
Abstract
Purpose
Data on colorectal cancer in Malaysia, particularly from southern regions such as Johor Bahru is underreported. To address this gap, we conducted a retrospective review of colorectal cancer patients treated in Johor Bahru 5 years ago.
Methods
The study included patients with colorectal cancer in year 2017 or 2018. We included only 63 patients with complete data. Patient’s sociodemographic features and clinical characteristics including site of tumour, staging, symptoms at presentation, and management/types of surgery was recorded and analysed in this study.
Results
There were 43 male and 20 female patients. The median age were 63 years, IQR = 55 -71. Chinese patients were disproportionately higher (60.3%), followed by Malay (36.5%). The tumor site is more often found in sigmoid (27.0%) and mid-rectum (22.2%). Anterior resection (74.6%) is the most frequently performed surgery. The 5-year survival rate of colorectal cancer patients was 63.5%. The 5-year survival rate of patients with stage I, stage II, stage III and stage IV disease were 66%, 81.8%, 68.6% and 0% respectively.
Conclusion
The clinical features of colorectal cancer in Johor Bahru closely resemble those in other regions of Malaysia. The survival rates among colorectal cancer patients in Johor Bahru, particularly in stages 1 and 4, are unexpectedly lower. This discrepancy in oncologic outcomes could be attributed to a small sample size. Therefore, the establishment of a unified surgical registry for all colorectal surgeries across Malaysia is recommended.
Introduction
Incidence of colorectal cancer may vary based on the economic and development status of the nation. Reported incidence rates of colorectal cancer in high income nation is approximately 40 to 45 cases per 100,000 persons. On the other hand, middle and low-income countries may observe as low as 3 to 4 cases per 100,000 persons. 1 This discrepancies of incidence rate between low and high income countries may attributed to lack of screening in diagnosis colorectal cancer; therefore the incidence may be hidden with only tip of iceberg being treated. 1 In Malaysia, we observed a higher incidence rate of 21.32 cases per 100,000, with its peak reported in the Chinese ethnicity at 27.35, followed by the Malays at 18.95, and the Indians with 17.55 cases per 100,000 persons. 2
The distribution by local population ethnicity and covering colorectal surgeon is disproportionate in several regions of Malaysia. Currently, there are higher number of colorectal surgeons in central part of Malaysia (Kuala Lumpur, Selangor) with higher proportion of Malay ethnicity in Northern part of Malaysia (Kedah, Kelantan). In major state of Kuala Lumpur alone, there are two university hospitals with colorectal surgery services and the reported 5-year survival rate of colorectal cancer was 60.5%. 3 In Seremban, the survival rate was reported to be 46.5% 4 and Kelantan was 34.3%. 5
The differing survival outcomes following colorectal surgery treatment may be attributed to variations in demographics, pre-existing health conditions, timing of diagnosis, and accessibility to early diagnostic and treatment options. Previous studies on colorectal cancer treatment outcomes have predominantly focused on the northern and central regions of Malaysia.3–5 Recognizing this gap, we aim to present the outcomes of colorectal cancer patients specifically from the southern state of Malaysia, Johor Bahru. This study seeks to characterize the demographics, clinical patterns, treatment trends, and retrospectively review the 5-year survival rates of colorectal cancer patients in this region.
Method
This retrospective series examines all colorectal cancer patients admitted to Hospital Sultanah Aminah in Johor Bahru between 2017 and 2018. The hospital has offered colorectal surgery services since 2009, predominantly led by a trained colorectal surgeon. In emergency scenarios, general surgeons primarily conducted colorectal cancer surgeries, with common procedures including transverse colostomy, right or left hemicolectomy, or Hartmann procedure. Elective colorectal cancer surgeries were mostly performed by colorectal surgeons, though some colectomies were conducted by general surgeons.
Patient data were retrieved retrospectively from handwritten records in the general surgery ward census database, excluding those diagnosed prior to the specified period due to extensive missing data. Hospital records containing information on demographics, comorbidities, diagnosis date, biopsy results, presenting symptoms, tumor location, clinical staging, surgical procedures, primary cause of death, and survival duration were anonymized and entered into a data proforma.
