
Abstract
In 2018, nine-valent human papillomavirus (HPV) vaccine eligibility expanded to include adults aged 27 to 45. This study aimed to identify knowledge, attitudes, and beliefs (KABs) about HPV and HPV vaccination among newly eligible mid-adult men, for whom uptake in adolescence and younger adulthood remains suboptimal. We conducted six virtual focus groups (N = 34 participants) with unvaccinated men aged 27 to 45 living in Southern California’s Inland Empire. Data were systematically analyzed to identify emergent themes using the rigorous and accelerated data reduction technique. The sample of men was diverse (79% Hispanic, non-Hispanic Black, Asian, or mixed race/ethnicity; 26% gay or bisexual) and captured participants from across the socioeconomic spectrum. Eighty-eight percent of participants had never received a provider recommendation to be vaccinated against HPV. Many had unanswered questions about HPV and HPV vaccination, could not recall any HPV-related cancers that affect men, and were unaware of their current eligibility for vaccination. Embarrassment and stigma surrounding vaccination against a sexually transmitted infection, concerns about vaccine side effects and safety, and preferences for preventing HPV via “safer sex” and monogamy were salient barriers to vaccination. Nevertheless, many men were eager to learn more about HPV vaccination and engage with health care providers around that topic. Interventions aimed at improving men’s knowledge, changing social norms, and supporting health providers to identify HPV vaccine-eligible patients may be especially fruitful for facilitating shared clinical decision-making between mid-adult men and their health care providers.
Introduction
Human papillomavirus (HPV) is a common sexually transmitted infection that can cause anogenital warts and cervical, genital, anal, and oropharyngeal cancers (Lewis et al., 2021). Men account for more than 40% of the nearly 45,000 cases of HPV-related cancers diagnosed in the United States annually, and oropharyngeal and anal cancers are on the rise for this population (Liao et al., 2022; Senkomago et al., 2019). To prevent new HPV infections and HPV-associated disease, HPV vaccination is routinely recommended for all 11-/12-year-olds, and catch-up vaccination is advised for unvaccinated individuals through age 26 (Meites et al., 2019). Despite these recommendations, as of 2019 only 37% of U.S. men aged 18 to 26 reported having ever been vaccinated against HPV (Black & Boersma, 2021).
In 2018, the U.S. Food and Drug Administration (FDA) expanded nine-valent HPV vaccine approval for use in adults aged 27 to 45. Since 2019, the U.S. Advisory Committee on Immunization Practices (ACIP) has recommended shared clinical decision-making about HPV vaccination for adults in this age group (Meites et al., 2019). Although evidence suggests the population benefit of vaccinating adults aged 27 to 45 would be minimal, ACIP recognizes “some adults who are not adequately vaccinated might be at risk for new HPV infection and might benefit from vaccination in this age range” (Meites et al., 2019, p. 700). Accordingly, the ACIP guidelines state that clinicians do not need to routinely discuss HPV vaccination with patients older than 26 years but rather “can consider discussing vaccination with persons who are most likely to benefit” (Meites et al., 2019, p. 700).
Mid-adult patients may ultimately bear the burden of initiating shared clinical decision-making conversations about HPV vaccination because (1) many health care providers are unaware of the new ACIP guidance and/or do not discuss HPV vaccination with eligible patients and (2) there is a lack of clinical guidelines to help providers identify patients who may still benefit from HPV vaccination after age 26 (Alber et al., 2021; Hurley et al., 2021; Thompson et al., 2021; Wheldon et al., 2021). Understanding the knowledge, attitudes, and beliefs (KABs) about HPV and HPV vaccination among 27- to 45-year-old men may thus be important for promoting shared clinical decision-making for this population and improving vaccine uptake among those at risk of acquiring new HPV infections.
Quantitative studies have begun to explore adults’ KABs about HPV and HPV vaccination within the context of new clinical decision-making guidelines for 27- to 45-year-olds. This research has identified low awareness of eligibility for HPV vaccination (Alber et al., 2021), low knowledge of HPV-related cancers that directly affect men (Thompson et al., 2020), concerns about HPV vaccine safety, and beliefs that the HPV vaccine is unnecessary (Muthukrishnan et al., 2022) among mid-adults, which may pose barriers to uptake. Mid-adults’ willingness to be vaccinated has been identified as being positively associated with level of knowledge about HPV vaccination, perceived ease of understanding HPV vaccine information, and perceived vulnerability to HPV-related cancers (Galvin et al., 2023). Positive attitudes toward HPV vaccination, perceived effectiveness of vaccines against HPV infection, and perceived likelihood of benefiting from HPV vaccination have been reported to increase mid-adults’ perceived likelihood of getting vaccinated (Thompson et al., 2021). Health care provider recommendation and perceived social norms have also been reported to predict mid-adults’ HPV vaccine uptake (Alber et al., 2021).
