
Abstract
People who are incarcerated have a disproportionately high risk of contracting human immunodeficiency virus (HIV). While there is no known cure for HIV, there are biomedical approaches that can successfully manage the virus and prevent its transmission. A total of 267 men who are incarcerated completed a cross-sectional survey focused on cancer health, HIV prevention, and mental health in three state prisons. The mean age was 39 years. The majority had an annual income of US$10,000 or less, self-identified as heterosexual, not married, had children, did not have any military status, and identified as African American/Black. Less than 4% indicated that they had heard about Pre-Exposure Prophylaxis (PrEP), and only 3% had heard of Post-Exposure Prophylaxis (PEP). PrEP and PEP effectively prevent HIV infection, but little attention has focused on increasing the knowledge and awareness of these HIV prevention interventions in the incarcerated population.
Introduction
While there is no known cure for human immunodeficiency virus (HIV), there are biomedical approaches to manage, prevent HIV and prolong life (Del, 2014; Mayer et al., 2010). The primary biomedical approaches for HIV prevention include: Treatment as Prevention (TasP), Pre-Exposure Prophylaxis (PrEP), and Post-Exposure Prophylaxis (PEP) (Mayer et al., 2010). TasP refers to a person living with HIV taking antiretroviral therapies (ART) to prevent HIV transmission. ART reduces the HIV viral load in blood to undetectable levels, thus making the possibility of transmission to a person living without HIV very low (Padian et al., 2008).
In 2012, the U.S. Food and Drug Administration approved PrEP, a daily oral pill, to address the prevention needs of people living without HIV (Fonner et al., 2016; Huang et al., 2018). Results from the PrEP clinical trials indicate it is safe to be taken daily and has been reported to reduce the risk of HIV infection through sexual intercourse among men who have sex with men/same-gender-loving men (MSM)/(SGLM) (Grant et al., 2010), transgender women (Shieh et al., 2019), and people who inject drugs (PWID) (Alistar et al., 2014; Beyrer et al., 2012).
PEP is an ART administered to someone when they have been potentially exposed to HIV (Centers for Disease Control and Prevention [CDC], n.d.). PEP is often used to prevent HIV infection in emergencies, including, but not limited to, sexual assault or sharing needles (World Health Organization [WHO], n.d.). PEP must be initiated within 72 hr of potential HIV exposure and is often compared with “Plan B,” the “morning-after” contraceptive pill, because both require administration within a 72-window period of potential exposure. PEP is a standard treatment in occupational and medical settings (WHO, n.d).
To reduce HIV infection, biomedical approaches to prevent HIV (i.e., TasP, PrEP, and PEP) must be targeted at vulnerable and marginalized groups at risk of transmission, including people who are incarcerated. The Joint United Nations Program on HIV and AIDS (UNAIDS, 2019), the leading advocate for rapid, coordinated policy initiatives responding to the HIV/AIDS pandemic, indicated that incarcerated people are 5 times more likely to be infected by HIV compared with those who are not incarcerated. In addition to incarcerated people, other vulnerable populations include MSM, SGLM, PWID and sex workers (UNAIDS, 2019). These marginalized groups are also significantly overrepresented among incarcerated people. As condoms and safe injection sites are not available in most prisons settings, people who are incarcerated are at higher risk of HIV than the general community (Dean et al., 2005; UNAIDS, 2019). HIV transmission within prison populations has been difficult to report due to low HIV testing, ethical issues, and medical mistrust of prison authorities (Seal et al., 2010; Westergaarda et al., 2013). These issues result in less reporting of condomless sex or intravenous drug use. HIV transmission rates are further exacerbated by the rapid turnover of inmates from incarceration to either release or transfer to other facilities (Hammett, 2006).
As people who are incarcerated are disproportionately impacted by HIV infection (Dean et al., 2005; Hammett, 2006; UNAIDS, 2019), there is a need for HIV prevention education in correctional settings focused on biomedical approaches (Alistar et al., 2014; Baral et al., 2012; Dolan, 1997; Grant et al., 2010; Shieh et al., 2019). Specifically, the little research on PrEP knowledge among incarcerated populations suggests low uptake (Brinkley-Rubinstein et al., 2020). This study describes the PrEP and PEP knowledge of men incarcerated in three U.S. state prisons to better understand specific knowledge gaps and limitations to future uptake of PrEP among incarcerated men.
