
Abstract
Paternal postnatal depression (PPND) is not a commonly recognized phenomenon. The aim of the study was to identify the Edinburgh Postnatal Depression Scale (EPDS) cutoff for Saudi fathers, to estimate PPND prevalence and to determine the risk factors of PPND among fathers of newborn in Saudi Arabia. A cross-sectional study of fathers with babies born up to 6 months prior to the survey was conducted. Fathers were screened using EPDS and demographic questionnaire. The fathers were selected using systematic random sampling from visitors to the birth registration office. A subsample of participants from the postnatal wards in a tertiary care was invited for additional evaluation by a psychologist using the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria for major depressive disorders. Receiver operating characteristic curve was utilized to identify fathers with depression; a cutoff of 8/9 was optimal to achieve sensitivity 77.8% and specificity 81.3%. Adjusted prevalence of PPND was reported with corresponding Wilson 95% confidence interval. Two hundred and ninety fathers completed the EPDS and demographic questionnaire. Of 72 invited participants, 57 (79.16%) attended the diagnostic interview. The average age of fathers was 34.97 ± 8.56 years, the average maternal age was 29.18 ± 7.41 years, average age of the newborn was 43.13 ± 35.88 days. PPND adjusted prevalence was 16.6% (95% CI [8.5, 25.6]). Paternal mental health needs equal attention during and postdelivery of newborn. Fathers should receive perinatal and postnatal mental health assessment to prevent behavioral problems in their children and disruption of relationship with their spouse.
Keywords
Depression is a leading contributor to global disease burden: over 300 million people worldwide were estimated to suffer from the condition in 2015 (World Health Organization, 2017). The prevalence of depression in the United States has doubled between 2005 and 2015 (Weinberger et al., 2018). Despite a plethora of available treatments, depression continues to be a burden because of the low detection rate. Detection is even more challenging in unsuspected groups, such as men, due to the stigma attached to the condition by society. Men suppress their feelings and are less likely to acknowledge depression. Men can exhibit symptoms that are less characteristic of depression, including irritability, anger, and aggression (O’Hara & McCabe, 2013). Research on parental mental health after childbirth focuses mainly on the adjustment of women during the transition to parenthood (Edward, Castle, Mills, Davis, & Casey, 2015).
Postpartum depression (PPD) is defined as “a non-psychotic depressive episode of mild to moderate severity, beginning in or extending into the first postnatal year” (Miller, 2002). PPD among women has been thoroughly investigated by researchers for over 50 years (Brockington, 2004). Conversely, depression among the fathers of newborn, termed paternal postnatal depression (PPND) or “sad dads,” is a phenomenon recognized infrequently, is underscreened and underdiagnosed (Brockington, 2004; Musser, Ahmed, Foli, & Coddington, 2013). The concept of PPND came to the fore in 1990 (Brockington, 2004), and has gained significant attention in recent years (Condon, Corkindale, & Boyce, 2004).
To date, two reviews had reported the estimated rate of depression among fathers of newborn. A meta-analysis in 2010 has reported PPND estimated rate as 10% (95% CI [8.5%, 12.7%]) with a mix of studies reporting depression rates at single versus two or more time points during the antenatal/postpartum period (Paulson & Bazemore, 2010). A more recent meta-analysis in 2016 reported the estimated rate of PPND 8.4% (95% CI [7.2%, 9,6%]; Cameron, Sedov, & Tomfohr-Madsen, 2016). Studies have shown that PPND estimated prevalence tends to decline with time during the postpartum period (Goodman, 2004). Prevalence of PPD among both partners has been reported as 19.6% at 4 weeks postpartum, which decreased to 4.7% at 8 weeks postpartum (Paulson & Bazemore, 2010).
In spite of a series of studies conducted throughout Europe and the East between 2001 and 2015 to validate a screening tool for fathers of newborn (Edmondson, Psychogiou, Vlachos, Netsi, & Ramchandani, 2010; Lai, Tang, Lee, Yip, & Chung, 2010; Loscalzo, Giannini, Contena, Gori, & Benvenuti, 2015; Massoudi, Hwang, & Wickberg, 2013; Matthey, Barnett, Kavanagh, & Howie, 2001; Tran, Tran, & Fisher, 2012), a recent insight considered only the mothers of newborn at high risk of developing depression (Reynolds & Patel, 2017).
