
Abstract
Introduction:
Paternal postnatal depression is a type of depression that occurs among male partners after childbirth. Although the problem has a multidimensional impact, there is limited data in low-income countries, including Ethiopia. Therefore, this study aimed to uncover this problem in the study setting.
Objective:
To assess paternal postnatal depression and associated factors.
Method and study period:
A community-based cross-sectional study was employed from April 1 to 30, 2023, among 423 fathers in Mattu Town, Southwest Ethiopia. A face-to-face interviewer administered a structured questionnaire prepared by the Open Data Kit tool. The study participants were selected by simple random sampling techniques. A binary and multivariable logistic regression analysis was used. Both crude and adjusted odds ratios with a 95% confidence interval were calculated, and a p-value of less than 0.05 was used.
Result:
Among 423 fathers, 412 participated, making the response rate 97.40%. The prevalence of paternal postnatal depression was 29.37% (95% confidence interval: 24.95%, 31.25). The poor wealth index (adjusted odds ratio (AOR): 1.67; 95% confidence interval: 1.88, 3.14), loneliness (AOR: 1.81; 95% confidence interval: 1.20, 3.20), poor social support (AOR: 6.08; 95% confidence interval: 2.55, 14.48), feeling of family income stress (AOR: 3.22; 95% confidence interval: 1.89, 5.50), and history of adverse pregnancy outcome (AOR: 3.00; 95% confidence interval: 1.62, 0.59) were significant associated factors at p-value less than 0.05.
Conclusions:
The study identified nearly 3 in 10 fathers suffering from paternal postnatal depression. Therefore, the Ministry of Health and other concerned bodies should focus on this population group to alleviate it. In addition, health professionals and extension workers should provide evidence-based care plans based on the identified factors.
Introduction
Postnatal depression is a type of depression that occurs after childbirth among couples. 1 It is a common and serious mental health problem that negatively affects how an individual thinks, feels, and acts. This problem is a common, debilitating, and potentially lethal disorder. 2 Common symptoms of paternal postnatal depression (PPND) are anger, violent behavior, an increase in substance use, irritability, low motivation, and poor concentration.
In addition, suicidal thoughts, withdrawing from relationships, and working a lot more or a lot less are some of the characteristics of husbands who suffer from depression.3–6 The birth of a child constitutes a major developmental event for both women and men. It has profound effects on the parents’ identities and couples’ relationships; therefore, it has an impact on family life.7,8
The arrival of a new baby adds responsibilities to partners that impact their finances and increase stress, which leads to PPND.9–11 Men’s emotional health can be overlooked during their partner’s pregnancy and the first year after childbirth, which is difficult to assess.12,13 Studies identified that a significant number of male partners can face mental health problems during the postnatal period, and when the men spend a lot of time with a baby, their testosterone level will drop, which leads to serotonin withdrawal which leads to depression. 14
Globally, depressive disorder is the leading cause of disability 15 and contributes to common mental disorders with the largest magnitude. 15 Common mental disorder is one of the current global challenges with a multidimensional impact on the world that ranges from 25% to 31% across the world. 16
A systematic review of the studies conducted during the COVID-19 pandemic revealed that the pooled prevalence of PPND was 25%, which was seven times higher than the pre-pandemic period. 17 In addition, a systematic review carried out on the studies done from 1990 to 2019 revealed that the prevalence of PPND ranges from 1.2% to 25.5%. 18 Some cross-sectional studies obtained from both high- and low-income countries on these population categories identified the largest magnitude of PPND, which ranges from 9% to 27.9%.19–25
Paternal postnatal depression has a worse multidimensional impact in both high- and low-income countries. It is now recognized as a serious and prevalent problem, associated with poorer well-being and functioning among all family members. 26 It can lead to significant paternal morbidity, like suicide attempts that are 46.5% higher than their counterparts and need special concern. 27 As it was identified, PPND worsens maternal postpartum depression, which has a significant impact on maternal–infant interaction and parent–child relationships.28–30
In addition, it has negative impacts on families, including increasing emotional and behavioral problems among their children, either directly or indirectly, and can lead to family dissolution. 31 Infant exposure to PPND can impair a child’s school performance and cognitive development.32,33 In addition to maternal, infant, and family health, PPND has a significant impact on the world economy as it threatens the workforce and increases healthcare costs. 34
The scholars have identified some factors that can lead to PPND. As was revealed by a systematic review conducted on studies conducted among fathers after childbirth, hormonal, maternal, and some sociodemographic factors were significantly associated with PPND. 18 The studies revealed that infants with sleep problems, a previous history of mental illness, and low social support were significantly associated with PPND.18,23,31 In addition, the study conducted in Japan identified a history of infertility treatment, parity, and economic anxiety as significantly associated factors with PPND.18,21,31
Currently, global mental health has been integrated with the sustainable development goal (SDG) agenda to overcome the challenges of mental health in both high- and low-income countries.35,36 In the new SDGs, the United Nations (UNs) has finally defined mental health as a global development priority and set the scene for an ambitious plan to tackle the world’s challenges in the coming 15 years. 37 In addition, Ethiopian Health Sector Transformation Plan 2 has plans to reduce noncommunicable diseases which might include mental health. 38
Paternal health is of paramount importance for maternal health, infant health, and the health of other family members. In addition, paternal health can increase maternal postnatal care utilization and infant immunization. Although mental health is a current global challenge in the health sector, paternal mental health problems are a neglected area in low-income countries. There is a gender difference in mental health throughout the life cycle of a human being, but PPND did not receive attention from scholars and researchers in low-income countries, including Ethiopia.