Method
Study Design
The Cancer Risk in Incarcerated Men’s Study (CRIIMS) was a two-phase, multi-method research project that examined tobacco, cancer health, and psychosocial factors related to health behaviors among men incarcerated in three state prisons in the Northeastern region of the U.S. (Valera et al., 2020). For additional details of Phase II, the cancer education program’s adoption in these facilities, see Valera et al. (2019). Human subjects’ approval for this study was granted by Rutgers University Institutional Review Board (IRB# Pro20170001184), the participating states’ Departments of Corrections, and the U.S. Office for Human Research Protections. Phase I of the study entailed recruiting and screening male inmates for study participation. There were 356 inmates recruited in this phase, 89 men did not meet the eligibility criteria. Participant eligibility criteria were as follows: (a) male; (b) at least 18 years old; (c) self-report use of cigarettes or another form of tobacco before incarceration; (d) self-identify as Black, Latino, White, or Other; (e) fluent in either English or Spanish. Written informed consent was obtained for the remaining 267 participants, who completed a cross-sectional survey that assessed their knowledge, attitudes, and beliefs related to tobacco, substance use treatment, physical health, psychosocial factors, and other lifestyle behaviors that contribute to cancer risk.
CRIIMS Phase I Recruitment Strategy
CRIIMS used several methods to recruit Phase I study participants. Prison counselors and correctional officers posted fliers and advertisements about the study on bulletin boards, cellblocks, and housing units. Prison officials also included a memo about the study on the TV broadcast system in two of the state prison facilities. Individuals interested in the CRIIMS study were instructed to contact the prison liaison, generating a callout list. Afterward, the research team was invited to meet potential participants on the callout list to discuss the study.
CRIIMS Phase I Questionnaire
In Phase I, 267 eligible study participants completed a paper-based, cross-sectional survey. The questionnaire included several standardized measures and was designed to describe various demographic characteristics of the participants. These characteristics included race and ethnicity, smoking status, education level, physical and medical health status, educational training opportunities during incarceration, and employment status. Other characteristic information that was gathered included: incarceration experience, prison conditions and treatment, tobacco and cancer health, psychosocial factors, health behaviors, and physical and mental health outcomes. The present study reports on demographic characteristics, knowledge, and awareness of HIV, PrEP, and PEP in Phase I of the parent study.
Measures
Demographic Characteristics
Race and ethnicity, age, education, income, sexual orientation, number of children, military status, marital status, and health condition were reported.
HIV Awareness
Participants were asked about their HIV status, whether HIV testing was performed during incarceration, the age they were diagnosed with HIV, and whether they were currently taking ART.
HIV Knowledge
HIV knowledge was assessed by asking participants about the myths, misconceptions, and facts about HIV. Participants responded to five statements by indicating “true,” “false,” or “I don’t know” on items related to HIV acquisition (Only people who have sex with others of the same sex get HIV/AIDS); how HIV is spread (Only people who look sick can spread the HIV/AIDS virus); birth control (Birth control pills protect women from getting the HIV/AIDS virus); ART (There are drugs available to treat HIV that can lengthen the life of a person infected with the virus); and the cure (There is no cure for AIDS).
Hepatitis C (HCV) Screening
Participants were asked whether they were tested for HCV during incarceration. They were also asked how long ago they had an HCV screening test done, their HCV status, and if positive for HCV, were they taking medication to treat it.
PrEP and PEP Knowledge and Awareness
PrEP and PEP knowledge was assessed using two questions: Have you ever heard of pre-exposure prophylaxis or PrEP? Have you ever heard of post-exposure prophylaxis or PEP? We asked them an open-ended question if they marked yes, “Can you tell me what you know about PrEP or PEP?”
