely to affect the HPV knowledge levels of assistant HCWs negatively. Vaccine hesitancy was also higher in the 27 to 40 age group. Knowledge about HPV, medical position, number of sexual partners, social habits, views on vaccination, cost, and religious and cultural values directly affect the rate of HPV vaccination and willingness to be vaccinated.
Highlights
There is a significant relationship between the level of knowledge about human papillomavirus (HPV) and the rate of vaccination as well as the willingness to be vaccinated.
Social and cultural habits influence HPV vaccination rates.
The importance of HPV vaccination for males is not well understood.
There is a need to raise awareness about HPV vaccination among male health care workers.
Introduction
In Turkey, especially in the male population, there is awareness that human papillomavirus (HPV) vaccination is only given to females (Sağtaş & Gürsoy, 2024). Surveys conducted among young people in Turkey show a low level of knowledge about HPV infection and vaccination. In addition, HPV vaccination rates are quite low (Gürdal & İlhan, 2024; Sulemana & Ardic, 2023). HPV can cause various types of genital warts, benign lesions, and cancers in both males and females. In females, HPV is primarily associated with genital cancers, while in males, it is a significant cause of oropharyngeal cancers (Roman & Aragones, 2021). Among the more than 100 known HPV genotypes, types 16 and 18 are particularly oncogenic and play a crucial role in the development of genital, anal, and head/neck cancers. Types 6 and 11 are mainly responsible for the development of genital warts (Bossart et al., 2020). Therefore, vaccination has a significant impact on the epidemiology of this disease, substantially reducing the incidence of HPV-associated cancers. In 2020, the Food and Drug Administration (FDA) also approved the HPV vaccine to prevent head and neck cancers. Since then, there has been a marked decrease in genital HPV infections and genital cancers, although this effect has not yet been observed in oropharyngeal cancers.
Despite these proven benefits, vaccination rates in communities generally remain lower than expected. In the United States, vaccination rates among adolescents aged 13 to 15 years are significantly below the 2030 target of 80%. In the United States, 76.8% of adolescents aged 13 to 17 years included in the 2023 survey had received ≥1 dose of HPV vaccine and 61.4% had received 3 or more doses of HPV vaccine (Chaturvedi et al., 2019; Pingali et al., 2024). A survey of 400 fathers aged 27 to 45 years in the United States found that 32% were unaware of the vaccine, 41% had received at least 1 dose, and 63% intended to vaccinate in the future (Quist et al., 2024). Global coverage for the first dose of HPV vaccine in girls grew from 20% in 2022 to 27% in 2023 (World Health Organization [WHO], 2024). Of the 54 African countries, 28 actively use the vaccination program, but only 5 have reached the 90% coverage rate the continent hopes to achieve by 2030. Across the region, 33% of young girls have received the HPV vaccine (Science & Health, 2024).
Studies across different races and populations have identified several factors that may influence vaccination rates, including sociodemographic structure, the developmental status of countries, education level, knowledge about vaccination, and religious, cultural, and moral values (Jiboc et al., 2024; Mihretie et al., 2022). This study evaluates HPV knowledge, related diseases, vaccination status, and attitudes toward vaccination among Turkish male health care workers (HCWs).
Materials and Methods
Survey Preparation
This study was designed as a descriptive cross-sectional survey conducted for 10 days between June 20 and 30, 2023. Health workers at the center were invited to fill out an information questionnaire, with the condition of volunteering. No information was requested, revealing the names or identities of the participants. A total of 30 questions were organized under 4 main categories: sociodemographic structure (age, place of living, marital status, number of sexual partners, medical role/position, smoking, alcohol, regular physical activity, private/family history of chronic disease, and private/family history of cancer), measurement of knowledge about HPV, measurement of knowledge about vaccination, and evaluation of attitudes toward vaccination. The survey was created using Google Forms and shared with volunteer participants via the “WhatsApp” application. The survey questions were developed by analyzing similar studies (Horio et al., 2023; Hu et al., 2021). In the second and third sections, participants’ knowledge about HPV and vaccination was assessed by asking them to choose from three options: yes, no, or no idea. Responses were then transferred to an Excel sheet, where they were scored. A correct response received 1 point, while other responses received 0 points.
