
Abstract
Human papillomavirus (HPV) can cause various diseases; low-risk strains can cause genital warts, whereas high-risk strains can cause cervical cancer and cancer of the vulva in women and cancers of the penis, anus, and oropharynx in men. Although HPV affects men, literature has reported that the prevalence of HPV vaccination is far lower among men than among women. Few studies have examined perceptions and acceptability of the HPV vaccine among men, particularly in Chinese communities. In this study, the acceptability of the HPV vaccine to men was investigated using Hong Kong men as a case group. A qualitative research approach was adopted. Thirty-nine men were purposively sampled for the in-depth individual semistructured interviews from June to October 2017 to investigate their perceptions of the HPV vaccine and the barriers for them to receive the vaccination. Limited knowledge and awareness of HPV-related issues, low perceived risk of HPV infection, perceived association between HPV vaccine and promiscuity, and lack of accessible official information on HPV-related topics were identified as the key barriers. These barriers intermingled with the sociocultural environment, cultural values of sexuality, and patriarchal gender values. HPV vaccine is shown to be socially constructed as a vaccine for women exclusively and for promiscuity. The participants were discouraged from receiving HPV vaccination because of its signaling of socially deviant promiscuity. Cultural taboo on sex served as a social oppression of open discussion about HPV vaccine and affected the participants’ perceived need of vaccination. Perceived insignificance of reproductive organs also influenced the participants’ perceived need of vaccination.
Human papillomavirus (HPV) infection is the most common sexually transmitted infection worldwide (Centers for Disease Control and Prevention, 2017a). HPV infection is not exclusively harmful to women, but it can also lead to negative health conditions among men. The most widely known consequence of HPV infection is cervical cancer, which is mostly caused by high-risk strains of HPV such as HPV-16 and 18 (Lowy & Schiller, 2012; Waheed, Gottschamel, Hassan, & Lössl, 2012). Oncogenic HPV genotypes are also responsible for more than 80% of anal cancers and approximately 50% of penile cancers (Crow, 2012). Anal cancer accounts for approximately 4% of all lower gastrointestinal cancers in the United States, and its incidence is rising steadily in men with 900 new cases every year (Partridge & Koutsky, 2006). HPV is also associated with approximately 25% of head and neck cancers in men (Moscicki & Palefsky, 2011). Among Whites and Blacks in the United States, 5.1 and 6.8 men per 100,000, respectively, suffered from HPV-associated head and neck cancers between 1998 and 2003 (Moscicki & Palefsky, 2011). Men who have a weak immune system or who have anal sex will have a higher risk of developing HPV-related cancers (Centers for Disease Control and Prevention, 2017b). Aside from cancers of the penis, vulva, anus (Giuliano et al., 2011; Moscicki et al., 2012), and oropharynx (Gillison et al., 2012), cutaneous and low-risk HPV types can cause benign skin warts (Pfister & Ter Schegget, 1997) and keratoacanthomas (Asgari et al., 2008). In the United States, at least 340,000 women and men are affected by genital warts every year, and about 1 in 100 sexually active adults have genital warts (Centers for Disease Control and Prevention, 2017a).
HPV infection is also prevalent in China (Ma et al., 2018). The national HPV prevalence was 15.6% in women with normal cervical cytology, and 14.5% among heterosexual men (Ma et al., 2018). A significantly high HPV prevalence of 59.9% was reported among men who have sex with men (MSM; Ma et al., 2018). The incidence of anal cancer and HPV-associated head and neck cancer in China is not well documented; however, a study does report that the incidence of anogenital warts in South China is as high as that in developed countries (Wei et al., 2017). In Hong Kong, the incidence of penile cancer has been on a steady increase, with 22 new cases in 1983 to 50 new cases in 2016, affecting a total of 1,012 men from 1983 to 2016 (Hong Kong Cancer Registry, 2018). The incidence of genital warts for males was estimated to be 292.2 per 100,000 persons per year, and men are reported with higher prevalence of anogenital warts than women (Cheung et al., 2018). These statistics illustrate that HPV infection is a disease burden for men in Chinese communities.
HPV vaccination is recommended by the World Health Organization (WHO) (2017) as an effective preventive measure. Although HPV can cause health problems for men, the prevalence of vaccination coverage is lower among men than among women. One study (Thompson et al., 2016) of trends in HPV vaccination uptake among college students in the United States reported that the vaccination prevalence among young men was far lower than that among young women from 2009 to 2013. Although the overall uptake among college students increased during the study period, coverage was approximately 26% lower among male college students than among their female counterparts. In 2016, HPV vaccine coverage in the United States reached approximately 49.5% among women but only 37.5% among men (Walker et al., 2017). In Hong Kong, HPV vaccines Gardasil® and Cervarix® have been available since 2006. Series of vaccine advertising campaigns, which were mostly directed by the pharmaceutical companies, were also started in the same year. The figures of HPV vaccination uptake are not well documented, but past studies report that only 768 women were vaccinated in 2008 (The Family Planning Association of Hong Kong), and only 9% of school-aged girls (Choi et al., 2013) and 9.7% of university female students at one university (Chen & Leung, 2016) were vaccinated in 2010s. Referenced from these figures, a lower HPV vaccination rate among men in Hong Kong is expected (Choi et al., 2018).
