
Abstract
Despite epidemiologic studies demonstrating the increased incidence of paternal postpartum depression, their emotional health is overlooked throughout their partner’s pregnancy and postpartum period as postpartum depression has been traditionally construed as a disease of women. Traditional masculinity norms also result in a lack of recognition and barriers to the treatment of depression in men. This study is aimed to determine the prevalence and factors of paternal postpartum depression among fathers whose wives gave birth. A community-based cross-sectional study was conducted from July 7 to 17, 2023. The 288 sample size was estimated using a single population proportion formula and selected by random sampling technique. The data were exported from Kobo Toolbox and analyzed using SPSS version 26. Candidate variables were identified in bivariate at p < .25 for the multivariate analysis. A p < .05 and adjusted odds ratio (AOR) were used to determine the significance. A total of 280 partners participated making a 97.22% response rate. Paternal postpartum depression was 19.6%(95% confidence interval [CI] = [15.4%, 24.3%]). It was significantly associated with history of depression (AOR = 4.4, 95% CI = [1.7, 10.9]), unplanned pregnancy (AOR = 4.7, 95% CI = [1.9, 11.3]), alcohol consumption (AOR: 3.0, 95% CI = [1.3, 7.4]), infant sleeping problem (AOR: 3.0, 95% CI = [1.1, 8.9]), and mode of delivery (AOR: 3.0, 95% CI = [1.3, 7.6]). This study concluded that paternal postpartum depression was high. The researchers recommended the inclusion of men’s mental health services like screening into women’s postnatal health care.
Keywords
Background
Postnatal depression is a nonpsychotic depressive disorder that occurs after the birth of a child, and it has been defined as a “downward spiral” and a “living nightmare” (Wood et al., 1997). During the postnatal period, men’s health can be influenced by many factors, leading to a greater sense of personal responsibility. It is a critical time that requires adjustments and may pose a risk for depression (Wang et al., 2021).
It is well established that fatherhood has a long-term positive and protective effect on men’s health. However, there is evidence that indicates men’s condition can be complex and demanding during the postnatal period which can lead to distress, anxiety, and increased risk of experiencing paternal postpartum depression (Philpott & Corcoran, 2018; Wang et al., 2021; Zhang et al., 2016).
In 2020, the pooled prevalence of paternal postpartum depression among fathers was 9.76% worldwide during the first year of their childbirth (Rao et al., 2020). The Global Burden of Diseases Study analyzed the data from 17 low- and middle-income countries (LMICs) and indicated that the prevalence of paternal postnatal depression was 18.4% (GBD 2015 Disease and Injury Incidence and Prevalence Collaborators, 2016). In Addis Ababa, Ethiopia, the magnitude of paternal postpartum depression was 19.3% during the first 6 to 8 weeks of child delivery in health facilities (Tuji et al., 2023). Even though a significant number of men experience depression after the childbirth of their wives, this phenomenon mostly remained less exposed and persisted affecting men as well as their families adversely (Shariat et al., 2022).
Paternal postpartum depression affects not only the mental health and well-being of fathers but also their partners and children in different dimensions (Fisher, 2017). The consequences of paternal postpartum depression include continued depression of the father, partner relationship problems, negative parenting, infant bonding problems, and developmental effects on infants, toddlers, preschoolers, grade school children, and adolescents (Barry et al., 2023; Field, 2018). Depression experienced by fathers is related to the future emotional and behavioral problems of the children (Challacombe et al., 2023; Leiferman et al., 2021).
Several factors contribute to the development of paternal postpartum depression. These factors can be infant-related, paternal factors, maternal factors, and family factors. Paternal unemployment, low social support, paternal negative life events, perceived stress, financial strain, history of mental illness, wives’ parity, maternal postnatal depression, low marital satisfaction, and infants’ sleep problems increase the risk of paternal postpartum depression (Fang et al., 2019; Wang et al., 2021). Psychological and social factors such as stress during pregnancy or delivery and quality of adjustment to life changes are strongly related to paternal postpartum depressive mood disorders (Yim et al., 2015).