Results
Demographics
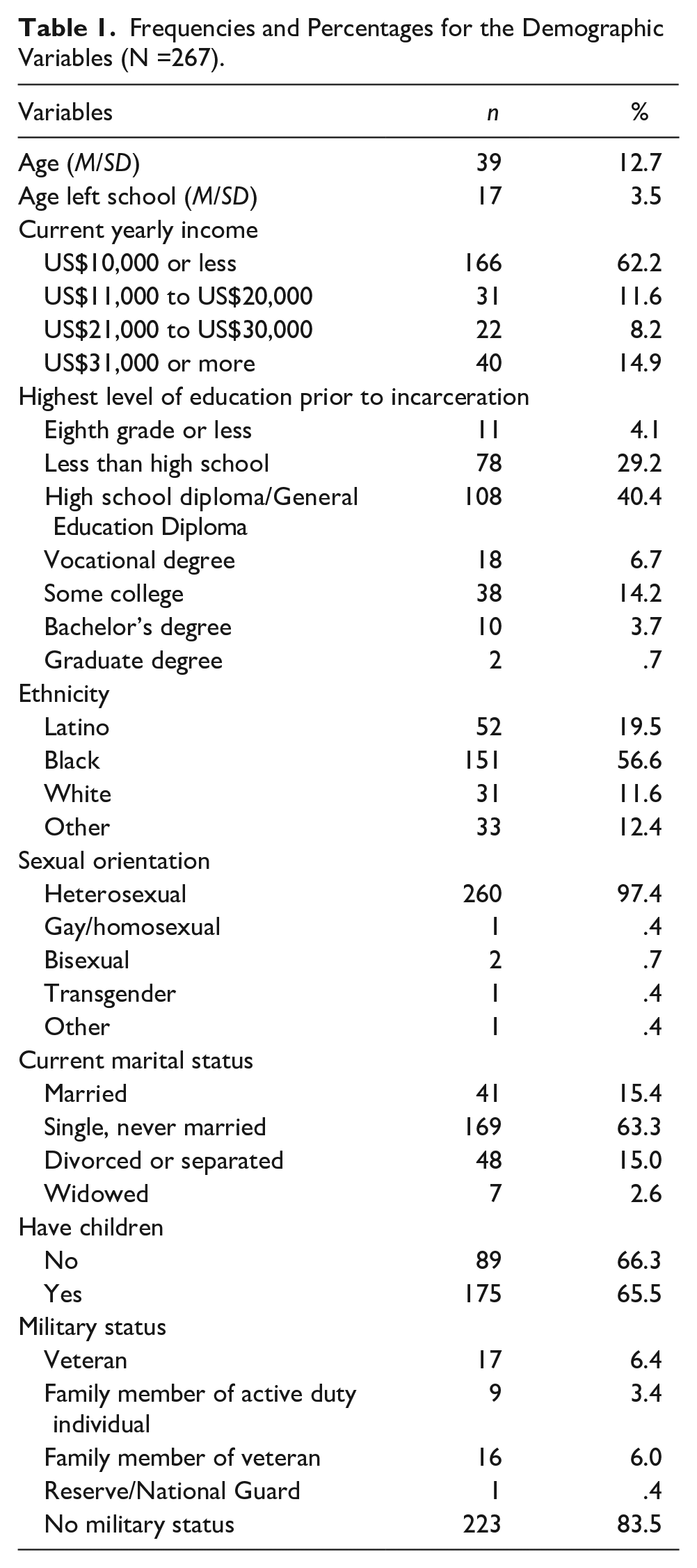
The study participants’ mean age was 39 years, and on average, respondents left school at age 17. Most respondents had an annual income of US$10,000 or less (n = 162; 62%), self-identified as heterosexual (n = 260; 97%), not married (n = 226; 84%), had children (n = 175; 65%), did not have any military status (n = 223; 83%), and the majority of respondents identified as Black (n = 151; 57%). Table 1 reflects the additional demographic characteristics of the study participants.
Frequencies and Percentages for the Demographic Variables (N =267).
Health Conditions
Most men self-reported average levels of health or better (n = 248; 93%), no physical disability (n = 183; 68%), and did not report having a diagnosis of cancer or HCV. The findings in Table 2 reveal that more than half of the sample (n = 143; 53.5%) had health insurance.
Frequencies and Percentages for the Health Measures (N =267).

Note. VA = Veterans Affairs.
HIV Variables
Most participants had received an HIV test (n = 245; 92%). Of those who self-disclosed their HIV status, the mean age of diagnosis was 38 years (see Table 3). In addition, the HIV knowledge scores, ranged from 0 to 5; the mean score was 3.78 (SD = 0.87), indicating low to moderate scores on HIV knowledge.
Frequencies and Percentages for the HIV Variables (N =267).

Note. HIV = human immunodeficiency virus.