Significance
Studies on HPV vaccination have examined factors influencing its promotion (Fisher, 2012; Valentino & Poronsky, 2016) and barriers to receiving HPV vaccination such as misconceptions, low perceived risk of infection, and high cost (Hamlish, Clarke, & Alexander, 2012; Liddon, Leichliter, & Markowitz, 2012; Pourat & Jones, 2012). Most of these studies have focused on women’s perceptions, with a paucity of men’s perceptions. Relevant studies in Hong Kong are even scarcer beyond a few studies on women’s perceptions of HPV vaccination (Chen & Leung, 2016; Choi et al., 2013; Lee et al., 2007; Li et al., 2013; Siu, 2013, 2014). Studies on the acceptability of the HPV vaccine to men are limited, and these quantitative studies (Cheung et al., 2018; Tian et al., 2018) have only focused on male college students (Cheung et al., 2018; Ratanasiripong, 2015; Tatar, Perez, Naz, Shapiro, & Rosberger, 2017); thus, qualitative studies and research on men of other age groups are scant. There is a lack of in-depth investigation of men’s perceptions and acceptance of HPV vaccines. This study investigated the perceptions and acceptability of HPV vaccine among men in Chinese communities by using Hong Kong as a case study and demonstrated how the underlying social and cultural values of a community can remarkably affect the acceptability of HPV vaccine among men.
Methods
Data Collection
A qualitative approach with in-depth individual semistructured interviews was conducted with 39 men from June to October 2017 in Hong Kong. Data saturation, which is defined as the point at which no new themes emerge from the data (Liamputtong & Ezzy, 2005), was achieved when 36 interviews were conducted. Purposive sampling was used to select participants with the following sampling criteria: (a) age of 18–65 years at the time of study, (b) birth and education in Hong Kong, (c) Hong Kong as the usual place of residence, and (d) no history of HPV vaccination receipt. Although HPV vaccination is recommended for men through age 21, and through age 26 for men who are homosexual, bisexual, or have immunocompromising conditions in the United States (Centers for Disease Control and Prevention, 2018), the sampling of this study included men through age 65. There is no strict age limit for men in receiving HPV vaccination in Hong Kong, as the 4-valent and 9-valent vaccines are suggested for males aged 9 years or above (Cervical Screening Programme, 2018). Furthermore, HPV prevalence is reported to be high for men up to 65 years of age in Chinese communities, with ages 25 to 50 years having a particularly high incidence and longer duration of HPV infection (Liu et al., 2014). Men aged 45 or above are documented as having a higher incidence of penile cancer than the 20–44 age group (Hong Kong Cancer Registry, 2018), and men who have engaged in risky sexual behaviors are more susceptible to HPV infection as documented up to 60 years of age (Apple Daily, 2006). Therefore, this study sampled men up to 65 years of age to suit the Chinese context. Sampling those who were born and educated and still reside in Hong Kong ensured that the participants had long years of social exposure and socialization in Hong Kong. By sampling the participants who had never received HPV vaccination, the perceptions of and barriers for men to get vaccinated can be revealed. HPV infection status was not considered as a sampling criterion because such testing for infection was not common among men in Hong Kong at the time of the study. None of the participants had ever received HPV screening and reported being diagnosed as having HPV infection and other sexually transmitted diseases.
Recruitment of participants was conducted in two stages. First, participants were recruited through public advertising on the campus of a university in Hong Kong. Recruitment posters with the sampling criteria were posted in various public facilities around campus. Twenty-eight participants were recruited. To ensure a wide socioeconomic mix of participants, a second stage of participant recruitment was conducted that targeted men in the local community. Recruitment posters were posted in primary care clinics. Eleven participants were recruited in the second stage. Participants were confirmed by the research team to ensure that they fulfilled the sampling criteria. Participant recruitment was complete when data saturation had been achieved.
Open-ended interviews were conducted to offer participants flexibility in expressing their experiences and perceptions. Prior to the interviews, an interview question guide (see online supplementary Appendix 1) was prepared based on the literature on male college students’ perceptions (Ratanasiripong, 2015; Tatar et al., 2017) and females’ perceptions on the HPV vaccine (Chen & Leung, 2016; Choi et al., 2013; Lee et al., 2007; Li et al., 2013; Siu, 2013, 2014). The purpose of the interview question guide was to focus the interviews on specified research questions while maintaining a flexible interview structure for the participants. The interview question guide covered participants’ perceptions of HPV, HPV-related diseases, and the HPV vaccine as well as the prevalence of discussion on these issues in the participants’ social networks and their incentives of and barriers to receiving HPV vaccination. As this study solely investigated perceptions of HPV vaccination, participants were not provided any information about HPV and HPV vaccines before the interviews to avoid potential skewing of data.
To ensure interview consistency, all interviews were conducted by the third author, who is male and experienced in qualitative research. In view of the sensitivity of the topic, the same gender of the interviewer as the participants could reduce the interviewer effect of sensitivity and reactivity of the participants (Lipps & Lutz, 2016). The interviewer received intensive training with respect to interviewing and probing techniques from the first author. All the interview audio files—with informed consent from the participants—were evaluated by the first author to ensure quality. All interviews were conducted in the participants’ mother tongue, namely Cantonese Chinese, to facilitate uninhibited discussion. Interviews lasted from 45 minutes to 1 hour each. No participants dropped out of this study. As compensation for the time contributed, each participant received a HK$200 supermarket cash coupon upon interview completion.
