
Abstract
The objective of the study was to assess the association between changes in plasma follicle-stimulating hormone (FSH) and the potential effect on idiopathic pulmonary arterial hypertension (IPAH) in male patients. A total of 116 male patients with IPAH and 53 healthy controls were included from XX Hospital. Plasma FSH concentration was assessed in all participants. Receiver operating characteristic curves were used to assess the mortality risk. Kaplan–Meier curve and Cox regression analyses were used to predict the value of FSH on the survival rate of male IPAH patients. The plasma FSH concentration in the IPAH group was significantly higher than that in the control group (p = .017). Nonsurvivors had significantly higher levels of FSH than survivors (p < .0001). FSH levels were positively correlated with World Health Organization Functional Class, mean pulmonary artery pressure, and pulmonary vascular resistance (PVR; p = .023, p < .0001, and p < .0001, respectively) and negatively correlated with 6-min walk distance (6MWD) and cardiac output (CO; p = .004 and p = .010). Cox regression model analysis showed that the levels of FSH were also the independent factors of mortality in male IPAH patients (p < .0001). The IPAH patients with higher FSH levels had higher PVR, lower 6MWD, CO, and a lower survival rate (p = .042, p = .003, p = .029, and p < .0001, respectively). Therefore, we identified that increased FSH levels were associated with disease severity in male patients with IPAH and independently predicted risk of disease and poor survival rate.
Keywords
Introduction
Idiopathic pulmonary arterial hypertension (IPAH) is a rare vascular disease whose main pathological feature is pulmonary vascular wall remodeling that leads to increased pulmonary vascular resistance, right ventricular hypertrophy, and ultimately, right heart failure and even death (Bienertova-Vasku et al., 2015). While epidemiological data report that pulmonary arterial hypertension (PAH) is more likely to occur in women, the prognosis in male patients is worse (Batton et al., 2018; Hester et al., 2019; Kjellström et al., 2019; Kozu et al., 2018). The changes in and potential roles of sex hormones and related metabolites in the pathogenesis of IPAH have attracted extensive attention. In previous studies, a great deal of work has been done on the potential role of sex hormones and their regulatory hormones in PAH and some progress has been made. Wu et al. (2018) explored pituitary–gonadal axis hormones in male PAH patients and reported that a higher estradiol/testosterone ratio and lower testosterone and progesterone levels were associated with the incidence of PAH (Wu et al., 2018). The study did not reveal the hormones that regulate the release of sex hormones. Follicle-stimulating hormone (FSH) is expressed differently in male PAH patients. FSH is a hormone synthesized and secreted by the pituitary gland. It is a glycosylated protein hormone and is named for its stimulating effect on the maturation of female follicles. FSH is an essential hormone in both men and women, regulating a series of physiological processes related to development, growth, puberty, sexual maturation, and reproduction (Das & Kumar, 2018). A large number of studies on cancer have identified that FSH receptors (FSHR) play an important regulatory role in blood vessels (Das & Kumar, 2018; Planeix et al., 2015; Wei et al., 2018; Z. Zhang et al., 2013). A study that analyzed sex hormone expression levels in female IPAH patients of reproductive age reported that high FSH expression indicated a high risk of morbidity and mortality in female IPAH patients of reproductive age (Y. Zhang et al., 2020). The potential impact of FSH on the level of changes and disease progression in male IPAH patients remains unclear. This study aims to explore the changes in plasma FSH levels in male IPAH patients and the effects on disease severity and prognosis in male IPAH patients.
Method
Study Sample
This study retrospectively included 116 male patients with IPAH who were admitted to XX Hospital from May 15, 2016, to August 13, 2020, with a mean ± standard deviation (SD) age of 42.3 ± 18.9 years. Inclusion was based on the diagnostic criteria of the European PAH guidelines, specifically, a mean pulmonary artery pressure >25 mmHg, as measured by right heart catheterization, and a pulmonary capillary wedge pressure ≤ 15 mmHg (Galiè et al., 2015). The exclusion criteria included pulmonary hypertension with a clear etiology (such as connective tissue disease and congenital heart disease), portal pulmonary hypertension, chronic pulmonary obstruction, chronic pulmonary thromboembolism, and left heart disease. We excluded patients with acute or chronic diseases that might affect hormone metabolism (e.g., acute or chronic infections, chronic autoimmune diseases, and previously identified primary endocrine diseases) and patients who received any hormone therapy (thyroid hormones, anabolic steroids, or corticosteroids) or medications that significantly inhibit hormone production during the study period or in the past.