To our knowledge, there is no concrete data on PPND to screen and treat male partners with this kind of problem in Ethiopia. Similarly, it did not receive attention from the health sector and researchers in low-income countries, as men can try to cope by hiding this problem from them. Therefore, this study aimed to assess the prevalence of paternal postnatal depression and associated factors in Mattu town, southwest Ethiopia, in 2023.
Methods
Study area and period
The study was conducted in Mattu town from April 1 to 30, 2023. Mattu Town is the administrative capital of Iluababor Zone, which is 553 km from the capital city of the country, Addis Ababa, and is the homeland of a natural forest registered by United nations educational, scientific and cultural organization called Yayo Forest which is enriched by organic coffee plants. In addition, the town is found in the greenest zone in the Western Oromia region and is endowed with natural resources like Bacho and Sor waterfalls that can attract tourists throughout the year.
The town has six kebele, namely Aba Saya, Gadisa Oda, Tabo, Kolokorma, Aba Mole, and Sor, with 42,496 households and a total population of 102,074. This town has one government referral hospital, one nongovernmental hospital (Hamlin Fistula Center), one governmental health center, six health posts, and 28 private clinics. The town annually has 3840 expected pregnancies and deliveries. 39 The report for 2022 showed that the total delivery for the town was 2592.
Study design
Community-based cross-sectional study design was employed.
Population
Source population
All men who have less than 1-year-old infants in Mattu town.
Study population
All selected men who have less than 1-year-old infants in Mattu town and who have lived in the area for at least 6 months.
Eligibility criteria
Inclusion criteria
All selected men who had less than 1 year of infants during the data collection period were included in the study.
Exclusion criteria
All men who lived in the area for less than 6 months and were less than 18 years old were excluded.
Sample size determination
The sample size is calculated using Open Epi Info software version 7.2 based on the proportion of PPND at 50% at a 95% confidence level with a degree of precision of 5% since there was no similar study conducted on this population category in the study area. Then it became 384, and by adding 10% non-response rates, finally 423 men were selected for this study.
Sampling techniques
Initially, the total number of deliveries in 2022 in the six kebele of Mattu Town was obtained from the Health Extension Workers logbooks, which were 2592. Then, based on the data obtained from each kebele, proportional allocation was done to get the final sample size. Then, proportionally allocated eligible men were selected by a simple random sampling method using the serial numbers of registered men, and selected houses were coded 1 week before the actual data collection period with the help of Health Extension Workers.
Study variables
Dependent variable
Paternal postnatal depression.
Independent variables
Independent factors for PPND were classified into sociodemographic factors (age, marital status, educational status, economic anxiety, wealth index, occupation, and family size), paternal personal, social, and infant-related factors (social support, loneliness, and infant health), and couples reproductive, health, and marital-related factors (satisfaction with the gender of the current baby, known diagnosed mental illness, index of pregnancy during the current baby, known history of adverse pregnancy outcomes, and mood of delivery).
