
Abstract
Low HPV vaccination rates among US Hispanics/Latinos remain a public health issue. This cross-sectional study investigated the perceived barriers and recommended sources related to HPV vaccination among 209 Hispanic/Latino college students in the United States. From a self-report questionnaire, barriers were insufficient provider recommendations and not having a regular care provider. Doctors, parents, and nurses were identified as the most effective sources for recommending HPV vaccination. Uncertain effectiveness was more likely to be reported as a barrier to HPV vaccination by participants who identified as Catholic. Participants born outside the U.S. were more likely to report “no recommendation received” and “not knowing where to get vaccine.” Health care providers can promote HPV vaccination by acknowledging familial allegiances of Hispanic/Latino college students. The role of religion and cultural beliefs in HPV vaccination among Hispanics/Latinos underscores the need for further research in this area. Universities could be a place of HPV awareness initiatives, as having more formal education does not translate into having more HPV knowledge. To decrease HPV vaccination barriers, the home-based vaccination program could potentially impact HPV vaccine uptake among Hispanic/Latino populations and should be further explored.
Introduction
Human papillomavirus (HPV) is the most commonly acquired viral infection of the reproductive tract in the world. 1 Long-lasting HPV infections can cause genital warts and certain kinds of cancer, including cancers of the cervix, anus, vagina, vulva, penis, and oropharynges. 2 The HPV vaccine is the first vaccine that effectively prevents HPV-attributable genital warts and cancers, such as cervical, anal, vaginal, and vulvar cancers. 3 HPV vaccination is routinely recommended at the age of 11 or 12 years and is also recommended for all individuals up to the age of 26 years who have not received adequate vaccination earlier. 4 Since the introduction of the HPV vaccine, there has been a substantial decrease of 81% to 88% in infections caused by HPV types associated with most HPV-related cancers and genital warts. 5 Additionally, there has been a 40% decrease in HPV-related cervical pre-cancers. Given the important role of HPV vaccination in preventing certain cancers, racial/ethnic disparities exist in HPV immunization. Hispanics aged 18 to 26 years (40.6%) in the United States were less possible to get an HPV vaccine in comparison with their white counterparts (49.7%). 6 Moreover, HPV vaccination rates among Hispanic/Latino college students studying in the United States were found to be lower compared to Caucasian students and students from other ethnicities (41%vs 63% and 51%). 7
The HPV vaccination rates among Hispanics/Latinos are well below the Healthy People 2030 objective of an 80% rate for HPV vaccination. 8 It is especially important to understand perceived barriers to HPV vaccination among Hispanic/Latino populations. This study focused on Hispanic/Latino college-aged students because they can make more autonomous decisions about HPV vaccination and can still get the vaccine. There is a limited number of studies examining perceived barriers to HPV vaccination among Hispanic/Latino college students. Research on general Hispanics/Latinos showed that the common barriers to HPV vaccination include misconceptions about no indication for males,9 -13 parents’ belief about their child’s non-engagement in sexual activity,10,14 inadequate HPV knowledge, 15 fear of encouraging promiscuity and stigmatization,16 -18 fear of side effects,13,14,19 -21 and lack of transportation. 20 Among the few studies specifically for Hispanic college students, the barriers to getting an HPV vaccine include affordability, 22 side effect concerns,23,24 knowledge deficits about the risks of contracting HPV infections,23,24 and lack of time.22,24
The purposes of the study were to (a) identify the barriers to obtaining the recommended doses of the HPV vaccine, (b) investigate the most effective sources of recommendation for HPV vaccination, and (c) assess factors (i.e., demographics, knowledge and attitudes regarding HPV and HPV vaccination) related to barriers to and recommendations for getting an HPV vaccine among a sample of Hispanic/Latino college students studying in the United States. The findings from this research have implications for informing the development of policies and interventions aimed at addressing barriers and improving vaccination rates among Hispanics/Latinos, with the overarching goal of reducing disparities in HPV-related incidents and mortalities within this population. The impact of a home-based vaccination program on HPV vaccine uptake and its potential to overcome specific logistical barriers among Hispanic/Latino populations are discussed in this study.
