
Abstract
Impairment of social functioning and low economic status may lead to the development of cardiovascular disease (CVD). This study aimed to evaluate the relationship between socioeconomic status (SES) and erectile dysfunction (ED) in patients with clinically significant CVD. A total of 808 male patients with ischemic heart disease (IHD) were recruited. Socioeconomic and demographic data as well as occupational data and the presence of modifiable risk factors were collected. Erection quality was assessed using the International Index of Erectile Function 5 (IIEF-5), while physical activity was evaluated using a modified Framingham questionnaire. Relationships among the presence of socioeconomic factors (marital status, education, income, occupational status, nature of work conducted, and demographic data), intensity of ED, and time from diagnosis of IHD were assessed. ED was diagnosed in 618 men (76.49% overall; severe in 23.14%, moderate to severe in 13.11%, moderate in 32.20%, mild in 31.55%). Patients with ED were older (61 ± 8.6 vs. 53 ± 9.1 years; p < .0001), were less active (6.97 ± 2.18 vs. 8.31 ± 2.34 Metabolic Equivalent [METs]; p < .0001), and had more modifiable risk factors (3.4 ± 1.1 vs. 3.2 ± 1.0; p < .0300). Higher education was associated with a lower probability of the occurrence of ED (OR = 0.7546; 95% CI [0.6221, 0.9153]). In patients with newly diagnosed IHD, SES correlated significantly with the presence of ED (p = .009). Education in patients suffering from CVD has a significant relationship with both the occurrence and degree of ED. Economic status was significantly linked to the presence and degree of ED only in patients with IHD diagnosed less than 2 months before entering the study.
Keywords
Dysfunction in social circles can lead to the development of chronic diseases, and cardiovascular disease (CVD) is often among them. In recent years, a stronger focus has been placed on socioeconomic status (SES) as a risk factor for CVD. The correlation between SES and the risk of CVD was described by Holme et al. in the year 1976. In that study, an almost two times higher risk of ischemic heart disease (IHD) was observed in men with a low SES compared to men with a higher SES (Holme, Hjermann, Helgeland, Lund-Larsen, & Leren, 1976).
Several epidemiological studies have also confirmed the correlation between a low SES and higher incidence rates of CVD (Brennan-Olsen et al., 2015; Mackenbach, Cavelaars, Kunst, & Groenhof, 2000). In addition to studies on the relationship between SES and clinically significant CVD, we also found studies evaluating the influence SES has on early preclinical forms of atherosclerosis, such as changes in the intima–media complex or erectile dysfunction (ED). Their occurrence is linked closely with the difference in physiology of circulation in arteries supplying the corpus cavernosum of the penis, in which the dysfunction of the epithelium and repeatedly disabled vessel relaxation leads to hemodynamic disruptions and ED (Kaiser et al., 2004; Lue et al., 2004; Montorsi et al., 2003). Available studies evaluate the connection between SES and the risk of occurrence of ED in men (Hosain, Latini, Kauth, Goltz, & Helmer, 2013; Martin et al., 2014; Weber et al., 2013).
The presence of ED was identified as a cardiovascular risk factor (Hippisley-Cox, Coupland, & Brindle, 2017; Uddin et al., 2018); however, the literature lacks reports that evaluate the interconnection between SES and ED in groups of patients with clinically significant CVD, a high percentage of whom suffer from ED. Despite angiographically confirmed atherosclerotic changes, not all patients with CVD present with ED. This raises the question as to what influence SES has on the occurrence and degree of ED, which negatively affects cardiovascular health in this group of patients. The answer to this will complement existing knowledge on factors influencing the development of ED.
Methods
The analyzed group of patients comprised men undergoing cardiac rehabilitation treatment in five different centers. All respondents were diagnosed with IHD. A subgroup of patients who were diagnosed less than 2 months before entering the study (patients with IHD “de novo”) were analyzed separately. The clinical characteristics of the analyzed group are outlined in Table 1.
Characteristics of the Analyzed Group.