Fifty-three men without IPAH who matched the IPAH group in health, age, sex, and geographical distribution were also included as controls. Cardiac, gynecological, and urological assessments were performed to ensure participants had no existing conditions that might affect plasma sex hormone concentrations. This study plan was approved by the Ethics Committee of XX Hospital (Ethics No. K12-089). Written informed consent was obtained from all participants prior to any study-related procedures.
Blood Collection and Testing
Venous blood samples were taken from all subjects and recorded relevant clinical information for subsequent studies. Plasma samples were prepared immediately, frozen at −20°C, and stored at −80°C until further analysis.
Test Index
The test indices used were heart rate, systolic blood pressure, diastolic blood pressure, and FSH concentration in both controls and patients with IPAH. In patients, the test indices also include N-terminal pro-brain natriuretic peptide (NT-proBNP), 6-min walk distance (6MWD), mean right atrial pressure (mRAP), mean pulmonary artery pressure (mPAP), pulmonary artery wedge pressure, pulmonary vascular resistance (PVR), cardiac index (CI), cardiac output (CO), and World Health Organization Functional Class (WHO-FC), which is used to evaluate the cardiac function of patients.
Measurements of Test Indices
Patients with IPAH underwent right heart catheterization 1 week after blood collection, and baseline hemodynamic indicators such as heart rate, systolic blood pressure, diastolic blood pressure, mean right atrial pressure, mean pulmonary artery pressure, pulmonary vascular resistance, and cardiac output were measured as described previously (Radu et al., 2010). No changes in patient clinical status were observed between blood sampling and right heart catheterization. Cubic CO was measured by cold isotonic sodium chloride solution thermal dilution method. PVR was calculated by dividing the difference between mPAP and pulmonary artery wedge pressure by CO. The WHO-FC was determined according to the European PAH guidelines (Galiè et al., 2015). Electrochemiluminescence immunoassays based on the Elecsys 1010/2010 system (Roche Diagnostics GmbH, Mannheim, Germany) were used to quantify total plasma FSH concentration.
Statistical Analysis
The data were expressed as mean ± SD, median and quaternary interval, or the percentages. The differences were examined using the independent t test, Mann–Whitney U test, chi-square test, or the appropriate Kruskal–Wallis analysis of variance. The correlations were evaluated using Pearson and Spearman correlation coefficients. Prognostic value was examined by Cox proportional hazards regression analyses. Receiver operating characteristic (ROC) curves were used to assess the cutoff values for the levels of FSH in patients with increased mortality risk. Survival curves were derived using the Kaplan-Meier method and were then compared with the log-rank test. The p value < .05 was considered statistically significant. Statistical analysis was determined with SPSS version 24.