Ethical Considerations
Ethical approval for this study was obtained from the Committee on the Use of Human and Animal Subjects in Teaching and Research of Hong Kong Baptist University (approval number HASC/15-16/0047). Prior to the interviews, each participant was given a study information sheet and consent form written in Chinese to ensure their understanding. Written consent was obtained from all participants. The interviews were audio recorded with the consent of the participants.
Data Analysis
The interviews were transcribed verbatim, and the participants were asked to review the interview transcripts for accuracy in the member checking procedure to ensure that the transcribed data had not been distorted. The transcripts were then translated from Chinese to English, and backtranslation was conducted to ensure the transcribed interviews were not distorted. The interview transcripts were analyzed line by line through an inductive coding process that enabled identification of the participants’ thinking and behavioral patterns (Liamputtong & Ezzy, 2005). This analysis offered a preliminary understanding of the participants’ thought patterns. A memo was drafted about each interview to identify critical data points. After data cleaning, the raw interview texts were read thoroughly for content familiarization and then reread to determine possible themes (Thomas, 2006). Distinct concepts were developed and used in memo documentation to enable systematic analysis of the interviews. The interview transcripts were segmented into meaning units (Thomas, 2006), which were labeled and then collapsed into categories (Thomas, 2006). Upper-level categories were identified based on the research questions, and in vivo coding was conducted (Thomas, 2006). Recurrent categories were highlighted. Overlapping codes and categories were consolidated to form broader themes after repeated examination and comparison (Thomas, 2006). The codes, categories, and themes derived from the data, alongside supporting interview quotes, were documented in a coding table (Green & Thorogood, 2004), where designated concepts and categories were highlighted to translate the interviews into meaningful symbols to enable understanding of the participants’ thoughts. The first and third authors coded the transcribed interviews separately but met regularly (once every 2 weeks) to discuss the coded data. Consensus in the coded data was achieved. NVivo 11 was used to help organize the data and coding.
Results
Participants
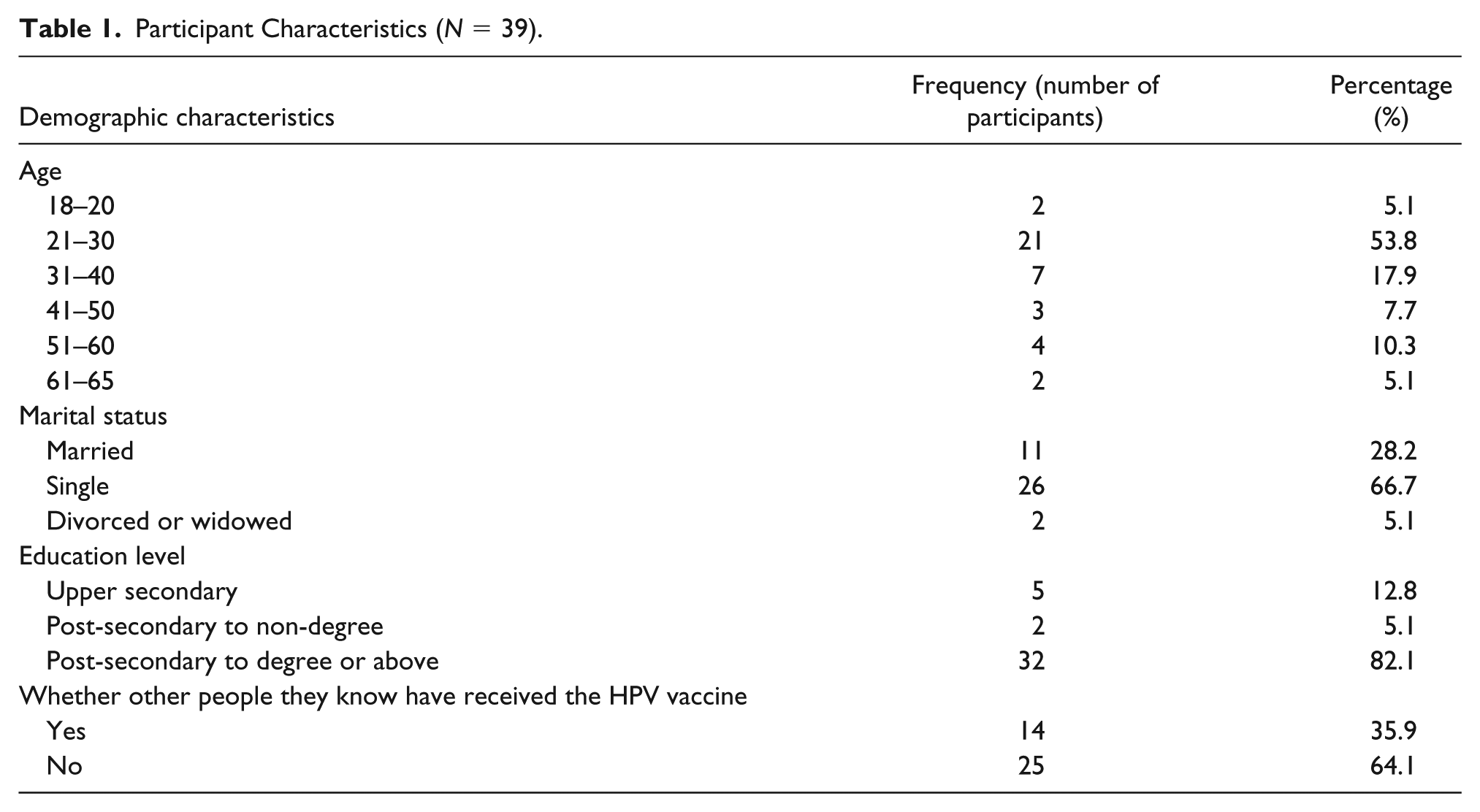
Table 1 presents the participant characteristics. Approximately 59% of the participants were within the age range of 18 to 30 years. Eighty-seven percent of the participants either had received or were receiving postsecondary education at the time of study. Although no participants had ever received HPV vaccination, 14 of them reported that some individuals in their social network—all of whom were women—had received HPV vaccination.