Methods
Design and Sample
A descriptive, cross-sectional design was used for this study. A person was eligible for the study if he or she was an English- or Spanish-speaking Hispanic/Latino college student who was enrolled in a college or university in the United States and at least 18 years of age at the time of recruitment. This study obtained approval from the Institutional Review Board at the university where the principal investigator is affiliated.
The investigators employed a network sampling strategy, also known as snowball sampling, 25 which has demonstrated success in collecting data from immigrant groups by utilizing referrals from early participants. 26 During the initial recruitment phase, the investigators reached out to potential participants they were already acquainted with and provided them an introductory letter. The letter provided an overview of the research (e.g., purposes, eligibility, contact information) and extended an invitation to join the study. The investigators also requested their assistance in recruiting other eligible participants for the research. Out of those approached, 8 students consented to take part in the study and were provided with a paper format questionnaire. They were also given the survey and the introductory letter to recruit potential participants. Participants’ informed consent was indicated by returning the completed survey. Respondents were instructed to return the completed survey to either the data collectors or mail it directly to the principal investigator.
Instrument
The self-report questionnaire, available in English and Spanish, consisted of 4 scales used to address study purposes. The questionnaire is only available in a printed paper format.
Demographic information
Demographic data included information about age, gender, birthplace, year in school, major, work status, marital status, religious preferences, and religiosity. The demographic data also contained items related to health insurance, primary care provider, and any history of cervical cancer in the participant’s family.
HPV knowledge scale
This scale comprises 16 true/false statements designed to evaluate knowledge regarding HPV and its vaccine. Of these, 13 items were originally used to assess HPV knowledge among female college students in Lebanon. 27 The investigators added 3 items in the scale to address the interrelationships between cancers, HPV vaccine, and Pap smears. These items were reviewed by experts to ensure content validity. One point was awarded for each accurate response. The score was calculated by summing the number of correct points and dividing it by the total of 16 items. The resulting value was then multiplied by 100 to obtain the final score, which ranged from 0 to 100. A higher score indicated a greater level of HPV knowledge. In this sample, the Cronbach’s alpha of .90 indicated excellent internal consistency.
Attitudes about HPV and HPV vaccination
Attitudes toward HPV and its vaccine were measured by 7 questions derived from the HPV Attitude Scale by Dany and colleagues. 27 All responses were scored on a Likert scale, ranging from strongly agree (1) to strongly disagree (5). The attitude score was calculated by averaging the responses to the 7 questions (range = 1-5). A lower score suggested a more positive attitude. For this study, Cronbach’s alpha was .76 for this scale.
Practices, barriers, and effective recommendations related to HPV vaccination
Regarding HPV vaccination practices, participants were asked to provide information on the country and age at which they received their first HPV vaccine dose, as well as the total number of HPV vaccine doses they had received. A single-item question with 10 choices (e.g., cost, concerns about side effects, other) was used to assess barriers to HPV vaccination. To evaluate effective sources of HPV recommendations, participants were asked to provide the name(s) of the most influential source(s) that recommended the HPV vaccine.
Statistical Analyses
Data analyses were performed by SPSS 25 (Windows). Descriptive statistics were used to summarize respondents’ demographic information, HPV knowledge and attitudes, HPV vaccination practices, barriers to obtaining the HPV vaccine, and sources providing effective recommendations for HPV vaccination. A multiple logistic regression analysis was conducted to assess factors (i.e., demographics, HPV knowledge and attitudes) related to barriers in obtaining HPV vaccination and effective sources providing recommendations for HPV vaccination. The analysis used a 95% confidence interval (CI). p < .05 was used to determine the significance level.
