
Abstract
The aim of this project was to review current research regarding postnatal depression in fathers and to present potential screening and referral options. The search was limited to scholarly (peer reviewed) journals and all articles were retrieved with date limits. Initial search parameters were the following: antenatal depression OR pregnancy depression OR postnatal depression OR perinatal depression AND father* OR men OR paternal. The search yielded 311 abstracts returned. With reference to the inclusion criteria and primary and secondary outcomes intended for the focus of this review, N = 63 articles were retrieved and read in full by the researchers. These articles were included in the final integrative review. Depression in fathers following the birth of their child was associated with a personal history of depression and with the existence of depression in their partner during pregnancy and soon after delivery. Based on the review the authors suggest routine screening and assessment of both parents should occur across the pregnancy and postnatal period. The use of the Edinburgh Postnatal Depression Scale for screening of depression in men needs to be linked to referral guidelines for those individuals who require further investigation and care.
Introduction
The World Health Organization (WHO) has reported that 450 million people globally are affected by mental illness (WHO, 2007), with gender being implicated as a critical determinant. In 2000, depression was reported as the leading cause of disability as measured by years lived with the disability and the fourth leading contributor to the global burden of disease measured as Disability Adjusted Life Years (Mathers, Boerma, & Ma Fat, 2008). More recently, depression has been identified as the second cause of Disability Adjusted Life Years s in the age category 15 to 44 years for both sexes combined (WHO, 2011). It is estimated that 51.8% of females and 48.2% of males in the United States experience depression (Kessler et al., 2003) at some time in their lives. In Australia, female depression rated higher than male depression prevalence where data were derived from a national sample of 10,641 people 18 to 75+ years of age (Wilhelm, Mitchell, Slade, Brownhill, & Andrews, 2003). Around a fifth (19%) of individuals in the United Kingdom had some indication of anxiety or depression with a higher proportion of women than men and a higher proportion of those aged between 40 and 59 or aged 80 and older (Beaumont & Lofts, 2013).
The mental health of women and the need for identification of mental illnesses such as depression during pregnancy and after the birth (postnatal depression [PND]) of their child is well described in the literature. What is often not considered is the mental health of fathers in the pre- and postnatal periods. Fathers are at risk of depression at this time, expressly if their partner becomes depressed, yet they are usually not the focus of screening (Ramchandani et al., 2011). Currently, the focus of care in the majority of maternity services is on the mother and infant. This integrative review aims to identify literature on PND in fathers and to present potential screening and referral options available to clinicians.
Objectives
The authors aimed systematically to search, critically appraise, and summarize the literature on PND in fathers and to review current screening options, impact on the family unit, and interventions available for fathers experiencing PND.
Method
Search Outcomes
The primary outcomes of interest were the following: screening, assessment, and referral of PND in fathers; paternal depression; and effects of paternal depression. Secondary outcomes of interest include adverse events of the depression.
Databases Searched
A search of the literature was undertaken using the following databases: Academic Search Complete, CINAHL Plus with full text, Health Source, Nursing/Academic, Medline complete, Psychology and Behavioural Sciences Collection, and SocINDEX with Full Text. The search was limited to scholarly (peer-reviewed) journals, and all articles were retrieved with no time limit. Initial search parameters were the following: antenatal depression OR pregnancy depression OR postnatal depression OR perinatal depression AND father* OR men OR paternal.
Inclusion Criteria
The inclusion criteria for this integrative review included articles written in English, paternal PND, and screening, assessment, and referral of PND in fathers.
Exclusion Criteria
The exclusion criteria used for this review included the following: articles not written in English, articles focusing exclusively on maternal PND, articles not subject to peer review, and editorials and other non-peer-reviewed material.
Quality Appraisal
The quality of the research was assessed with reference to the Critical Appraisal Skills Program qualitative research checklist and the Critical Appraisal Skills Program: Cohort Studies is a methodological checklist (Taylor et al., 2000).
Synthesis
Data were extracted by two of the researchers. Extracted data were collated and synthesized.
Results
The search yielded 311 abstracts. With reference to the inclusion criteria and primary and secondary outcomes intended for the focus of this review, 63 articles were retrieved and read in full by the researchers (see Figure 1).

PRISMA of abstracts returned.
Prevalence and Risk Factors
In the 1990s, PND in fathers was generally considered rare (Lane et al., 1997). More recently, paternal PND is gaining recognition as a significant problem that negatively affects the family unit. There are also increasing amounts of research demonstrating that the prevalence of PND in fathers is not as rare as first thought and that there are risk factors for the development of PND in fathers that health care professionals should be aware of.
