
Abstract
Awareness of risk for oropharyngeal cancer from oral human papillomavirus (HPV) infection is low among men in the United States. This pilot study tested messages communicating oral HPV and oropharyngeal cancer risk among a sample of U.S. young adult men (aged 18–26). Six oral HPV and cancer risk messages were tested in an online survey. Participants (N = 68) were randomly assigned to one of two message sets, each containing three unique text-based messages. Participants evaluated messages separately based on various measures (e.g., perceived message effectiveness [PME], novelty). One-way repeated measures ANOVAs were used to assess evaluation differences within message sets. Participants provided open-ended feedback about each message, which were synthesized into overarching themes. Participants were receptive to the risk messages, rating them high on PME (mean range = 3.72–4.25 out of 5) and other measures. Analyses identified three high-performing messages. For example, participants rated a message about HPV-linked oropharyngeal cancer risk rates in men versus women higher on attention and novelty than two other messages in the same set (both ps < .05). Participants were shown three messages (instead of all six) in each message set to minimize survey fatigue. Common themes from open-ended feedback were that participants liked the short-form structure of the messages and that the messages used gender-tailored language. In conclusion, oral HPV and oropharyngeal cancer risk messages may be useful for increasing risk awareness among men in the U.S. Further work should test such messages in rigorous experimental contexts to assess their efficacy in modifying other health outcomes, such as HPV vaccination behaviors.
Introduction
Compared to women, men in the United States (U.S.) have low awareness about their eligibility for the human papillomavirus (HPV) vaccine (Laserson et al., 2020) and are less likely to be vaccinated against HPV (Zou et al., 2022). National data from 2013 to 2018 show that only 27% of young adult men (ages 18–26 years) have received at least one dose of the HPV vaccine (Boersma & Black, 2020). This low uptake is problematic given that men are at high risk of contracting oral HPV and developing HPV-linked oropharyngeal cancer (e.g., mouth and throat cancer) (Morand et al., 2022). Research is needed to identify effective ways to communicate about the risks of oral HPV and oropharyngeal cancer to this population.
Low perceived risk of HPV may be hindering vaccine uptake among young adult men. One review described college-aged men to underestimate their risk of contracting HPV and inaccurately believe the virus only affects women (Laserson et al., 2020). Findings from a qualitative study reported that unvaccinated adult men typically perceive HPV infection as a disease that only affects women and are unaware the HPV vaccine can also prevent cancers in men (Alaraj et al., 2023). The men in this study expressed concerns about getting the HPV vaccine, including concerns about vaccine safety and potential side effects. Low awareness of the HPV vaccine (Brewer et al., 2007)—combined with perceptions that HPV does not affect them—presents an opportunity to educate this population with public health campaigns and interventions aimed at increasing awareness and subsequent vaccination behaviors.
HPV messages framed in the context of cancer prevention could be an effective way to educate young adult men and increase their perceived risk for HPV. Similar strategies have been effective for motivating young adult women and parents of adolescent girls to get the vaccine (Pathak et al., 2022). For example, a cervical cancer communication campaign for college women reported that messages designed to increase awareness of susceptibility of HPV and acceptability of the HPV vaccine influenced participants’ self-reported vaccination likelihood (Sundstrom et al., 2018). In addition, Lyson et al. (2019) used Twitter to test the influence of HPV and cervical cancer prevention messages on women’s HPV awareness and knowledge. Findings indicated that brief, tailored messages on social media increased HPV awareness among their study sample.
There is a dearth of work testing HPV and cancer messages among men to increase vaccination. One study by Nan (2012) tested the effectiveness of an HPV informational pamphlet about genital HPV infection in increasing vaccination intentions in a sample of college-aged men and women and reported that vaccination intentions were associated with both message framing (i.e., gain vs. loss) and participants’ motivational orientation. Overall, men in this study were less likely than women to engage in any type of HPV prevention, including vaccination, suggesting they may be less influenced by HPV risk messaging. However, this study did not assess messages linking oral HPV and oropharyngeal cancer.