The knowledge score for HPV (8 questions = 8 points) was calculated by summing the scores of the responses in the second section. The total knowledge score for vaccination (8 questions = 8 points) was similarly calculated by adding the points for the responses in the third section. In addition, an overall HPV knowledge score (16 questions = 16 points) was derived by combining the scores from both sections. Participants who achieved ≥70% of the total score were classified as having good knowledge, while those who scored lower were classified as having poor knowledge (Doğan et al., 2023). In similar surveys, the cut-off point for knowledge level measurement is taken as 70% and above. In our study, categorization was made according to the same cut-off point (Sahin et al., 2022).
The Sample Size
To determine the sample size, a previous study on tetanus vaccination was used as a pilot study (Doğan et al., 2023). The Raosoft Calculator tool was employed for the sample size calculation. In the calculation made with 5% margin of error and 95% confidence interval (CI), it was determined that at least 322 male health workers should be included in the study, considering that there are approximately 2,000 male health workers (doctors and nurses) and assistant health workers (personnel other than doctors and nurses) in our region. Female HCWs, individuals under 18 years of age, non-HCWs, and foreign nationals were excluded from the study.
Data Analysis
All statistical analyses were conducted using R version 4.3.0 in RStudio version 2023.06.0+421. R programming was also used for plotting the graphics. Statistical significance was set at p < .05 for all tests. Data are presented as frequency (percentage) or mean ± standard deviation (SD). The normality of the variables was tested using the Shapiro-Wilk test. The Mann–Whitney U test was employed to compare the medians of general HPV knowledge levels between different groups. Categorical variables were compared using the Chi-square test or Fisher’s exact test. Chi-square tests and phi coefficients were used to examine associations between variables, such as HPV vaccine knowledge and willingness to vaccinate. Logistic regression analyses were conducted to investigate the factors influencing general HPV knowledge level and willingness to receive the HPV vaccine further. The first logistic regression model assessed the effects of medical role, age, alcohol use, and regular physical activity on the likelihood of having a poor knowledge level about HPV. The model was statistically significant, χ2(4) = 62.7, p < .001, explaining 24.9% (Nagelkerke R2) of the variance in HPV knowledge level and correctly classifying 77.3% of cases. Odds ratios (ORs) were reported to quantify the associations between predictor variables and poor knowledge levels. A second logistic regression model was conducted to examine the effects of age, alcohol use, regular physical activity, medical role, number of sexual partners, and HPV vaccine knowledge score on the likelihood of unwillingness to receive the HPV vaccination. This model was also statistically significant, χ2(4) = 126, p < .001, explaining 46.0% (Nagelkerke R2) of the variance in HPV knowledge level and correctly detecting 82.3% of cases.
Study Approval and Participants
This study received approval from the local Ethics Committee of Bolu Abant Izzet Baysal University, Faculty of Medicine, Turkey (date: 19/06/2023, approval no: BAIBU/192). The voluntary nature of the survey, its purpose, and the expected outcomes were clearly outlined in the first part of the questionnaire form. No identifying information, such as participants’ names or surnames, was collected, and participation was limited to volunteers. No informed consent form was required from participants.
Results
Participants
A total of 322 male HCWs completed the questionnaire. The majority of participants were aged 27 to 40 years (n = 193; 59.9%), followed by those aged 18 to 26 years (n = 91; 28.3%). Specialist physicians made up the largest group (n = 185; 57.5%), followed by medical practitioners (n = 100; 31.3%) and assistant HCWs (AHW; n = 37; 11.5%). Most participants (n = 297; 92.2%) resided in urban areas, and half were married. A significant proportion of participants (n=90; 28%) reported having no active sexual partners, while (n = 35), 10.9% acknowledged having three or more sexual partners. Over 60% reported no history of smoking (n = 197), alcohol consumption (n = 200), chronic disease (n = 220), or cancer (n = 260). Detailed demographic characteristics of the participants are provided in Table 1.
Characteristics of the Health Care Professionals Who Participated in the Survey (n = 322)

Awareness of the HPV Vaccine
The mean general HPV infection and vaccine knowledge score was 12.07 ± 3.79. As shown in Figure 1, participants mostly provided accurate responses to questions related to HPV infection, whereas a higher rate of incorrect answers was observed for questions concerning HPV vaccination. Vaccinated respondents had significantly higher general HPV knowledge scores than unvaccinated respondents (p < .001). In addition, those willing to be vaccinated had significantly higher knowledge scores compared with those unwilling to be vaccinated (p < .001). The question “HPV infection can only be transmitted sexually” received the most incorrect responses, with 70% (n = 225) of participants answering incorrectly in Figure 2.