Disparities in HPV and HPV vaccine-related knowledge and awareness by gender, socioeconomic status (SES), and race/ethnicity have been documented in quantitative studies of U.S. adults aged 18 and older, prior to HPV vaccine age eligibility expansion. These studies indicate that males, lower SES, Hispanic, and Black individuals tend to have lower HPV vaccine-related awareness and knowledge compared with their female, higher SES, and non-Hispanic White counterparts (Boakye et al., 2017; McBride & Singh, 2018; Osazuwa-Peters et al., 2017). Though heterosexual men can transmit HPV and experience negative HPV-related outcomes, most of the previous research on HPV and men has focused exclusively on gay and bisexual men who have sex with men (Cooper et al., 2018). Moreover, few HPV vaccine-related studies have focused on racial/ethnic minority U.S. men (Cooper et al., 2018).
Qualitative research considering KABs about HPV or HPV vaccination among U.S. mid-adult men since FDA approval of the vaccine for 27- to 45-year-olds is scant. This study qualitatively examines mid-adult men’s baseline KABs about HPV and HPV vaccination using a racial/ethnically diverse sample. In doing so, it aims to generate nuanced knowledge for guiding interventions to promote shared clinical decision-making about HPV vaccination for men who are newly eligible due to age expansion.
Methods
Setting
This study was part of a larger research project documenting barriers and facilitators to HPV vaccination among adults in Southern California’s Inland Empire. This 27,000 square mile region situated adjacent to Los Angeles and Palm Springs is larger than 10 United States and has a population of more than 4.6 million (Newman & Paci, 2020). The Inland Empire has a higher poverty rate compared with the rest of California and the United States overall (Brady et al., 2018) and is racial/ethnically diverse, with approximately 52% of residents identifying as Hispanic and a further 17% identifying as part of a non-Hispanic racial minority group (Newman & Paci, 2020). The region also faces a severe shortage of health care professionals leaving residents medically underserved with limited access to health care providers (Newman & Paci, 2020).
Participants and Recruitment
The Socio-Behavioral Institutional Review Board at the University of California, Riverside approved the study. Participants were recruited through email announcements from community health organizations, posters in 20 community health clinics, and social media posts on Facebook, Instagram, Twitter, and Reddit. Men aged 27 to 45 were eligible to participate if they (1) lived in the Inland Empire, (2) could speak and understand English, (3) identified as White, Black, Hispanic, and/or Asian (the four most populous racial/ethnic groups in the region), (4) had not received any previous HPV vaccines, and (5) had access to an Internet-enabled phone, tablet, or computer.
Participants enrolled in the study by completing an online consent form and survey that collected demographic information, confirmed registrants met all inclusion criteria, and allowed participants to choose a pseudonym that would be used to link survey responses with focus group data. To prevent fraudulent participation, we reviewed GeoIP addresses and excluded any registrants who enrolled from outside of California or who screened out and made repeated registration attempts (Kramer et al., 2014). Fifty registrants qualified for the study and were invited to participate; 34 participated and received US$30 electronic gift cards as incentives.
Focus Groups
We used focus groups to elicit group-level norms and values and to solicit in-depth explanations from participants (Liamputtong, 2011). Due to the COVID-19 pandemic, we conducted focus groups virtually using a text-based Adobe Connect chatroom. Unlike video-based virtual focus groups, this text-based format did not require individuals have a webcam or high-bandwidth Internet connection to participate. This modality also allowed participants to discuss potentially sensitive health-related information anonymously with one another and may have helped reduce logistical barriers to participation for some individuals from marginalized racial/ethnic and/or socioeconomic backgrounds that can be difficult to recruit for face-to-face groups (Campbell et al., 2001; Rupert et al., 2017; Woodyatt et al., 2016).