Operational definitions and measurements
Paternal postnatal depression: Partners who scored greater than or equal to 10 out of 30 will be considered to have depression symptoms, and code “1” was given. Partners who scored less than 10 out of 30 were not considered to have depression symptoms, and code “0” was given for this study. 40
Paternal loneliness: Based on the University of California Los Angeles (UCLA-3) 20-item Loneliness Scale, partners who score less than 28 (have no loneliness) were coded “0,” and code “1” was given for those who scored greater than or equal to 28 (have loneliness). 41
Social support: Men who scored on the Oslo-3 social support scale 3–8 out of 14 were classified as “poor social support,” 9 to 11 as “moderate social support,” and scores from 12 to 14 as “strong social support” after the overall score is summed up. 42
History of adverse pregnancy outcome: It was defined as a partner whose wife has at least one of the following: spontaneous abortion, stillbirth, early neonatal death, or a neonate with congenital anomalies for this study. 43
Economic Anxiety: Feeling of worry about family budget (yes/no). 21
Household Wealth Index: Principal component analysis was done based on items collected based on ownership of assets and properties. Then it was classified into three equal parts: poor coded “1,” medium coded “2,” and rich coded “3” based on previous study. 44
Data collection tool and methods
The tool contains sociodemographic characteristics, a tool to assess outcome variables, a tool to assess paternal personal, social, reproductive, health, and infant-related factors, and a wealth index tool. This tool was developed after similar and related online published literature was reviewed.6,15,20,41,42,45
Paternal postnatal depression was assessed using the Edinburg postnatal depression tool, which is commonly used to identify self-reported depression symptoms. It has 10 items, with each item having a minimum score of “0” and a maximum score of “3.” Based on related previous studies, a cut point of ⩾10 was used to identify depression symptoms, and <10 was used to classify no depression symptoms. The content validity of the tool was done. The internal consistency of the tool was checked and had a Cronbach’s alpha test of 0.81, which has specificity and sensitivity of 78.2% and 89.5%, respectively. 40
The paternal loneliness assessment tool was adapted from the validated University of California Los Angeles (UCLA-3) 20-item Loneliness Scale (Version 3) that has 20 items on a Likert scale, with each item having a minimum score of “1” and a maximum score of “4” that is classified as “Never, Rarely, Sometimes, and Always” with the values 1, 2, 3, and 4. From the total of 20 items, 9 will be reversed scored based on the responses of the respondents, as explained in the supplementary material. The tool has a minimum score of 20 and a maximum score of 80, and the Cronbach’s alpha test of 0.94. 41
Social support is assessed by the validated Oslo-3 social support scale. The tool has three items, with item number one having four options and the last two items having five Likert scale options. It was classified as poor social support for scores 3–8 out of 14, moderate social support for scores 9–11, and strong social support for scores 12–14 out of the total score. This tool is validated to assess social support in the general population. 42 The data were collected by three trained public health officer graduates and supervised by two public health officers who have experience in data collection and supervision. Written informed consent was obtained after they were informed of the purpose of this study.
Data quality control and assurance
To assure data quality, the tool was translated from the English language to Afan Oromo and then retranslated back into English. A pre-test was done on 10% of the sample size at Bedele Town. Initially, training was given to data collectors as well as supervisors on the questionnaires and the data collection process. Supervision is held by supervisors daily to ensure the clarity, accuracy, and consistency of the collected data.
Data processing and analysis
The collected data were exported from ODK (Open Data Tool Kits) to SPSS Version 25 for cleaning and further analysis. 46 Descriptive statistical analyses, such as frequencies, summary measures, and variability, were used to describe the characteristics of the study participants. A bivariable analysis was done to see the association between the independent variable and the outcome variable using binary logistic regressions. The assumptions for binary logistic regression were checked.
The model goodness of fit test was tested by Hosmer–Lemeshow and Omnibus. 47 All variables with a p < 0.25 in the bivariable analyses were included in the final model of the multivariable analyses to control all possible confounders. A multi-collinearity test was carried out to see the correlation between independent variables using a variance inflation factor >10 and tolerance (T) <0.1, which was considered suggestive of the existence of multi-collinearity. A crude and adjusted odds ratio (OR) with 95% CI was estimated at a p-value of 0.05 and declared statistically significant. Finally, the results were presented in simple frequencies, summary measures, tables, figures, and narrative form.
