
Abstract
HIV self-testing (HIVST) plays a significant role in addressing the health care needs of high-risk populations, particularly men who have sex with men (MSM). The present systematic review and meta-analysis provide an assessment of the prevalence of HIVST among MSM within the last 5 years. Seven databases (PubMed, Web of Science, Cochrane, Scopus, EMBASE, ProQuest, and EBSCOhost) were searched systematically from January 1, 2018 to March 10, 2023. After an independent search and quality assessment, the pooled prevalence was calculated using a random-effects model. Eight relevant studies were finally included in our study from an initial pool of 288 articles identified through a systematic search. Our meta-analysis revealed that the pooled prevalence of HIVST among MSM is 8% (95% CI: 5%–14%). Significant heterogeneity was noticed among the studies, with an I2 value of 99% and a 95% prediction interval of 3% to 11%. Geography emerged as a significant moderator of this heterogeneity (p < .001). Specifically, studies from China reported a notably higher prevalence of 20% (15%–26%), while other countries reported a lower prevalence of 5% (3%–6%). A symmetrical Doi plot with a Luis–Furuya–Kanamori (LFK) index of −0.57 indicated no publication bias. HIVST has a low take-up among MSM globally. Factors leading to variation in HIVST need to be studied. The coordinated efforts of policymakers, health care providers, and affected communities are required in HIVST promotion.
Introduction
The first case of HIV was reported more than 35 years ago. Since then, 85.6 million people have been infected, and 40.4 million died from AIDS-related illnesses (Joint United Nations Programme on HIV/AIDS [UNAIDS], 2023). HIV spreads faster in situations where there are power imbalances, inequalities, stigma, and discrimination. The epidemic has been so diverse that in 2018, over half of the new HIV infections were found among key populations (UNAIDS, 2019). Men who have sex with men (MSM) contributed to 17% of new HIV infections worldwide. MSM has a 28 times higher risk of acquiring HIV in comparison to other heterosexual men (UNAIDS, 2023).
HIV is a prime concern in key populations and is a real challenge to the attainment of Sustainable Development Goals (SDGs) by the United Nations in the context of health, partnership, equality, and justice (World Health Organization [WHO], 2017). The Joint Program on HIV/AIDS by the United Nations targets global progress to achieve 95-95-95 (95% diagnostic coverage, 95% therapeutic enrolment, and 95% viral control) by 2025 across all population groups to reach the SDG of ending AIDS by 2030 (Heath et al., 2021).
HIV self-testing (HIVST) is a public health strategy to diagnose hard-to-reach populations and bring linkage-to-care services closer to populations where traditional testing locations are not easily accessible. HIVST involves collecting and performing a rapid diagnostic test on one’s oral fluid or fingerstick blood and interpreting one’s result with little or no training outside a health care setting. In 2012, the Food and Drug Administration (FDA) approved its first and only rapid oral over-the-counter HIVST to provide results within 20 min. Another type of HIVST includes a specimen collection kit that contains supplies to collect blood from a fingerstick at home. The dried sample is sent to a lab for testing, and a health care provider provides the results. HIVST, which involves finger prick blood tests, was approved by the WHO in 2016 (Ma & Manabe, 2023).
WHO advocates HIVST to target those who are hesitant to test, including at-risk populations. It maintains privacy and convenience for HIV testing (WHO, 2019). Fifty-two countries have begun implementing HIVST, whereas 98 countries have policies encouraging the same. However, many countries have yet to introduce HIVST as a routine approach (WHO, 2023).
A systematic review and meta-analysis (SRMA) published in 2017 by Zhang et al. explored the effectiveness of HIVST in enhancing HIV testing and linkage to care among MSM. The review included 23 studies and found that around 20% of people undergoing HIVST were first-timers. More people from lower-income countries were first-time testers than their counterparts (C. Zhang et al., 2017). Since then, there has been a rise in the research on HIVST among MSM exploring the factors associated with HIVST uptake and effectiveness in this population, as well as the influence of HIVST on HIV testing rates and linkage to care. It was observed that 32% of MSM in the United Kingdom had never tested for HIV despite having high infection risks (Vera et al., 2019). Uptake of HIVST tests was higher through vending machines compared to testing by community outreach workers almost six times (Vera et al., 2019).