Maternal depression has been identified as the strongest predictor of paternal depression during the postnatal period (Goodman, 2004). Depression in fathers following the birth of their child is also associated with a personal history of depression (Gao, Chan, & Mao, 2009) where a history of severe depression and high prenatal symptom scores for depression and anxiety have been determined as the strongest predictors of paternal depression in the postnatal period (Ramchandani, Stein, et al., 2008).
The literature suggests a detailed assessment of fathers during the postnatal period, especially when their female partners are depressed, to allow for timely and appropriate treatment and/or interventions (Schumacher, Zubaran, & White, 2008). Paulson, Dauber, and Leiferman (2006) explored the individual and combined effects of PND in mothers and fathers and parenting behavior. In their study, a national sample of 8,865 cases was further narrowed down to include only those biological mothers with corresponding resident father data, yielding a final sample size of 5,089. Of these, 14% of mothers and 10% of fathers exhibited levels of depressive symptoms that were associated with clinical diagnoses such as depression with or without anxiety. Escriba-Aguir and Artazcoz (2011) reported similar rates of PND in their longitudinal study (n = 687 mothers and n = 669 fathers) with 9.3% of mothers and 3.4% of fathers diagnosed with depression at 3 months and 4.4% of mothers and 4.0% of fathers diagnosed with depression at 12 months postpartum.
Many studies report the onset of paternal depression often followed depression in the mother (Dudley, Roy, Kelk, & Bernard, 2001; Edmondson, Psychogiou, Vlachos, Netsi, & Ramchandani, 2010; Figueiredo & Conde, 2011; Hanington, Heron, Stein, & Ramchandani, 2012; Pinheiro et al., 2006; Veskrna, 2010; Wee, Skouteris, Pier, Richardson, & Milgrom, 2011) with approximately 10% prevalence overall. Furthermore, studies in this review revealed an association for paternal depression with having an unsupportive relationship and being unemployed (Ballard & Davies, 1996; Davé, Nazareth, Sherr, & Senior, 2005). Other factors associated with an elevated risk of paternal PND include a personal history of depression and/or anxiety, maternal depression during pregnancy, older age, low levels of marital satisfaction, financial/life stressors, a feeling of incongruity between expectations of parenthood and the realities, lack of outside social supports for parenting, poor social functioning, dissatisfaction with partner support, poor communication between the parents, gender of the child for some cultures, adaptation impaired paternal/newborn bonding, and/or feelings of exclusion from maternal/newborn bonding (Bradley & Slade, 2011; Buist, Morse, & Durkin, 2003; Davé et al., 2005; Davey, Dziurawiec, & O’Brien-Malone, 2006; Kim & Swain, 2007; Mao, Zhu, & Su, 2011; Matthey, Barnett, Ungerer, & Waters, 2000; Paulson & Bazemore, 2010; Skari et al., 2002; Van Den Berg et al., 2009).
Our review also highlighted that men and women differ in their knowledge and beliefs about the symptoms and causes of PND, which has implications for antenatal education and postnatal care involving education for the family. PND is often perceived by women as having a biological rather than psychosocial cause, thus having implications for recognition of these symptoms for men. More specifically, the condition is unique to women who are pregnant and give birth, potentially excluding men in consideration of PND. Also, the recognition of anxiety in women and their partner (via screening) in the postnatal period was relatively low, although higher among those with mental health training. As revealed in this review, screening for PND in fathers is often underestimated, holding implications for screening, assessment, and treatment for postnatal mood conditions (Edmondson et al., 2010; Fisher, Kopelman, & O’Hara, 2012; Goodman, 2008; Lai, Tang, Lee, Yip, & Chung, 2010; Matthey, 2008; Matthey, Barnett, Howie, & Kavanagh, 2003; Tran, Tran, & Fisher, 2012) ultimately having implications for families.