Another experiment by McRee et al. (2010) tested different HPV-related message vignettes among a sample of men in the U.S. (ages 18–59 years). Results identified that vignettes communicating risk of genital warts and HPV-linked cancer (e.g., anal and oral) increased vaccination willingness compared with vignettes only communicating risk of genital warts. Notably, this study only examined HPV-linked cancer risk messages mentioning genital warts. Thus, it is unclear whether HPV-linked cancer messages without the mention of other health issues are effective among young adult men.
The current pilot study sought to address gaps in HPV communication research by testing health messages about oral HPV-linked oropharyngeal cancer risk among a sample of young adult men. Each message was two sentences, used plain language, and contained information, including statistics, on the incidence and effects of oral HPV and oropharyngeal cancer among men (Centers for Disease Control and Prevention, 2022; Chaturvedi et al., 2019). In addition, the structure of the messages was informed by fuzzy trace theory (Blalock & Reyna, 2016; Reyna, 2012), which suggests that people are more likely to retain the gist, or general meaning, of health information rather than exact numbers or phrases in a message. The goal of this work is to identify potential messages and themes that can be used in campaigns targeting this at-risk population.
Methods
Oral HPV and Cancer Messages
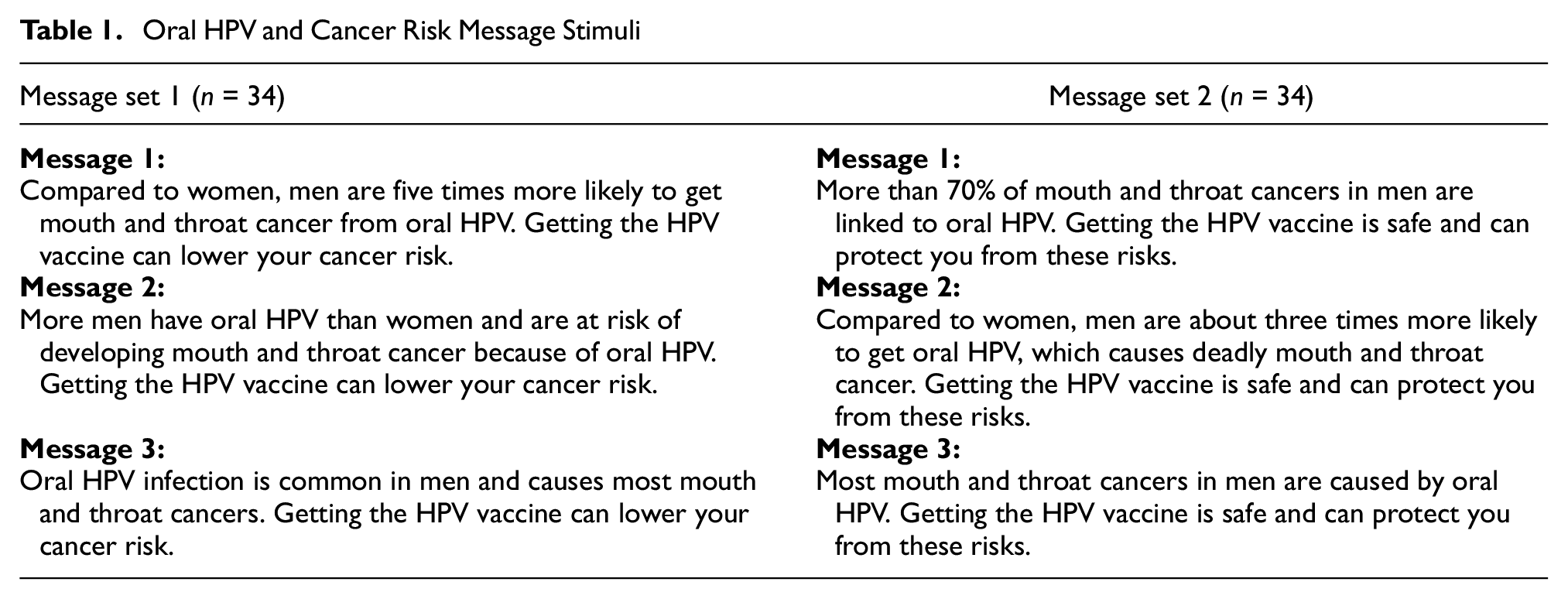
We developed and evaluated six unique oral HPV and oropharyngeal cancer messages in the current pilot study. These messages were designed to increase awareness of the link between oral HPV and oropharyngeal cancer in men and motivate this population to get vaccinated against HPV. Each message was structured in two sentences. The first sentence provided educational information about oral HPV and cancer risk and was specific to a male audience. The second sentence promoted the efficacy and health benefits of getting the HPV vaccine. Based on social comparison theory, which predicts individuals will appraise health risks in comparison to other relevant groups (Festinger, 1954; Tennen et al., 2000), one message was “Compared to women, men are five times more likely to get mouth and throat cancer from oral HPV. Getting the HPV vaccine can lower your cancer risk.” See Table 1 for a full list of messages.