It was suggested that paternal postpartum depression screening should be an essential aspect of optimal care for the fathers and the entire family dynamic (Curry et al., 2019; Kennedy & Munyan, 2021). However, men’s emotional health is overlooked during their partner’s pregnancy and throughout the first postpartum year as postpartum depression has been traditionally construed as a disease of women. Furthermore, epidemiologic studies have demonstrated that the incidence of depression in men is markedly underestimated because of diagnostic bias where the men, the community, local health professionals, and researchers may also not consider men could suffer from postpartum depression unlike women (Eddy et al., 2019; Scarff, 2019). The majority of studies in Ethiopia also focused on maternal depression. There is a scarcity of studies on paternal postpartum depression (Asaye et al., 2020; Ayen et al., 2024; Zegeye et al., 2018). Traditional masculinity norms also result in a lack of recognition and barriers to the treatment of postpartum depression in men (Seidler et al., 2016; Staiger et al., 2020).
In sub-Saharan African countries including Ethiopia, there is low consideration of paternal postpartum depression and the previous researchers recommended further consideration of this case (Kerie et al., 2018). Little is known about paternal postpartum depression in Ethiopia. This study was proposed to determine the prevalence and associated factors of paternal postpartum depression among fathers whose wives gave birth in the last 6 months in Seka town, Southwest Ethiopia.
Method and Materials
Study Area and Period
This study was conducted in Seka Chekorsa Town in Jimma Zone, Oromia region of Ethiopia. It is located 20 km away from Jimma town, the Jimma Zone’s capital town, and 370 km from Addis Ababa the capital city of Ethiopia. According to population projection data, Seka Chekorsa District’s total population was 310,721 in 2023, whereas Seka Town’s population was 43,822. Of these, 25,476 were males and 18,346 were females. Seka Town has two urban Kebeles and two public health institutions. The study was conducted from July 7 to 17, 2023.
Study Design and Population
A community-based cross-sectional study design was employed. The study population for this study was all the randomly selected male partners whose wives gave birth and were living in Seka town during the study period. Partners were included in the study with the criteria of being partners of wives who gave birth within the preceding 6 months and living with the women since her conception.
Sample Size Determination and Sampling Technique
The sample size was determined using a single population formula: n = (Zα/2)2p(1 −p)/d 2, where “n” is the minimum required sample size, “Zα/2” is the standard score value for a 95% confidence level (CI) for two-tail normal distribution, “p” is the population proportion of paternal postpartum depression (19.3%) (Tuji et al., 2023), and “d” is the margin of error. Adding 20% for the nonresponse rate, the final sample size became 288.
A systematic random sampling technique was used to select the required sample size from source populations. The sample was allocated proportionally to each Kebeles based on the number of partners whose wives gave birth in the preceding 6 months. The data on the number the partners were obtained from the Town’s health management information system and each kebeles’ health extension workers’ folder. Based on the total number of deliveries in each kebeles, the sampling interval was calculated, and the sample was taken every two intervals after the selection of the first partner by lottery method.
Data Collection and Analysis
A structured interviewer-administrated questionnaire was adopted and adapted from relevant literature and translated into Afan Oromo—a language in the study area (Ayinde & Lasebikan, 2019; Cox et al., 1987; Wang et al., 2021). A pretest was performed in Shabe Sombo Town. One supervisor and three data collectors (two health extension workers and one BSc midwife) were trained for data collection. Data were collected from study participants at their homes through interview-administered face-to-face interviews using the Kobo toolbox software. The data were exported from the Kobo toolbox to Excel and then to IBM SPSS version 26 software for analysis.
Descriptive statistics were done to get frequencies, percentages, and cross-tabulations. The Hosmer–Lemeshow model fitness for goodness-of-fit test was checked. Binary logistic regression analysis was employed to identify candidate variables for multiple logistic regressions. Finally, the presence of an association of independent variables with paternal postpartum depression was declared at p < .05 with AORs at 95% CI in multivariable analysis.
Paternal postpartum depression was measured using the Edinburgh Postnatal Depression Scale, and the fathers were considered as having depression when they scored ≥10 (Edmondson et al., 2010).