Impact of Paternal Postnatal Depression
Relationships between mothers and fathers following the birth of their child can be fraught and depression is more likely to develop in both mothers and fathers in the first year of birth (Davé, Petersen, Sherr, & Nazareth, 2010). Having an unplanned pregnancy is associated with higher levels of paternal depression with lower mother–father relationship happiness, increased risk of disharmony within the relationship, and higher coparental conflict (Bronte-Tinkew, Scott, Horowitz, & Lilja, 2009; Muscat, Thorpe, & Obst, 2012; Nishimura & Ohashi, 2010; Ramchandani et al., 2011). If fathers experience PND, it can affect not only the interactions they have with their children but also interfere with the interactions with the child by their partner (Bradley & Slade, 2011). Work by Goodman (2008) demonstrated that maternal PND is associated with increased paternal depression resulting in higher paternal parenting stress and the risk of couple morbidity, with implications for bonding with the infant and maintaining relationships (Edhborg, 2008; Edhborg, Matthiesen, Lundh, & Widstrom, 2005). For fathers, the individual impact of PND depression includes working and short-term memory loss (Pio De Almeida et al., 2012) and on the ability to perform tasks at their place of employment (Melrose, 2010). PND in fathers can negatively affect the child as well as other relationships within the family unit. The children of depressive fathers are at risk for emotional and behavioral problems (Schumacher et al., 2008). Paternal depression is believed to have a specific effect on their children’s early behavioral and emotional development (LeFrançois, 2012; Letourneau et al., 2012; Ramchandani et al., 2011; Ramchandani, Stein, Evans, & O’Connor, 2005). Negative father and child relationships can lead to detrimental cognitive, behavioral, social, and emotional development of children (Fletcher, Feeman, Garfield, & Vimpani, 2011; Goodman, 2008; Paulson et al., 2006; Paulson, Keefe, & Leiferman, 2009; Sethna, Murray, & Ramchandani, 2012; Wanless, Rosenkoetter, & McClelland, 2008), psychiatric conditions developing in later childhood (Ramchandani, O’Connor, et al., 2008; Ramchandani, Stein, et al., 2008), and some research suggest this impact is more significant in male children (Hanington, Ramchandani, & Stein, 2010; Ramchandani et al., 2005; Ramchandani, O’Connor, et al., 2008). Davé et al. (2005) reveal that fathers experiencing a lower mood was associated with a negative infant temperament measured by the Infant Characteristics Questionnaire. Davis, Davis, Freed, and Clark (2011) reported that fathers experiencing depression were less likely to spend time reading to their 1-year-old child and more likely to report using spanking, which is supported in findings by Paulson et al. (2006), who state that depressive symptoms in both mothers and fathers is negatively associated with positive activity, such as reading and singing songs, with their child. Relationships are also affected between father and child, for example, depressed fathers are more likely than nondepressed to smack/spank their child (Davis et al., 2011).
Screening for PND in Fathers
The Edinburgh Postnatal Depression Scale (EPDS) was devised as a screening measure for postpartum depression in women; it can also be applied during pregnancy. Best practice guidelines indicate the EPDS should be used by health professionals as a component of the assessment of women for symptoms of depression in the antenatal period and women in the postnatal period. The EPDS assesses symptoms of anhedonia and reactivity, self-blame, anxiety, panic, coping, sleeplessness (due to unhappiness), sorrow, tearfulness, and thoughts of self-harm. The EPDS is a 10-item scale that includes questions such as “I have been able to laugh and see the funny side of things” and “I have blamed myself unnecessarily when things went wrong.” Respondents indicate on a 4-point scale the response that best describes the way they have been feeling over the past seven days. Items are scored from 0 to 3 with a resulting range of 0 to 30. The EPDS has been validated and used extensively in screening for depression in new mothers; some studies have reported its use with fathers. Matthey, Barnett, Kavanagh, and Howie (2001) recruited couples at two time points—antenatally and at 6 weeks postnatally—and EPDS scores in 208 fathers and 230 mothers were validated using the Diagnostic Interview Schedule. In the fathers, using distress (depression or anxiety disorders) as the criterion, a cutoff of 5/6 was optimum, whereas for mothers the optimum cutoff screening was at 7/8. The lower cutoff values for fathers was mostly due to differential response to the “crying” item. In a study exploring the sensitivity of the EPDS for fathers (n = 607) 6 weeks after the birth of their child, the EPDS identified 5% of fathers to have depressive symptoms (using a cutoff of >10) as compared with 3.4% with a male depression scale (Gotland Male Depression Scale; Madsen & Juhl, 2007; see Table 1 for details related to Scale cutoff points for men for the EPDS and other depression screening scales). Thus, the EPDS is a suitable screening tool for fathers in the postpartum period, albeit cutoffs are different to those applicable in women. It is important to note the EPDS does not diagnose depression (Dennis, 2005) but can alert the clinician to the need for a full diagnostic interview.
Scale Cutoff Points for Men for the EPDS and other Depression Screening Scales.