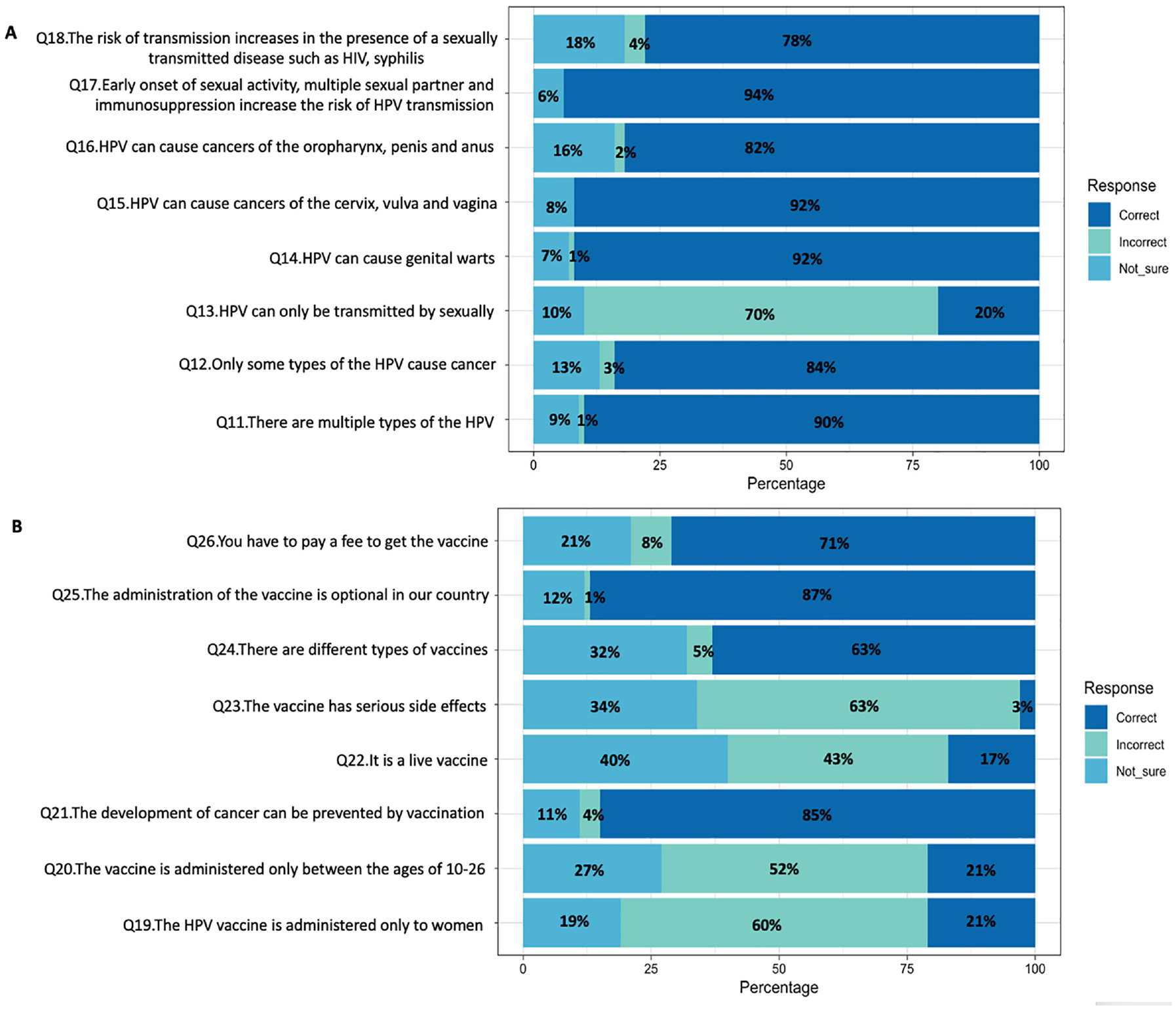
(A) Responses to the Knowledge Questions About HPV Given by the Male Health Care Professionals. (B) Responses to the Knowledge Questions About HPV Vaccine Given by The Male Health Care Professionals (n = 322)

General HPV Knowledge Scores by Vaccination Information
Vaccine Awareness and Willingness Association
There was a significant and moderately strong association (Phi = 0.26, p = 2.94e-06) between HPV vaccine knowledge level and willingness to vaccinate. A significant but modest association (Phi = 0.17, p = 1.86e-03) was also found between HPV vaccination knowledge level and vaccination status (Figure 3). The primary reasons for unwillingness to get vaccinated for HPV are illustrated in Figure 4, with the most common being “Don’t know about HPV vaccine” (26.8%; n = 86), followed by the perception of not needing the HPV vaccination (22.4%; n = 72).