Between November 2020 and January 2021, we conducted six 90-min focus groups with five to seven participants in each group. Group size was consistent with best practices for conducting synchronous text-based online focus groups, which recommend upper limits of five to eight participants in each group (Hinkes, 2021; Lobe, 2017). To elicit baseline KABs about HPV and HPV vaccination, participants were not given any preliminary educational information about HPV, HPV vaccination, FDA approval, or ACIP recommendations. A research assistant was present in each focus group and monitored access to the chatroom. The study’s principal investigator moderated the focus groups using a semistructured interview guide, which has been previously published and is publicly available (Polonijo et al., 2022). The interview guide covered two areas relevant to this study: (1) knowledge and beliefs about HPV and HPV vaccination and (2) attitudes toward HPV vaccination. Participants used pseudonyms and engaged in group discussions. When questions arose about HPV or HPV vaccination that participants were unable to answer among themselves the moderator relayed basic information provided by the U.S. Centers for Disease Control and Prevention (CDC, 2020). For example, participants often questioned the upper age limit for HPV vaccination, and, in response, the moderator stated the vaccine was “approved for use in adults up to age 45.”
Data Analysis
We calculated descriptive statistics for the demographic surveys using Stata 16. Focus group chat logs were downloaded, and any identifying information disclosed by participants was removed. The deidentified data were then imported into Microsoft Excel and analyzed using the “rigorous and accelerated data reduction” technique (Watkins, 2017). This entailed reviewing the data in relation to the question: “What are men’s KABs about HPV and HPV vaccination?” Text that did not address this question was removed, and the remaining text was open coded (Corbin & Strauss, 2014) by two of the study’s authors to identify themes that emphasized recurring patterns in the data. Representative quotes were then linked to participants’ age, education, and race/ethnicity data from the sociodemographic survey for interpretation. A third author reviewed the final themes and codes to confirm interpretations maintained internal validity. Any discrepancies in coding were resolved through discussion. No new themes had emerged upon the analysis of the sixth focus group, suggesting we had reached data saturation.
Results
Participant Characteristics
Descriptive statistics for the sample (N = 34) are detailed in Table 1. Participants were between the ages of 27 and 41 (median = 30.5 years) and were diverse in terms of race/ethnicity, with 44% identifying as Hispanic (n = 15), 24% (n = 8) as non-Hispanic Black, and 12% (n = 4) as Asian or mixed-race/ethnicity. About three-quarters of participants (74%; n = 25) identified as heterosexual. Household incomes ranged from US$0 to more than US$150,000; the median household income of participants (US$50,000) was approximately US$15,000 to US$20,000 lower than the median household income in the Inland Empire region (U.S. Census Bureau, 2022), reflecting the fact that income tends to increase with age and our sample was relatively young. Most participants were unmarried (62%, n = 21), had health insurance (82%, n = 28), and had a bachelor’s degree or higher level of education (68%, n = 23). Twenty-six participants had previously been eligible for HPV vaccination (when aged 9 to 26 years), among which 88% (n = 23) had never received a health provider recommendation to be vaccinated against HPV.
Sample Characteristics (N = 34)

Note. HPV = human papillomavirus.
The highest household income value has been suppressed to protect participant confidentiality. bWe combined Asian and mixed race/ethnicity participants into a single category to protect participant confidentiality. cAmong only those participants who were previously eligible for HPV vaccination when aged 9 to 26 years (n = 26).
Questions About HPV and HPV Vaccination
Though participants were not prompted to ask questions about HPV or HPV vaccination, several raised such questions throughout the focus group discussions. We provide examples of these questions, summarized thematically, in Table 2. Overall, questions focused on how to prevent HPV transmission, how to test for HPV infection, the etiology of HPV and HPV-related cancers, criteria for HPV vaccine eligibility, the safety profile of HPV vaccines, and how/where to access HPV vaccines.
Questions About HPV and HPV Vaccination

Note. HPV = human papillomavirus.
Qualitative Themes
Six key themes emerged from the qualitative data: (1) low awareness and limited knowledge about HPV and HPV vaccination, (2) perceptions of HPV as a “women’s only” disease, (3) embarrassment and stigma surrounding HPV vaccination, (4) safer sex and monogamy as preferred means of HPV prevention, (5) concerns about HPV vaccine side effects and safety, and (6) health care providers as trusted sources of HPV vaccine information. We summarize these themes in Table 3 and provide an in-depth discussion of them below.