Follow-up was conducted through telephone interviews until death or the study’s endpoint, set at December 31, 2022, with patients’ statuses recorded as deceased or alive at this date. Analysis compared ethnicity, age, presenting symptoms, and clinical staging between deceased and surviving subjects.
The study protocol was reviewed and approved by the local hospital review board, with informed consent waived due to anonymization of patient details. Compliance with the principles of the Declaration of Helsinki was ensured by the Institutional Review Board.
Results
Clinical characteristics of colorectal cancer patients in Hospital Sultanah Aminah, Johor Bahru, 2017 to 2018
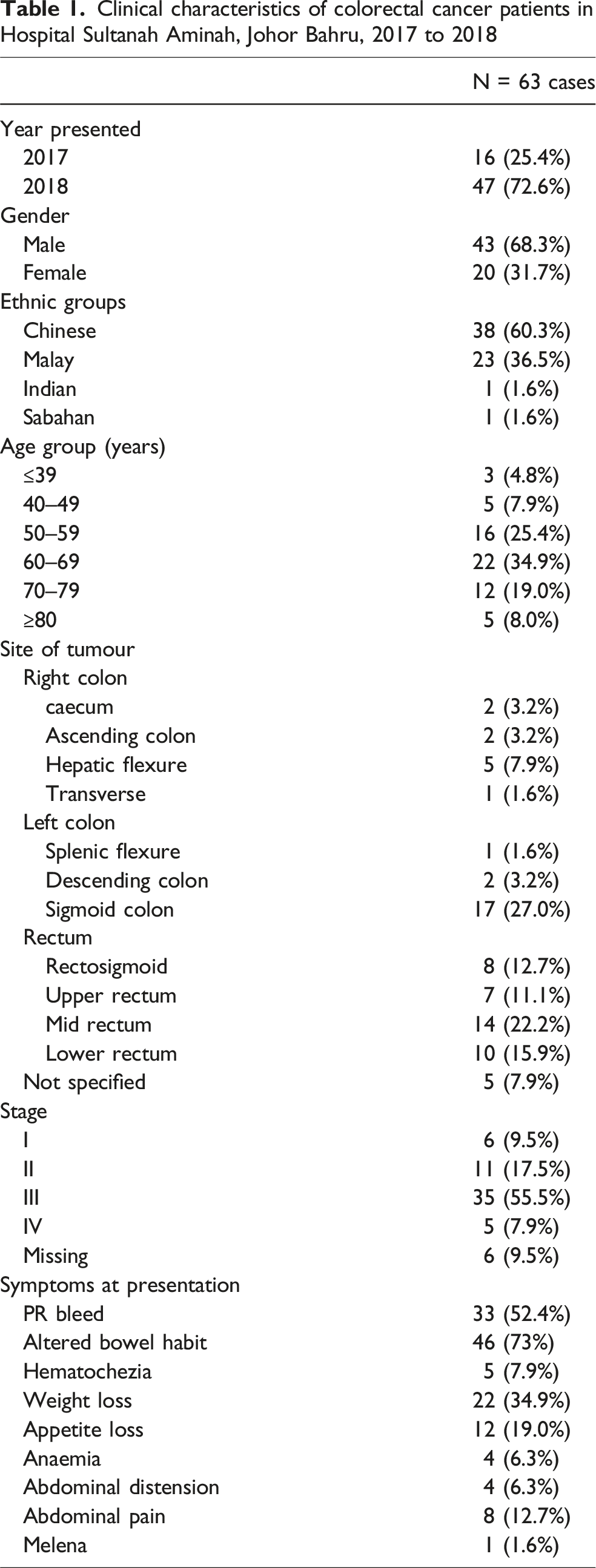
Commonest site of tumour was located at sigmoid colon (27 %) and followed by mid rectum at 22.2 %. Most of the patients (n = 34) were diagnosed at stage 3 amounting to up to more than 50%., and five patients were diagnosed at stage 4 (Table 1). The common presenting symptoms were altered bowel habit (n = 46), per rectal bleeding (n = 33) and weight loss (n = 22). (Table 1).
Types of surgery performed

*It was noted that some patients underwent more than 1 type of surgery.