Results
Participant Characteristics
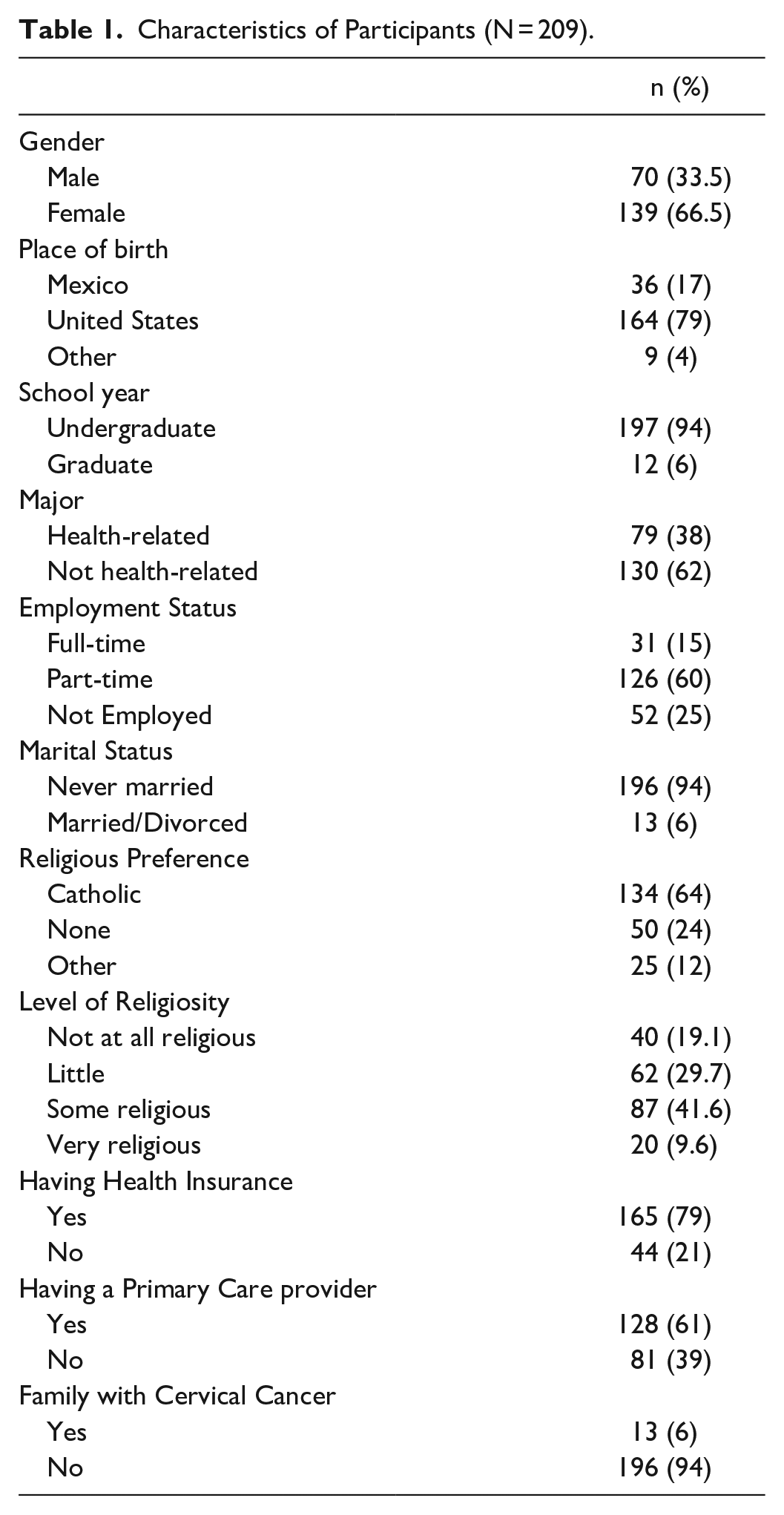
A convenience sample of 210 participants was recruited from multiple colleges and universities in the USA. Only one participant completed the survey in Spanish and this participant’s responses were excluded from statistical analysis for a sample of 209. The age of 209 participants ranged from 18 to 36, with a mean of 20.89 years (SD = 3.14). As displayed in Table 1, 209 participants were predominantly female (66.5%), born in the U.S. (79%), in the undergraduate program (94%), and worked part-time (60%). Sixty-four percent self-identified as Catholic with 51.2% having at least some level of religiosity. Most reported having health insurance (79%) and a primary care provider (61%). Approximately 6% reported having a family member with cervical cancer.
Characteristics of Participants (N = 209).