Several risk factors have been associated with PPND, such as unemployment, unplanned pregnancy, poor marital relationship, poor social support, lack of family support, previous history of depression, presence of depression during antenatal period, maternal depression, joint family versus nuclear family (Condon et al., 2004; Nishimura & Ohashi, 2010; Paulson & Bazemore, 2010). Studies have reported an association between PPND and the development of emotional and behavioral psychiatric disorders among their children (Pinheiro et al., 2006; Ramchandani et al., 2008). PPND needs to be recognized as a serious public health issue. It is deemed necessary to identify fathers with PPND in order to prevent developing childhood emotional and behavioral problems (Ramchandani, Stein, Evans, & O’Connor, 2005) .
The reported percent of total years lived with disability (YLD) in Saudi Arabia is 9.5% due to depression (World Health Organization, 2017). The prevalence of maternal postpartum depression (MPPD) among Saudi women is 14% (Al-Modayfer, Alatiq, Khair, & Abdelkawi, 2015) compared to internationally reported figures of 4.5%–20% (O’Hara & McCabe, 2013). However, PPND among fathers of a newborn baby is relatively a new concept in Middle East and Saudi Arabia. A study conducetd in an Arab country; Egypt, had reported 31.8% prevalence of depression in expecting fathers (Moussa et al., 2012) compared to reported 13.3% estimated rate in Canada among first-time expecting fathers (Da Costa et al., 2017). To our knowledge, there is no current estimate for the prevalence of PPND in Saudi Arabia. Furthermore, estimates provided from other published studies might have limited generalizability to the Saudi population due to the difference in cultural and social values.
The shifting of home responsibilities, with an increase in working women and greater involvement of fathers in childcare, puts men at increased risk of developing depression. Fathers of a newborn baby also experience changes in life, like mothers (Kim & Swain, 2007). Simultaneously, men are approximately 50% less likely to seek mental health treatment than women (Gonzalez, Alegria, & Prihoda, 2005). The cost on services utilized by fathers diagnosed with PPND was (£1,103.51), higher than those without depression (£945.03; Edoka, Petrou, & Ramchandani, 2011), that emphasizes the need for early detection and treatment of PPND. The current study addresses the limitations of the literature by identifying the Edinburgh Postnatal Depression Scale (EPDS) cutoff for Saudi fathers, to estimate the prevalence of depression among fathers of newborn and to determine the risk factors for PPND.
Methods
Study Design and Participants
This is a cross-sectional study conducted among Saudi fathers with babies born up to 6 months before survey administration during 2016. The study sample included 290 fathers who could read and write. Arabic was the native language of all participants. All participants had filled a self-filled survey that included a validated screening tool (EPDS) for identifying depression and set of questions composed of: demographics (six items), employment-related factors (five items), family-related factors (six items), wife-related factors (four items), pregnancy-related factors (seven items), psychological well-being factors (three items), and social support factors (two items). Out of 290, a subsample of 72 (25%) fathers was invited in a tertiary care center’s postnatal ward for diagnostic interviews by a psychologist. The information obtained from the subsample was used to determine the EPDS optimal score for the Saudi population as well as used to correct for the apparent prevalence obtained from the screening tool.
Participants were selected using systematic sampling based on the rate of visitation from those attending postnatal wards at a tertiary care hospital or the birth registration office in Riyadh, Saudi Arabia (where all fathers are required to visit within 30 days of childbirth to obtain their child’s birth certificate). Participants filling only the demographic and EPDS questionnaire were verbally consented at the introduction of the survey. The questionnaire was distributed by the study team. The completed questionnaires were collected immediately in an envelope to maintain the confidentiality of the responses. Ethical approval was obtained from the King Abdullah International Medical Research Center Institutional Review Board with the approval number (RC13/206/R).