Ethical Consideration
Ethical clearance was obtained from the Institutional Review Board (IRB) of Jimma University Institute of Health with the reference number JUIH/IRB/467/23. Informed verbal consent was obtained from all study participants. Verbal consent was taken considering that all the study participants were adults (aged at least 20 years) who could decide based on the given information, the study was focused on a nonsensitive topic, the study had no sample collection procedure (no specimens collection), and the researchers used an application for the data collection procedure. Before going for the verbal consent, the participants were informed about the objective of the study, possible risks (such as the time the interview might take), and the benefits of the study to themselves, their communities, and the researchers. After receiving this information, participants were allowed to ask questions or express any doubts. The main researcher’s contact information was provided for future reference. Finally, participants were asked if they agreed to participate in the study. When the men agreed to proceed, the data collector marked a “☑” next to the “Yes” option on the tablet for the question “Do you agree to participate in the study?” before going to the interview.
Participants were informed that the data would be kept private and confidential and used only for research purposes. The participants were also assured that they had the right to refuse or withdraw if they were not comfortable with the question at any time during the interview. Personal privacy was respected, and no personal identifier was used on the questionnaire. The study was conducted according to the IRB’s guideline.
Results
Socio-Demographic Characteristics and Paternal Characteristics
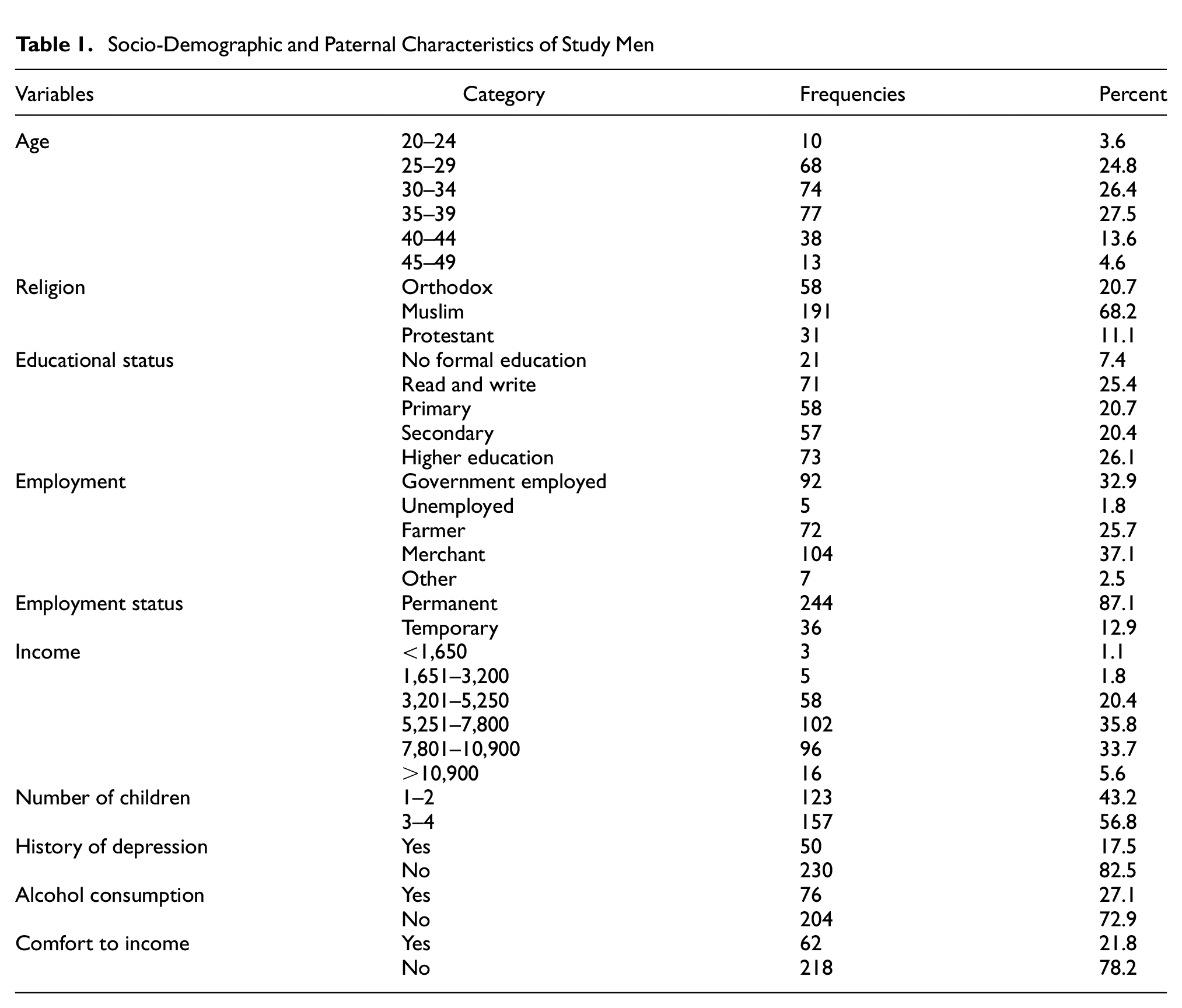
Two hundred and eighty partners successfully participated in the study making a response rate of 97.22%. About 159 (56.8%) of the partners have three to four children. Nearly one-third (76, 27.1%) of them consume alcohol, and 50 (17.5%) of them have a history of depression (Table 1).