Knowledge and Attitudes Regarding HPV and Its Vaccine
Among 209 participants, the mean score on the 16 HPV knowledge questions was 40.64 ± 27.26 (ranging from 0 to 100), indicating a low-moderate level of HPV knowledge. The mean score of 7 questions related to attitudes toward HPV and the HPV vaccine was 2.38 ± 0.56 (ranging from 1 to 5), indicating a moderate attitude.
Barriers to HPV Vaccination
As exhibited in Table 2, 77 (36.8%) reported that they had never received the HPV vaccine, while 23 (11%) were uncertain about their vaccination status. Among the 109 vaccinated respondents, 105 reported receiving their first HPV vaccine in the United States, with an average age of 14.90 years. For participants who were not fully vaccinated, the barriers were (a) no healthcare providers recommended the HPV vaccines (n = 61), (b) the lack of a regular healthcare provider (n = 30), (c) vaccination not considered due to sexual inactivity (n = 29), (d) no knowledge of where to get HPV vaccine (n = 28), or (e) the perception of having no risk for HPV (n = 23).
Practices, Barriers, and Effective Recommendations Related to HPV Vaccination (n = 209).
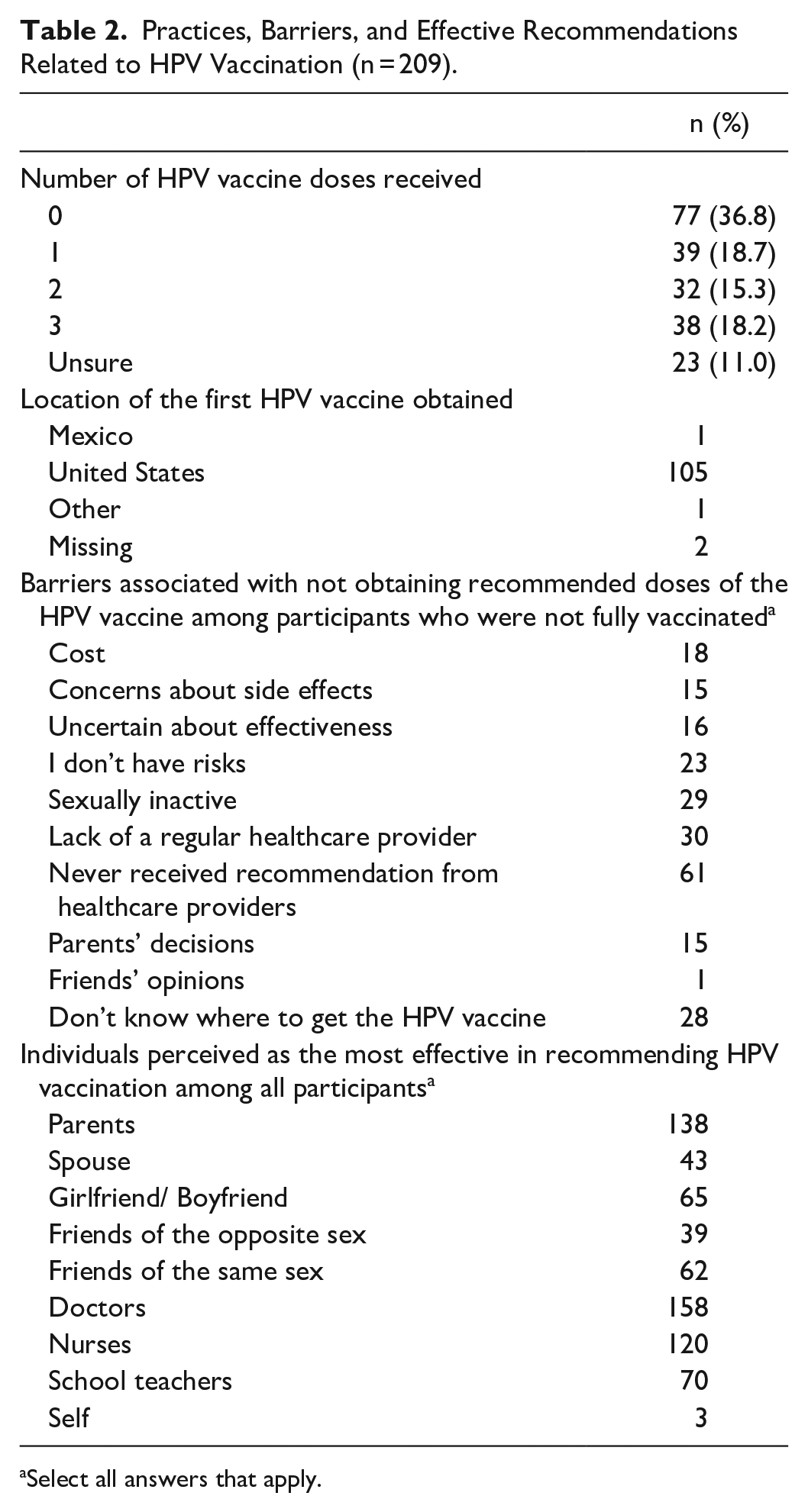
Select all answers that apply.