Instrument
The EPDS is a 10-item self-rating scale designed to screen for depression among mothers (Cox, Holden, & Sagovsky, 1987). The EPDS has been demonstrated to be a valid tool to identify depression among fathers (Edmondson et al., 2010; Lai et al., 2010; Loscalzo et al., 2015; Massoudi et al., 2013; Matthey et al., 2001; Tran et al., 2012). The fathers of newborn were screened using an Arabic version of the EPDS translated by Ghubash, Abou-Saleh, and Daradkeh (1997). The scale identifies symptoms over the preceding 7 days. Each item has four possible responses, which are scored from 0 to 3; the total score ranges from 0 to 30. Fathers were excluded if they had a history of psychiatric illness, received medication for the psychiatric illness, if their newborn were older than 6 months, or if they missed out any of the EPDS responses.
Diagnostic Interview
Out of 290 participants, 72 (24.8%) participants who completed the demographic and EPDS questionnaire were immediately invited to participate in the diagnostic interview and undergo evaluation by a psychologist using the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria for major depressive disorders. Fathers who agreed to participate in the diagnostic interview were enrolled after providing written consent. The psychologist was blinded to their EPDS responses. The participants who were identified with major depression by the psychologist were advised to consult their primary care physician for further evaluation and assessment. The DSM-5 scoring system was considered the gold standard.
The potential risk factors of depression among fathers of newborn were identified as demographics, employment related, family support, family set-up (joint vs. nuclear family), social support, pregnancy related, family history of depression, wife having postpartum depression, and psychological well-being (feeling isolated from the partner, whether had received overspeeding ticket postdelivery) correlates.
Statistical Analysis
Quantitative variables, including parents’ age, child’s age, and the number of children living in the house, were summarized and reported in terms of means, standard deviation, median, and interquartile range (IQR). Categorical variables, such as educational level, occupation, income level, family history of psychiatric illness, and information related to pregnancy, spouse, and family, were reported in terms of frequency tables and percentages. All variables were compared between fathers with and without depression using the Chi-square test of independence and Wilcoxon rank sum test. Statistical tests were declared significant at an α-level of less than .05. The cutoff value for the EPDS score was determined using a receiver operating characteristic (ROC) curve. Participants with a total EPDS score of ≥9 were considered to have depression. The prevalence of depression among fathers was estimated by dividing the number of fathers identified as depressed based on an EPDS cutoff of 9 by the total number of fathers in the study. The proportion was then corrected for the estimated sensitivity and specificity of the EPDS tool in the Saudi population. The apparent and adjusted prevalence was reported in terms of point estimate and corresponding Wilson 95% confidence intervals. Logistic regression was used to explore the risk factors for depression. The results were reported as odds ratios, 95% confidence intervals, and p values. Analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA).
Results
Study Sample
A total of 347 fathers were invited to participate in the study. Of them, 57 (16.42%) were excluded because they had missed some EPDS responses or had a history of psychiatric illness. Thus, 290 fathers completed the EPDS survey. A convenient sample of 72 (24.8%) fathers were invited to undergo a structured interview with a psychologist, of whom 57 (79.16%) consented and agreed. The 15 (20.83%) who did not agree to participate in the diagnostic interview were not statistically different (in terms of demographics and other factors) from the 57 (79.17%) who had participated.
Sociodemographic Characteristics
Of the 290 fathers enrolled in the study, the mean reported paternal age was 34.97 (SD = 8.56) years, maternal age was 29.18 (SD = 7.41) years, and the mean reported age of the newborn was 43.13 (SD = 35.88) days (Table 1). Out of 290 reported, 67 (23.04%) were first-time fathers, whereas 184 (63.23%) were experienced fathers. Two hundred and seventy one (93.12%) fathers had one newborn. Sixty-seven (23.02%) fathers were in their twenties, the majority 147 (50.51%) were in their thirties, 44 (15.12%) were in their forties, and 13 (4.46%) were in their fifties or older.
Demographic/Employment-Related Characteristics of Fathers With/Without Depression.