Qualitative Themes and Exemplary Quotes
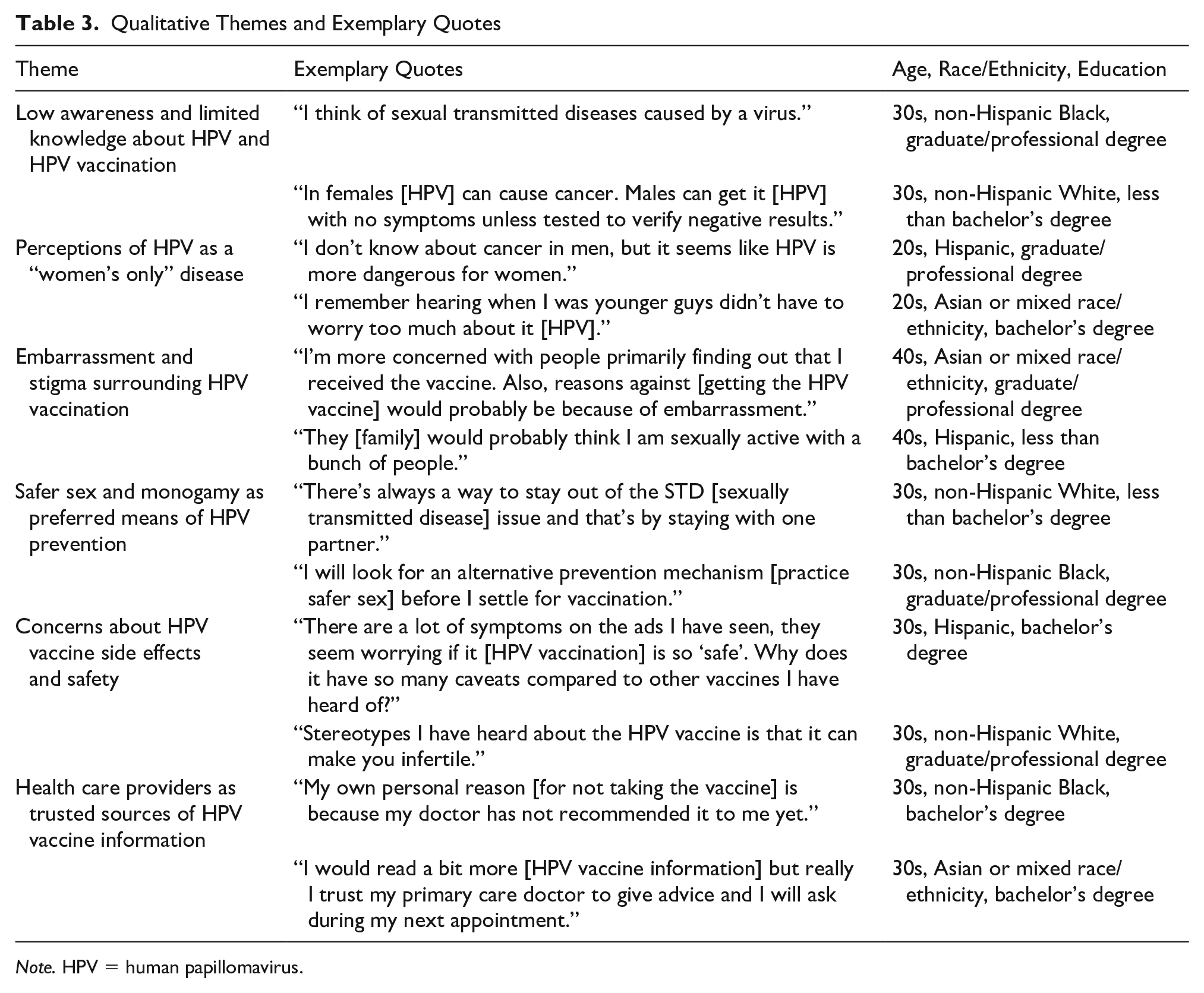
Note. HPV = human papillomavirus.
Low Awareness and Limited Knowledge About HPV and HPV Vaccination
Participants across all racial/ethnic and educational groups reported limited awareness and knowledge about HPV and HPV vaccination. Participants identified social media, “trusted health websites” (e.g., WebMD, MayoClinic, and Planned Parenthood), pharmaceutical advertisements, and discussions with family and friends as their primary sources of HPV and HPV vaccine information. Most participants reported HPV was transmitted via “unsafe sex” but were unaware HPV can be transmitted via sexual skin-to-skin contact alone. Though many participants recalled HPV caused genital warts, most participants were unaware of any HPV-related cancers that affect men. Many participants reported that HPV vaccination is recommended for teenagers, while the vast majority were unaware the vaccine had been FDA-approved for adults through age 45. For example, one participant emphasized: “All I know is there is an age limit, and I am over the age limit” (30s, Asian or mixed race/ethnicity, graduate/professional degree).