The Most Effective Sources of Recommendations
The respondents stated that the most effective sources to recommend the HPV vaccine were doctors (n = 158), parents (n = 138), and nurses (n = 120) (see Table 2).
Factors Related to Barriers and Recommendation Sources
The multiple logistic regression results showed that barriers to not obtaining the recommended dose of HPV vaccine were significantly associated with certain conditions (see Table 3). “Uncertain effectiveness” as a barrier to HPV vaccination was more likely to be reported by participants who identified as Catholic (OR = 16.51, 95% CI [1.91-142.9], p = .011), participants with greater knowledge about HPV (OR = 1.29, 95% CI [1.09-1.53], p = .003), and participants with more negative attitudes toward HPV and its vaccine (OR = 3.87, 95% CI [1.18-12.66], p = .025). The perception of “not having risks” was more likely to be reported as a barrier by male participants (OR = 3.37, 95% CI [1.76-6.90], p = .00). Participants born outside the U.S. were more likely to report “no recommendation received” (OR = 2.21, 95% CI [1.05-4.66], p = .038) and “not knowing where to get vaccine” (OR = 2.94, 95% CI [1.08-8.00], p = .035) as barriers to HPV vaccination. “Not knowing where to get the vaccine” was more likely to be reported by respondents who were not Catholic (OR = 0.35, 95% CI [0.14-0.87], p = .024) and had lower levels of HPV knowledge (OR = 0.084, 95% CI [0.74-0.96], p = .01). No significant associations were found between the barriers and other study variables.
Multivariate Analysis for Barriers to Not Receiving Recommended HPV Vaccine.
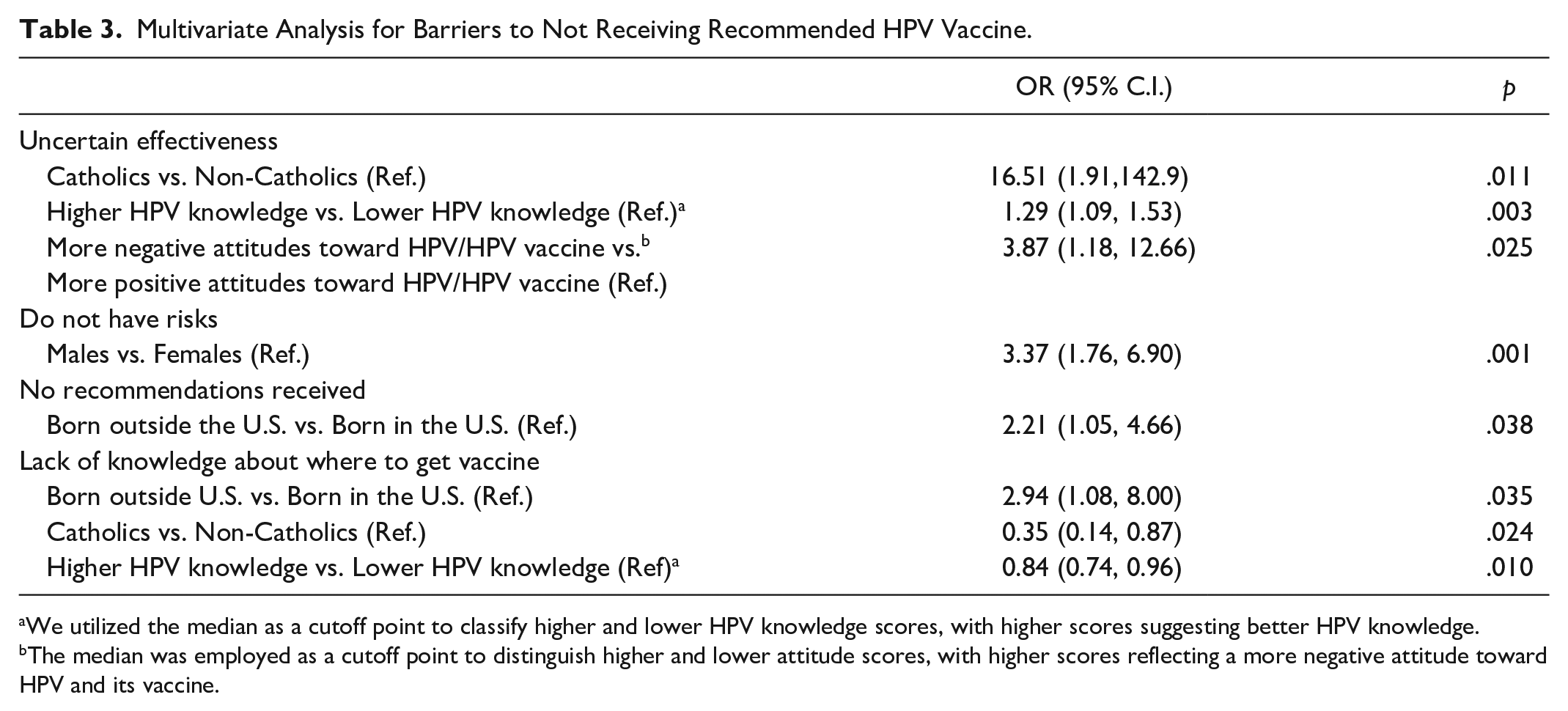
We utilized the median as a cutoff point to classify higher and lower HPV knowledge scores, with higher scores suggesting better HPV knowledge.
The median was employed as a cutoff point to distinguish higher and lower attitude scores, with higher scores reflecting a more negative attitude toward HPV and its vaccine.