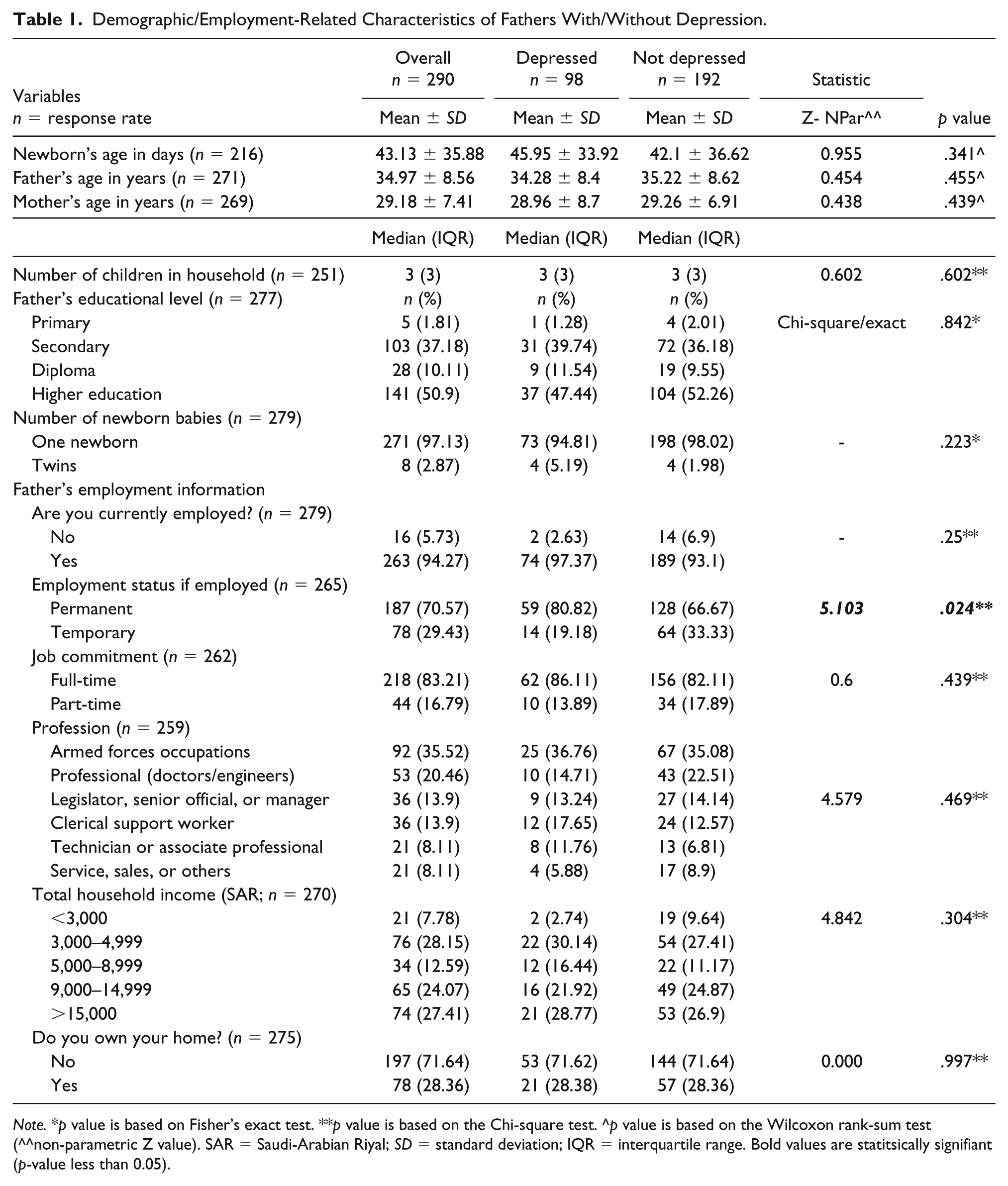
Note. *p value is based on Fisher’s exact test. **p value is based on the Chi-square test. ^p value is based on the Wilcoxon rank-sum test (^^non-parametric Z value). SAR = Saudi-Arabian Riyal; SD = standard deviation; IQR = interquartile range. Bold values are statitsically signifiant (p-value less than 0.05).