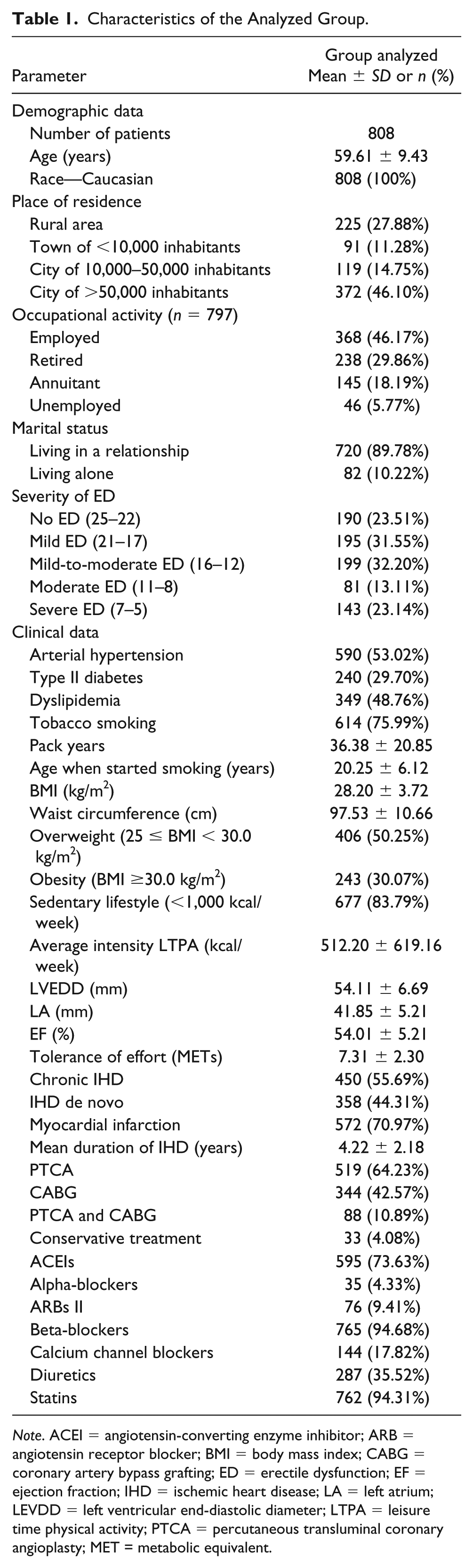
Note. ACEI = angiotensin-converting enzyme inhibitor; ARB = angiotensin receptor blocker; BMI = body mass index; CABG = coronary artery bypass grafting; ED = erectile dysfunction; EF = ejection fraction; IHD = ischemic heart disease; LA = left atrium; LEVDD = left ventricular end-diastolic diameter; LTPA = leisure time physical activity; PTCA = percutaneous transluminal coronary angioplasty; MET = metabolic equivalent.
All patients gave informed consent to participate in the study, conducted with the use of a questionnaire developed by authors. The questions listed in the questionnaire were answered by the patients themselves. Uncertainties could be clarified with an assistant. During completion of the questionnaire, the necessary privacy was ensured, and the patients’ answers were not influenced by a third party. The questions were posed in a closed-ended manner. The obtained data were encoded, ensuring every respondent full protection of his personal data, and analyzed.
Questions on socioeconomic factors such as marital status, education, income, occupational status, nature of work conducted, and demographic data such as age, sex, race, and place of living were included. The survey considered the period of a minimum 10 years before the survey. Due to the negative influence of SES on IHD, the patients were classified into two categories: patients with de novo IHD, in whom the treatment in the cardiac rehabilitation center marked the first manifestation of IHD (duration of 2 months) and patients with chronic IHD (mean duration of 3.55 years). Responses about marital status were subdivided into two categories: (a) in a relationship, (b) single (bachelor, divorced, widower). None of the participants confirmed his homosexual orientation. The question about the level of education had four options: (a) basic education (incomplete basic and basic), (b) vocational qualification, (c) secondary (incomplete secondary, secondary, postsecondary), and (d) higher education (bachelor’s degree, master’s degree, PhD). The income was stated in net value, in the local currency, available per person in the household per month. In order to perform the analysis, the net value was changed to the percentage of the average net income (3,858.51) in the national economy in the year 2017. Income was divided into four groups: (a) ≤25.92% of the average income, (b) >25.92% and ≤51.83% of the average income, (c) >51.83% and ≤77.75% of the average income, and (d) >77.75% of the average income. The question about the nature of work performed included three options: (a) physical, (b) intellectual (over half the time in a seated position), and (c) management.