Results
Clinical Features
We summarized the general clinical data and hemodynamic indicators of patients with IPAH and normal controls. Compared with the control group, the heart rate among patients with IPAH was higher, but the systolic and diastolic blood pressure were slightly lower in patients (p = .005, p = .001, and p = .030, respectively; Table 1). No significant differences were observed in age and body mass index between the two groups (p = .076 and p = .659; Table 1). Control subjects were all survivors. IPAH patients included 62 nonsurvivors and 54 survivors. There were significant differences of the nonsurvivor numbers between control subjects and patients (p < .0001; Table 1).
General Information on the IPAH and Control Groups.
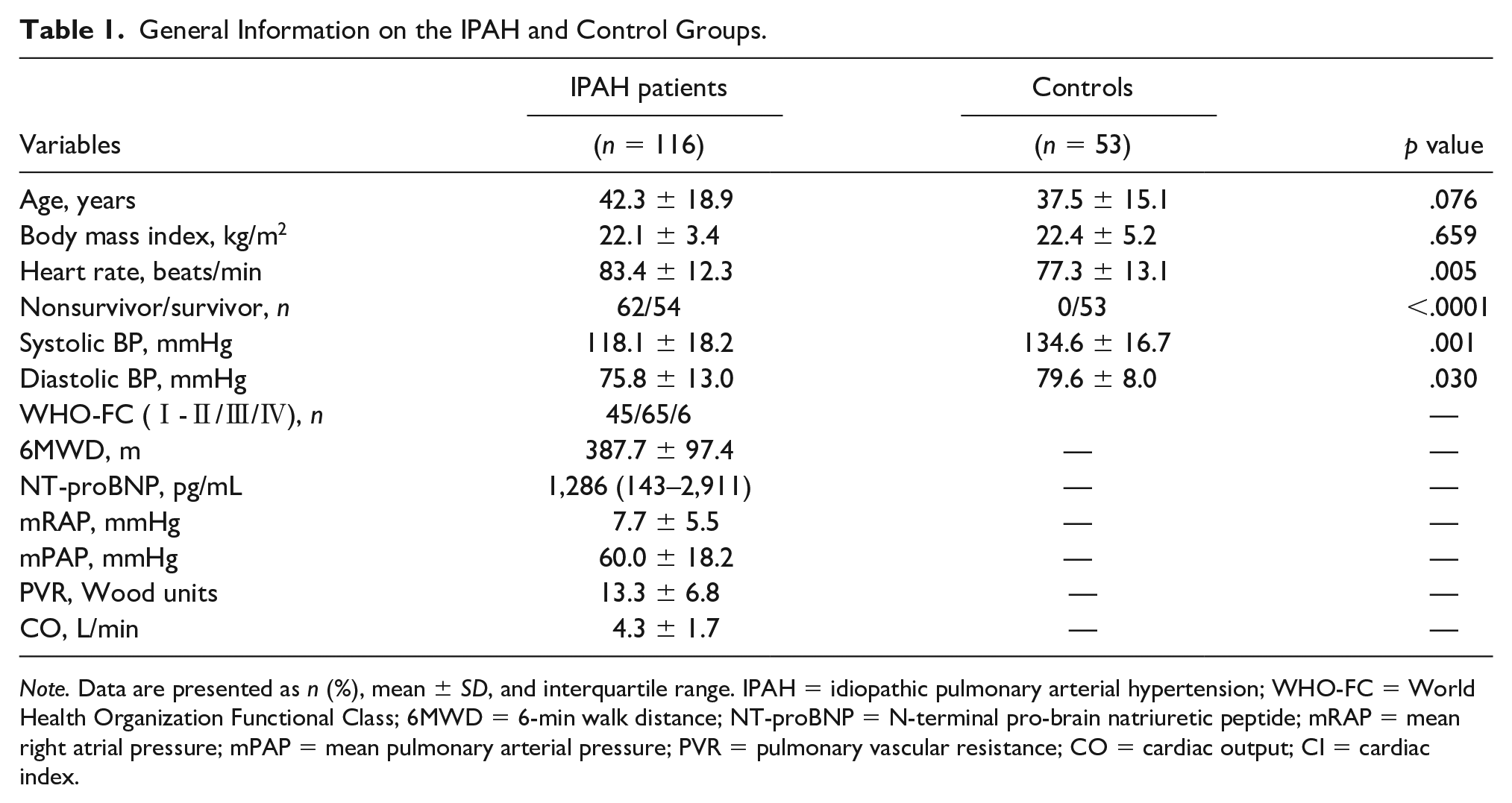
Note. Data are presented as n (%), mean ± SD, and interquartile range. IPAH = idiopathic pulmonary arterial hypertension; WHO-FC = World Health Organization Functional Class; 6MWD = 6-min walk distance; NT-proBNP = N-terminal pro-brain natriuretic peptide; mRAP = mean right atrial pressure; mPAP = mean pulmonary arterial pressure; PVR = pulmonary vascular resistance; CO = cardiac output; CI = cardiac index.
Comparison of FSH Levels Between Patients and Control Group
Plasma FSH concentrations in IPAH patients were significantly higher than those in the control group (p = .017; Figure 1A). The survivors with IPAH had significant lower plasma FSH concentrations compared with nonsurvivors in IPAH (p < .0001; Figure 1B).

Comparison of FSH Concentrations Between Controls and IPAH Patients: (A) Comparison of FSH Concentrations Between Controls and IPAH Patient and (B) Comparison of FSH Concentrations Between Nonsurvivors and Survivors With IPAH.
Correlation Analysis
We found mild to moderate negative correlations between the plasma FSH levels and 6MWD, CO, and CI in all patients (p = .004, p = .01, and p = .009, respectively; Figure 2). There were mild positive correlations between the FSH levels and WHO-FC in the patients (p = .023; Figure 2). We also observed moderate positive correlations between FSH levels and mPAP, and PVR in the patients (p < .0001 and p < .0001; Figure 2). There were no significant correlations in the plasma FSH levels with mRAP and NT-proBNP in these patients (p = .053 and p = .104; Figure 2).