(A) The Association Between HPV Vaccine Knowledge Level and Willingness Status. (B) The Association Between HPV Vaccine Knowledge Level and Vaccination Status

Reasons of Unwillingness to Get Vaccinated for HPV (n = 117)
Factors Affecting General HPV Infection Knowledge and Willingness to Vaccinate
Logistic regression analysis was conducted to determine the effects of medical role, age, alcohol use, and regular physical activity on the likelihood of having poor HPV infection knowledge (Table 2). Assistant HCWs were 20.15 times more likely to have poor HPV infection knowledge compared with specialists and medical practitioners. Participants aged 27 to 40 years had a decreased likelihood of poor knowledge (OR = 0.56, 95% CI = 0.33–0.96) compared with other age groups.
Logistic Regression Analysis on the Predictors of Knowledge Level About Human Papilloma Virus and HPV Vaccine

Note. HPV = human papillomavirus; OR = odds ratio; CI = confidence interval; AHW = assistant health care workers.
p < .05.
Another logistic regression analysis assessed the effects of age, alcohol use, regular physical activity, medical role, number of sexual partners, and HPV vaccination knowledge score on the likelihood of willingness to vaccinate (Table 3). A 1-unit increase in HPV vaccine knowledge score was associated with a 66.9% (n = 215) decrease in the likelihood of unwillingness to vaccinate. Participants with 3 or more sexual partners had approximately 0.31 times lower odds of unwillingness to vaccinate compared with those with fewer partners. Participants aged 27 to 40 years had approximately 2.09 times higher odds of unwillingness to vaccinate compared with other age groups.
Logistic Regression Analysis of the Predictors of Willingness to Receive the HPV Vaccine

Note. HPV = human papillomavirus; OR = odds ratio; CI = confidence interval; AHW = assistant health care workers.
p < .05.
Discussion
Globally, different strategies have been developed to prevent HPV infection-related diseases in males, with some having a significant impact on the workforce. Males’ sexual behavior patterns directly affect females regarding HPV infection-related pathologies. Therefore, it is important to include males in HPV vaccination programs for their safety and their partners’ health (Giuliano et al., 2024). However, as seen in our study, various factors influence prophylactic HPV vaccination in males. Factors include knowledge about HPV infection and vaccination, willingness to vaccinate, cost, concerns about side effects, religious and cultural awareness, parental awareness, and HCWs’ preferences regarding gender for vaccination (Kara Elitok et al., 2020; Olusanya et al., 2023).
A study conducted among health care providers in the United States aimed to identify early detection of HPV infection-associated oropharyngeal cancer in gay and bisexual men. The study found that health care providers focusing on HIV and LGBTQ issues were more aware of HPV infection-associated oropharyngeal cancer in these populations and were more prepared to take action (Zoschke et al., 2023). In another study on Jordanian physicians’ attitudes toward HPV screening and vaccination, a significant lack of knowledge about non-sexual transmission of HPV was found. Female physicians had a higher level of knowledge about HPV infection transmission routes and vaccination compared with males and were more positive toward HPV infection screening and vaccination. Physicians aged ≤ 25 years and academic physicians were more knowledgeable about HPV vaccines than their non-academic counterparts. Knowledge level was directly correlated with more positive attitudes toward vaccination and screening (Qaqish et al., 2023).
A study involving 530 family physicians in France found that 335 (63.2%) recommended HPV vaccination for boys. Since French guidelines recommended HPV vaccination for males, there has been an increase in vaccination. Factors such as academic status, support for extending HPV vaccination guidelines to males, using continuing medical education as the primary source of information on HPV vaccines, and requests for training on HPV vaccines were associated with recommendations for male vaccination (Habermacher et al., 2023).
In another study involving 1,723 male university students in Turkey, only 4.9% (n = 84) reported receiving the HPV vaccination, with the primary barrier being a lack of knowledge on when to vaccinate (49.5%; n = 852). Other significant determinants of HPV vaccination included marital status, sexual orientation, chronic diseases, family history of cervical cancer, and awareness of HPV infection (Gürsoy & Sağtaş, 2023).