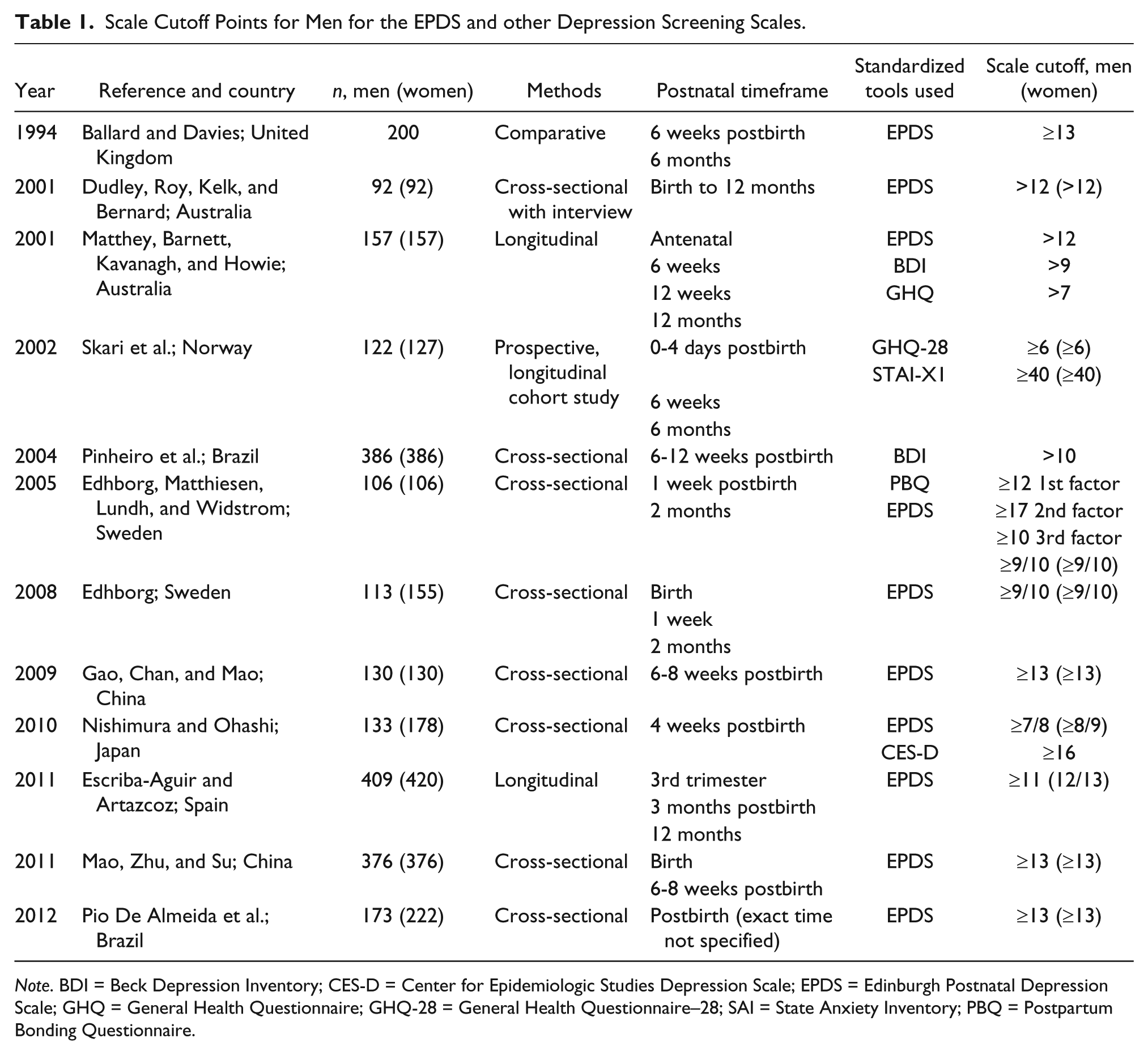
Note. BDI = Beck Depression Inventory; CES-D = Center for Epidemiologic Studies Depression Scale; EPDS = Edinburgh Postnatal Depression Scale; GHQ = General Health Questionnaire; GHQ-28 = General Health Questionnaire–28; SAI = State Anxiety Inventory; PBQ = Postpartum Bonding Questionnaire.
Interventions for Fathers With PND
Areias, Kumar, Barros, and Figueiredo (1996) and Morse, Buist, and Durkin (2000) have emphasized the importance of prevention and treatment for fathers with PND. Prevention was the focus of a randomized controlled trial of the impact of education and support (i.e., antenatal education led by a male facilitator and a 6-week postpartum education and support materials) for fathers with a breast-feeding partner (Tohotoa et al., 2012). The results revealed that both the intervention and control group experienced anxiety prior to birth but fathers in the intervention group reported less anxiety measured using the Hospital Anxiety and Depression Scale than those in the control group at first night of the hospital-based antenatal program and at 6 weeks postpartum. Additionally, fathers reporting higher levels of perceived social support throughout the pregnancy experience significantly lower levels of depression and distress 6 weeks postdelivery (Castle, Slade, Barranco-Wadlow, & Rogers, 2008). Interventions such as cognitive behavior therapy, group therapy, comprehensive antenatal psychosocial assessment, and the traditional psychodynamic therapy can be effective for men experiencing PND (Fletcher, Vimpani, Russell, & Sibbritt, 2008; Spector, 2006). Furthermore, support gain through sharing experiences among other fathers in the transition toward fatherhood can have benefit (Chin, Hall, & Daiches, 2011).