Participant Characteristics (N = 39).
Participants’ Barriers to Getting Vaccinated Against HPV
Limited knowledge and low awareness of HPV-related issues, low perceived risk of HPV infection, perceived association between HPV vaccine and promiscuity, and lack of accessible official information on HPV-related topics were identified as the key barriers that had prevented the participants from receiving HPV vaccination.
Limited knowledge and low awareness of HPV-related issues
All participants demonstrated limited knowledge about HPV-related issues. HPV- and HPV-vaccine-related health illiteracy was apparent in the participants’ answers to the question, “Have you ever heard of HPV?” with “no” as the most popular response. However, participants’ responses of “no” did not necessarily indicate a total unawareness of HPV. As the conversation progressed, they were able to refer to some impression they had received from advertisements about HPV vaccination. In particular, most participants mentioned the advertisements featuring woman celebrities:
Have you ever heard of HPV?
No.
What about the HPV vaccine?
I haven’t heard of HPV, let alone the HPV vaccine.
Could you think again more precisely? You haven’t heard the term “HPV” even once?
Hmm… I remember an advertisement acted by Ah Sa [a woman celebrity]. Is she a spokesperson for the vaccine?
Yes, she is one of them.
Then, yes, I have heard of it. If my memory is correct, G.E.M [a woman celebrity] and Gigi [a woman celebrity] are spokespeople too. I’ve heard about it but I don’t know much about HPV and the vaccine.
The advertisement about the HPV vaccine involving woman celebrities mentioned in this passage was the most typical main information source of HPV among the participants. It gave the participants a brief impression of HPV and the HPV vaccine:
When I was studying at the university, I had seen the [vaccine] poster on campus, such as in the hostel, lobby, or near the main entrance of the teaching buildings. However, I do not know much about it, maybe it is for cervical cancer from the name. After all, I did not take a detailed look at that time.
The advertisement was broadcasted on public transports. I have seen the [vaccine] posters on buses and on MTR [Mass Transit Railway], featuring woman celebrities. However, I just paid attention to the look of the celebrities, but not the details of the posters. I just know it is a vaccine for cervical cancer from the name, and that’s all I know.
The participants, therefore, cannot be described as having acted in total unawareness of the vaccine because they were able to reference the HPV vaccination advertisement and its message about protection against cervical cancer, because the HPV vaccine was referred to as a “cervical cancer vaccine” in the advertisements. The woman celebrities’ promotion in these advertisements also reinforced the beliefs held among the participants that vaccination was a concern for women but not for men.
An association between HPV and AIDS was identified; approximately half of the participants demonstrated confusion between HPV and human immunodeficiency virus (HIV)—the virus that causes AIDS:
HPV is the main cause of AIDS… But I think it can be cured nowadays.
HPV can cause some problems with the immune system such as AIDS. It is transmitted through unsafe sex, especially anal sex.
Limited knowledge of the efficacy of HPV vaccination was prevalent among the participants; those who confused HPV with HIV assumed that the HPV vaccine could prevent AIDS. Additionally, most of the participants believed that the HPV vaccine was available only for women, which was an idea contributed by the Chinese labeling of the HPV vaccine as a “cervical cancer vaccine.” Only a few participants recognized that HPV can also lead to diseases that can affect men such as genital warts. However, even though these few participants were aware that HPV can lead to diseases that affect men, they did not necessarily realize that both men and women can receive HPV vaccination, because they were also misled by the Chinese name of the vaccine and believed that the vaccine was only for women:
I think the vaccine is not our [men’s] business, because it is called a “cervical cancer vaccine” and so of course it is not for me. I do not have a uterus anyway.
I know HPV can lead to “cauliflower” [a nickname of genital warts in Cantonese Chinese] and can affect me. However, the vaccine seems not for me, because it is called a “cervical cancer vaccine.” The vaccine only targets women. I’d feel odd if I asked for that.
A few participants noted that both men and women are eligible for HPV vaccination; however, their understanding of the efficacy of the vaccine appeared incomplete. Some participants believed that the HPV vaccine could eradicate HPV from men’s bodies:
Perhaps I have some types of HPV that do not cause any health problems [for me]. However, if I have passed these viruses to my partner, she may be affected and get cervical cancer. Getting vaccinated can remove HPV from my body, so I will not pass it to her.
The participants had limited knowledge about HPV and HPV-related issues. Although all the participants were aware of the advertisements about HPV vaccination, the advertisements failed to provide concrete information. The woman celebrities in the advertisements and the Chinese name of the HPV vaccine reinforced the beliefs among participants that HPV vaccination is exclusively a preventive measure for women.