One hundred and forty-one (50.9%) fathers reported that they had received higher education. Of 259 fathers who had an occupation, 92 (35.52%) were employed in the armed forces, 53 (20.46%) were professionals (doctors/engineers), 36 (13.9%) were managers, and 36 (13.9%) were clerical support workers, 21 (8.11%) were associate professionals, and 21 (8.11%) were sales professionals. With regard to total income, 74 (27.41%) fathers reported a total monthly income of Saudi-Arabian Riyal (SAR) ≥15,000. The majority of the fathers 263 (94.27%) were employed; 218 (83.2%) had full-time employment, and 187 (70.57%) had a permanent job. Seventy-eight (28.36%) fathers owned their own home. The median number of children living in each household was 3 (IQR = 3). Demographic/employment-related characteristics were not significantly different between fathers with and without depression. However, the employment status, permanent versus temporary, was significantly different between fathers with and without depression (χ2 = 5.103, p = .024; Table 1).
Prevalence of Depression Among Fathers of Newborn
Of the 290 participants, 98 (27.9%; 95% CI [23.1, 33.4]) appeared to be depressed according to the EPDS cutoff score of 8/9. The estimated prevalence was corrected for tool sensitivity (77.8%) and specificity (81.3%), and the final estimated prevalence was reduced to 16.6%, with a 95% confidence limit (Wilson score) of 8.5%–25.6%.
Figure 1 summarizes the unadjusted prevalence at different cutoffs reported in the literature. The prevalence increases or decreases by using the cutoffs determined for other samples.

Apparent prevalence of depression in the study sample at different Edinburgh Postnatal Depression Scale cutoffs based on the literature.
Marital, Wife, Family Support, and Psychological Well being Related Correlates of Depression
Several factors related to marital relationship, family, and social support were examined among the fathers. Most of the fathers, 276 (98.92%), were married and living with their wives. Almost all fathers, 274 (98.56%), reported a good marital relationship, and the majority, 261 (92.55%), had just one wife. Only 25 (9.03%) reported that their wives were depressed. One hundred and fifty-five (55.96%) fathers reported that their wife went to her mother’s house for delivery, whereas 102 (52.31%) fathers reported that their wife was joined by her mother at their home. The family setup was reported as nuclear by 228 (81.14%) of the fathers. Almost all fathers, 280 (99.64%), reported a good relationship with their parents, and 244 (86.83%) received the support of friends. The marital-, wife-, and family-related characteristics were not different between fathers with and without depression.
Twenty-four (8.66%) fathers reported that they were spending more time at work to disconnect from home and family; however, this was not significantly different between fathers with and without depression (χ2 = 0.025, p = .875). Speeding ticket was received by 47 (16.97%) of the fathers after their newborn’s birth. Thirty-six (13%) fathers felt isolated and disconnected from their partner. The number of fathers who reported feeling isolated and disconnected from their partners was significantly different between fathers with and without depression (χ2 = 6.322, p = .012; Table 2).
Information Related to the Family, Wife, and Pregnancy for Fathers With/Without Depression.

Note. *p value based on Fisher’s exact test. **p value based on the chi-square test. IVF = in vitro fertilization. Bold values are statistically significant (p-value less than 0.05).
Pregnancy-Related Correlates of Depression
Almost half of the fathers, 159 (56.9%), reported that the pregnancy was planned. Only 12 (4.3%) had conceived using in vitro fertilization (IVF). Almost all fathers, 262 (93.91%), had attended antenatal checkups with their wives, and 224 (80.58%) had attended their newborn’s delivery. The mode of delivery was reported as vaginal by 191 (67.97%) fathers, and cesarean section by 91 (34.73%) fathers. Thirty-one (11.07%) fathers reported complications during childbirth. Forty-four (15.83%) fathers had lost a child before. Twenty-two (8.27%) fathers reported that their newborn had been diagnosed with congenital birth defects/syndromes. Variables related to pregnancy were not significantly different between fathers with and without depression (Table 2).
ROC Curve Analysis
The results of the ROC curve analysis are summarized in Table 3 and Figure 2. The area under the curve was 0.81. A score of 8/9 was identified as the optimal cutoff for screening for depression among fathers. A cutoff of 8/9 yielded a sensitivity of 77.8% and a specificity of 81.3%. At a cutoff of 8/9, 7 of 9 depressed fathers and 39 of 48 nondepressed fathers were classified correctly, giving an overall accuracy of 80.7%. The gold standard test (DSM-5) showed that nine (15.79%) fathers were depressed.