Perceptions of HPV as a “Women’s Only” Disease
Many participants reported they considered HPV to be “serious” due to the cancer risks it poses to women. As one heterosexual participant shared, “I’m not so worried about me, I couldn’t handle the possibility of giving it [HPV] to a partner and them developing cancer because of me” (30s, non-Hispanic White, less than bachelor’s degree). Most participants also only knew of female friends or family members that had been vaccinated against HPV and lacked awareness of the utility of vaccinating men. As one participant shared, “I thought it was more important for young ladies to get vaccinated and didn’t realize how important it was for men as well” (40s, Hispanic, less than bachelor’s degree). Despite initially conceptualizing HPV as a “women’s only” disease, upon learning that HPV-related cancers affect men, several participants reported being open to being vaccinated. For example, one participant shared: “if people were told about the cancer, they’d want to get vaccinated” (40s, Hispanic, less than bachelor’s degree).
Embarrassment and Stigma Surrounding HPV Vaccination
Some participants reported that embarrassment and stigma surrounding vaccination against a sexually transmitted infection were perceived barriers to HPV vaccination. For example, multiple participants expressed believing HPV vaccination was only necessary for people with multiple concurrent sexual partners and/or reported that friends, family, or health care providers might assume they were promiscuous if they were to seek HPV vaccination. As one participant noted: “family might be questioning why I would get such a vaccine” (40s, Asian or mixed race/ethnicity, graduate/professional degree). A few participants reported they anticipated negative reactions from members of local religious communities which could deter them or other men in their community from HPV vaccination. For example, one participant shared: “[the] religious community might balk at the idea [of HPV vaccination] if they’re conservative in views of pre-marital sex” (30s, Asian or mixed race/ethnicity, graduate/professional degree).
Safer Sex and Monogamy as Preferred Means of HPV Prevention
Several participants suggested that practicing “safer sex” and maintaining monogamous relationships were effective, and preferred means of HPV prevention that negated the need for vaccination. For example, one participant who had previously been eligible for HPV vaccination before age 27 shared that they had not been vaccinated because they were “always practicing safe sex and [using] condoms” (30s, non-Hispanic Black, less than bachelor’s degree), while another recalled, “I have been told [by a health care provider] I should get the HPV shot. However, I refused because I never thought of a reason to get it. I am sexually active but only with one person.” (20s, Asian or mixed race/ethnicity, less than bachelor’s degree).
Other participants reasoned that possible monetary costs associated with vaccination outweighed any vaccination benefits for men currently in monogamous relationships. As one participant emphasized, “Why would I justify the full price of [the HPV vaccine] if I’m in a committed relationship? [I’m] not having sex with randoms” (30s, non-Hispanic White, less than bachelor’s degree). Although a few monogamously coupled participants acknowledged that they would consider HPV vaccination because the long-term stability of relationships are unknown, most didn’t foresee a possibility of ever having future sexual encounters which could lead to HPV transmission. Some participants even suggested that getting vaccinated would erode trust within existing monogamous relationships. For example, one participant explained: “it could be construed as wanting to protect yourself if you are stepping out [cheating] on your partner” (20s, non-Hispanic White, less than bachelor’s degree).
Concerns About HPV Vaccine Side Effects and Safety
Concerns about HPV vaccine side effects and safety were raised by several participants. Some reported they had heard HPV vaccines had more serious side effects compared with other vaccines, or noted they considered HPV vaccination to be “new” with an unknown long-term safety profile. As one participant shared: “We don’t know how many years it will take for these side effects to emerge. It can cause long-term side effects to some of the people” (20s, non-Hispanic Black, less than bachelor’s degree). Multiple participants noted specific concerns about HPV vaccination causing sterility, impotence, or damage to the health of any future children, for example: “Has it been out long enough to know long-term side effects such as sterility or impotence, or any links to birth defects?” (30s, Asian or mixed race/ethnicity, graduate/professional degree). To alleviate these concerns, participants expressed a desire to hear about the experiences of men who had been vaccinated against HPV in adulthood and/or see concrete statistical data on the safety profile of HPV vaccination among men in their age group.