Jin et al. (2019) carried out a cross-sectional study in the 14 provinces of China on MSM who were never tested for HIV. They offered web-based HIVST to MSM and found that over 40% tested themselves the first time, and around 20% of them were HIV-positive. Among non-testers, ones assuming either of the roles (insertive or receptive) are more likely to be HIV-infected (Jin et al., 2019). Another study in China found that around 40% of MSM underwent HIVST. Majority of them had experience of prior HIVST (38.3%) than first-timer HIVST (28.6%, p = .031). More MSM having a history of substance use during sex (22.8% vs. 15.4%, p = .049) and multiple sexual partners (76.1% vs. 59.4%, p < .001) were found among prior HIVST in MSM (Yang et al., 2022).
The significant factors facilitating and inhibiting HIVST were studied using in-depth interviews among 20 MSM and transgender women (TGW) in the Philippines (Mphande et al., 2021). Perceived facilitators of HIVST were confidentiality, convenience, and normalization of HIVST in the country. The barriers to HIVST implementation were a lack of privacy and confidentiality at the time of HIVST kits’ delivery (Mphande et al., 2021). Sison et al. (2022) observed that MSM prefer HIVST due to the stigma of HIV testing and associated provider mistrust.
To better understand HIVST prevalence among MSM and identify determinants associated with its uptake, an SRMA was carried out on published studies. U.S. Centers for Disease Control and Prevention endorses that people at risk of HIV should get tested at least once a year (DiNenno et al., 2017). The present SRMA has been planned to synthesize the prevalence of HIVST by MSM in the past year and to identify factors associated with HIVST uptake. The studies published in the English language since 2018 were sought. The studies were considered eligible if the reported data was on HIVST during the past year by MSM older than 18 years of age.
It was hypothesized that the prevalence of HIVST among MSM would vary by geographic region, study population, and HIVST distribution strategy. This is the first SRMA of HIVST prevalence among MSM, using studies published from 2018 onwards. The findings of the review may help to inform HIV prevention strategies for MSM, particularly in settings where traditional HIV testing services are inaccessible or stigmatizing.
Method
Research Question Selection Criteria
The literature was searched based on the Population, Exposure, Outcome, and Study type (PEOS) criteria (Supplementary Table S1). The keywords “Men who have sex with men,”“MSM,” gay, “HIV self-test,”“HIVST,” and “prevalence” were used. Keywords, terms with an asterisk in the title or abstract, and MeSH terms were used. As mentioned in the search strategy, seven databases and preprint servers were included (Supplementary Table S2). References of included studies and relevant reviews were screened. Studies published between January 2018 and March 2023 were considered for screening. The prevalence of HIVST among MSM was the primary outcome of our research. The registration number is CRD42023387331 in the International Prospective Register of Systematic Reviews (PROSPERO).
Screening of Studies
Two independent authors (R.D. and S.S.) reviewed the potentially eligible full-text articles for suitability and then extracted data from these. In case of disagreement at any step, the authors reached a consensus after discussion. The third author (M.A.S.) solved the contradictions. The literature search, screening of studies, and data extraction were performed by following the Preferred Reporting Standard of Systematic Reviews and Meta-Analysis (PRISMA-2020) guidelines (Supplementary Table S3).
Quality Assessment
Two independent authors (R.D. and K.G.) assessed the risk of bias as suggested by the National Institute of Health. If there was a disagreement, a similar process was followed as earlier.
Statistical Analysis
We used the random intercept logistic regression model for the meta-analysis. The heterogeneity among the articles was assessed by prediction interval, I2, τ, and τ2, in which the percentage of variability was determined (not sampling error). If there is heterogeneity, the subgroup analysis and the meta-regression were done to find the potential sources of heterogeneity. In addition, the Doi plot and Luis–Furuya–Kanamori (LFK) index evaluated the potential publication bias of the included studies. Dissymmetry was evaluated visually by Doi plot. The Baujat plot and influence diagnostic demonstrate the influence and heterogeneity contribution of the individual studies. A leave-one-out meta-analysis was also carried out. The robustness of the results for the primary outcome was evaluated by sensitivity analyses based on study quality and the influence of individual studies. All statistical analyses were conducted using R-programming language (v4.2.1), with p < .05 (two-sided) regarded as statistically significant.
Results
Eligible Studies
The search yielded 288 records. Deduplication resulted in 222 unique records. Following a title-abstract screening, 37 studies were reviewed further, and four were deemed eligible. Preprints, websites, and citation searches identified four new eligible studies. Eight studies were eligible for the SRMA (Bien-Gund et al., 2022; Bil et al., 2019; Guerras, Belza, et al., 2022; Guerras, Hoyos, et al., 2022; Hong et al., 2021; F. Liu et al., 2020; Sison et al., 2022; Wei et al., 2018). The process is depicted in Figure 1.