The presence of ED was evaluated by an abridged international coefficient of erection quality (International Index of Erectile Function 5; IIEF-5), composed of five questions giving the total score between 5 and 25 points. ED was identified if the total number of points were 21 or less (≤21; Rosen, Cappelleri, Smith, Lipsky, & Peña, 1999).
The survey included questions regarding the presence of modifiable risk factors of ED in the patients. The presence of those reported was additionally confirmed through analysis of medical documentation of the participants, which also served as a source of clinical information. The modifiable risk factors for ED assessed included tobacco smoking, arterial hypertension, dyslipidemia, diabetes, abnormal body weight (overweight and obesity), as well as a sedentary lifestyle (low intensity of health-promoting physical activity).
Health-promoting physical activity was defined as planned, aimed, and regular physical activity, which included commuting, either on foot or by bicycle, provided that it lasted longer than 15 min at a time. To assess the level of health-promoting physical activity, participants filled out a worksheet on physical activity based on the Framingham questionnaire. The estimation of intensity of physical activity was based on the Framingham questionnaire (Arsenault et al., 2010). A value of 1000 kcal/week (Drygas, Kostka, Jegier, & Kuński, 2000) was accepted as the cutoff level of minimal physical activity for CVD prevention.
Patients who presented with ED caused by the surgical treatment of prostate hyperplasia or prostate cancer were excluded from the study. None of the analyzed patients underwent reparative procedures in the abdominal, aorta, or iliac arteries. None of the patients had been treated neurologically due to cardiovascular incidents in the central nervous system or orthopedically due to a severe injury of the spine or pelvis. None of the patients was undergoing psychiatric treatment or taking antidepressant medication; none reported memory problems, underwent dialysis, or was treated by an endocrinologist.
The credibility of the data from the IIEF-5 and the Framingham questionnaire was verified by performing comparisons between the total amount of points obtained in the original survey and a follow-up survey conducted a minimum 7 days later in 96 randomly chosen subjects.
The study was performed after obtaining approval from the local bioethics committee (KB–433/2010) as part of a targeted cardiosexual education program provided with the help of presentations, traditional printed materials (brochure, movie, IIEF-5 questionnaire), and websites. Conducted continuously since 2011, the education program has reached 16,447 patients so far.
Data were statistically analyzed. The Student’s t-test for independent variables was used for comparisons between groups of variables with a normal distribution; the Mann–Whitney U test was used for comparisons between two groups of variables with a distribution other than normal. Comparison between observed and expected values was performed with the Pearson chi-square test with the Yates modification for 2 × 2 tables. Relationships between two measurable features were analyzed with Spearman’s rank correlation coefficient; the significance of the relationship was tested with the t statistics. Logistic regression modeling was conducted along with calculation of odds ratios (ORs) with 95% confidence intervals. Data were presented depending on their distribution and type as mean and standard deviation, median (interquartile range), or number (percentage). Differences were considered statistically significant at p < .05 (mainly two-tailed distribution; one-way [the right-tailed distribution] was used for the chi-squared statistics only). Statistical analysis was carried out with Statistica software v. 12 (StatSoft, Tulsa, OK, USA).
Results
In the study group, ED was present in 618 (76.49%) patients. The patients with ED were characterized by a significantly higher age (61.61 ± 8.60 vs. 53.12 ± 9.11, p < .0001), a lower tolerance of physical activity (6.97 ± 2.19 METs vs. 8.31±2.35 METs, p < .0001), a higher diastolic value of the left ventricle (54.71 ± 6.74 mm vs. 52.28 ± 6.20 mm, p < .0001), a lower ejection fraction of the left ventricle (53.32 ± 9.71% vs. 56.11 ± 8.93%, p < .001), more pack years in tobacco smokers (38.04 ± 21.25 vs. 30.95 ± 18.56, p = .0004), and a higher mean number of modifiable risk factors (3.36 ± 1.05 vs. 3.15 ± 1.03, p = .0299). A statistically significant percentage of patients presenting with ED were patients with diabetes (33.50% vs. 17.37%, p < .0001) or those who led a sedentary lifestyle (87.22% vs. 72.63%, p < .0001). The statistically significant probability of developing ED increased due to age by a factor of 1.115705 (95% CI [1.09, 1.14]; p < .0001), presence of diabetes by 2.396 (95% CI [1.59, 3.61]), and sedentary lifestyle by 2.571 (95% CI [1.73, 3.82]). The degree of ED was statistically significantly linked only to age (R = −0.45, p < .0001). The occurrence of ED and its intensity was not linked to the presence of other risk factors: body mass index (BMI) value, waist circumference, previous myocardial infarction, ongoing CVD, and invasive or pharmacological treatments.
