
Abstract
People suffering from rheumatoid arthritis are normally prescribed with physical exercises. The realization of these exercise routines should be supervised to prevent wrongly adopted postures or bad movements that end up harming the affected articulations. The motivational component associated with a supervised session is also important. On the contrary, having access to qualified supervision is not always possible due to different reasons, such as tight schedules, limited mobility, or economic reasons. This article presents a system for at-home rehabilitation, based on Microsoft Kinect, that resembles the role played by the physiotherapist during the supervision of an exercise session. The system not only supervises the realization of exercises but it also collects and manages information about the exercise-session history. Additionally, and despite affecting young people, rheumatoid arthritis is a disease that mainly affects seniors. For this reason, the system provides a natural interface to ease the interaction. Finally, the performance of the proposed system has been evaluated using a three-dimensional dynamic measurement system as a gold standard to validate the accuracy of the measurements. Obtained results demonstrate the potential of the Kinect-based system for at-home rehabilitation exercise routines.
Keywords
Introduction
Rheumatoid arthritis (RA) is one of the most common musculoskeletal disorder affecting up to 1% of the general population worldwide. 1 This disease causes joints to be swollen leading to ankylosis. This systematic inflammation not only leads to morbidity and long-term disability but also to an important burden in terms of societal and economic cost to both patients and health services. 2
RA patients tend to bend damaged joints, adopting a more comfortable and less painful position. However, after being bent for long periods, returning them to their original state might not be possible due to muscle shrink. To avoid this situation, RA patients should maintain an adequate level of physical activity. In this sense, RA patients are normally prescribed with a pharmacological treatment to deal with pain as well as an exercise routine that will help them to reduce pain, stay more energetic, and reduce weakness while preventing accidents due to their lack of agility. 3
Exercise routines are normally prescribed and supervised by a physical therapist. Daily routines are unfeasible for many patients due to the economic cost, time constraints, and the impossibility to travel to a health center on a daily basis. Nevertheless, unsupervised realization of exercise routines is neither a good solution since it could be ineffective or unsafe. 4 Unsupervised activities could lead patients to adopt inappropriate corporal poses that might damage joints. There is, therefore, a trade-off between the need for supervision and the comfort and convenience of exercising at home. Despite the demonstrated benefits derived from physical therapy, 5 patients continuation of this type of treatments dramatically drops with time, especially when they are performed in an unsupervised manner. 6
The use of computer-aided rehabilitation systems has attracted much attention from the research community.7–12 Not so long ago, the main inconvenience that had to be addressed when automating any aspect related to human kinetics was the high cost involved in the required hardware and the participation of trained staff. This barrier has been eliminated to some extent since Microsoft Kinect was launched for the video game industry in 2010 and the release of a software development kit (SDK) that opened up the possibility of developing new applications based on it. Moreover, wearable technologies are also opening new lines of research, such as those based on foot pressure sensor analysis, 13 which could be used for body posture analysis in combination with depth and RGB images.
The work of Hondori and Khademi 14 reviews the impact of Kinect on physical therapy and rehabilitation. Regarding skeletal tracking, despite the increase in accuracy when compared with systems based on RGB images, Kinect struggles under occlusions or noisy environments, as pointed out by Hondori and Khademi. 14 Still, same authors conclude that Kinect accuracy is acceptable for rehabilitation purposes. Similarly, the work in Webster and Celik 15 presents a review of the use of Kinect for elderly care and stroke rehabilitation, paying special attention to the spatial accuracy, rehabilitation methods, and limitations. Webster and Celik 15 conclude that, in general, Kinect has a significant potential to be used as a cost-effective solution for motion capture systems in the context of rehabilitation.
Several applications based on Kinect have been presented in recent years. A system for gait assessment in people with a stroke is presented in Clark et al. 16 The work in Galna et al. 17 is intended for people with Parkinson’s disease and proposes a rehabilitation method based on a video game to enhance motivation among users, while providing a preliminary assessment of user’s safety. Postural stability is shown to be enhanced in individuals with Parkinson’s disease according to the results presented in Shih et al. 18 after an exergaming intervention using Kinect.
Despite the promising results obtained from state-of-the-art systems for rehabilitation support, therapists cannot be totally relegated from the process once the exercise routine has been prescribed. On the contrary, they have to be kept in the loop to monitor and assess the patient performance and motivation as well as to prescribe appropriate changes in the routine and assess the advances. 12 Motivation plays an essential role not only on determining adherence to the rehabilitation routines 19 but also on its outcome. 20 In fact, identified barriers to treatment adherence 21 evidence the importance of therapist supervision in the early identification of such barriers. The work in Colombo et al. 22 refers to the awareness of the performance obtained and the quantity and quality of the feedbacks as elements that can influence the patient motivation. In Cameirão et al., 23 strategies based on gaming and coaching are analyzed for at-home stroke rehabilitation.