Health Care Providers as Trusted Sources of HPV Vaccine Information
Several participants noted that they considered their health care providers to be trusted sources of HPV vaccine information. For example, one participant shared: “I trust my doctor and his group to tell me what I should know” (30s, Asian or mixed race/ethnicity, bachelor’s degree). After learning HPV vaccination is recommended for everyone up to age 26, and approved for adults up to age 45, many participants expressed surprise that HPV vaccination had never been recommended to them. Some even reported plans to follow-up with their health care providers. As one participant stated, “This chat will be enough for me to seek out information and bring it up with my PCP [primary care provider]” (20s, Asian or mixed race/ethnicity, bachelor’s degree). Some participants also emphasized the significant impact that a health provider recommendation would have on their HPV vaccine decision-making, for example: “a doctor’s recommendation would be very influential in my decision of getting the vaccine” (30s, Asian or mixed race/ethnicity, graduate/professional degree).
Discussion
To our knowledge, this is one of the first qualitative studies to examine U.S. mid-adult men’s KABs about HPV and HPV vaccination since vaccine eligibility was expanded to include 27- to 45-year-olds in 2018. In doing so, it contributes to better understanding factors that contribute to suboptimal rates of HPV vaccination among men and highlights four key areas for intervention to promote shared clinical decision-making about HPV vaccination between men and their health care providers.
First, despite having been recommended for males since 2011 (CDC, 2011) and approved for men up to age 45 since 2018 (Meites et al., 2019), men in this study had low knowledge and awareness about HPV vaccination and perceived HPV to be a “women’s only” disease. Most men were unaware that HPV vaccination can prevent oropharyngeal, anal, and penile cancers, which contributed to low perceived vaccine utility. Most men were also unaware that they may be candidates for shared clinical decision-making about HPV vaccination with health care providers. These findings echo quantitative studies of U.S. adults published following the FDA approval of HPV vaccines for 27- to 45-year-olds that reported low awareness about the expanded age eligibility (Alber et al., 2021; Fokom Domgue et al., 2020) and limited knowledge of HPV-related cancers that affect men (Thompson et al., 2020).
Several health theories suggest individuals are more likely to adopt a behavior when an issue is salient to them or they perceive themselves to be susceptible (Montano & Kasprzyk, 2015). Hence, our findings further suggest there is a critical need for reliable information targeted at mid-adult men that highlights their vulnerability to HPV and eligibility for shared clinical decision-making about HPV vaccination. Specific questions identified by men in our study regarding HPV transmission, etiology, and testing, as well as HPV vaccine eligibility, safety, and access highlight key knowledge gaps that are salient for inclusion in HPV information resources. Distribution of information at points of health care access is likely critical for reaching men at an opportune time for engaging in shared clinical decision-making with their health care providers (Bridges et al., 2015), Distribution of information on social media, health websites, and via pharmaceutical advertisements may also be useful for reaching men in spaces where they are already accustomed to receiving information about HPV vaccination.
Second, despite being approved by the FDA in 2006 and established as safe for men aged 27 to 45 (Giuliano et al., 2015; Maldonado et al., 2022), our participants perceived HPV vaccines to be “new” and were concerned about nonspecific long-term side effects and negative impacts on their reproductive capacity. Similar concerns about “newness” and safety have been identified in quantitative studies of adults regarding HPV and relatively newer COVID-19 vaccines (Momplaisir et al., 2021; Muthukrishnan et al., 2022). A study of KABs among women aged 27 to 45 conducted after FDA approval of HPV vaccination for this age group demonstrated women share similar concerns about the impact of HPV vaccination on their reproductive capacity (Polonijo et al., 2022). These concerns are indicative of significant barriers to shared clinical decision-making which should be directly addressed in targeted interventions.