Other analyzed factors included the educational status, income, marital status, nature of the work conducted, and the place of residence.
In the analyzed group, 52 men had a basic education (6.44%), 288 (35.69%) a general vocational qualification, 305 (37.79%) secondary education, and 161 (19.95%) higher education. The educational status was statistically significantly related with the occurrence of ED (p = .0047).
A higher education was associated with lower probability of severe ED with OR being 0.7546 (95% CI [0.6221, 0.9153]). The median score on the IIEF-5 questionnaire in patients with a basic education was 17 (Q25 = 5, Q75 = 17), with a vocational qualification 16 (Q25 = 11, Q75 = 21), with secondary education 16 (Q25 = 11, Q75 = 21), and with higher education 17 (Q25 = 11, Q75 = 23). The data indicate a statistically significant correlation between the level of education and the degree of ED (R = .0923, p = .0087). In Figure 1, the scoring on the IIEF-5 questionnaire is shown by level of education. Accounting for patient age and the presence of modifiable risk factors for ED in the analysis did not change the direction of the obtained results, which were still statistically significantly linked to the level of education. Among the analyzed modifiable risk factors, education was significantly linked to the presence of hyperlipidemia (p = .0086), tobacco smoking (p = .0020), and the intensity of health-promoting physical activity (R = 0.0845, p = .0163). The percentage of patients presenting with hyperlipidemia increased within the given categories of education: 20 (38.46%) with basic, 134 (46.37%) with vacational, 146 (47.87%) with secondary, and 94 (58.39%) with higher education. In tobacco smoking, the percentage declined with higher levels of education: 39 (75.00%), 234 (80.97%), 237 (77.70%), and 104 (64.60%) respectively. In patients with a basic education, health-promoting physical activity was the lowest, amounting to 298.01 ± 475.75 kcal per week and different from the remaining education categories (474.77 ± 576.38 kcal – vocational, 573.69 ± 669.69 kcal – secondary, and 535.28 ± 620.08 kcal – higher). For the presence of increased body weight (overweight, obese), arterial hypertension, diabetes, and a sedentary lifestyle, no statistically significant correlation was observed between the presence of those factors and the patient’s level of education. No correlation was found for other analyzed parameters: age, number of pack years in tobacco smokers, age at which they began smoking tobacco, waist circumference, analyzed echocardiological parameters, exercise tolerance, presence of myocardial infarction, duration of CVD, mode of invasive treatment, and pharmacotherapy.

International Index of Erectile Function 5 (IIEF-5) questionnaire scores for levels of education.
In the group of men with coronary artery disease (CAD), the lowest SES was characterized by a per capita household income at ≤25.92% of the average monthly net national income for the year 2017. Overall, 205 (25.40%) patients belonged to this category. An income of between 25.92% and 51.83% of the average net income was observed in 384 patients (47.58%), while 163 respondents (20.20%) fell into the third category, between 51.83% and 77.75% of the average net income. Overall, 55 patients (6.82%) had the highest average net income value or greater than 77.75% of the average net national income per month. The SES analyzed for the whole group of respondents was statistically significantly correlated only with the educational status (R = 0.4638, p < .0001) shown in Table 2 and waist circumference (R = 0.0815, p = .0470).
The Relationship Between the Presence of Erectile Dysfunction and Attained Education Level in Men With Cardiovascular Disease.

Note. ED = erectile dysfunction.
The analysis performed on the group of patients with IHD de novo showed the presence of a statistically significant relationship between SES and the presence of ED (p = .009). Table 3 shows the number and percentage of patients belonging to each economic status category, subdivided into patients who presented with ED and those who didn’t.
Relationship Between the Presence of Erectile Dysfunction and the Average Income of Men With Cardiovascular Disease.

Note. ED = erectile dysfunction. aAverage net income in the national economy in the year 2017. bPearson chi-square test.