As displayed in Table 4, older respondents demonstrated a lower likelihood of indicating spouses as their most effective source in recommending HPV vaccination (OR = 0.25, 95% CI [0.10-0.63], p = .003). Respondents with greater HPV knowledge were more inclined to mention their same-sex friends as the most effective sources in recommending HPV vaccination (OR = 1.02, 95% CI [1-1.03], p = .022). Participants with lower attitude scores (more positive attitudes) were prone to indicating doctors as the most effective individuals in recommending HPV vaccination (OR = 0.47, 95% CI [0.23-0.95], p = .036). No other significant relationships were found.
Multivariate Analysis of the Most Effective Individuals in Recommending HPV Vaccination.
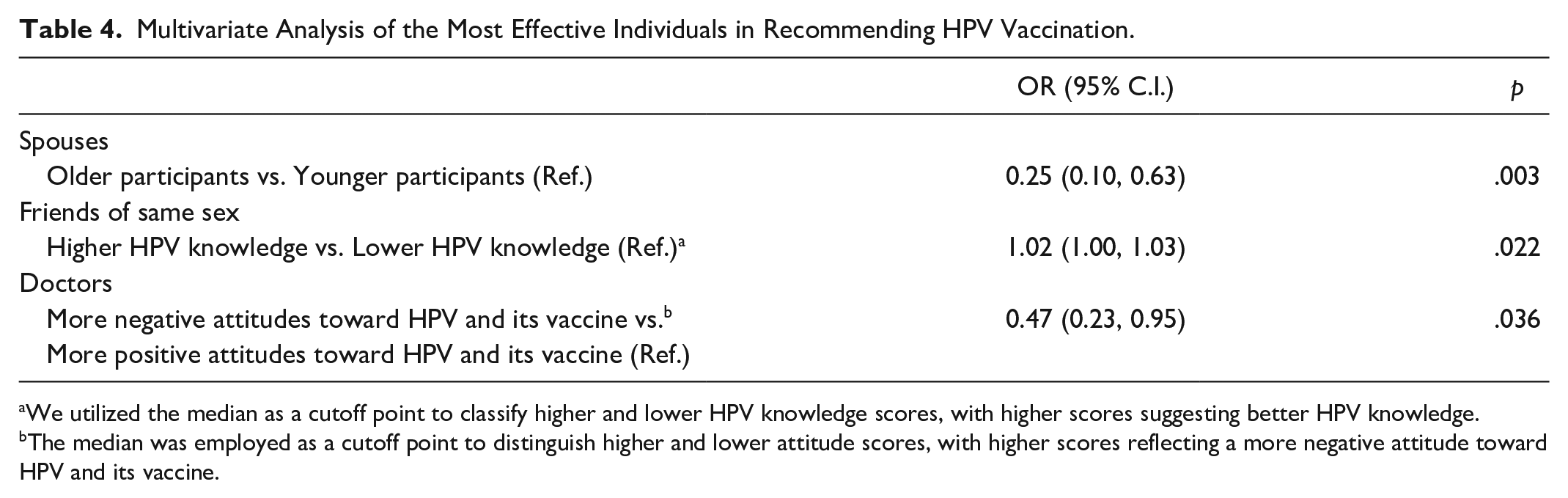
We utilized the median as a cutoff point to classify higher and lower HPV knowledge scores, with higher scores suggesting better HPV knowledge.
The median was employed as a cutoff point to distinguish higher and lower attitude scores, with higher scores reflecting a more negative attitude toward HPV and its vaccine.
Discussion
Our study aimed to identify the barriers to obtaining the recommended dose of the HPV vaccine and determine the most effective sources for recommending HPV vaccination among Hispanic/Latino college students studying in the United States. This study is one of the first to examine this issue, which is a timely endeavor given the findings. The lapsed performance by and/or absence of a healthcare provider served as the most cited barrier for not obtaining the HPV vaccine. Our findings are similar to earlier studies that highlight the significance of healthcare providers and their recommendation in promoting HPV vaccination among Hispanic/Latino populations.20,23,24 This reliance on a regular healthcare provider could result in not acquiring the recommended preventive services for HPV infections, leading to subsequently higher HPV-related diseases. Campus health centers are in the optimal position to emphasize HPV vaccinations while strengthening these students’ capacity to take an active role in their health care.