Oral HPV and Cancer Risk Message Stimuli
Message content, was informed by evidence on the incidence and effects of oral HPV and cancer among men (Centers for Disease Control and Prevention, 2022; Chaturvedi et al., 2019). In addition, framing of the messages was, in part, informed by fuzzy trace theory about disease risk and vaccination communication (Blalock & Reyna, 2016; Reyna, 2012). This theory suggests people encode gist (general meaning) and verbatim (exact numbers/phrases) representations after exposure to a message communicating risk. The two-part message format encouraged gist encoding such that participants could read the short message and easily understand there is a general harm linking oral HPV and oropharyngeal cancer in men. The second sentence in each message communicated that there is a way to easily avoid this cancer risk through vaccination. Fuzzy trace theory suggests that gist encoding may lead to the adoption of positive health behaviors, such as getting vaccinated (Blalock & Reyna, 2016).
Participants and Procedure
This message testing study was exploratory and intended to inform a larger experimental investigation. As such, a modest sample size (N = 70) of participants were enrolled from Prolific, a recruitment platform for online research, and recruitment took place in March 2023. Inclusion criteria were that participants self-identified as male, lived in the U.S. and were ages 18–26 (years). We excluded two participants due to incomplete age data (provided by Prolific), resulting in a final analytic sample of N = 68.
After being pre-screened and meeting inclusion criteria, participants were redirected to the online survey platform Qualtrics to begin the study. Participants first provided informed consent and answered questions about general HPV knowledge and HPV vaccine awareness. Next, participants were randomized to one of two message set conditions (n = 34 each). Conditions exposed participants to three unique messages about oral HPV and cancer risk, one at a time and in random order. We chose to show participants three messages (instead of all six) in each message set group to minimize survey fatigue. Participants answered a series of message-specific (after each exposure) and aggregate (after all message exposures) message evaluation items. This study was deemed as exempt human subjects research by the National Institutes of Health Institutional Review Board (approval no. 001588). All participants provided informed consent prior to enrollment in the study.
Measures
Demographics and HPV Knowledge
We report participant age and race based on demographic data provided by Prolific. Since previous research has documented low HPV knowledge and awareness among young adult men (Giannone et al., 2022; Laserson et al., 2020), we assessed this among our sample with five questions. First, participants were asked if they had ever heard of HPV (yes/no) and if they had ever heard of the HPV vaccine (yes/no). Participants were then asked who should receive the HPV vaccine, with response options including “boys ages 11 or 12,” “girls ages 11 or 12,” “males ages 9 through 26,” “females ages 9 through 26,” or “males and females ages 9 through 26” (correct response). Participants could also indicate that they did not know. Next, participants were asked who HPV affected, with response options being “only women,” “only men,” or “both women and men” (correct response). Participants could also indicate that they did not know or could choose an “other” response option. Finally, we asked participants to select ways that HPV was spread (all that apply). Example response options to this question included “handshakes” and “bathroom floors.” Correct responses were “oral sex,” “open-mouth kissing,” and “sexual intercourse.” All HPV knowledge questions were adapted from previous literature (Williams et al., 2015).
Perceived Message Effectiveness (PME)
A brief composite measure, informed by previous literature (Noar et al., 2018), was created to assess PME. The measure began with the stem, “How much does this message make you. . .” and included the following three items: (a) believe getting the HPV vaccine will protect you, (b) think getting the HPV vaccine is a good idea, and (c) want to get the HPV vaccine. PME items were assessed on a 5-point scale ranging from “not at all” (1) to “a great deal” (5). Reliability of the measure across messages was acceptable ([Cronbach’s coefficient] α = .82–.90).