Ethical statements
Ethical clearance was obtained from the Research Ethics Review Committee of Madda Walabu University College of Health Sciences, Sheshemene Campus, with reference number CBE/057/15. All methods were performed following the principles of the Helsinki Declaration. A voluntary written informed consent and signature were obtained before starting the interview. The name of the respondent was not used except as a unique code for communication. Fathers with this problem are counseled by the data collectors and supervisors to visit health institutions nearby at the end of interviews.
Results
Sociodemographic characteristics of the study participants
Of the total 423 fathers, 412 participated in the study, with a response rate of 97.40%. The mean and standard deviation of the participant’s age were 36.35 and 9.90, respectively. As it was revealed, 89 (21.6%) and 41 (10%) have no formal education and a diploma or above, respectively. The study identified that 30.6% were at a poor economic level and 47.3% were at a medium economic level. In addition, 34% felt family income stress (Table 1).
Sociodemographic characteristics of the study participants in Mattu town, Southern Ethiopia, 2023.
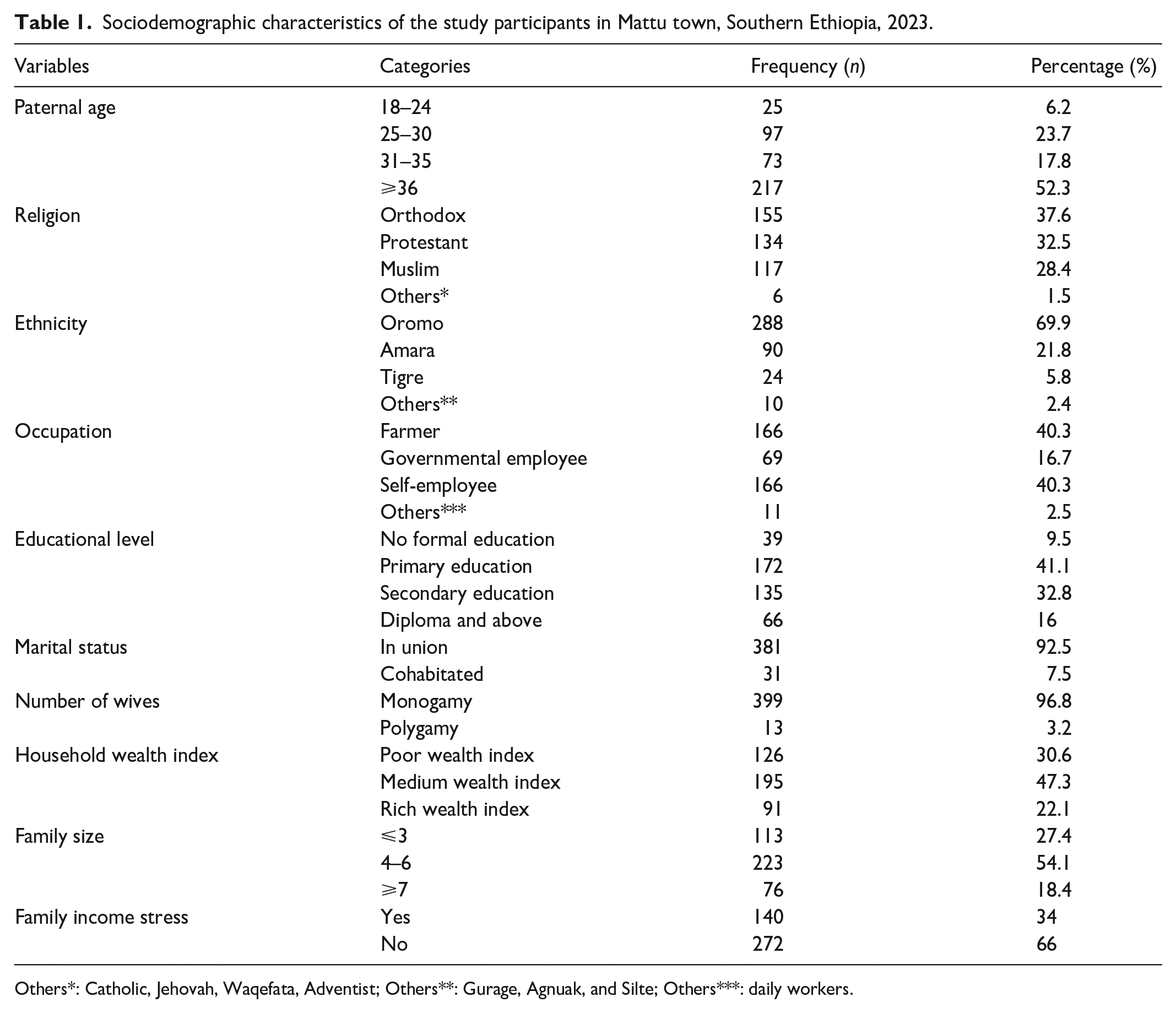
Others*: Catholic, Jehovah, Waqefata, Adventist; Others**: Gurage, Agnuak, and Silte; Others***: daily workers.