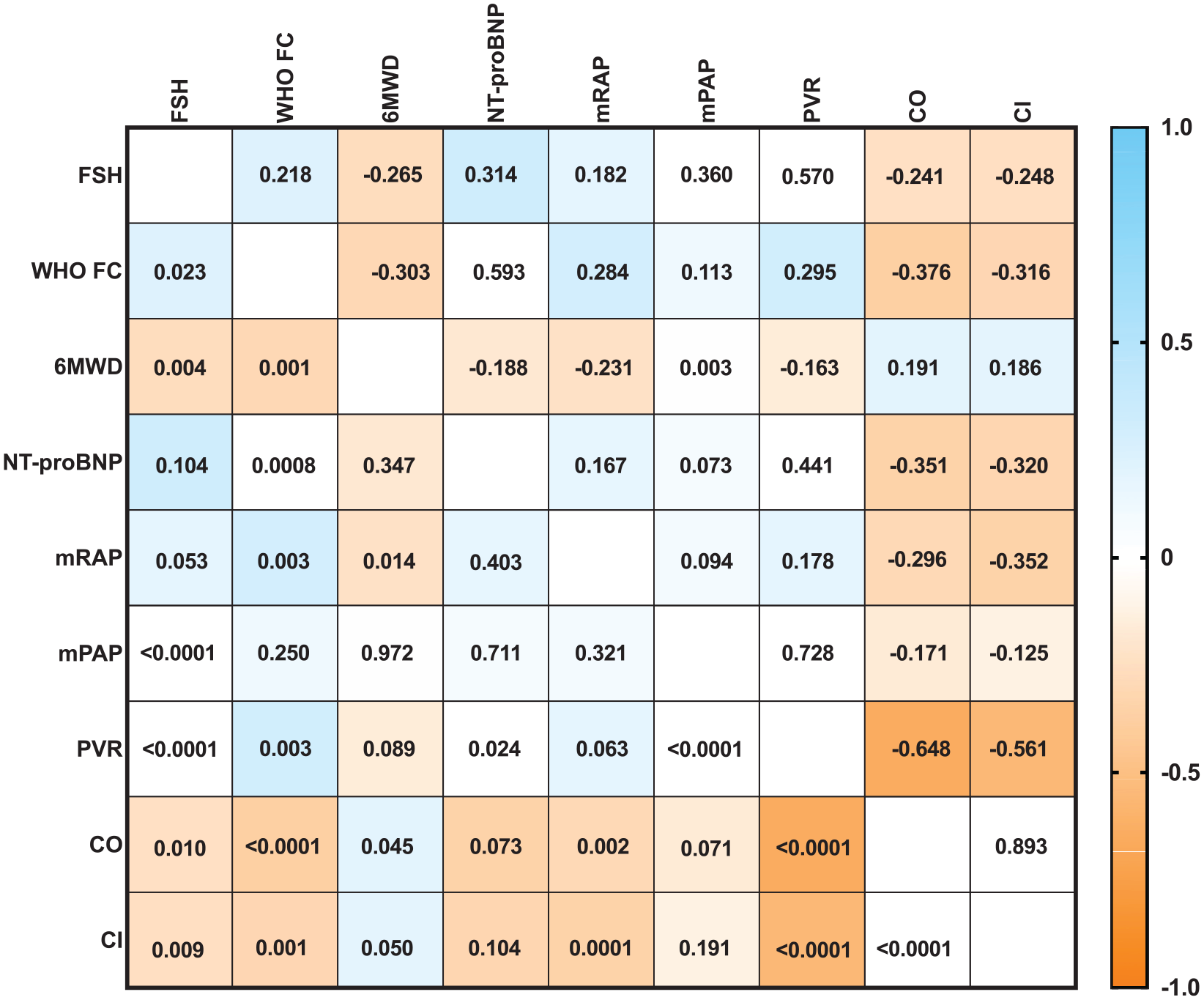
Correlation Between FSH and Various Clinical Parameters in All Patients With IPAH.
Univariate and Multivariate Cox Regression Analysis
In the univariate Cox proportional hazards analysis, WHO-FC, 6MWD, mRAP, mPAP, PVR, CO, and FSH levels were significantly related to mortality for all patients (p = .003, p < .0001, p = .002, p = .007, p < .0001, p < .0001, and p < .0001, respectively; Figure 3). And the multivariate forward stepwise Cox proportional hazards analysis revealed that 6MWD, CO, and FSH levels were independent predictors of survival for all patients (p = .006, p = .005, and p < .0001, respectively; Figure 3). 6MWD, CO, and FSH therefore play the significant roles in predicting the outcome of pulmonary hypertension (PH) in this cohort.

Univariate and Multivariate Cox Regression Analysis.
ROC Analysis
We performed ROC analyses to assess the sensitivity and specificity of FSH, CO, and 6MWD as predictors for the mortality of PH (Figure 4). FSH showed an area under the curve of 0.883 as a predictor of the mortality of PH (p < .0001; Figure 4). The ROC-optimal FSH cutoff value was 5.94, with a sensitivity and specificity of 78.7% and 88.0% respectively. CO could also be a predictor of the mortality of PH, with an initial cutoff value of 4.31 for predicting the mortality and a sensitivity and specificity of 62.0% and 77.0%, respectively (area under the curve = 0.732; p < .0001; Figure 4). In a further analysis, 6MWD showed an area under the curve of 0.715 as a predictor of mortality (p < .0001; Figure 4). The ROC-optimal 6MWD cutoff value was 415, with a sensitivity and specificity of 64.0% and 86.7%, respectively (Figure 4).