Low perceived risk of HPV infection
The participants’ limited knowledge and low awareness of HPV and the HPV vaccine intertwined with their low perceived risk of HPV infection, which in turn led to their low perceived need to receive the vaccination. Based on the perceived correlation between HPV vaccine and cervical cancer, all the participants believed that HPV and HPV vaccination were irrelevant to men, and thus to them. As a result of this perception, the participants exhibited no interest or motivation to learn about HPV and the HPV vaccine:
I do not think I have to get the jab. Basically, I cannot get cervical cancer and therefore I do not need this [vaccine]. Even if I have the virus, it will not affect me. Therefore, why do I need to know about this vaccine? It is none of my business.
Although a few participants were aware that HPV can lead to genital warts and can affect men, all of them expressed low perceived risk of contracting genital warts:
I will not get vaccinated since my chance of getting “cauliflower” [a nickname of genital warts in Cantonese Chinese] is low… People with many sex partners are at higher risk… I am not this kind of person.
“Cauliflower” [a nickname of genital warts in Cantonese Chinese] is a sexually [transmitted] disease. I do not think I am sexually active enough to get it. I am very well behaved. I just have one girlfriend in each relationship, and only have the most traditional sex… I never do anal…
Perceiving genital warts as a sexually transmitted disease, the participants believed they were at low risk because they were not sexually promiscuous, which was perceived as the predominant cause of genital warts. The participants perceived themselves as pursuing a “well-behaved sexual life,” which, in their definition, referred to sex with a single partner in each relationship. They were not motivated to receive HPV vaccination because of the low perceived risk.
Another interpretation of risk among the participants was the possibility of damage to their health. The participants’ perception of this type of risk was low because they believed the consequence of genital wart infection to be mild:
Even if I get “cauliflower” [a nickname of genital warts in Cantonese Chinese], it will not kill me. They will just make my stuff [genital area] look ugly. If it will not kill [me], I will not bother to care.
These few participants perceived genital warts as nonfatal and as presenting negligible consequences in the unlikely occurrence of infection. Their perceptions of the low risk of contracting or being harmed by genital warts led them to perceive HPV as nonthreatening. These perceptions further contributed to their low perceived need for vaccination.
The participants’ price assessment of the HPV vaccine also reflected their low perceived need to receive the vaccination. Regardless of their personal financial situation, participants evaluated the financial value of vaccination based on their perceptions of the vaccine’s protective value in relation to their health:
No matter how much the vaccine is, it is expensive for me because I will never get the diseases that are caused by this virus. Even it only costs one dollar [equivalent to US$0.13], it is expensive, because I will never get those diseases.
If the vaccine is effective in protecting my health, then it is cheap even if it costs 5,000 dollars [equivalent to US$641]. However, I do not need the vaccine, so it is expensive even it just costs 50 dollars [equivalent to US$6.41].
These participants judged vaccination based on not its actual financial cost but rather its perceived usefulness and protective value for their health; this correlated with their understanding of HPV-related issues. The vaccine was perceived as expensive if considered unnecessary.
Perceived association between HPV vaccination and promiscuity
Perceptions of HPV and HPV-related diseases as associated with promiscuous sexual behavior also prevented more than half (74.4%) of the participants from receiving HPV vaccination. The following excerpt represents the most typical perception among these participants:
Who will need the vaccine?
Promiscuous people and perhaps sex workers, too. They have many sex partners, and their frequent sexual activity makes them more susceptible to sexually [transmitted] diseases, and the vaccine can give them more protection.
Do you think that getting the vaccination indicates one is promiscuous then?
Hmm… That is a difficult question, but I will say…hmm…no. It’s more like having the vaccine provides more protection and allows people to become promiscuous.
This sounds interesting. Then is this a reason for you not to get vaccinated?
Probably yes. Perhaps ladies will think I am promiscuous if I get the vaccine, and then I will not be able to get a girlfriend.
The stereotype that the purpose of HPV vaccine is to prevent sexually transmitted diseases and that only promiscuous individuals and sex workers require the vaccination remarkably prevented the participants from receiving the vaccination. To the participants, receiving vaccination could imply to others that they were promiscuous. This concern discouraged the participants from receiving vaccination.
Lack of accessible official information on HPV-related topics
The difficulty in obtaining official information about HPV-related issues and the HPV vaccine was a remarkable barrier for the participants—one that prevented them from being aware of the needs for getting the vaccination. As mentioned, the vaccine advertisements with women celebrities were the main source from which the participants had obtained any understanding of HPV-related issues and the HPV vaccine. The advertisements provided limited information such as the name of the vaccine and its function in preventing cervical cancer. Apart from these brief advertisements, the participants had little exposure to HPV-related information.
Conversations about HPV-related issues were rare in the social networks of all the participants. The participants had never discussed HPV and HPV vaccination with their health-care providers, because they perceived the vaccine as irrelevant to them. They had never discussed these issues with their family members or male peers as well, because they perceived talking about the vaccine—which was perceived as sex-related—as inappropriate, though they had some brief communications about the HPV vaccine with their female peers. These discussions were usually so brief that they had failed to provide substantive information to the participants:
Have you ever talked about HPV or the HPV vaccine with anyone?
No.
Have you ever talked about it with your family members?
No. I think it is not good to talk about this with others, because they may feel uncomfortable if these sex matters are chatted openly.
Then how about doctors or nurses? Have you ever asked them about the vaccine?
No. I did not think about asking them, because the vaccine is not for men, so there is no point for me to ask them about the vaccine. But some female friends did talk about the vaccine with me.
What were these discussions about?