PRISMA Flowchart Depicting Included Studies in Systematic Review and Meta-Analysis
Characteristics and Quality of the Included Studies
The sample size ranges from 240 to 6,563, while 19,254 participants are included in the total. Three studies were conducted in China and several parts of Europe each. One study was conducted in the United States and the Philippines. Key findings and characteristics of each study are presented in Table 1.
Summary of the Included Studies in the Systematic Review (N = 8)
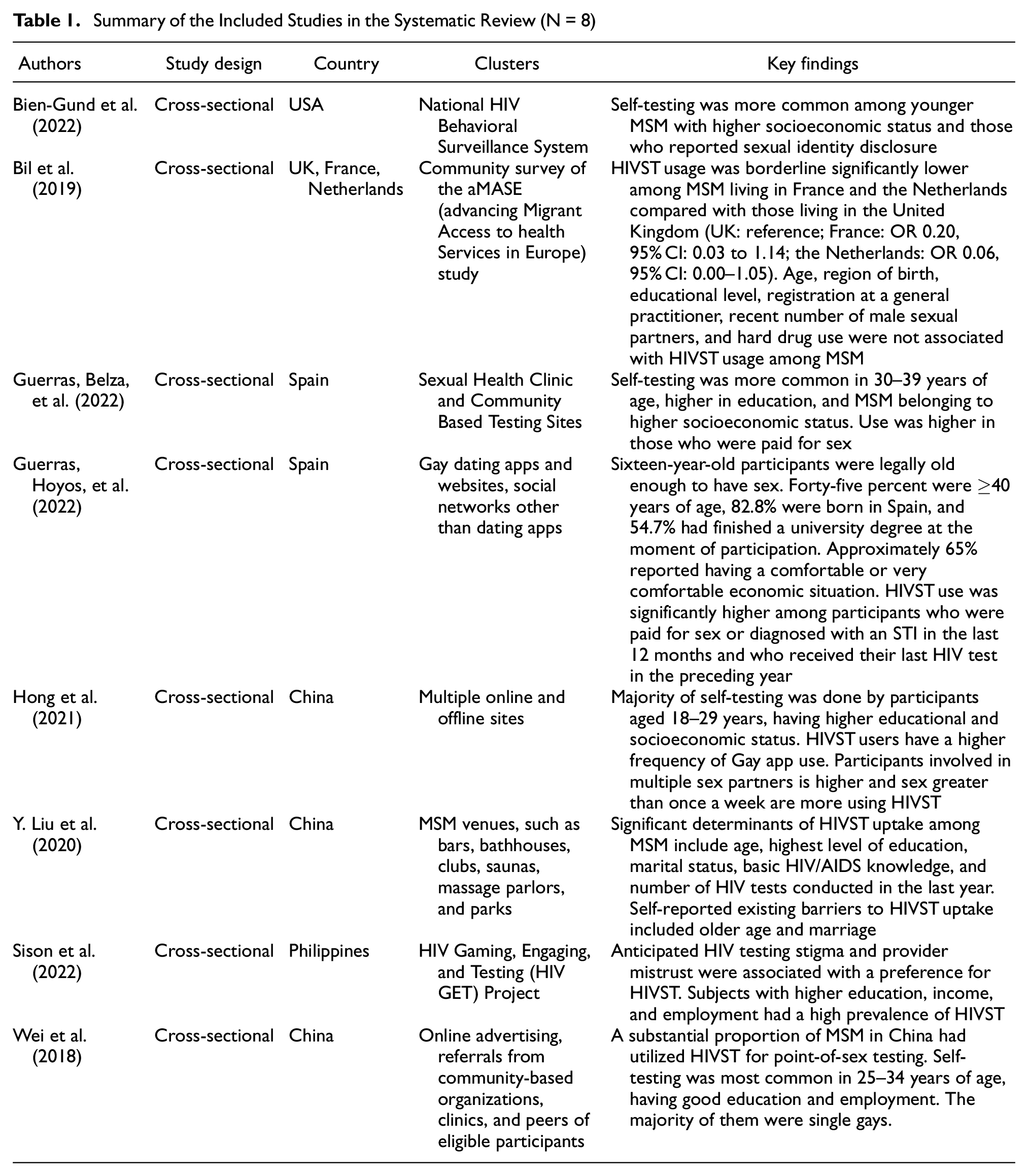
Out of the eight studies, six are of good quality, and two are of fair quality. None of the studies were of poor quality (Supplementary Table S4).