Our study focused exclusively on male HCWs, which is somewhat different from other studies. It was found that male HCWs in our region had sufficient knowledge about HPV but insufficient knowledge about vaccination. Particularly, AHWs had lower levels of knowledge than doctors. Our findings suggest that the level of HPV infection knowledge directly affects the vaccination rate, as those with sufficient knowledge were more likely to be vaccinated. There was a significant and moderately strong relationship between HPV infection knowledge and willingness to vaccinate, while the relationship with the vaccination rate was significant but weaker. The lack of vaccination despite willingness may also be due to HPV vaccines not being covered by the social security institutions in Turkey. The cost of vaccination, borne by individuals, may be a significant barrier. The price of the Gardasil 9-valent vaccine in Turkey ranges from 2,400 to 3,000 Turkish Liras ($92–115) per dose, while the Gardasil quadrivalent vaccine (HPV Quadrivalent [Types 6, 11, 16, and 18] Vaccine, Recombinant) costs between 1,000 and 1,800 Turkish Liras ($38.4–69.2) per dose. With a minimum wage of $588 (as of October 24, 2024), these costs can be prohibitive for individuals.
A study on HPV vaccination among male nurses found that while general HPV knowledge was moderate, knowledge of the HPV infection screening test, HPV vaccine, and current HPV vaccination programs was low. The vaccination rates among participants were relatively low, and most were not considering vaccination. HPV infection knowledge was found to influence nurses’ attitudes and awareness (Sağtaş & Gürsoy, 2024). In our study, it was observed that AHWs had lower knowledge levels than medical doctors. We also found that poor HPV infection knowledge levels were influenced by age and social habits. The 27 to 40 age group was less likely to have poor knowledge than other age groups. In addition, the number of sexual partners and HPV vaccine knowledge level were directly correlated with the willingness to vaccinate.
Other reasons for the low vaccination rate, despite willingness, may include fear of side effects, vaccine hesitancy, religious and cultural values, and parental guidance. A study in Italy on vaccine-related adverse events after 12 years of HPV vaccination experience found no new medically confirmed safety concerns or serious, rare, or unexpected adverse events associated with HPV vaccines (Scavone et al., 2019). In a study involving parents in Turkey, the willingness to vaccinate their daughters was 45%, with an even lower rate likely for boys (Kilic et al., 2012). In Turkey, a significant portion of the population supports anti-vaccination, with awareness that vaccines cause infertility, contain harmful ingredients, or offend religious sentiments. Similar arguments were identified among male HCWs in our study, with 22.4% stating they did not need vaccination, 9% expressing fear of side effects, 14.5% doubting the effectiveness of vaccination, and 13% citing religious and cultural reasons. Studies in Turkey involving health care professionals and parents have identified barriers such as distrust in childhood vaccines, sociodemographic structure, education level, male gender, anxiety about the negative effects of vaccines, anti-vaccination sentiments, conspiracy theories, and inadequate control of imported vaccines (Kaya & Aydın-Kartal, 2022; Kaydirak et al., 2020; Sağtaş & Gürsoy, 2024).
Limitations
Our study has several limitations. First, only male HCWs were surveyed, leading to a lack of homogeneity in age and profession. Second, our study includes data from a single region and cannot be generalized to the entire country. Third, the questionnaire did not use a validated scale. The questions were developed exclusively for this study by adapting them from similar surveys. Finally, non-HCWs were not included. Suggesting a separate evaluation of adolescents’ and non-HCWs’ attitudes toward.
Conclusion
This study evaluated the level of HPV infection and vaccine knowledge, awareness, and attitudes toward vaccination among male HCWs in Turkey. By comparing our data with similar studies conducted in Turkey, particularly among university students, we aimed to provide a general overview. We found a significant relationship between the level of knowledge about HPV infection and vaccination rate and willingness to vaccinate. Sociodemographic factors, alcohol consumption, physical activity, and occupational group also influenced knowledge levels and willingness to vaccinate. The number of sexual partners was another factor that increased the willingness to vaccinate. Based on similar studies conducted in Turkey, we anticipate that other factors affecting vaccination rates and willingness to vaccinate include fear of side effects, suspicion of vaccines, vaccine hesitancy, conspiracy theories, financial costs, and religious and cultural values. Multicenter studies are needed to contribute to the literature on this subject.
Footnotes
Acknowledgements
We would like to thank the female health personnel working in our center for their support to the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.