Message-Related Attitudes
Message-related attitudes were assessed using a three-item scale developed for this study. The scale began with the prompt, “This message is . . .” Responses to attitude items were on 5-point bipolar scales. Response anchors were (a) not helpful–helpful, (b) not informative–informative, and (c) not useful–useful. Reliability of the measure across messages and message conditions was acceptable (α = .90–.94).
Additional Message-Specific Evaluation Items
After each message exposure, message-related attention (“How attention grabbing is this message?”) and believability (“How believable is this message?”) were assessed. These items were assessed on a 5-point scale ranging from “not at all” (1) to “a great deal” (5). Message-related novelty was measured by asking participants to respond to the statement, “I learned something new from this message.” Responses to message novelty were on a 5-point scale ranging from “strongly disagree” (1) to “strongly agree” (5). Considering previous research shows potential for interpersonal effects of health messages to influence behavior (Hendriks et al., 2014), we also asked participants how likely they were to share each message with their friends, family members, and health care providers (assessed separately), with response options on a 5-point scale ranging from “not at all” (1) to “a great deal” (5). Participants also had the option to select “not applicable” for the message sharing items. Finally, participants were asked to separately respond in open-ended format what they liked and what could be improved about each message.
Aggregate Message Evaluation Items
Participants were asked three aggregate message evaluation items (designed for this study) after exposure to all three within-group messages. Each item began with the stem, “Which of these statements. . .” and included the following items: (a) makes you most worried about the chances of getting cancer from oral HPV, (b) is most believable, and (c) makes you want to get the HPV vaccine the most? In response to these items, participants were asked to choose one of the three messages they were exposed to; only the first sentences of each message were used as response options as the second sentence of each message was the same. Responses were mutually exclusive, meaning participants could only select one of the three messages as an answer for each aggregate evaluation item.
Data Analysis
Descriptive statistics were used to characterize participant demographics and their responses to HPV knowledge questions. One-way, repeated measures ANOVAs were used to assess message evaluation differences within message sets (e.g., assessing PME differences among Messages 1 to 3 in Message Set 1). We chose to use nonparametric analyses (i.e., Friedman rank-sum tests) for these ANOVAs to account for the low sample sizes in the message set conditions (both n = 34) and nonnormally distributed data. We computed post hoc analyses on these comparisons using Wilcoxon tests and applied a Bonferroni p-value adjustment. Finally, we used frequencies and proportions to assess and visualize participants’ responses to the aggregate message evaluation items. These analyses were computed using R (version 4.2.2).
We used an inductive coding approach to examine the open-ended message feedback (Tracy, 2019). Responses were read multiple times and we created thematic codes reflecting what participants liked and what they thought could be improved about each message. Codes and themes were agreed on by the research team. Analyses were conducted using NVivo.
Results
Participants Characteristics and Prior HPV Knowledge
Mean age (in years) of participants was 22.84 (SD = 2.47). Participants identified as white (n = 39; 57%), Black or African American (n = 8; 12%), Asian (n = 8; 12%), more than one race (n = 8; 12%), or some other race (n = 5; 7%). Most participants (n = 59; 87%) had heard of HPV prior to this survey, but less than half (n = 32; 47%) had ever heard about a vaccine for HPV. Only about one-third (n = 21; 30%) of participants correctly knew that men and women ages 9–26 were eligible for the HPV vaccine. Finally, most participants (n = 50; 74%) correctly knew that HPV affected both men and women, but only 19% (n = 13) selected each of the correct responses about how HPV was spread (i.e., via oral sex, open-mouth kissing, or sexual intercourse).
Individual and Aggregate Evaluations of the HPV Messages
Within-group message evaluations are in Table 2 and aggregate message evaluation results are in Figure 1. We report differences for the two message sets separately (n = 34 for each message set).
Evaluations of the HPV Messages Grouped by Message Set

Note. Mean values with different subscripts in the same row are significantly different at p < .05 by pairwise comparison, nonparametric post hoc tests with Bonferroni correction.