Sort of sharing only. For example, one of my female friends got the jab, and shared [a photo] with us through Snapchat. She also mentioned it when we were having lunch together.
Did you learn more about the vaccine or other issues from this chat?
Basically no. Just a small chat only. I just learnt that she got the shot.
Another popular information source about HPV and HPV vaccination for participants was the Internet, though it may transmit distorted health information. Approximately half of the participants referred to information about HPV-related issues that they had encountered online:
You know the vaccine can protect against cervical cancer. Apart from that, do you know anything else about HPV, the vaccine, cervical cancer, or diseases related to HPV?
I know removing the uterus is the best way to prevent cervical cancer.
Removing the uterus?
Yes.
How did you learn that?
From an online forum.
Was the forum particularly for sharing medical information?
No, just some posts on a local forum.
Did any netizens who shared that information claim themselves as health-care providers?
So far, I haven’t met any health-care providers on the Internet.
Then, do you trust this information that you came across on that forum?
So-so. Some [topics] are medical discussions. Some are netizens’ personal experiences. Some are news sharing. I think most of them are real as they have links to the information attached. Also, I think removing the uterus sounds reasonable to prevent cervical cancer. After all, it does not matter if you do not have a uterus, because it is optional; you won’t die even if you do not have a uterus. Similarly, even if you get cervical cancer, you can still survive because you can simply remove the uterus and then recover. It is a minor organ only. It [cervical cancer] does not act like other cancers such as lung cancer or liver cancer, because they are major organs and so you can really die of them.
Participants, therefore, experienced remarkable difficulty in accessing official information about HPV and the HPV vaccine. The Internet and female friends were their only sources of information. Rarely did participants mention health institutions as a source of information. The participants did not think about asking health-care providers, as they perceived the HPV vaccine as irrelevant to their health.
Discussion
Limited knowledge and low awareness of HPV-related issues, low perceived risk of HPV infection, perceived association between HPV vaccination and promiscuity, and lack of accessible official information on HPV-related topics were the major interacting barriers that prevented the participants from receiving HPV vaccination. These barriers intermingled with the sociocultural environment, cultural values of sexuality, and patriarchal gender values, reinforced by the women-targeted approach of vaccine promotion. Most participants believed HPV vaccination was a “women’s concern” of no consequence to men, which is consistent with overseas literature (Tatar et al., 2017). Patriarchal gender values and cultural values with respect to sexuality had also discouraged participants from receiving HPV vaccination.
Social Construction of HPV Vaccination as a Women’s Concern of No Consequence to Men
Studies have reported that in Asian countries, men’s limited knowledge about HPV and HPV-related issues is the result of a combination of low vaccine coverage in Asia and women-oriented vaccine promotion (Daley et al., 2017). The data collected in this study verified this phenomenon. Participants’ limited knowledge about the HPV vaccine shows consistency with that of young men from the United States (Ratanasiripong, 2015) and Canada (Tatar et al., 2017). All participants demonstrated limited knowledge and awareness of the HPV vaccine generated by particular advertisements with a woman-focused approach. Stereotyping of the HPV vaccine as a women’s vaccine was constructed by the use of woman celebrities in the vaccine advertisements, which comprised the entirety of the participants’ “knowledge” about the HPV vaccine. The gender-biased approach in vaccine promotion has, in turn, resulted in the participants’ perception of HPV vaccination as a women’s concern of no consequence to men.
The Chinese term for the HPV vaccine, “cervical cancer vaccine,” further reinforced the cultural construction of HPV vaccination as a concern exclusively for women. This name has contributed to the participants’ distorted perceptions of HPV vaccination as irrelevant to men. Although the Chinese term for the vaccine may have enhanced women’s awareness of its role in the prevention of cervical cancer, this name obscures the vaccine’s efficacy in preventing genital warts and cancers of the penis, anus, and oropharynx, which can affect men. The Chinese term for the vaccine has generated a sense of apathy among the participants toward HPV-related issues and the HPV vaccine, thereby decreasing their awareness and thus discouraging them from receiving vaccination.
In semiotics, language refers not merely to communication through speech and writing but rather to a system of interrelated, meaningful signs. Ferdinand de Saussure (1983) developed the formulation of “signifier” and “signified” to describe the construction of linguistic signs. Barthes (1973) suggested that connotation and denotation comprise linguistic sign construction. The structure of language and its relationship to meaning-forming processes is interlocked. According to the Sapir–Whorf hypothesis (Spradley & McCurdy, 1996), human experience is mediated through culture and language. Analysis of people’s lexicon can explain various factors in their physical and social environments. Language and vocabulary influence people’s perceptions, and thus affect their attitudes, behaviors, and worldviews. An individual’s “real world” is unconsciously constructed based on the language habits of one’s social group(s). In other words, language creates people’s perceptions of reality and shapes their worldview (Spradley & McCurdy, 1996).