Socio-Demographic and Paternal Characteristics of Study Men
Relationship-Related Characteristics
All of the partners were married and almost all of them 279 (99.3%) were living together with their partner, whereas only one partner (0.7%) was living separately during the data collection. Two hundred and sixty-nine (95.2%) partners were monogamous. Almost all of the partners 257 (90.2%) had a good relationship with their partners and support from friends 224 (79.4%) (Figure 1).

Relationship-Related Characteristics of Study Participants
Infant and Environmental-Related Characteristics
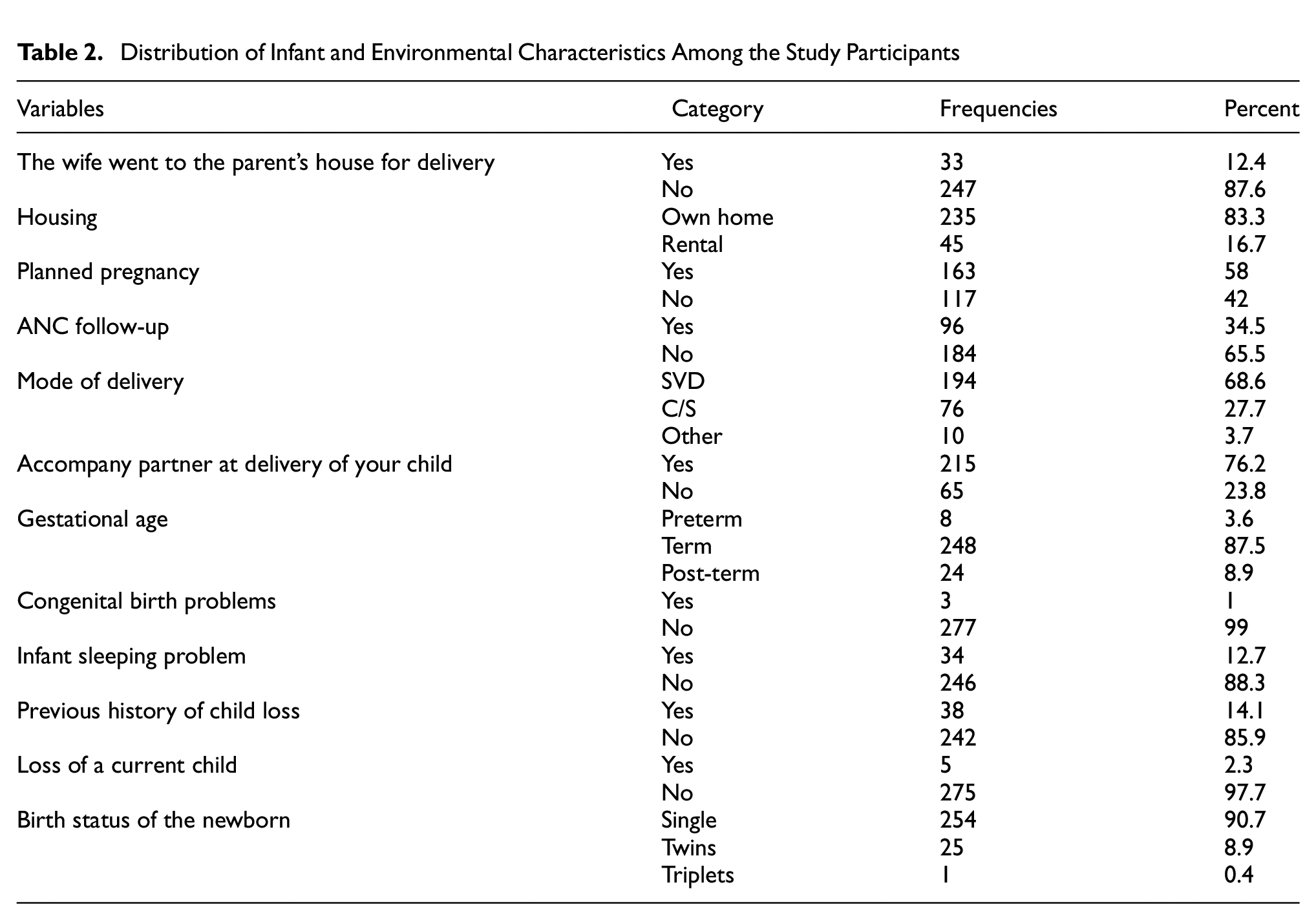
The majority of the partners 235 (83.3%) were living in their own homes. A rare number (33, 12.4%) of the respondents’ spouses delivered their babies at their mothers or families’ homes. Infant sleeping problems and current and previous child loss were 34 (12.7%), 5 (2.3%), and 38 (14.1%), respectively. Regarding the newborns, 254 (90.7%) of newborns were single, and 163 (58%) of pregnancies were planned. Infants born with congenital problems were three (1%) (Table 2).
Distribution of Infant and Environmental Characteristics Among the Study Participants
Prevalence of Paternal Postpartum Depression
The score of about one-fourth of the partners was above the cutoff point, and hence, the prevalence of paternal postpartum depression was 19.6% (95% CI = [15.4%, 24.3%]) (Figure 2).

Prevalence of Paternal Postpartum Depression in Seka Town, Jimma Zone
Factors Associated With Paternal Postpartum Depression