In this group of patients, the level of education was also statistically significantly linked to the number of points scored on the IIEF-5 questionnaire (p = .03215). Table 4 presents the number and percentage of patients belonging to the given economic status and their points on the IIEF-5 questionnaire. In patients with IHD de novo and those belonging to the two lowest categories of average net income (≤51.83%), ORs for ED to occur dependent on the economic status were 0.911 (95% CI [0.484, 1.712]) for the categories >51.83% and ≤77.75% of the net income value and 0.259 (95% CI [0.112, 0.597]) for the category >77.75% of net income value.
Relationship Between the Degree of Erectile Dysfunction and the Average Income in Men With Cardiovascular Disease.

Note. ED = erectile dysfunction. aThe percentage of the average net income in the national economy in the year 2017. bPearson chi-square test.
Marital status significantly influenced scores on the IIEF-5 (p = .0095). In married men, the median point score was 16 (Q25 = 11, Q75 = 21); in patients living alone, it was 14 (Q25 = 8, Q75 = 19). Marital status also was statistically significantly linked to waist circumference of the respondents (p = .027). Men who lived alone had an average circumference of 97.81 ± 10.63 cm; in married men, it was 94.66 ± 9.51 cm. Marital status had no statistically significant effect on the remaining analyzed parameters.
Among 368 occupationally active patients, physical work was performed by 184 (52.12%), intellectual work by 125 (35.41%), and work in a management position by 44 (12.46%). The nature of the work performed was not statistically significant in terms of the analyzed parameters.
The size of the patients’ town or city was statistically significant with regard to the number of risk factors the patients reported (R = 0.0943; p = .0073). In rural areas, the mean number of risk factors for ED was 3.18 ± 1.08; in small towns, 3.26 ± 0.94; in average cities, 3.32 ± 1.08; and in inhabitants of big cities, 3.40 ± 1.04. The place of residence had no statistical significance on the remaining analyzed parameters.
Discussion
A high percentage of patients with CVD are burdened with ED; in our cohort as many as 76.49% suffered from ED. This results from the joint pathogenesis of ED and CVD, which manifests as damage to the vascular endothelium and as disruptions in the activity of the autonomic nervous system (Kałka et al., 2016). In clinical trials on the contribution of SES to the pathogenesis of CVD, patient income and educational status are most often evaluated; marital status, nature of occupational work, and other factors accessible for evaluation are less commonly tracked. Our study showed that patients with ED were older, less educated, and less active. In patients with newly diagnosed IHD, SES correlated significantly with the presence of ED.
The present study includes several limitations. As this is a cross-sectional study, only relationships between analyzed variables could be presented without determining their causative effects. It also should be noted that information about income is protected by patients; therefore, patient self-reports may be of limited reliability.
However, evaluation of the SES comprises many individual social aspects beyond income and education. In patients with IHD, they are associated with biological factors connected to the primary disease, which causes this group of patients to be particularly difficult to analyze. In addition to studies evaluating the influence of SES on morbidity and mortality due to clinically present CVD, studies evaluating its relationship with preclinical forms of atherosclerosis have begun to emerge in the literature. In the prospective study Atherosclerosis Risk in Communities (ARIC), a strong link between SES and the occurrence of dysfunctions in microcirculation has been observed. (Fretz et al., 2016) Overall, 15,792 Americans took part in the study and two forms of SES were taken into account (individual defined as income and educational level and myocardial damage defined as elevated cardiac troponin T level). The participants of the study did not present with CVD; the intima–media thickness (IMT) and peripheral arterial disease (PAD) were used as preclinical markers of atherosclerosis. The individual SES correlated significantly with the mean value of IMT, whereas the environmental SES did not influence the IMT to such a significant extent, as SES values from the lowest tercile correlated with higher values of IMT in comparison to SES values from the highest tercile. The analysis also showed that a lower individual SES is linked to a higher OR value for PAD, but the environmental SES did not show a correlation with the occurrence of PAD (Carson et al., 2007). Another study showed a statistically significant interchangeable relationship between SES and preclinical damage to the myocardium evaluated by an elevated value of a highly sensitive isoform of cardiac troponin (hs-cTnT; Fretz et al., 2016).