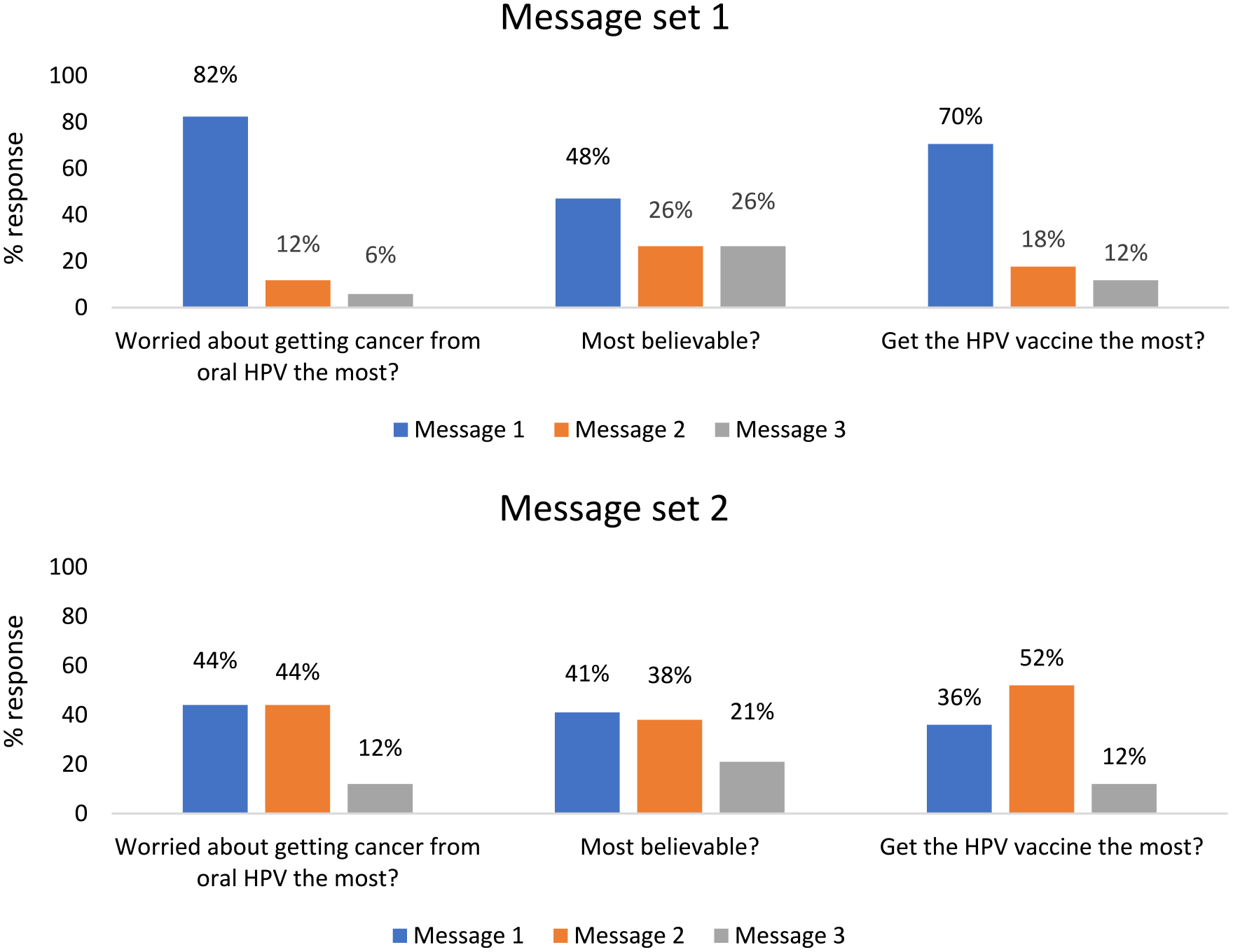
Aggregate HPV Message Evaluations Grouped by Message Set
Participants randomized to message set 1 evaluated the following three message statements: Message 1 compared with women, men are five times more likely to get mouth and throat cancer from oral HPV; Message 2 more men have oral HPV than women and are at risk of developing mouth and throat cancer because of oral HPV; and Message 3 oral HPV infection is common in men and causes most mouth and throat cancers. Participants rated the messages differently on attention ((Friedman) χ2 = 9.64, p = .008), with post hoc comparisons indicating that Message 1 was rated higher on attention than both Message 2 ((Wilcoxon) W = 221, p = .004) and Message 3 (W = 255, p = .026). Messages were also rated differently on novelty (χ2 = 9.49, p = .009), with comparisons indicating novelty was higher for Message 1 than Message 2 (W = 132, p = .020), but not Message 3. Furthermore, likelihood of sharing message content with family differed across messages (χ2 = 7.48, p = .024), with comparisons indicating Message 1 was more likely to be shared with family than Message 3 (W = 102, p = .04), but not Message 2. Messages 2 and 3 were rated similarly across all evaluation items. Finally, Message 1 was the most selected statement for all three aggregate message evaluation items (most worried about getting cancer from HPV: 82% [n = 28]; most believable: 48% [n = 16]; and most likely to get the HPV vaccine: 70% [n = 24]).