Longitudinal studies identify a high incidence of distress in couples during mid to late pregnancy (Morse et al., 2000), some of which is related to changes in intimacy and sexual behaviors as a couple. Health care professionals are well placed to discuss some of these potential sexual/intimacy changes and expectations to facilitate a more positive transition to parenthood for father and mothers (Condon, 2006). Education can be facilitated by health care professionals and be accessed through other forums. For example, father-inclusive guidelines added to website information regarding perinatal depression can assist fathers with connection to their newborn or for possible interaction with other fathers (Fletcher, 2011), and early indications indicate access to this education for fathers can positively influence their approach to parenting (Fletcher, Vimpani, Russell, & Keatinge, 2008). Pilot work performed by Letourneau, Duffett-Leger, Dennis, Stewart, and Tryphonopoulos (2011) reported that fathers whose partners had PND experienced barriers such as not knowing where to look for PND resources and the difficulty in reaching out to others, whether it be social supports or referrals to health care professionals.
Implications for Practice: Referral Options
For fathers the potential stigma related to paternal depression may represent a barrier to help-seeking behaviors and subsequent referral for paternal PND. Referral is a four-stepped process that involves assessment, education, brokering for services for patients, and linking of the patient into the referral endpoint (Blashki et al., 2003). General practitioners and psychiatrists have a key role in the referral pathway for the management of PND. Importantly, the assessment provides an opportunity for engagement of the patient and their partner. This includes establishing an effective therapeutic relationship, education, providing a rationale for treatment, and explaining expected timeframes (RANZCP, 2009). A recent systematic review supports that any psychosocial or psychological involvement, compared to usual postpartum care, is associated with a decrease in the rate of depression within the first year postpartum (Dennis & Hodnett, 2007). Referral options for parents postnatally include general practitioners, psychiatrists, psychologist and other allied health professionals with mental health expertise, as well as mental health nurses.
Implications for Policy, Practice, and Research
Routine screening and assessment of both men and women needs to occur during periods of interaction with health professionals across pregnancy and the postnatal period. The use of the EPDS for screening of depression in both mothers and fathers is appropriate in terms of sensitivity and specificity of the scale, in addition to the user friendly nature of the scale, which can be easily adapted to routine practice in the hospital or postnatal setting. Since the family unit is affected by depressed fathers as much as it can be affected by depressed mothers, screening both parents in practice is logical. For fathers, support from their partner, PND educational programs, PND and particularly paternal PND health promotion campaign potentially influencing community behaviors, policy for paid paternal leave, as well as consideration of mental health care may help fathers cope with stressful experiences during the postnatal period. Further examination of sexual relationship and communication between parents is potentially an area that can offer insight into paternal PND. An area for further exploration in light of a paucity of literature is the experience of fatherhood including adopted children, the number of children, and the role of culture on the experience of paternal PND.
Limitations
An integrative review offers a unique perspective of the current literature regarding paternal PND; however, there are limitations associated with using different research methods that can contribute to a lack of rigor and bias. When mixed data are synthesized together, there could be a chance of invalid assumptions. This review was limited to peer-reviewed articles. Inclusion of gray literature and book chapters might have brought others perspectives.
Conclusions
This integrative review revealed the recognition, assessment, and treatment of PND in fathers after the birth of their child rarely happens in practice, even thought there are potential benefits to the father, the mother, and the family in the early assessment of paternal depression. Additionally, very little has been reported on current practices that includes assessment and referral of fathers during the perinatal period. Some barriers may well be related to timing of screening/assessment and referral and whether this is an intervention to be undertaken by the hospital obstetric hospital staff or the obstetrician or for fathers to self-refer to their own general practitioner if they experience mood changes. Clinicians working in the obstetric field as well as community service providers need to be aware of PND not only in the mother but also in the father. Clinicians need to consider increasing their awareness of the referral options available in their institution and/or community for both mothers and fathers where further assessment is required. Education for midwifery staff is required, since highlighting the existence of PND in men may be a new consideration for staff. The recognition of the health of the family unit as a whole (including the father) rather than components parts (i.e., mother and baby) presents an opportunity to lead the way in excellence in clinical care for these health care consumers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.