Bivariate analysis was performed to identify candidate variables for multivariate analysis at p < .25. Accordingly, variables such as birth status of the newborn, family income, comfort to family income, cigarette smoking, alcohol consumption, history of depression, chat chewing, relationship with parents, friend support, family support, number of wives, happiness to baby sex order, history of family mental illness, partner support, mode of delivery, gestational age, housing condition, unplanned pregnancy, attending antenatal checkup with a partner, infant sleeping problems, and child loss before the birth of this child were identified for multivariable model.
In multivariable analysis, five variables were significantly associated with paternal postpartum depression. Thus, partners who had a history of depression were about four times (AOR = 4.4, 95% CI = [1.7, 10.9]) more likely to have paternal postpartum depression than partners who did not have a history of depression. The odds of paternal postpartum depression were nearly five times higher (AOR = 4.7; 95% CI = [1.9, 11.3]) among partners of women who had unplanned pregnancies than their counterparts.
Partners who currently drink alcohol had three times increased odds of developing depression compared to partners who did not drink (AOR = 3.0; 95% CI = [1.3, 7.4]). In comparison to fathers who did not have newborn sleeping problems, the odds of paternal postpartum depression were three times higher among those whose newborn had sleeping problems (AOR = 3.0; 95% CI = [1.1, 8.9]). Partners whose wives delivered a child by cesarean section were three times more likely to develop paternal postpartum depression than those whose wives delivered by spontaneous vaginal mode (AOR = 3.0, 95% CI = [1.3, 7.6]) (Table 3).
Multivariate Logistic Regression Analysis Result of Paternal Postpartum Depression Among Partners of Women Who Gave Birth in the Last 6 Months in Seka Town

COR = crude odds ratio, AOR = adjusted odds ratio, 1 = reference variable.
Significant variables.