Receiver Operating Characteristic Curve Analysis.

Note. EPDS = Edinburgh Postnatal Depression Scale. *The cutoff used to identify depression.

Sensitivity and false-negative rate of Edinburgh Postnatal Depression Scale scores in the study sample.
Risk Factors of Depression
The potential risk factors of PPND among fathers of a newborn during postnatal period are summarized in Table 4. Multiple logistic regression using maximum likelihood estimation was used to obtain the odds ratio. Variable selection was based on the response rate, theoretical relevance, pattern of correlation with outcome, and computational feasibility. Initial model included demographic, employment-related, social support of friends/family, family history of depression, marital relationship, pregnancy-related, wife having postpartum depression, and psychological well-being correlates, with less than 30% missing values. Variables with least relevance and that showed weak relationship with outcome variable were eliminated one by one to achieve the final model. The final results included close relative with depression, family setup, social support of friends/family, if the wife is reported as depressed by father, marital relationship, father spending more time at work, and father feeling isolated and disconnected from partner. None of the correlates were identified as statistically significant, except that depressed fathers were more likely to feel isolated or disconnected from their partners compared with nondepressed fathers, with a significant odds ratio of 2.74 (95% CI [1.23, 6.1]) (Table 4).
Risk Factors of Depression Among Fathers of Newborn.

Note. Probabilistic model is based on the probability of having depression. CI = confidence interval; SE = standard error. The italics are reference groups. *Statistically significant p-value
Discussion
The EPDS has been validated in fathers of newborn across Europe and Far East countries, with a variation in reported cutoffs. This is the first study to establish the validity of the EPDS among Arabic-speaking fathers of newborn in the Middle East and Saudi Arabia. The established EPDS cutoff in the current study is 8/9, higher than those established for depression (major or minor) in Vietnam (4/5) (Tran et al., 2012), but more or less similar to the one reported for (major or minor) depression (10/11) in Australia, UK, and China (Edmondson et al., 2010; Lai et al., 2010; Matthey et al., 2001). Italian and Swedish studies reported higher cutoffs, 12/13 compared with 8/9 (Loscalzo et al., 2015; Massoudi et al., 2013). The use of different cutoffs had been reported in a series of Australian studies, cutoff 5/6 for depression or anxiety disorder, and 10 or more for reporting minor or major depression (Matthey et al., 2001). However, using the EPDS-3A (three items; 3, 4, and 5), a score of 4 or more can be used for screening anxiety disorder among fathers (Matthey, 2008; Matthey & Agostini, 2017). The sensitivity, 77.8%, and specificity, 81.3%, in the current study are low compared with those reported in Chinese (91% sensitivity, 97% specificity) and Italian (90% sensitivity and 90% specificity) studies (Lai et al., 2010; Loscalzo et al., 2015), but higher than that reported in the Vietnamese study (68% sensitivity, 77% specificity; Tran et al., 2012).
The current study results depict an EPDS cutoff closer to that of the UK/China, but substantially different from that reported by Italy/Australia. This wide variation in cutoff is caused by the geographic location of the study setting as well as cultural factors. One reason for the variation is the use of heterogeneous samples: in the Italian study, the sample of fathers was very diverse in terms of inclusion criteria, and the majority of fathers had grown-up children (Loscalzo et al., 2015). The time of screening depression has also varied across studies; antenatal versus postnatal. Another reason for the variation is that the symptoms of depression vary between men and women; men suffer with anger, irritability, emotional rigidity, and sleep disturbance (Edward et al., 2015). Men are more likely to have difficulty focusing on work and abuse alcohol/drugs. The symptoms also vary within populations. The prevalence of PPND varies depending on the cutoff used. The use of nonvalidated cutoff leads to a different clinical interpretation of the rates of perinatal depression (Matthey, Henshaw, Elliott, & Barnett, 2006).