Pooled Prevalence and Heterogeneity
Eight studies reported the prevalence of HIVST among MSM in the current analysis. The pooled prevalence is 8% (95% CI: 5%–14%) (Figure 2).

Forest Plot Showing the Pooled Prevalence of HIV Self-Testing in Men Having Sex With Men
The reported estimates ranged from 3.3% to 26.7%. The estimates of the individual studies demonstrated the heterogeneity with an I2 of 99% and a τ2 of 0.73. The prediction interval lies between 1% and 45%. The heterogeneity has been demonstrated graphically (Supplementary Figure S1). Different clustering methods were used to identify causes of heterogeneity (Supplemental Figures S2: A-C). Subgroup analyses and meta-regressions were performed to explore the heterogeneity.
This considerable variation between the studies has been explained partially by exploring the reasons for heterogeneity by carrying out subgroup analysis for countries and continents. Stratifying the studies into those conducted in China and those conducted outside, and based upon the continent, the subgroup differences were significant in both cases (Q = 49.20, p < .01; Q = 59.92, p < .01). The tau-squared statistic for studies in China and those outside reduced from 0.73 to 0.10 and 0.08, respectively (Table 2).
Subgroup Analysis for Pooled Prevalence of HIV Self-Testing in Men Having Sex With Men

Meta-regression was carried out for the study sizes, which is not significant (p = .53), presented by a bubble plot (Figure 3).
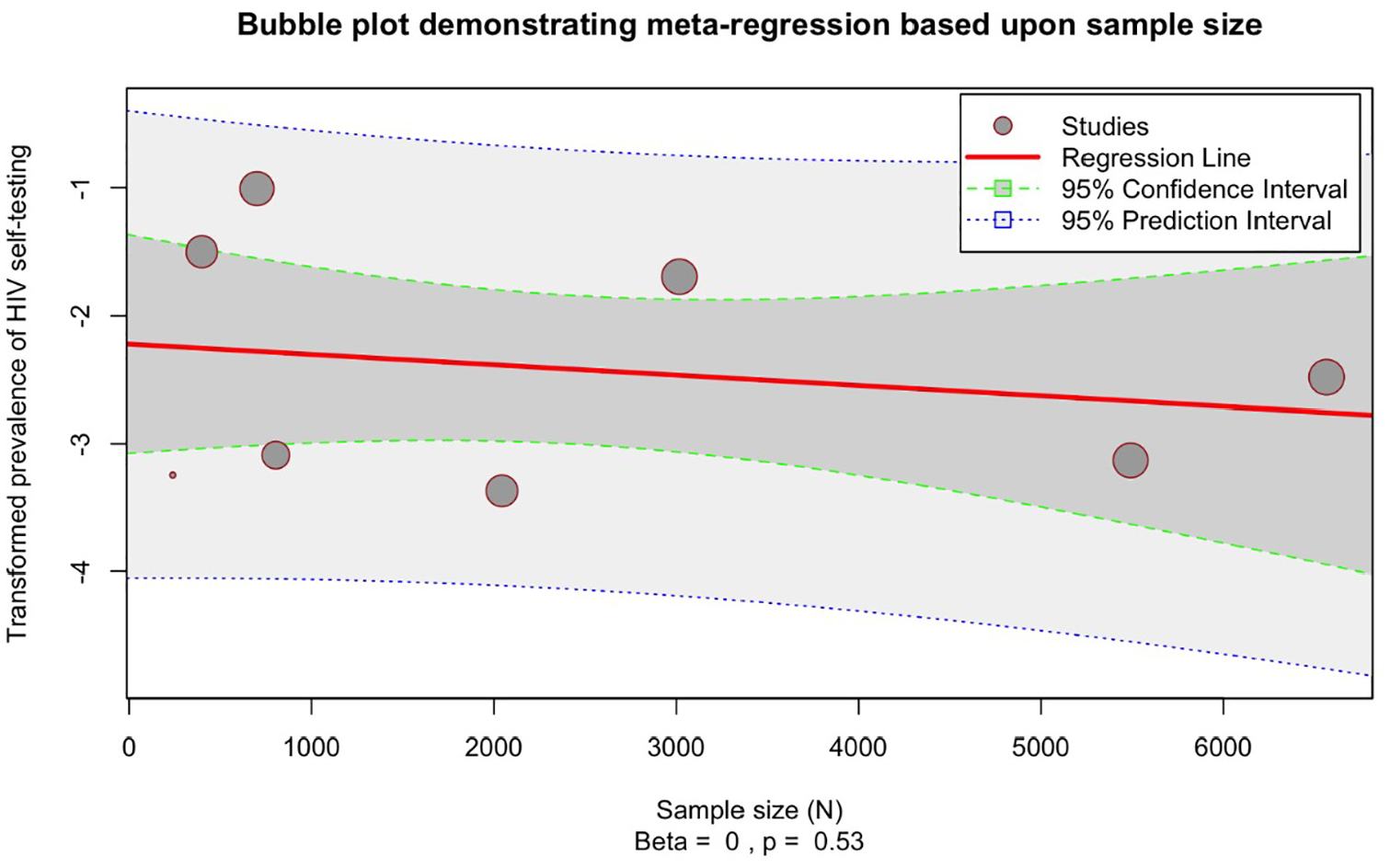
Bubble Plot Showing the Effect of Sample Size on the Pooled Prevalence of HIV Self-Testing in Men Having Sex With Men
Influence Assessment and Sensitivity Analysis
A Baujat plot (Figure 4) was constructed and used influence diagnostics (Supplementary Figure S3) and leave-one-out meta-analyses (Supplementary Figure S4) to identify the contribution of studies to the influence and heterogeneity. The Baujat plot shows that three highly influential studies caused the overall heterogeneity (Guerras, Hoyos et al., 2022; Hong et al., 2021; F. Liu et al., 2019).

Baujat Plot Identifying the Influence and Heterogeneity Contributions of Individual Studies
The primary analysis of the present review included participants of legal age, 16 years from Spain as that group falls into our target adult population (Guerras, Hoyos, et al., 2022). However, this study was excluded from a sensitivity analysis. The pooled prevalence did not change considerably with this step. It increased from 8% (95% CI: 5%–14%) to 9% (95% CI: 5%–16%) with an I2 of 99% (Supplementary Figure S5).
Another sensitivity analysis omitted the studies that contributed considerably to the pooled estimate and the overall heterogeneity. The pooled estimate changed from 8% (95% CI: 5%–14%) to 6% (95% CI: 3%–11%) with an I2 of 97% (Supplementary Figure S6).
A symmetrical Doi plot with an LFK index of −0.57 did not detect any small-study effect or publication bias (Supplementary Figure S7).