The negative influence of SES on microcirculation affects not only the pathogenesis of CVD but also other clinical manifestations, such as ED. The analysis of over 100,000 respondents of the 45 and Up Study showed that moderate/complete ED was linked to a lower SES. In patients with less education, the OR was 1.56 (95% CI [1.47, 1.66]) compared to respondents with a higher education; in patients with a yearly income of less than 20,000 USD, OR was 1.85 (95% CI [1.75, 1.95]) compared to those earning over 50,000 USD per year. In addition, an insignificant increase in the risk of ED has been observed in persons who were single in comparison to people in relationships (OR 1.10; 95% CI [1.06, 1.15]; Weber et al., 2013).
Similar results were obtained regarding the income of diabetic patients. Their monthly income served as an independent predictive factor for the occurrence of ED as well as the severity of the disease’s symptoms (OR for the group with the highest income was 0.285 in comparison to the group with the lowest income; Hosain et al., 2013). Martin et al. (2014) confirmed the significant role of SES, showing that not only a low income but also the mode of employment served as a predictive factor for the remission of ED. Cho et al. (2003) indicate that the incidence rate of ED in the Korean population is correlated with a lower level of education, physical work, and a lower income. However, other research shows that a high income as well as being in a relationship put subjects at a substantial risk of having risk factors for sexual dysfunction, but only in patients under the age of 40 years (Lynch, Davey, Harper, & Bainbridge, 2006).
Similar to other analyses, we found a statistically significant (p = .0047) influence on the presence of ED by the level of education in men with CVD. In the least educated subjects, 88.46% had ED; in the most educated, 67.08% did. More education was thus associated with a lower chance of developing ED, with an OR value of 0.7546. The correlation between the level of education and the presence of ED in the group of patients with CVD remained significant after taking into account patient age and the presence of modifiable risk factors for ED. Furthermore, the level of education was also significantly (p = .0086) linked to the intensity of ED, with more educated patients displaying less severe ED.
The mean score on the IIEF-5 questionnaire for the least educated respondents was 12.15 ± 6.65 points; for patients with a higher education, it was 16.42 ± 6.74. The level of education in respondents with CVD was also linked to the presence of modifiable risk factors for the disease. Among the analyzed risk factors, it was significantly linked to the presence of hyperlipidemia (p = .0086), tobacco smoking (p = .0020), and the intensity of health-promoting physical activity (p = .0162). According to Lynch et al. (2006), patients from lower socioeconomic groups are characterized by higher total cholesterol and low-density lipoprotein (LDL) cholesterol values, more tobacco smoking, as well was a lower exercise tolerance and less physical activity. Similar observations were made by Weber et al. (2013) after an analysis performed on a group of 101,674 patients aged 45 years and up, who were not treated due to prostate cancer: Of these, 25.14% presented with mild ED, 18.79% with moderate ED, and 16.77% with severe ED. The risk of moderate-to-severe ED was higher in men with a low SES, with a higher BMI, currently smoking tobacco, leading a sedentary lifestyle, and suffering from diseases such as diabetes and CVD, compared to men without those dysfunctions.
Household income per capita and average household income are two more integral socioeconomic factors, which influence sexual dysfunction and have been the subject of many studies. In a study performed on 4,755 veterans of the war in Iraq and Afghanistan with a mean age of 29 years (age range 19–64), sexual dysfunction was present in 5.5% (N = 265). In younger patients (aged 18–40), this was statistically significantly (p < .05) influenced by yearly income, marital status, post-traumatic stress syndrome, and arterial hypertension (Hosain et al., 2013). Lower income, as well as advanced age, higher values of abdominal fatty tissue, low alcohol intake, higher risk of the presence of sleep apnea, and the presence of depression and diabetes served as predictive factors for ED incidence in a group of 810 randomly chosen men between the ages of 35 and 80 years, followed up for 5 years, who were patients in clinics based in Northern and Western parts of Adelaide, Australia. In this analysis, a lower age and current employment status were predictive factors of ED remission (Martin et al., 2014). Likewise, a cross-sectional hospital study with 249 men at a mean age of 43.39 years with diabetes lasting on average 6.22 years, who were treated in five hospitals in Ethiopia, showed that income (OR = 0.285, 95% CI [0.132, 0.615]) was an independent prognostic factor for ED, as were age and the duration of diabetes. ED was present in 69.9% of the analyzed population (Seid, Gerensea, Tarko, Zenebe, & Mezemir, 2017).