The advantages of using the EPDS are that it is open access, it takes only a short time to administer, it is easy to understand, and it is a reasonable tool for screening fathers of newborn for PPND provided that recalibration is performed based on the specific study setting, population, and culture. Studies have reported use of the Gotland Male Depression Scale (GMDS) instrument apart from the EPDS. The Swedish study reported combining the EPDS and GMDS as the Edinburg–Gotland Depression Scale (EGDS) which showed higher sensitivity than the EPDS alone (Madsen & Juhl, 2007; Psouni, Agebjorn, & Linder, 2017).
The result of this study indicates that 16.6% fathers of newborn have PPND. This is the first study to report the prevalence of postnatal depression among fathers of newborn in Saudi Arabia. Prior published results have reported PPND ranging between 2% and 31% (Bergstrom, 2013; Edoka et al., 2011; Goodman, 2008; Matthey et al., 2001; Moussa et al., 2012; O’Hara & McCabe, 2013; Zhang et al., 2016). In the Egyptian study, the reported depression rate (31.4%) among expecting fathers is higher compared to 16.6%; however the results are based on the non-validated cutoff 10 or higher during antenatal period (Moussa et al., 2012). The results are more or less similar to the one reported in Sweden, 10.3% at 3 months postpartum (Bergstrom, 2013); in the UK, 12.7% at 7 weeks postpartum (Edoka et al., 2011); in the United States, 13% at 2 months postpartum (Goodman, 2008); and in China, 20.4% at 2 weeks postpartum (Zhang et al., 2016). The prevalence is higher than that reported in Turkey, 1.8% at 2–6 months postpartum (O’Hara & McCabe, 2013), and in Australia, 3.3% at 6–9 weeks postpartum (Matthey et al., 2001). The comparison with prior published studies is difficult since different methodological approach and diagnostic criteria of depression was used. These studies were selected for comparison because the EPDS was used as a screening tool. However, the time of PPND assessment varied across the studies.
The prevalence of PPND among Saudi fathers, 16.6%, reported in this study is very similar to that of MPPD, 14%, reported among Saudi mothers (Al-Modayfer et al., 2015). The estimated prevalence of PPND can be as high as 50% if the mother is also depressed (Goodman, 2004). Depression among fathers tends to start later than among mothers, and the rate of depression among fathers increases at 6 and 9 months postchildbirth (Goodman, 2004). The estimated prevalence of PPND tends to decline over time during the postnatal period (Goodman, 2004).
There are several confounding factors in PPND research, the most important of which is the lack of standard criteria to diagnose PPND. Other factors that can lead to divergent prevalence results include different methodologic approaches, different assessment tools for screening, clinical heterogeneity, the timing of depression assessment (antepartum/early postpartum vs. late postpartum), study setting, and social and cultural restraints (Paulson & Bazemore, 2010). Such differences make the generalization of results very difficult.
Several risk factors are associated with PPND, such as unemployment, unplanned pregnancy, poor marital relationship, lack of family support, previous history of depression, the presence of depression, the presence of maternal depression, joint families, sex of the baby, and antenatal paternal depression (Moussa et al., 2012). Among them, MPPD has been identified as the most significant risk factor for the development of PPND, and fathers are 8.4 times more likely to get depressed if their partner is depressed (Pinheiro et al., 2006). Researchers have recommended that fathers should be screened for depression, especially if their partners are depressed (Pinheiro et al., 2006). A study conducted in Japan reported no association between maternal and paternal depression, but reported that PPND was associated with employment status, past history of psychiatric treatment, and unplanned pregnancy (Nishimura & Ohashi, 2010).
The relationship of several factors with the risk of depression among fathers was examined in this study. The risk factors were identified based on prior literature, and cultural and social values. Interestingly, no significant association was identified between PPND and suspected risk factors such as employment status, social support of family/friends, family history of depression, family setup, maternal postpartum depression (as reported by fathers), marital relationship, and spending more time at work. The only risk factor significantly associated with PPND was feeling isolated and disconnected from one’s partner. These results are inconsistent with prior studies that reported associations between similar risk factors and paternal depression (Moussa et al., 2012; Nishimura & Ohashi, 2010). One possible reason of insignificance is sample size to assess risk factors. The second possible reason is use of unstandardized methods for risk factors measurement. One of the compelling predictors of PPND reported in the literature is maternal depression (Goodman, 2004). Past history of depression is also associated with PPND (Spry et al., 2018). In the current study, fathers with a history of depression were excluded, which indicates that PPND can appear as first-time depression among men. Fathers who reported social support during pregnancy reported less depression (Castle, Slade, Barranco-Wadlow, & Rogers, 2008).