Discussion
HIVST may be preferred by MSM who are reluctant to seek facility-based testing due to the attached stigma. Therefore, the present review was undertaken to assess the global prevalence of HIVST among MSM.
This SRMA showed that 8% of MSM had undergone HIVST at least once in the preceding 12 months. The findings remained consistent with several sensitivity analyses. Excluding a study with a slightly different population and excluding three overly influential outliers also resulted in similar estimates, that is, 9% (5%, 16%) and 6% (3%, 11%), respectively. The results show significance between-study heterogeneity (I2 = 99%), and future studies are expected to give an effect size between 1% and 45%. However, this heterogeneity can be partially explained by the following factors influencing the prevalence. The two subgroups based on geography significantly moderated the variation in effect size. China reported a much higher prevalence at 20% (15%−26%) than other countries at 5% (3%−6%). This probably contributed to Asia having a much higher prevalence at 14% (7%−26%) than Europe at 4% (3%−5%) and North America at 8% (7%−8%). HIVST kits were also readily available in China through government-sponsored pilot initiatives and on e-commerce websites. In the absence of specific national policies or regulating guidelines about the sale of HIVST kits in China, there was extensive use of it among MSM in comparison to other countries (F. Liu et al., 2019). Moreover, China has scaled up HIV testing since 2004 by establishing a vast number of voluntary counseling and testing centers as an essential strategy to prevent onward transmission and repeated testing of high-risk populations (L. Zhang et al., 2012). The easy availability of health education and accessibility to HIVST kits might be the reasons for the high reporting of HIVST among MSM in China in comparison to other countries. Despite the US FDA approval of the first and only self-test in 2012, the regulatory barriers had dissuaded companies from applying for FDA approval for their HIV self-tests. However, numerous HIVSTs have been prequalified by the WHO (Ma & Manabe, 2023).
The results of this meta-analysis reveal that HIVST among MSM is still relatively low, with only 8% undergoing testing at least once in the previous 12 months. This finding highlights the pressing need to scale up HIVST programs among MSM. Expanding HIV testing and counseling on risk reduction is essential for decreasing the prevalence of HIV infection among MSM (Guerras, Hoyos, et al., 2022). Significant barriers to HIV testing include the stigma of the gay population and HIV-related discrimination, type of sexual relationship and partner preferences, the perception that HIV means death, low perception of risk or threat, and being unaware that testing is offered free of cost (Xu et al., 2020).