Another reason given for not receiving the HPV vaccine was that participants reported that they were not sexually active. This misconception that is constructed on restrictive social taboos and cultural mores diminishes the reality of the risk for contracting HPV infections, and it has been reported in other studies.24,28 Implementing campus-based educational strategies to address misconceptions surrounding the HPV vaccine is crucial for Hispanic/Latino college students. It is also equally important to consider the preferred methods of learning and discussing this topic. Health messages delivered through a narrative format or media have the potential to improve HPV knowledge, attitudes, and intentions among Hispanics/Latinos.29,30
Doctors and nurses along with parents were identified as the most effective sources for recommending the HPV vaccine. Our findings are congruent with those of other studies,9,24 where healthcare providers have an important role in influencing Hispanics’ decisions regarding HPV vaccination. While the strong family ties and filial piety embedded in Hispanic culture influence the decision-making process of Hispanic/Latino college students, our results concur with earlier studies conducted among Hispanic populations where family members’ perspectives immensely impacted or rather governed the health decision-making process.17,23,24 To facilitate successful HPV vaccination among Hispanic/Latino college students, it is crucial to involve doctors, nurses, and family members in the intervention. Additionally, tailoring the message to specifically address the individual concerns and unique needs of each student and family member is of utmost importance.
Participants with a Catholic affiliation tended to express more uncertainty regarding the effectiveness of the HPV vaccine. With White, Black, and Hispanic parents, a study was conducted to examine the role of religion in getting the HPV vaccination. 31 The results indicated that parents with greater attendance at their church were more likely to oppose HPV vaccination. Hispanic/Latino college students may face a conundrum when their parents’ traditional and religious views conflict with their health-conscious views about sexual behavior and safe practices. The influence of religion on HPV vaccination efforts among Hispanic/Latino students highlights an area for future research.