The formation of the Chinese term for “HPV vaccine,” we argue, is based on the patriarchal value system of Hong Kong. Gender values are crucial in the social construction of illness (Lorber & Moore, 2002). The term “cervical cancer vaccine” excludes references to other potential HPV-associated diseases and places the burden of disease on women rather than on men. The emphasis on cervical cancer in the Chinese term for the vaccine reflects gender values embedded in patriarchal Chinese communities, contributing to the social construction of female body as a “diseased body” (Lorber & Moore, 2002; Rieker & Bird, 2005) that requires biomedical monitoring, intervention, and treatment. Therefore, referring to the HPV vaccine as a “cervical cancer vaccine” conforms to a patriarchal value system, and the embedded gender values encompass a patriarchal conception of health. The term “cervical cancer vaccine” not only downplays other diseases potentially caused by HPV but also implies that women are an at-risk group that must be protected from HPV and that men, by contrast, are absent to the risk of HPV in the discourse, though genital warts—which can affect men—are indeed the commonest consequence of HPV infection (Centers for Disease Control and Prevention, 2017a). Even the government health authorities have also referred to the HPV vaccine as a “cervical cancer vaccine” in their promotion of the Community Care Fund Free Cervical Cancer Vaccination Pilot Scheme since October 2016, which subsidizes HPV vaccination only for teenage girls (Community Care Fund Free Cervical Cancer Vaccination Pilot Scheme). Such naming may have influenced the government’s upcoming HPV vaccination policy, as only school girls are the focus as indicated in The Chief Executive’s 2018 Policy Address (The Chief Executive’s 2018 Policy Address, 2018). As Baer, Singer, and Susser argued (1997), health institution policies can remarkably influence the health perceptions and related health behaviors of people. Therefore, the distorted perceptions of the participants may be further enhanced by the government’s use of this Chinese term and policies. This health promotion is not value free but rather follows the patriarchal belief system of Hong Kong, as women are the traditional focus of discourse about the HPV vaccine. Consequently, men, including the participants of this study, perceived HPV vaccination as irrelevant to them, and are discouraged from receiving this preventive health measure as a result.
This patriarchal value system, thus, has resulted in the health inequality between men and women in preventive health against HPV, ending up in undermining men’s health, in which men are reported with higher prevalence of anogenital warts than women (Cheung et al., 2018). Men are disadvantaged in obtaining protection against HPV. Men’s limited accessibility to HPV vaccination can thus lead to their increased vulnerability and disease burden related to HPV—especially with respect to genital warts, which are indeed the commonest outcome of HPV infection (Centers for Disease Control and Prevention, 2017a).
Social Construction of the HPV Vaccine as a Sex-Related Taboo
Most participants perceived HPV infection and associated diseases as diseases transmitted through promiscuous sex. The participants commonly perceived HPV and HIV to be the same virus, believing that promiscuous sexual behavior was the only means of HPV transmission. This confusion was demonstrated in their emphasis on the HPV’s causation of not only cervical cancer but also AIDS. Consequently, participants constructed an association among HPV, promiscuity, AIDS, and cervical cancer. Therefore, another name “HPV vaccine” that has been used more recently in Hong Kong may reinforce the confusing relationship between HPV and promiscuous sexual behavior. Consistent with overseas literature (Tatar et al., 2017), their references to their perceived “moral” and “well-behaved” sexual activities thus serve as an explanation for their low perceived risk of HPV-associated diseases and low perceived need for vaccination. The HPV vaccine, thus, has been socially constructed as a vaccine for, and of, promiscuity, which is a cultural taboo according to traditional Chinese sexual values (Meston, Trapnell, & Gorzalka, 1996). Participants were discouraged from receiving HPV vaccination because of its signaling of socially deviant promiscuity. This is consistent with overseas literature, where social norms (Tatar et al., 2017) and subjective norms (Ratanasiripong, 2015) can serve as remarkable deterrents for men, thus preventing them from receiving HPV vaccination.
HPV-related issues are intertwined with sexual health issues. Cancers of the cervix, anus, and penis are all related to reproductive organs. Lack of discussion of these topics as experienced by the participants was not only a consequence of the participants’ low awareness and low perceived risk of HPV-related diseases but was also related to the cultural environment into which the participants had been socialized. The relationship between culture and health care is well established (MacLachlan, 1997). Culture shapes individuals’ conduct, perceptions, and behaviors. Chinese cultural norms substantially influence illness-related behaviors and health seeking in Chinese communities (Lin, Kleinman, & Lin, 1981). The Hong Kong Chinese are noted to be conservative toward sex (China Daily, 2004); open discussion about sex is rare in families and schools (South China Morning Post, 2015). Under such cultural context, sex has been internalized as a cultural taboo, resulting in an avoidance of open conversations about sex-related topics. The absence of conversation on HPV-related topics as experienced by the participants demonstrates the internalized taboo of talking about sex, be it with family, peers, or other members of an individual’s social network. This social and cultural oppression of discussion on sex had discouraged participants from discussing HPV-related topics and obtaining relevant information, which substantially influenced their perceived need to receive HPV vaccination. The cultural taboo, thus, has made health information inaccessible, which disadvantages and inhibits men from pursuing preventive measures against HPV as a result.
Perceptions of reproductive organs among participants may have influenced their perceived need to receive HPV vaccination. A previous study reported that misconceptions and misunderstandings about reproductive organs are indeed not uncommon (Harmanli, Ilarslan, Kirupananthan, Knee, & Harmanli 2014). In contrast to the Western experience, which regards reproductive organs as important to being whole as a person (Harmanli et al., 2014), the participants of this study perceived the diseases of reproductive organs as less serious than those of other organs. Among those few participants who were aware of the potential risk caused by HPV on men, they had a low perceived risk as HPV was perceived as having a limited outcome to men—an unpleasant look of the genital area. Reproductive organs were perceived as “optional,” “minor,” and easily isolated from the human body, and thus from life and death. Although the participants’ discussion mainly concerned women’s reproductive organs, it still hints at how the perceived insignificance of reproductive organs may have contributed to the participants’ low perceived risk of HPV-related diseases, and ultimately to their low perceived need to receive HPV vaccination.