Participants randomized to Message set 2 evaluated the following three message statements—Message 1: more than 70% of mouth and throat cancers in men are linked to oral HPV; Message 2: compared with women, men are about three times more likely to get oral HPV, which causes deadly mouth and throat cancer; and Message 3: most mouth and throat cancers in men are caused by oral HPV. Participants rated the messages differently on PME (χ2 = 14.2, p < .001), with post hoc comparisons indicating PME was higher for Message 1 (W = 210, p = .003) and Message 2 (W = 222, p = .006) than Message 3. Ratings on attention also differed across messages (χ2 = 13.8, p < .001), with comparisons indicating attention was higher for Message 1 (W = 207, p = .003) and Message 2 (W = 141, p = .04) than Message 3. Participants rated the messages differently on attitudes (χ2 = 17, p < .001), with comparisons indicating attitudes was higher for Message 1 (W = 200, p = .011) and Message 2 (W = 178, p = .019) than Message 3. Furthermore, message ratings differed in terms of novelty (χ2 = 11.5, p = .003), with comparisons indicating novelty was higher for Message 1 (W = 104, p = .034) and Message 2 (W = 104, p = .036) than Message 3. Messages 1 and 2 were rated similarly across all evaluation items. In addition, Messages 1 or 2 were the most selected statements for the three aggregate evaluation items (most worried about getting cancer from HPV: 88% [n = 30]; most believable: 79% [n = 27]; and most likely to get the HPV vaccine: 88% [n = 30]).
Open-Ended Feedback About the HPV Messages
Common findings and illustrative quotes from participants’ open-ended feedback about the messages are in Table 3. Over one-third of participants (n = 24; 35%) liked that messages were short, to the point, and had clear language. About half (n = 30; 44%) noted the importance of numbers and statistics in the messages. For example, one participant mentioned, “I liked the part about how men are 5 times more likely to get cancer from HPV, because it causes a lot more concern.” About half of participants (n = 32; 47%) also emphasized that messages tailored to their gender were attention grabbing and persuasive. For example, one participant stated, “As a man I feel a greater need to get the vaccine to protect myself.”
Open-Ended Feedback About the HPV Messages

Participants also provided feedback about how to improve the messages. For example, about one-third (n = 24; 35%) wanted more statistics or numbers added to the messages. In addition, one-quarter (n = 17; 25%) of participants stressed that they would like more detail on HPV and the HPV vaccine in the messages, with one participant noting “[the message] needs statistics on how much the vaccine has lowered the HPV infection rate.” Finally, a small number of participants (n = 6; 9%) suggested adding sources to validate the message content (e.g., “According to the CDC . . .”).
Discussion
This pilot study assessed HPV and vaccine knowledge and awareness among a sample of young adult men in the U.S., as well as perceptions of risk messages communicating the link between oral HPV and oropharyngeal cancer. Broadly, results showed low awareness of both the HPV vaccine and knowledge that young adult men are eligible to receive the vaccine. Findings also indicated some oral HPV and oropharyngeal cancer risk messages were evaluated more favorably than others by our study sample. Together, these findings speak to the need for additional oral HPV prevention initiatives targeting men in the U.S. and suggest that certain prevention messaging strategies, such as gender-framed messages, may be perceived as effective when communicating oral HPV-related cancer risk to this audience.