Participants born outside the United States were more likely to state not knowing where to get vaccinated and a lack of provider recommendation as barriers to HPV vaccination. In a study conducted with Hispanics born in the U.S. and Hispanics immigrated to the U.S., 32 the U.S. born Hispanics were more likely to know about the HPV vaccine, where HPV vaccine information can be acquired, and how to get the HPV vaccine. One plausible explanation involves the parents’ low acculturation level and lack of parental education that impacted the children’s knowledge and awareness about HPV vaccination. Another possible reason could be due to a disruption in the medical homes among Hispanic adolescents, as medical homes offer accessible and continuous health care. Hispanic adolescents who do not have a medical home may face additional challenges in completing their second and third doses of the HPV vaccine due to difficulties in identifying appropriate healthcare resources. 14 Previous research has also shown that Spanish-speaking parents were less likely to be encouraged to initiate the HPV vaccine series or receive physician recommendations for HPV vaccination.13,33 Providing information to students about the available types of healthcare during the enrollment process is crucial, as it empowers them to take an active role in managing their healthcare within the university setting.
Male respondents were more likely to report “not having risks” as a barrier to HPV vaccination. In a qualitative study conducted with male Hispanic college students, the majority did not acknowledge their risk for contracting HPV and believed that it primarily affected women. 24 This misinformation may stem from the delayed recommendation for males to receive the vaccine and the initial focus on females as the targeted population for vaccination. Another possibility could encompass the stigmatization about discussing sexually transmitted infections, 34 which nurtures a “dating more” or assumption that sexual partners are healthy if they appear to be. 35 To address misconceptions, researchers utilized a photographic short story format, also known as a “fotonovela,” to enhance perceived susceptibility and improve attitudes toward the HPV vaccine for Hispanic youths. 29 The fotonovela education could be delivered in schools (e.g., classrooms, waiting rooms of student health clinics), homes, or other settings as a subtle yet stimulating teachable moment about the HPV vaccine.
Implications for Home Health Care Providers
Our findings underscore the importance of implementing policy changes that target the challenges associated with achieving effective HPV vaccination coverage among Hispanic/Latino populations. Key barriers identified in our study included the lack of HPV vaccine recommendation from healthcare providers, absence of regular healthcare providers, misconceptions regarding the HPV vaccine, limited knowledge about where to obtain the HPV vaccine, and participants from immigrant families. In a proactive approach, home health care providers could play a crucial role by providing education about HPV and informing individuals in the Hispanic/Latino community about available resources during home care services.
To address HPV vaccination barriers among Hispanic/Latino populations, modifying vaccine administration policies to enable home healthcare providers to administer the HPV vaccine at clients’ homes can help overcome certain logistical challenges. This approach eliminates the need for individuals to travel to clinics or doctors’ offices, provides flexible scheduling options, and delivers care in the comfort of their own homes. By recognizing the significant role that family plays in Hispanic/Latino culture, this home-based approach could create a supportive environment during the vaccination process by actively involving family members. Policies and protocols should address supply, storage during transportation, vaccine education, record keeping, and vaccination administration when administering HPV vaccine in the home setting. 36
Limitations of the Study
One of the limitations of this study was the use of a self-report survey. Participants may have over- or underreported when answering. Another limitation of this study is the challenge in generalizing the findings due to the small sample size and cross-sectional design. In addition, all the participants chose the English version of the survey. It is possible that findings could differ if the sample included a larger number of participants who preferred Spanish. Finally, we acknowledge that data on factors such as geographic regions, cultural beliefs, generation, acculturation level, place of residence, and the utilization of campus health centers, which could potentially influence HPV vaccination, were not collected in this study.
Conclusions
The findings in this study have implications for program development that considers the cultural and religious aspects in addressing HPV infections in a global community. Research should investigate how cultural and religious beliefs can act as facilitators or barriers to the uptake of the HPV vaccine. Understanding these factors is crucial as an initial step toward developing interventions aimed at increasing vaccination rates. University health facilities should consider developing a campus-based initiative that involves family members, nurses, and physicians in promoting HPV vaccination to achieve positive outcomes. A home-based vaccination program could potentially impact HPV vaccine uptake among Hispanic/Latino populations and should be further explored.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.