
Abstract
Providers’ attitudes toward male human papillomavirus (HPV) vaccination may influence the implementation of new guidelines. Although 24 of 31 (77%) Pediatric and Family Medicine providers interviewed between 2009 and 2010 favored vaccinating males, only 3 (12%) offered vaccination. Providers who did not offer vaccination felt that parents would not be interested in vaccinating sons and were largely unaware of serious HPV-related disease in males.
Introduction
Human papillomavirus (HPV) infects approximately 20 million men and women in the United States each year. HPV infection can cause anal, penile, and oropharyngeal cancers in men, and approximately 7,000 HPV-associated cancers are diagnosed in men annually (Advisory Committee on Immunization Practices [ACIP], 2011). Infection with four HPV types can be prevented by the quadrivalent HPV vaccine, which is given in three injections at a cost of $108 to $130 per injection (ACIP, 2011). In 2009, the ACIP of the Centers for Disease Control and Prevention issued a permissive recommendation (allowing without explicitly recommending) for the use of quadrivalent HPV vaccination in males. Few providers began offering HPV vaccine to males, however, and recent estimates indicate that only 2% of eligible males have been vaccinated (Reiter, McRee, Kadis, & Brewer, 2011). On October 25, 2011, the ACIP issued a revised statement recommending universal vaccination of 11- to 12-year-old males with catch-up vaccinations for males aged 13 to 21 years (ACIP, 2011). The revised, stronger recommendation came in response to new data showing that vaccination could effectively prevent both genital warts and anal cancer precursors (Centers for Disease Control and Prevention, 2010; Palefsky et al., 2011), and epidemiologic data showing the increasing importance of HPV as a causal factor for head and neck cancers (D’Souza & Dempsey, 2011). Although the new recommendations will likely cause some improvement in HPV vaccination levels for males, their adoption may remain slow if physicians are unaware of the rationale behind the strengthened recommendations. The critical role of provider recommendation in HPV vaccination for females has been amply documented (Cates et al., 2010; Conroy et al., 2009; Guerry et al., 2010; Rosenthal et al., 2010, Vadaparampil et al., 2011). Yet current experience with HPV vaccination indicates a complex decision-making process, and only 32% of girls have been completely vaccinated 4 years after the introduction of universal recommendations (Centers for Disease Control and Prevention, 2011). Because offering the vaccine for boys may raise additional concerns (Weiss et al., 2010), this study aimed to describe providers’ thought processes around HPV vaccination for males.
Method
Between August 2009 and December 2010, we recruited 23 physicians (6 males, 17 females) and 8 nurse practitioners (all females) at four community health centers in Boston, Massachusetts, that serve primarily low-income, minority, and non-English-speaking populations. All practitioners providing primary care to adolescents, including HPV vaccination for females, in Pediatric and Family Medicine departments were eligible for inclusion; providers were recruited via e-mail, with a 54% participation rate. Using one-on-one, semistructured, qualitative interviews, we assessed providers’ attitudes and behaviors around HPV vaccination. Interviews lasted for 25 to 60 minutes, and the providers received no compensation. To address this study’s primary research question, all participants were asked, “How would you feel about offering the HPV vaccine to males?” Providers were then probed to elicit the reasons underlying these feelings. Twenty-six providers were interviewed after publication of the October 2009 permissive HPV vaccine recommendation for males. We determined whether these providers were aware of the new recommendations and whether they offered HPV vaccination to their male patients. Verbatim transcripts were analyzed using methods informed by grounded theory and content analysis (Charmaz, 2006). Primary coding was performed by RP and reviewed by JC for consistency. This study was approved by the institutional review board at Boston University School of Medicine.