Staging at Diagnosis of colorectal cancer patients in Hospital Sultanah Aminah, Johor Bahru 2017-2018

Discussion
The estimated 5 years survival rate of colorectal cancer for all stages in current series is 51.6%, similar to other series from central and northern Malaysia with rates of 34% to 60.5%.3–8 It is observed that there is lower survival rate in stage 1 and stage 4 (Table 3). This rate may be skewed due to lower sample size in these stages. In stage 2 and 3 alone, the survival rate of 81.8% and 68.6% for 5 years is close to the national registry and regional series nationwide. 9 When look into individual death for patients in stage 1 category, there were unrelated from the cancer. The stage distribution in current series is skewed with small numbers of stage 1 and stage 4 disease (Table 3). The underreporting of the stage 4 cancers may be due to local policy as these patients may be treated non-operatively by general surgeon without referral to colorectal surgeon, as such these cases may not be captured during the retrospective review. Upon reviewing the data from Stage 1, the causes of death for the four cases were identified as follows: advanced prostate cancer, ischemic heart disease, end-stage renal failure, and disease progression in a patient with poorly differentiated squamous cell carcinoma of the anorectum, who had defaulted on treatment.
In Stage 4 cancers, all cases demonstrated liver metastasis. Additionally, two cases exhibited lung metastasis, and one case had ovarian metastasis.
The clinical characteristic of current cohort of colorectal cancer patients showed consistent trend with other Malaysian series. It is observed 87.3% of the subjects were age more than 50 years, comparable to the National Cancer Registry database which reported 81.7% aged of 50 or above. 9 These patients often present late with altered bowel habit, per-rectal bleeding and abdominal pain 10,11. There is a male preponderance of 68.3% slightly higher than observed in other series in Seremban at 59.3% 4 and Alor Setar at 55.9% 9 The Chinese had a proportion of 60% of colorectal cancer in current series; and this is not in accordance with the racial composition in Johor Bahru with Malay predominant (Malay 53.3%, Chinese 30.3%, Indian 6.5%). 8 The higher proportion of Chinese race with colorectal cancer may suggest inherent genetic predisposition or dietary relationships for cancer development. This may need further local genomic epidemiology study to confirm it. [2] The common tumour locations in current series show no differences from usual pattern which are sigmoid and rectal tumours. 4 Hence, majority of these patients had anterior resection (Table 2).
From this current analysis, only 63 subjects from 2017 to 2018 was identified and included for the analysis. This is fraught with multiple local limitations in data collection together with a great extent of missing data. As the hospital records were kept in traditional handwritten format, the tracing was made difficult due to poor documentation, poor record keeping and missing operative data. 12 This numbers may be not reflect the true admissions due to colorectal cancers as in comparison, the local surgeon’s logbook observed at least 100 new cases of colorectal cancer operated in 1 year. Hence, there is a high rate of underreporting of the actual colorectal cancer in 2017 to 2018. Nonetheless, current dataset from these 63 subjects allow a clinical trend to be presented and discussed.
Conclusion
In Johor Bahru, colorectal cancer patients exhibit clinical characteristics similar to those in other states of Malaysia. Predominantly male and typically aged over 50 years, they often present at advanced stages (3 and 4) with symptomatic manifestations. The most common tumor location is in the rectum or sigmoid, and anterior resection emerges as the primary surgical intervention. Notably, there is a higher prevalence of colorectal cancer among individuals of Chinese ethnicity.
Survival rates at 5 years for stage 2 and 3 stand at 81.8% and 68.6%, respectively. However, due to limited sample size, conclusive survival rates for stage 1 and 4 remain elusive. We advocate for further prospective series encompassing all surgical centers that perform colorectal cancer surgeries across the country.
Footnotes
Author contributions
Conceptualization: TJH.
Data curation: TJH, RLZM.
Formal analysis: TJH, HZA, KTJL, LYS, AS, ARAL, CSY, KLKL, ICJL.
Funding acquisition: TJH.
Investigation: HZA, KTJL, LYS, AS, ARAL, CSY, KLKL, ICJL.
Methodology: TJH, HTCL, CKK.
Project administration: TJH, HTCL, CKK.
Visualization: TJH, HTCL, CKK.
Writing–original draft: TJH, HZA, KTJL, HTCL, CKK.
Writing–review & editing: TJH, HTCL, CKK.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.