Reproductive, personal, substance use, and social-related factors
Of the total study participants, 31.1% did not plan to have an infant before the index of pregnancy, and 18.2% preferred to have a selected gender of infant. In addition, 77.2% of men have a good relationship with the couple’s family, and 86.6% of the study participants’ infants are in good health. Of the total participants, 28.2% and 49.3% were alcohol and khat users, respectively. Furthermore, 24.3% of participants have a feeling of loneliness and 37.4% have poor social support; 10.1% of participants have a diagnosed mental health problem; and 22.8% have a history of adverse pregnancy outcomes (Table 2).
Reproductive, personal, substance, and social-related factors.

CS: cesarean section; SVD: spontaneous vaginal delivery.
Prevalence of paternal postnatal depression among men who have less than 1-year-old infants in Mattu town, southern Ethiopia, 2023
As identified by this study, the prevalence of PPND is 29.37% (95% confidence interval: 24.95%, 31.25%) (Figure 1).

Prevalence of paternal postnatal depression among men who have less than 1-year-old infants, Mattu, Southwest Ethiopia, 2023.
Factors associated with paternal postnatal depression among men who have less than 1-year-old infants in Mattu town, Southwest Ethiopia, 2023.
In the binary logistic regression, eight factors were fitted at 95% CI with a p-value of less than 0.25. After the effects of confounders were controlled in a multivariable logistic regression model, five factors were significantly associated with PPND at 95% CI with a p-value of less than 0.25. The odds of PPND among fathers at poor economic levels were 1.67 times higher than those at rich economic levels (AOR = 1.67, 95% CI: 1.88, 3.14), and the odds of PPND among fathers who have loneliness were 1.81 times higher than those who did not have loneliness (AOR = 1.81, 95% CI: 1.20, 3.20). In addition, the odds of PPND among fathers who have low social support were 6.08 times higher than those with strong social support (AOR = 6.08, 95% CI: 2.55, 14.48).
Furthermore, the odds of PPND among fathers with a feeling of family income strain were 3.22 times higher than their counterparts (AOR = 3.22, 95% CI: 1.89, 5.50), and the odds of PPND among fathers whose wives have a history of adverse pregnancy outcomes were 3.00 times higher than whose wives never experienced it (AOR = 3.00, 95% CI: 1.62, 5.59) (Table 3).
Factors associated with paternal postnatal depression among fathers who have less than 1-year-old infants in Mattu town, Southwest Ethiopia, 2023.

AOR: adjusted odds ratios; COR: crude odds ratios; PPND: paternal postnatal depression.
Significantly associated factors at p-value < 0.05, “1”: Reference group.
Discussion
This study revealed that PPND was a significant problem in Mattu Town. Wealth index, social support, loneliness, history of adverse pregnancy outcomes, and feeling of family income stress were significantly associated factors with PPND at p-values less than 0.05.
The prevalence of PPND was 29.37, which is almost comparable with the study conducted in Guangzhou, South China, at 24.0% and Jeddah, Saudi Arabia, at 27.3%.45,48 This might be due to the similarity in the cut-point value taken to define PPND. However, it was higher than the studies conducted in Ireland, which was 12%, Saudi Arabia, which was 16.6%, and China, which was 7.5%.20,23,49 This might be due to the small sample size used for the study conducted in Ireland and Saudi Arabia. In addition, the difference in the study conducted in China might be due to the difference in the cut value used to define depression symptoms, as 13 was used, which misses participants with this problem.
Furthermore, it was lower than the study conducted in Saudi Arabia at Sultan Military Hospital, at 32.7%. 50 This might be due to the difference in the cut value to classify depression or not, as the study conducted at Sultan Military Hospital took a cut value of nine.