Results
Twenty-four of 31 providers (77%) expressed support for vaccinating males in addition to females. They explained that they wished to prevent the sexual transmission of HPV from males to females: “Everyone understands the reason for cervical cancer [is HPV], but girls aren’t getting it without being with the boy who has it” (see Table 1). However, offering the vaccine to boys and their parents could entail a “hard sell.” Several providers felt that appealing to altruism would be insufficient to motivate vaccine acceptance: “I can already envision some of the reactions parents might have, that their child’s not going to get cancer, so why should they get the vaccine?” Only 2 providers (6%) were aware of any cancer prevention benefits of HPV vaccination for males. Ten (32%) were aware that HPV vaccination could prevent genital warts, but only 2 (6%) felt that genital wart protection was adequate motivation to vaccinate. Two providers (6%) who mentioned that HPV vaccination could reduce anal cancer did not find this argument compelling: “You don’t want to be in a situation where you make a value judgment that you’re going to vaccinate all men for cancer prevention in some men who are going to happen to be homosexual.” Some practitioners felt that offering the vaccine to males was simply not worth the cost or effort: “I don’t think the cost benefit is there to give it to boys. . . . I don’t think that it’s justified by how many cases of cervical cancer it’s going to reduce.” Unaware of the cancer risk for males, they felt they lacked a compelling argument to motivate male patients and parents to accept vaccination.
Provider’s Thoughts on Providing Human Papillomavirus (HPV) Vaccination to Males
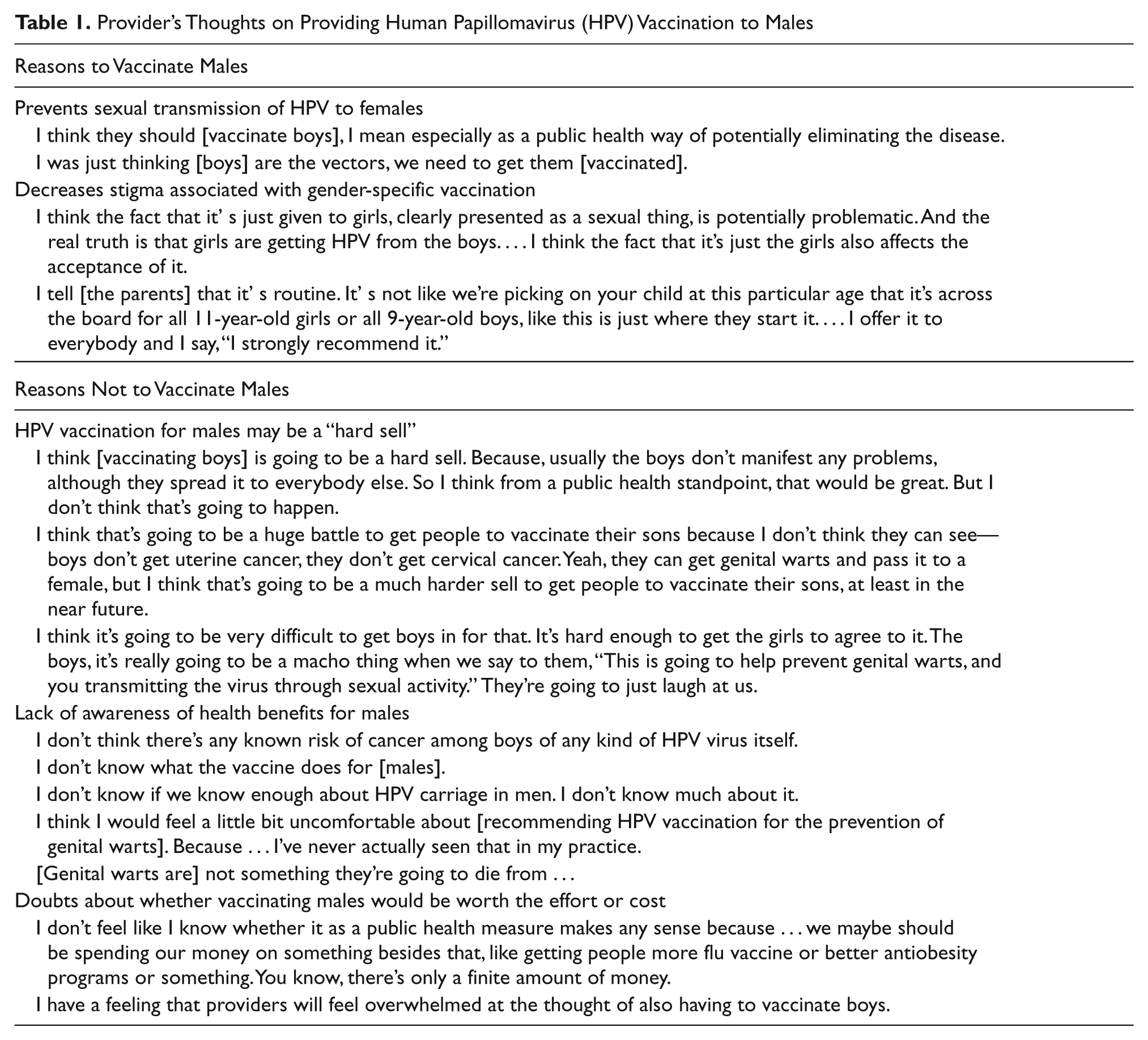
Three of 26 providers (12%) interviewed after the October 2009 permissive recommendation for males offered vaccination to their male patients. In contrast to the concerns reported above, these providers reported positive responses among male patients and parents. Providers who vaccinated both males and females also felt that offering vaccination to both genders reduced the potential stigma associated with offering a vaccine against a sexually transmitted infection to girls only. A pediatrician whose practice included many families with conservative social values reported that parents of young girls often deferred HPV vaccination because of its association with sex, but parents of boys did not: “Nobody tells me, ‘Oh no, we are going to wait until next year.’” Two adolescent providers who vaccinated males estimated that 50% to 90% of their male patients accepted their recommendation to receive HPV vaccination.