In the analyzed group of patients with CAD, most (72.98%) belonged to the two lowest categories of income, or just over 50% of the average net income in the national economy for the year 2017. Only 20.20% of respondents belonged to the highest category. The economic status for the group of patients with CVD as a whole was not substantially linked to the presence of ED or its intensity. For patients who were undergoing cardiac rehabilitation due to the first clinical manifestations of IHD (de novo IHD), the analysis showed that SES is statistically significantly linked to the presence of ED (p = .009) as well as its intensity (p = .0322). This may result from the fact that the development of the primary disease in patients with chronic IHD led to the worsening of their SES. The need to purchase medication and the limitations put on health could have had a negative influence on their ability to perform occupational work, which could have negatively influenced the SES of men in this group. This is not observed in the group of patients with de novo IHD, who had not experienced severe limits in their income since the diagnosis. Difficulties in evaluating SES can also be linked to the fact that the analyzed data has been obtained directly from the respondents via questionnaires. Therefore, it cannot be ruled out that some of the respondents overstated or understated their income, which could have influenced the obtained results.
In the literature, empirically obtained proof has been found to support the hypothesis that a lower economic status is linked to a higher probability of many risk factors negatively influencing sexual health. At the moment, no consensus exists on the contribution of SES to the development of ED, as proofs are limited to other risk factors that also lead to deterioration of sexual health (Tang, Rashid, Godley, & Ghali, 2016). One would expect that the accumulation of risk factors could be linked to patients’ socioeconomic factors, insofar as a lower status could indicate a lack of awareness of their negative influence on sexual functioning and the resulting lack of need to address them. However, Kałka et al. (2018) showed in a group of 417 men at a mean age of 61.10 ± 9 years with CVD and ED that both a higher education (p < .0001) and a higher economic status (p < .0004) were significantly correlated with a higher number of known risk factors for ED.
A high percentage of the evaluated group of patients with CVD presented with the presence of modifiable risk factors for ED. Four of six analyzed risk factors for ED were present in over 50% of patients belonging to the analyzed group and the presence of ED was statistically significantly correlated (p < .0299) with a higher mean number of analyzed modifiable risk factors; two modifiable risk factors were not significantly linked to SES. Therefore, in this case, it is difficult to identify any direct links between socioeconomic factors and modifiable risk factors whose presence would be connected to the presence of ED. It should be kept in mind that the patients analyzed in this group had atherosclerosis, and a substantial number of them did not present with any significant past coronary incidents. In such patients, the presence of ED is caused by restrictions that result from the underlying disease, such as a substantially limited exercise tolerance, a lowered left ventricular ejection fraction, pharmacotherapy for IHD, or hormonal changes (Kałka, Karpiński, et al., 2017; Kałka et al., 2018).
Besides the issue of socioeconomic factors’ influence on the occurrence and degree of ED in this group of patients, the most crucial point from a practical perspective seems to be the relationship between socioeconomic factors in patients with IHD with their knowledge about the possibility of performing sexual activity and treatment options for ED (Akkus et al., 2002; Kałka, Gebala, Borecki, Pilecki, & Rusiecki, 2017). Kałka, Gebala, et al. (2017) performed an analysis on 1,007 patients after a myocardial infarction with a mean age of 60.18 ± 9.13 years, establishing that the level of education statistically significantly determined (p < .001) the knowledge about the return to sexual activity and the possibility of treating ED. In another study, Kałka, Karpiński, et al. (2017) emphasized that the level of education in patients with IHD also significantly determines (p < .0001) the patient’s expectation of the treating cardiologist to address the topic of sexual activity during the consultation (p < .0001). This is significantly connected (p = .0031) to the frequency of addressing this topic during cardiological consultation.
In all of the cited studies, a higher SES had a positive influence on the patients’ sexual health in men in general and in patients with cardiovascular disease. This supports the implementation of early preventive social and environmental measures, which can have an influence on SES and thus have a positive impact on the sexual health of men.
Conclusions
A low economic status was statistically significantly linked to the presence and degree of ED only in patients with CVD that occurred de novo. Additionally, the level of education in patients suffering from CVD has a significant relationship with both the occurrence and degree of ED. This indicates that patients with newly diagnosed CVD may become less employable despite the necessity of expenses on treatment and require more attention and education after being informed about the diagnosis of CVD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.