Discussion
This study planned to determine the prevalence and factors associated with paternal postnatal depression among partners of women who gave birth in Seka town, Ethiopia. A significant number (19.6%) of partners had symptoms of depression showing that a substantial number of partners were suffering from paternal postpartum depression. This finding goes in line with findings from studies conducted in different parts of the world, for example, 17% in Japan (Suto et al., 2016), 16.6% in Saudi Arabia (Shaheen et al., 2019), 17.8% in Nigeria (Ayinde & Lasebikan, 2019), 19.3% in Addis Ababa of Ethiopia (Tuji et al., 2023), and 19% in Ethiopia community-based studies (Ayinde & Lasebikan, 2019).
On the contrary, the finding of this study is lower compared to the paternal postpartum depression (28%) in Uganda (Huang et al., 2017). This difference could be due to the difference in the tool used to measure the partners’ depression status where this study used the Edinburg depression scale while the others used the Patient Health Questionnaire that was validated for Ugandan adults.
Factors Associated With Paternal Postpartum Depression
The finding of this study identified that partners who had a history of depression had a higher risk of experiencing paternal postpartum depression. This significance is supported by the study conducted in Japan (Suto et al., 2016). The association could be because stress and previous depression exacerbate and amplify depression. Paternal postpartum depression is more likely to occur in people with a history of depression (Qobadi et al., 2016). It was also concluded that stressed-out fathers were more likely to have depressive symptoms (Shariat et al., 2022).
Having unplanned pregnancies among wives was significantly associated with paternal postpartum depression. This finding is in line with a study conducted in Nigeria (Ayinde & Lasebikan, 2019). Unplanned pregnancy leads to unplanned delivery that can impact the social, economic, and cultural aspects of the modern life of the fathers (Brown & Eisenberg, 1995). Unplanned pregnancies can lead to an increased risk of mental health issues in fathers after childbirth as it can impose an identifiable risk for mental health problems (Smith et al., 2023).
The odds of paternal postpartum depression were significantly higher among alcohol-consumer partners. This might be because drinking alcohol affects the brain in many ways, and it is likely to cause and aggravate feelings of depression during intoxication and the subsequent withdrawal (Tipple et al., 2016).
Partners having an infant with sleeping problems were more significantly faced paternal postpartum depression. This result is consistent with the findings of studies conducted in Ireland (Philpott & Corcoran, 2018) and Western China (Zhang et al., 2016). Infant sleeping problems can be a problem for the fathers not to sleep enough during the postpartum period. Also, the partners may become worried about the healthiness of the child, and this might cause them to develop depression. The sleeping problem can be the exacerbator, relapsing factor, and symptoms of depression in human beings (Fang et al., 2019). The links between infant sleeping problems and parents’ postpartum depression are bidirectional and dynamic, so poor infant sleep may influence parental behaviors and poor infant sleep appears to be a family stressor and a risk factor for depression (Fang et al., 2019; Meerlo et al., 2015; Symon & Crichton, 2017).
This study revealed that the partners of wives who gave birth by cesarean section were more likely to have paternal postpartum depression. Evidence also indicates that any type of cesarean section delivery increases the risk of family postpartum depression (Xu et al., 2017). Cesarean section delivery increases the risk of postpartum depression by violating expectations about childbirth (Lobel & DeLuca, 2007).
Limitation
Although our study offers unique insights into how postpartum depression can affect partners of women who gave birth, the data collection method, which involved interviewer-administered questionnaires, may have introduced bias. While our study relied on an important study area in the country, these data are limited from sorting the study population into first-time fathers and those that fathered many children, the early period after child delivery, and lately, at 6 months.
Conclusions
Paternal postpartum depression within 6 months of child delivery was high among partners whose wives gave birth in Seka Town. Alcohol consumption, having a previous history of depression, unplanned pregnancy, having a child with an infant sleeping problem, and mode of delivery are an identified significant predictor of paternal postpartum depression in the study area. The authors like to recommend research that explores the lived experiences of fathers with paternal postpartum depression including their coping mechanisms. Also, it is recommended for the consideration of postnatal follow-up that includes mental and reproductive health screening and counseling services for fathers and to create awareness about postnatal depression among the fathers of newborns where possible.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclosed that the first author received a small amount of funding for data collection from Jimma University.