Third, embarrassment and stigma surrounding vaccination against a sexually transmitted infection combined with beliefs that practicing “safer sex” and monogamy are preferable means of HPV prevention were additional barriers to shared clinical decision-making about HPV vaccination identified by the men in our study. Concerns about stigma identified in our sample corroborate research suggesting social norms are influential for shaping adults’ HPV vaccine uptake decisions (Alber et al., 2021), while anticipated embarrassment and stigma have been identified as barriers to HPV vaccination among younger adults (Dibble et al., 2019) and newly eligible mid-adult women (Polonijo et al., 2022). Studies of other population groups have also reported that monogamously coupled individuals perceive lower levels of HPV-related threat which deters vaccination (Muthukrishnan et al., 2022; Thompson et al., 2017, 2019; Waters et al., 2021; Wheldon et al., 2018). Combined with our finding that friends and family were primary sources about HPV vaccination for men, our study suggests changing broader social norms surrounding HPV vaccination may be an important target for interventions that aim to promote shared clinical decision-making between men and their health care providers.
Fourth, despite being preferred sources of HPV vaccine information among the men in our study, most participants had never discussed HPV vaccination with a health care provider. Given that more than a decade of research finds health care provider recommendation is the key driver of HPV vaccine uptake (Alber et al., 2021; Fokom Domgue et al., 2020; Gilkey & McRee, 2016; Polonijo & Carpiano, 2013), clinical encounters are a missed opportunity for HPV vaccine promotion among unvaccinated adult men. Coupled with previous research on HPV vaccination suggesting (1) health care provider recommendations tend to be less frequent and of lower quality when the patient is male (Gilkey & McRee, 2016) and (2) many U.S. physicians are unaware of the new shared clinical decision-making guidance for 27- to 45-year-olds (Hurley et al., 2021), our findings underscore the importance of HPV vaccine promotion interventions aimed at health care providers. Clear decision-making tools that assist health care providers in identifying male patients that may benefit from HPV vaccination after age 26 are critical, given low levels of knowledge and awareness among mid-adult men limit their ability to initiate shared clinical decision-making conversations themselves. As complimentary evidence suggests some racial/ethnic minority patients are less likely to receive routine HPV vaccine recommendations from health care providers (Fenton et al., 2018; Polonijo, 2020; Ylitalo et al., 2013), such guidelines could be leveraged to address these inequities.
Limitations
This study provides nuanced insight into the KABs about HPV and HPV vaccination among men aged 27 to 45. Though the results are regionally specific and not generalizable to the entire United States, findings may be comparable to other racial/ethnically diverse U.S. regions where medical care is scarce. Participants were recruited online and via community health clinics; thus, the study does not represent individuals without Internet connections and/or another or no source of health care. Using text-based virtual focus groups allowed us to engage with a racial/ethnically and socioeconomically diverse sample of men, however we were unable to examine the potentially differing KABs of non-English speakers. Filtering participants with duplicate and foreign GeoIP addresses was necessary for ensuring participants met the study inclusion criteria, however, could have led to the exclusion of some legitimate participants. Though the text-based focus group format solicited shorter and less detailed responses than are typically generated in face-to-face focus groups, previous studies comparing these formats have reported the content and themes produced to be remarkably similar (Campbell et al., 2001; Woodyatt et al., 2016). Finally, during focus group discussions, participants were told HPV vaccination had been approved for adults aged 27 to 45 but were not given an explicit description of ACIP guidance or its underlying rationale. Hence, it is possible that some participants assumed HPV vaccination was universally recommended for their age group, affecting their responses.
Conclusion
Understanding mid-adult men’s KABs about HPV and HPV vaccination is critical for informing interventions to promote equitable shared clinical decision-making with health care providers. Men aged 27 to 45 may be receptive to HPV vaccination yet have unanswered questions about the vaccine and the HPV virus, lack knowledge about the utility of HPV vaccination, and be unaware of their own vaccine eligibility. Concerns about HPV vaccine side effects and safety, embarrassment and stigma, and beliefs that safer sex and monogamy are sufficient for HPV prevention serve as additional barriers to men’s HPV vaccine uptake. Interventions aimed at improving mid-adult men’s knowledge, changing social norms surrounding HPV and HPV vaccination, and supporting health providers to identify eligible patients may be especially fruitful for promoting HPV vaccination among men who may still benefit from vaccination after age 26.
Footnotes
Acknowledgements
The authors thank Durga Mahapatra for assistance with data collection and Christina Reaves, Michelle C. Burroughs, Shaleta Sultan-Smith, and Carla Urmeneta for assistance with study recruitment and administration.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a Community Medicine and Population Health Mini-Grant from the Center for Healthy Communities at the University of California, Riverside School of Medicine and the Riverside Community Health Foundation (2020). The funders had no involvement in study design; data collection, analysis, and interpretation; or writing and submission of the article.