The present review findings suggest that localized strategies need to be developed and implemented in regions with low testing rates, such as Europe and North America (Bien-Gund et al., 2022; Bil et al., 2019; Guerras, Hoyos, et al., 2022; Vera et al., 2019). The results indicate a pressing need for scaling up HIVST programs in this population and risk reduction interventions for this group. It is crucial to implement innovative and targeted interventions to increase their awareness of the importance of regular HIV testing and reduce high-risk behaviors (Indravudh et al., 2020). Information dissemination through social networks, peer-to-peer, and social media through emails and short messages were effective ways of diffusing HIVST in the MSM community to reach non-testers (Jiang et al., 2020; Tso et al., 2016). Integration of HIV testing in routine medical care, MSM-friendly attitude of health care professionals, and acceptance of gay/bisexuals in the community through legal recognition with protection, and home self-testing are critical facilitators of early diagnosis of HIV (Wei et al., 2014). A positive experience for the client throughout the process is necessary to transform an HIV tester into a promoter. This requires a multidisciplinary approach involving social workers, health care providers, researchers, community leaders, and policymakers in identifying and implementing effective interventions. As the acceptability of HIVST among MSM in certain countries is high, it is essential to explore experiences and choices for HIVST among partners of MSM across countries (Kwan et al., 2023). While HIVST has shown promising results in increasing testing rates among MSM in some countries, it is not a substitute for comprehensive HIV care and treatment services (Ekholuenetale et al., 2022; Xu et al., 2020). Integration of HIVST into existing health care services can ensure that individuals who test positive are referred to appropriate care and treatment (Katz et al., 2018). Leveraging HIVST services in the Mobile Health (mHealth) program with public–private partnership can also expand its accessibility. Regulatory reforms in the countries could accelerate HIVST, which can be a crucial component of ending the HIV epidemic (Steehler & Siegler, 2019).
There are limitations to the results of this SRMA. Studies included in this meta-analysis were limited in number and may have needed to be representative of all MSM populations. Further research is needed to explore contextual factors such as socioeconomic status, access to health care services, and stigma toward MSM individuals and barriers that may affect HIVST uptake and HIV testing rates in different regions (Dovel et al., 2018; Narasimhan et al., 2021; Wise et al., 2019).
Conclusion
HIVST has a low take-up among men having sex with men. But, it is an optimistic intervention that can help to enhance the rate of diagnosis among MSM populations and promote timely linkage to preventive and curative services. However, implementing HIVST should be informed by context-specific factors, and research on its effectiveness in different cultural contexts is necessary. A comprehensive strategy for HIV prevention among MSM populations could involve a multifaceted approach that addresses structural and contextual barriers to testing and treatment. This can only be achieved through the coordinated efforts of policymakers, health care providers, and affected communities.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883241276436 – Supplemental material for Prevalence of HIV Self-Testing Among Men Who Have Sex With Men: Evidence Synthesis by Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-jmh-10.1177_15579883241276436 for Prevalence of HIV Self-Testing Among Men Who Have Sex With Men: Evidence Synthesis by Systematic Review and Meta-Analysis by Rekha Dutt, Kapil Goel, Muhammad Aaqib Shamim, Shalini Singh, Bijaya Kumar Padhi, Vaibhav Prakash Anjankar and Aravind Gandhi P. in American Journal of Men's Health
Footnotes
Contributors
R.D. and K.G. conceptualized the study and designed the protocol. R.D. and M.A.S. did the PROSPERO registration. R.D., K.G., S.S., and M.A.S. did the literature review, collected data, and assessed the quality of the studies. R.D. and V.P.A. verified the data. M.A.S. and B.K.P. analyzed the data. M.A.S. and A.G. interpreted the results. M.A.S., A.G., R.D., and V.P.A. wrote the initial draft of the manuscript. All the authors have reviewed, edited, and provided critical comments. All authors had full access to all the data in the study and had the final responsibility for the decision to submit for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The publication of this article is funded by Datta Meghe Institute of Higher Education and Research, Wardha, India.
Ethical Statement
An ethical review does not apply to this study since it used data that is available in published literature.
Trial Registration
Data Sharing Statement
Documents containing all the extracted data have been made available in the manuscript and accompanying supplementary material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.