ROC Analysis of the Patient Group Based on FSH Concentration as a Predictor of Death.
Comparison of Clinical Features Between Patients With Low and High FSH Levels
To further verify the influence of FSH expression on the disease severity of IPAH, we divided the patients with IPAH into the low FSH group (FSH < 5.94 mIU/mL) and high FSH group (FSH ≥ 5.94 mIU/mL). The differences in several clinical parameters between the two groups were compared. 6MWD and CO in the low FSH group were significantly increased (p = .003 and p = .029; Figure 5A, C). Conversely, PVR was significantly decreased in the low FSH group (p = .042; Figure 5B).

Comparison of 6MWD, PVR and CO Between Male IPAH Patients With high and low FSH Concentration.
Kaplan–Meier Survival Curve
The Kaplan–Meier curve was used to analyze the predictive value of FSH expression on survival. IPAH patients with a low FSH level had significantly better survival than patients with a high FSH level. The Kaplan–Meier analysis indicated that the prognosis was significantly better for the IPAH patients with FSH relative levels <5.94 than for the IPAH patients with FSH relative levels ≥5.94 (p < .0001; Figure 6).

The Kaplan–Meier Survival Curves of Patients With Different FSH Concentration Levels.
Discussion
This study is the first known evaluation of FSH expression in male patients with IPAH. The results showed that FSH expression in male patients with IPAH was significantly higher than that in normal men. The study showed that the higher the FSH level, the lower the survival rate. Increased FSH levels were associated with severity and were an independent predictor for lower survival rate of patients with IPAH.
The results of a previous study reported that FSH expression in women of reproductive age with IPAH was significantly higher than that in healthy women of reproductive age, which confirmed sex differences reported in a number of clinical studies on IPAH (Y. Zhang et al., 2020). However, in another previous study on sex hormones and male PAH patients, no differences in FSH expression were reported between male PAH patients and normal men. This difference may be because IPAH is only one type of PAH and the pathogenesis may vary among the PAH subtypes (Wu et al., 2018). Male IPAH patients with low FSH expression were also found to have higher mortality and shorter survival during follow-up. More accurate prognostic analysis is thus needed to elucidate the sex differences in FSH expression in IPAH.
This study also found that male patients with low FSH levels had worse hemodynamic indicators such as mean right atrial pressure, pulmonary vascular resistance, and cardiac output. FSH concentration was significantly negatively correlated with mean right atrial pressure, mean pulmonary arterial pressure, and pulmonary vascular resistance. That is, decreased FSH expression results in increased pulmonary blood vessel pressure and decreased cardiac output. These results indicate that FSH is strongly associated with the deterioration of pulmonary vascular and cardiac function in male IPAH patients, but the specific mechanism remains to be further explored. Although no direct evidence has been obtained on the role of FSH in IPAH, FSH has been reported to modulate vascular function in cancer patients. Li et al. (2017) identified that FSH could accelerate the occurrence of atherosclerosis by increasing VCAM-1 expression in endothelial cells. Serviente et al. (2019) reported a significant negative correlation between FSH and blood flow–mediated vasodilation in women with high cardiopulmonary fitness. These previous study findings indicate further elucidation of FSH expression in pulmonary vessels and heart tissues in PAH and its influence on FSH function in subsequent studies.
This study has some limitations. First, considering it was a retrospective study, the elucidation of the underlying mechanism of action involved was not an objective of the study. The association found in this study cannot infer causation because the sample size was small, and whether impaired sex hormone levels are a common phenomenon in the course of IPAH disease could not be determined. Second, we did not investigate the levels of FSH in lung tissues or pulmonary artery smooth muscle cells (PASMCs) of patients, which were significantly correlated with dysfunction. However, the specific mechanisms involving FSH and the changes in cell phenotypes could not be clarified.
Conclusion
In conclusion, this study preliminarily revealed that FSH levels were significantly correlated with disease severity in male patients with IPAH. Particularly, men with higher FSH levels had a lower survival rate in IPAH. However, the specific mechanisms involved need to be investigated in further studies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Program of National Natural Science Foundation of China (81870042), Program of Shanghai Pulmonary Hospital (FKLY20005), Program of Natural Science Foundation of Shanghai (21ZR1453800).