N = 14.
HCV Status
Many participants had an HCV screening test performed (n = 171; 64%) and did not have HCV. See Table 4 for the range of responses as to when the screening test was conducted. A total of two (0.7%) respondents were currently taking medication for HCV infection.
Frequencies and Percentages for Hepatitis C Measures (N =267).

PrEP and PEP Knowledge
Only 3.7% (n = 10) of participants indicated that they had heard about PrEP, and only 3% (n = 8) of participants noted that they had heard of PEP (see Table 5). Among those who said they had heard of PrEP, the participants indicated that PrEP is: (a) A shot you take beforehand due to high-risk occupation; (b) Prevents you from getting HIV; (c) Using a condom or other preventive steps against harm; (d) Can prevent HIV if taken regularly; and (e) Morning-after pill or equivalent. Among participants who reported hearing about PEP, they noted that PEP is: (a) one pill that stops you from getting HIV; (b) A shot after questionable unprotected exposure to another human being or a possible exposed item; (c) You take after being exposed to the virus; and (d) To keep safe.
Frequencies and Percentages for PrEP and PEP Variables (N =267).

Note. PrEP: pre-exposure prophylaxis; PEP = post-exposure prophylaxis.
Assessing the Relationship Between Age, Knowledge About PrEP and PEP, and HIV Knowledge
The sample was divided into approximately three age groups: 19 to 32 years, 33 to 43 years, and 44 years and older. Cross-tabulation with chi-square procedures was conducted to determine whether PrEP and PEP knowledge differed across age groups. The findings reveal that PrEP knowledge did not differ significantly across age groups, χ2(2) = 0.37, p = .831. Similarly, PEP knowledge did not differ significantly across age groups, χ2(2) = 1.29, p = .526.
To determine whether HIV knowledge scores differed across age groups, a nonparametric Kruskal–Wallis procedure was conducted (due to the distribution of HIV knowledge scores being highly skewed). The findings revealed that HIV knowledge differed significantly across age groups, KW(2) = 6.70, p = .035. Adjusted pairwise comparison procedures indicated that respondents aged 19 to 32 years (M = 3.55, SD = 1.06) had significantly lower HIV knowledge scores than respondents aged 33 to 43 years (M = 3.96, SD = 0.59), p = .039.
Assessing the Relationship Between Race/Ethnicity, Knowledge About PrEP and PEP, and HIV Knowledge
Cross-tabulation with chi-square procedures was conducted to determine whether PrEP and PEP knowledge differed across race/ethnicity. The findings reveal that PrEP knowledge did not differ significantly across race or ethnicity, χ2(3) = 3.24, p = .357. Similarly, PEP knowledge did not differ significantly across racial groups, χ2(3) = 5.92, p = .116.
A nonparametric Kruskal–Wallis procedure was conducted to determine whether knowledge scores differed across race and ethnicity. The findings revealed that HIV knowledge did not differ significantly across ethnicity, KW(3) = 3.50, p = .320.
Assessing the Relationship Between HIV Testing and Knowledge About PrEP and PEP
Cross-tabulation with chi-square procedures was conducted to determine whether PrEP and PEP knowledge differed across those who have been tested for HIV. The findings revealed that PrEP knowledge did not differ significantly across those who were tested for HIV, χ2(1) = 10, p = .748. Furthermore, PEP knowledge did not differ significantly across those who received HIV testing during incarceration, χ2(1) = 0.32, p = .575.
Discussion
The present study investigated the PrEP and PEP knowledge and awareness of men incarcerated in three state prisons. Only two studies have explored PrEP understanding in people in the carceral system (Brinkley-Rubinstein et al., 2018, 2020). Consistent with the existing studies (Brinkley-Rubinstein et al., 2018, 2020), our findings indicate that incarcerated men have very low PrEP/PEP knowledge across age groups, demographics, and among those who were tested for HIV. Brinkley-Rubinstein and colleagues (2020) identified that 12% (n = 45) of participants knew about PrEP, while less than 4% (n = 10) in the present study knew about PrEP, and only 3% (n = 8) knew about PEP. Both figures suggested that knowledge of PrEP is very low among people who are incarcerated, and focusing on PrEP education would be a prudent use of social welfare resources to reduce HIV transmission in a high-risk population.