Poor social support was a significantly associated factor with PPND, which was corroborated by the study conducted in Ireland and the systematic review conducted on paternal postnatal depression.18,23 This might be because, during the postnatal period, paternal responsibility may increase to take care of the couple, family members, newly emerged family members, or the emerged offspring, which may affect the psychological health of the male partner as they lack adequate help during this time.
In addition, the feeling of economic stress about family income was a significantly associated factor with PPND. This is supported by the evidence obtained from the study conducted in Japan. 21 This might be due to the increase in economic demand for family members as a result of the addition of a new family member. Then it can increase paternal responsibility, which may lead to economic stress for the fathers, which may end up with PPND.
Similarly, the poor wealth index is significantly associated with PPND. This is supported by evidence obtained from the study conducted in Ireland. 23 This might be during the postnatal period, the physical and emotional demands of family members increase, and it can result in PPND if they are unable to fulfill them. Furthermore, a history of adverse pregnancy outcomes is a significantly associated factor with PPND. To our knowledge, no literature supports this finding. This might be due to the psychological trauma of sadness they faced as a result of the adverse pregnancy outcome that leads to depression if they are unable to control their sadness related to the problem they faced.
Finally, loneliness is a significant factor associated with PPND. However, to our knowledge, we have not found any literature that supports this finding. This might mean that fathers may feel lonely if they have not had someone beside them since the time of childbirth for psychological support to prevent mental health distress as a result of loneliness.
Limitations and strengths of the study
The major limitation of this study was the study design, which is a cross-sectional study design. In addition, the study has not assessed maternal postnatal depression, which may influence paternal postnatal depression. This is the first study conducted on paternal postnatal depression, specifically in the study area.
Conclusions and recommendations
Overall, PPND is a significant paternal health problem in this study setting. Low social support, loneliness, a history of adverse pregnancy outcomes, a feeling of family income stress, and the household wealth index were significantly associated factors with PPND. Based on the findings of this study, the Ministry of Health and other concerned bodies should develop strategies that enable them to overcome the problem.
In addition, screening for paternal postnatal depression should be incorporated into maternity and child health care, as it has significant health problems for mothers and infants. Furthermore, it is better to screen both the mothers and partners jointly by community health extension workers to detect the problem early and prevent further consequences. Finally, it is better if it is studied through a strong study design with their wives.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231208265 – Supplemental material for Paternal postnatal depression and associated factors: Community-based cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121231208265 for Paternal postnatal depression and associated factors: Community-based cross-sectional study by Lema Fikadu Wedajo, Solomon Seyife Alemu, Melese Adugna Tola and Shelema Mengistu Teferi in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to acknowledge Madda Walabu University Sheshemene Campus for providing us with ethical clearance. In addition, our heartfelt thanks go to our study participants, data collectors, and supervisors.
Authors’ contributions
All the authors have contributed equally from proposal development to final manuscript development. Conceptualization: Lema Fikadu Wedajo, Solomon Seyife Alemu, Melese Adugna Tola, and Shelema Mengistu Teferi. Data Curation: Lema Fikadu Wedajo. Formal analysis: Lema Fikadu Wedajo. Investigation: Lema Fikadu Wedajo, Solomon Seyife Alemu, Melese Adugna Tola, and Shelema Mengistu Teferi. Methodology: Lema Fikadu Wedajo, Solomon Seyife Alemu, Melese Adugna Tola, and Shelema Mengistu Teferi. Project administration: Lema Fikadu Wedajo. Resources: Lema Fikadu Wedajo, Solomon Seyife Alemu, Melese Adugna Tola, and Shelema Mengistu Teferi. Software: Lema Fikadu Wedajo. Validation: Lema Fikadu Wedajo, Solomon Seyife Alemu, Melese Adugna Tola, and Shelema Mengistu Teferi. Visualization: Lema Fikadu Wedajo and Solomon Seyife Alemu. Writing: original draft: Lema Fikadu Wedajo. Writing (review and editing): Lema Fikadu Wedajo, Solomon Seyife Alemu, Melese Adugna Tola, and Shelema Mengistu Teferi.
Availability of data and materials
The data used for this study are available upon reasonable request from the corresponding author at any time if required.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical clearance was obtained from the Research Ethics Review Committee of Madda Walabu University College of Health Sciences, Sheshemene Campus, with reference number CBE/057/15. All methods were performed following the principles of the Helsinki Declaration.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from each study participant after they understood the nature and benefits of the study.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.