Overall, participants were receptive to messages about HPV-linked oropharyngeal cancer. Across both message sets, PME and message-related attitude scores were high, indicating message receptivity. Messages containing either a relative cancer risk or relative HPV risk statistic (e.g., “Compared to women, men are about three times more likely to get oral HPV, which causes deadly mouth and throat cancer.”) were perceived as attention grabbing and provided participants with novel information. Paired with the sample’s low awareness about their risk for contracting HPV, these results add to previous literature (Alaraj et al., 2023; Giannone et al., 2022; Laserson et al., 2020) suggesting messages communicating HPV-related cancer risk to men should likely use language aimed at increasing their perceived risk relevance of HPV and cancer.
Similar to prior risk communication research (Calo et al., 2018; Lama et al., 2022), findings from participants’ open-ended feedback about the study messages supports the use of short, clear, and plain language messages when conveying risk about HPV. In addition, several participants in this pilot study suggested including additional information about HPV and the HPV vaccine in the messages (e.g., how the virus spreads and vaccine efficacy statistics), and some even recommended that the messages include attributable sources (e.g., “According to the CDC”) to validate message credibility. These findings suggest that young adult men in the U.S. may be open to learning about this health issue from trusted sources, which is critical given that HPV-related mis-and disinformation content often circulates on social media (Kornides et al., 2023; Massey et al., 2020; Oh et al., 2023). Drawing from this feedback, future health efforts tailored to young adult men should likely use multiple strategies (beyond short messages) to educate this population about their risk for oral HPV.
Notably, the six oral HPV and oropharyngeal cancer messages pretested in this study were partially informed by fuzzy trace theory, which acknowledges that people have a limited capacity for information and typically encode the general meaning or gist of risk messages better than verbatim content (Blalock & Reyna, 2016; Reyna, 2012). The messages were designed to convey a general link between oral HPV and cancer to men, while also communicating there is an easy way to prevent this risk through vaccination. The specific statistics we used were intended to facilitate gist encoding (e.g., “five times at risk” → “I am at high risk”). Given participants’ favorable evaluations of the study messages overall, our findings lend some preliminary support for the use of gist messaging when communicating HPV risk to young adult men. Although, more work explicitly testing verbatim vs. gist messages in similar study contexts is still needed.
Finally, a surprising finding among our sample was participants’ low message sharing scores. Regardless of relationship type (i.e., friend, family member, health care provider), participants did not seem willing to share the HPV messages. These findings suggest this sample of young adult men may be reluctant to talk about HPV with others. Regardless, additional research should investigate ways to increase willingness to communicate about HPV risk with peers.
Strengths of this study include pretesting several theory-informed oral HPV and oropharyngeal cancer risk messages using language tailored to young adult men, and the use of multiple message evaluation items to assess message receptivity and perceived effectiveness. A limitation of this study was its modest sample size, which may have hindered our statistical power to detect differences in message evaluations within message set groups. Another limitation is that we recruited participants using a convenience sampling method through Prolific. Future studies should consider testing similar messages in different experimental contexts (such as including a control message group) with a large and representative sample. In addition, experiments should examine message exposure effects on key HPV prevention outcomes such as HPV-related risk beliefs and vaccination behavior. Finally, more qualitative research on this topic, such as focus groups or interviews, could add to our understanding of how young adult men perceive HPV-linked oropharyngeal cancer risk messages.
Conclusion
Risk of oral HPV is high in men and can lead to harmful consequences such as oropharyngeal cancer. Among our pilot study sample, we found that young adult men were receptive to risk messages about oral HPV-linked oropharyngeal cancer—particularly messages mentioning their relative risk of contracting oral HPV compared to women. Given low overall HPV vaccination rates and poor awareness of oral HPV infection risk among men in the U.S., it is critical research continues to develop and test messages aimed at increasing HPV-related knowledge and risk beliefs among this population to ultimately affect vaccination outcomes.
Footnotes
Disclaimer
The opinions expressed by the authors are their own and this material should not be interpreted as representing the official viewpoint of the U.S. Department of Health and Human Services, the National Institutes of Health or the National Cancer Institute.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded through an internal National Cancer Institute Division of Cancer Control and Population Sciences Collaborative Research Award for Fellows in Training (CRAFT).