Although advertisements for the “cervical cancer vaccine” had given the participants a brief impression of HPV-related issues, further information about HPV-related issues had been scarce to them. Participants’ conversations about HPV-related issues and the HPV vaccine with those in their social network failed to offer constructive recommendations, and the quality of information they found online varied. Participants rarely discussed the vaccine with their health-care providers because of the perceived irrelevance of HPV and HPV vaccine to themselves. Consequently, limited and distorted knowledge and low perceived risk of HPV were unresolved, or worse, aggravated, thereby reinforcing the low perceived need for men to receive HPV vaccination. Because discussion of the HPV vaccine with health-care providers was reported to increase men’s incentive to getting vaccinated (Tatar et al., 2017), health-care providers are encouraged to take the initiative of proactively discussing the vaccine with men in order to overcome social and cultural constraints. This can help enhance awareness and the perceived need to receive HPV vaccination among men in Chinese communities.
Moving Forward: Promoting the HPV Vaccine to Chinese Men
Given the social and cultural barriers experienced by the participants, future HPV vaccination promotion to men in Chinese communities should be culturally responsive to address the vaccination hurdles. The findings of this study have important implications for public health strategies to fight HPV in the future, and one of the first steps is creating a new Chinese name for the vaccine to promote awareness of the relevance of HPV to the health of both men and women. According to current drug naming protocol, the nonproprietary names of medicinal substances are assigned by the WHO’s International Nonproprietary Name (INN) Expert Group, and each substance is recognized globally by a unique name that adheres to three requirements: (a) corresponding to the classification suggested by WHO and include the specified stem or suffix, (b) reflecting its scientific characteristics, such as chemical structure and pharmacological properties, and (c) the names should be distinctive in sound and spelling while not being inconveniently long (WHO, 2004). However, WHO INN guidelines only focus on the English naming of medicinal products, and there has been no strict policy regarding the Chinese naming of medicinal products. The more usual practice for the Chinese naming of medicinal products is the direct translation of INN according to pronunciation and meaning (Guo & Xu, 2017), which may not warrant awareness from the public as the translated names are often incomprehensible to people.
To attract the attention of men but not ignore the importance of the HPV vaccine to women, the new Chinese name for the HPV vaccine should be comprehensible and relevant to both men and women. Confirmed by a physician with a specialist registration in dermatology and venereology (see Acknowledgment section), the new Chinese name of the HPV vaccine should include both “cervical cancer” and “genital warts” in the naming. This new name, along with other potential names that allude to the consequences of HPV and the uses of HPV vaccine, will be tested for Chinese men’s responsiveness in an experiment according to the Stages of Change Model (Edberg, 2007) in the next stage of this study. It is hoped that a new name for the vaccine will motivate Chinese men to move from precontemplation (not intending to take action) to contemplation (thinking about changing some time in future) in HPV vaccination, and ultimately, to act (action) and receive the vaccine.
Limitations
All the study participants had received at least a high school education, and the majority had received postsecondary education. Men whose highest education level was junior high school or lower were not included in the sampling. Also, those men who had received HPV vaccination were excluded from the sampling, which serves as a limitation in examining the incentives of getting vaccinated. Further studies on men with a wider range of education levels and on those who have received HPV vaccination should be conducted to provide a more holistic analysis of this subject.
Conclusion
Limited knowledge and low awareness of HPV-related issues, low perceived risk of HPV infection, perceived association between HPV vaccine and promiscuity, and a lack of accessible official information on HPV-related topics served as key barriers for the participants to receive HPV vaccination. These barriers were reinforced by the sociocultural environment, cultural values of sexuality, and patriarchal gender values in Hong Kong. Promotion of the HPV vaccine as a “cervical cancer vaccine” with a woman-focused approach also heavily influenced the participants’ uninformed perceptions of HPV-related issues. In addition, patriarchal gender values and oppressive cultural norms in relation to sex had influenced the participants’ perceptions and their intentions to receive the vaccination. To overcome the social and cultural constraints, health-care providers are encouraged to take the initiative of proactively discussing the vaccine with men. This may enhance the awareness and perceived need to receive HPV vaccination among men in Chinese communities.
Supplemental Material
Appendix_1_interview_guide – Supplemental material for Barriers to Receiving HPV Vaccination Among Men in a Chinese Community: A Qualitative Study in Hong Kong
Supplemental material, Appendix_1_interview_guide for Barriers to Receiving HPV Vaccination Among Men in a Chinese Community: A Qualitative Study in Hong Kong by Judy Yuen-man Siu, Timothy K.F. Fung and Leo Ho-man Leung in American Journal of Men’s Health
Footnotes
Acknowledgements
We would like to sincerely thank Dr. Tak-shing Au, a physician with a specialist registration in dermatology and venereology and a Fellow of the Royal College of Physicians (Edinburgh), of the Hong Kong Academy of Medicine, and of the Hong Kong College of Physicians, for his professional medical advice on the new Chinese naming of the HPV vaccine for the study’s upcoming experiment. We would also like to thank all the research participants for sharing their views in this project and making this project possible.
Authors’ Note
The coding and analysis of this study can be provided by the research team upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the General Research Fund, Research Grants Council, University Grants Committee, Hong Kong (grant number: 12641016).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.