Although there are similarities between these two studies, there are also crucial differences. Brinkley-Rubinstein et al. (2020) screened 417 men during medical intake at the Rhode Island Department of Corrections (RIDOC). RIDOC is unique in that it is a combined jail and prison facility. In the screening, the researchers asked the men about their race and ethnicity, HIV risk factors (injection drug use, history of condomless sex with a man), perceived risk for HIV, history of testing for HIV, and interest in being tested for HIV while incarcerated. The participants were also asked about their knowledge of PrEP, their interest in learning more about PrEP, and whether they would take PrEP medication to prevent HIV.
The RIDOC study combines jail and prison inmates (Brinkley-Rubinstein et al., 2020), while the present study included only inmates housed in state prisons. In addition, the racial composition of these two studies is differ. Most participants in this study self-identified as Black (n=151; 57%), with significantly fewer respondents identifying as Latino (n = 52; 19%) and White (n = 31; 12%). The RIDOC study, however, had a much more racially heterogeneous population, with respondents identifying as White (n = 193; 47%) and remaining respondents identifying as either Black (n = 115; 28%) or Latino (n = 96; 23%) (Brinkley-Rubinstein et al., 2020). In addition, our study participants indicated a higher rate of previous HIV testing (n = 245; 92%) than in the RIDOC study (n = 239; 61%) (Brinkley-Rubinstein et al., 2020).
Limitations and Strengths of the Study
Although this present study contributes to the corrections and men’s health literature, it does contain some limitations. This research only included incarcerated men in state prisons. It did not include data on PrEP and PEP use in incarcerated women, limiting the study findings’ ability to generalize to other populations. Furthermore, the present study did not have questions about the behavioral risk of incarceration or HIV risk-taking behaviors, resulting only in its focus on knowledge and awareness of PrEP and PEP. The present study is unable to contextualize the findings beyond knowledge and understanding of PrEP and PEP.
Despite these limitations, this study has several strengths. The findings provide data reporting that most incarcerated men in this study have low knowledge of PrEP, PEP, and HIV in a population potentially at high risk of HIV transmission. The study also captures relevant demographic characteristics (e.g., educational attainment, income, marital status) and health status (e.g., health insurance coverage, HIV and HCV status, previous HIV and HCV testing) critical in understanding the context of HIV in the correctional setting.
The study participants faced significant societal barriers separate from incarceration; over half of the sample (n = 166) reported less than US$10,000 in income, and a combined 74% (n = 197) reported making US$20,000 or less. Approximately 33% (n = 89) of participants did not complete high school or receive a GED. This is limited income is particular concern as the generic Truvada (PrEP) is sold at an average retail price of US$1,860.13. Truvada must be taken for at least 28 days for therapeutic effect if administered as PEP. Furthermore, 32% (n = 85) of participants responded that they did not have health insurance coverage, and 31% (n = 82) reported a physical disability. These demographic characteristics should be considered beyond only focusing on behavioral risk-taking behaviors. Men who are incarcerated could benefit from a holistic approach to PrEP and PEP health education interventions, including ensuring that releases are enrolled in medical coverage.
Implications
PrEP and PEP knowledge hold future utility, as they can be used to inform interventions targeting populations within the justice system. Furthermore, linkage to PrEP and primary care services immediately upon prison release should be considered. Examples of these services include substance use treatment facilities, especially agencies offering Medications for Opioid Use Disorder (MOUD), and community-based medical clinics. Concentrating education resources around these services could help reach many newly released individuals. Additional future research involving incarcerated and formerly incarcerated populations would allow HIV prevention researchers to determine whether similar populations, such as women, gain knowledge about PrEP and PEP over time (Caponi et al., 2019; Collic, 2002). Additional studies would also permit HIV prevention researchers to examine whether there are persistent knowledge gaps among populations depending on their incarceration setting (i.e., prison vs. jail) (Valera et al., 2017).
Conclusion
People who are incarcerated bear a disproportionate burden of many health conditions, including HIV infection. Other marginalized populations that bear a disproportionate burden of HIV infection are overrepresented in the U.S. criminal justice system. PrEP and PEP are biomedical approaches that are effective in preventing HIV infection. Little attention has focused on increasing knowledge and awareness of these HIV prevention interventions in the incarcerated population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Health/National Cancer Institute to Dr. Pamela Valera (K22 CA197066).