The symptoms of depression vary between men and women; the most commonly reported depressive symptoms among fathers of newborn are exhaustion, irritability, despair, anger, emotional rigidity, self-criticism, sleep disturbance, risk-taking behavior, and alcohol and/or drug abuse (Brownhill, Wilhelm, Barclay, & Schmied, 2005; Goodman, 2004; Martin, Neighbors, & Griffith, 2013). The causes of PPND among fathers are a sense of responsibility, the inability to cope with changes due to the arrival of a new baby, changes in lifestyle, changes in the marital relationship, lack of sleep, increased expenses, and increased workload (Goodman, 2004).
The study fills a gap in the literature regarding PPND among Saudi fathers. The findings provide direction for perinatal mental health assessments during the transition to parenthood. The results were strengthened by EPDS validation in the study sample. The results of the field survey are applicable to the general population because a random sample of fathers was selected from all fathers living in the central region and visiting the birth registration office. The generated results are unbiased because the psychologist was blinded to the participants’ EPDS scores. Unlike other studies, fathers with a prior history of depression were excluded. The sample was homogeneous in terms of the age of the baby. The prevalence is reported after adjustment for sensitivity and specificity.
Limitations
The current study has some limitations. The tool was less sensitive, and requires validation keeping in mind the social, cultural, and religious beliefs of society. A focus group discussion is needed to develop a tool specifically intended to be used among fathers.
Because of the study setting, assessment of the newborn’ mothers for depression was impractical. Consequently, the ability to understand the impact of maternal depression on paternal depression was impaired. To mitigate the issue, a simple, self-reported question about the mother’s depression status was included in the questionnaire. Because of the lack of a control group of normal individuals, it was impossible to assess whether the observed depression rates differed from that reported in the general population. This study has relied on a single psychologist to assess the ground of truth of depression. This approach might have an implication on the reproducibility of the estimated prevalence. Finally, the sample size is not very large which might impact the generalizability of the results; however the sample size is close to the average sample size (313) reported across studies.
The EPDS is a reasonably sensitive tool for screening fathers of newborn for PND provided that recalibration is performed based on specific populations and cultures. However, the current diagnostic criteria of PND are biased toward women’s response to depression. Diagnostic instruments to measure symptoms specific to depression in men may result in an increase in detection of the condition (Martin et al., 2013). There is a need to develop an instrument focused on the mental health of men during the perinatal period.
Conclusion
Depression in men is a serious problem, and most men with the condition suffer without acknowledging it because of the stigma attached to depression by society. PPND must be recognized as a serious public health issue. Both men and women experience depression, but the willingness of men to share their feelings after a newborn’s birth differs from that of women (Brownhill et al., 2005). It is necessary to identify fathers with PPND to prevent the development of behavioral problems in their children and disruption of their relationship with their spouse. Perinatal mental health assessment should focus on the family as a unit. Most laypeople and health-care workers are unaware of PPND. Therefore, clinicians working in obstetrics and pediatrics must be educated about PPND. There is a need to develop an instrument focused on the mental health of men during the perinatal period. Future long-term cohort studies at different time points (antenatal, postnatal, and during the years of child growth) are recommended to determine the implications of PPND.
Footnotes
Acknowledgements
The authors would like to thank all the fathers who shared their experiences. The authors would also like to thank the KAIMRC for providing the grant and the postnatal ward nurses for their support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the King Abdullah International Medical Research Center (KAIMRC) with the grant number RC13/206/R. The funder had no further role in the study design, data collection, analysis or interpretation of the data, report writing, or decision to submit the article for publication. The views expressed in paper are solely of authors.