Discussion
In light of the new recommendations promoting universal HPV vaccination for males, understanding provider attitudes and actions with regard to this vaccine gains increasing importance. Although prior research indicated that most physicians supported HPV vaccination for males, research with both parents and providers raised concerns that parents may be more reluctant to vaccinate sons than daughters (Watts et al., 2009; Weiss, Zimet, Rosenthal, Brenneman, & Klein, 2010). In our study, although 24 providers (77%) expressed support for vaccinating males in addition to females, only 3 (12%) offered the vaccine to males in their practices. Providers seemed hesitant to offer vaccination to both because they felt that parents might be reluctant to accept vaccination and because they were unaware of serious HPV-related diseases in males. Only 2 providers (6%) were aware that HPV vaccination could prevent anal dysplasia, and none knew that HPV could cause oropharyngeal cancers. Providers who did offer vaccination, however, reported that male patients and their parents were receptive to vaccination, in some cases more so than females. Providers who offered HPV vaccination to both genders felt that universal recommendations helped reduce the stigma associated with offering a vaccine against a sexually transmitted infection to females only. Our findings are limited as we studied a small, convenience sample of providers working with low-income, minority patients in health centers where vaccinations are subsidized by the state; financial and patient-related concerns may be different in other settings.
In conclusion, the new guidelines for universal HPV vaccination for males may not lead to a rapid increase in vaccination rates if providers feel reluctant to offer HPV vaccine to males out of concern for negative parental reactions and if they remain unaware of the health benefits of HPV vaccination for males. Targeted provider education on the benefits of HPV vaccination for male patients, specifically the association of HPV with anal and oropharyngeal cancers in men, may be important for achieving vaccination goals.
Footnotes
The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; or preparation, review, or approval of the manuscript. Dr. Perkins wrote the first draft of the manuscript; no payment, grant, or honorarium was given to produce this work.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
Funding for this project was provided by an American Cancer Society Mentored Research Scholar Grant (MRSG-09- 151-01).