Motivated by the need to combine the benefits of at-home rehabilitation and therapist supervision, as well as trying to maximize the performance awareness and the feedback provided to patients, this work proposes a system, known as ArthriKin, based on Microsoft Kinect, a low-cost depth camera. The system is intended to supervise and provide real-time feedback, similarly to what a therapist would do during a session. In addition, the proposed system keeps records of the patient activity, enabling therapists and doctors to assess their progression over time.
The ArthriKin system
ArthriKin is intended to supervise the execution of exercise routines while providing real-time corrections when deviations in trajectories or body poses are detected. The proposed system, as depicted in Figure 1, comprised a set of modules that can be analyzed from the main stages they intervene in, which are known as
The data acquisition module, which uses the depth camera (in this case Microsoft Kinect) to record body movement.
The natural interface module, employed for user interaction and for guiding patients through the exercise routine, correcting them when deviations are detected.
The activity data logging module, in charge of recording the patient performance during the exercise session, enabling afterwards the medical staff to supervise patient performances.
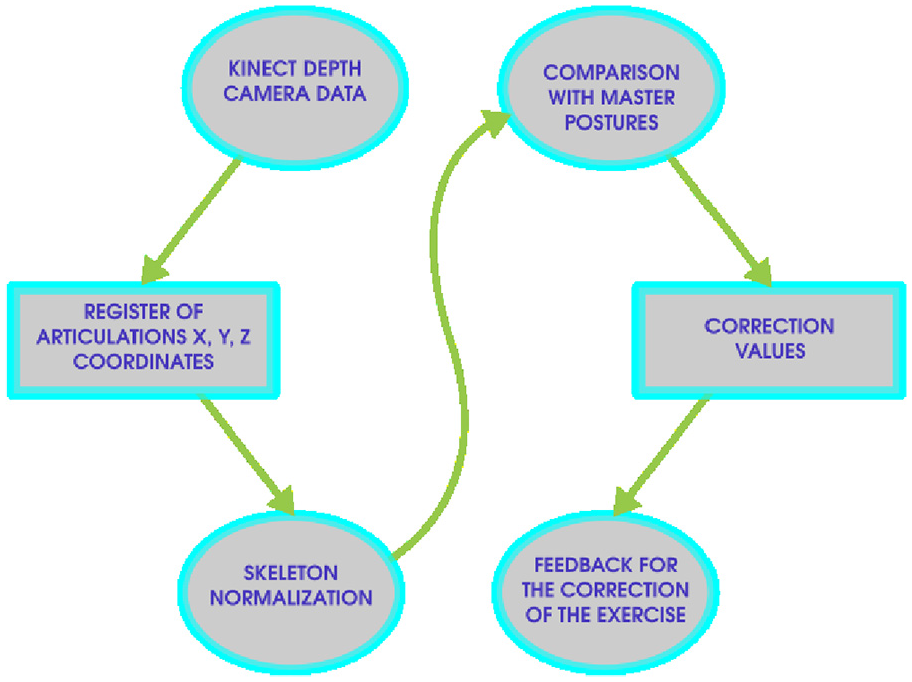
Stages involved in the ArthriKin architecture.
Data acquisition
This module is responsible for recording the different body postures adopted during the execution of the exercise routine. The implementation of this module has been achieved by resorting to the Microsoft Kinect SDK to extract the skeletal features of the captured posture for each frame. These features, as depicted in Figure 2, consists in the three-dimensional (3D) points representing the position of each one of the considered skeleton joints.

Skeleton representation. The circles in the skeleton represent joints.
Pose representation
ArthriKin is based on the skeleton information provided by the Microsoft Kinect SDK. This information, however, has to be conveniently parsed and stored so that representative features can be easily extracted. XML files are employed to track the position and orientation of the 20 joints comprising the skeleton. Moreover, additional information such as the frame number, the detected user ID, and the timestamp are also recorded.
The execution of a certain exercise will generate a collection of XML files that should be conveniently stored. A NoSQL database, namely eXist DB (http://www.exist-db.org/), has been employed for persistence purpose.
Calibration
During the calibration process, different measures are carried out in order to adapt the exercise routine to the particular body characteristics and the environment. This process is especially important for patients performing the exercise routine from a wheelchair due to the distortions introduced in the body posture in those cases.
The calibration is carried out in a two-stage process. First, the camera records a set of frames during the initial 5 s. From each frame, the body pose is represented as a skeleton and parsed in an XML file. After this initial stage, the following points, as depicted in Figure 3, are computed:
Inner point. It refers to the internal point of the limb. If the exercise involves an arm, this refers to the shoulder. If it involves a leg then, the inner point refers to the hip.
Middle point. In this case, the middle point of the arm refers to the elbow, whereas for a leg it refers to the knee.
External point. This refers to the hand in the case of an arm and the foot in the case of a leg.
Floor. This measure identifies the floor position based on the foot position.

Lower and upper limb points.
This stage results in four different vectors of points, corresponding to each tracked limb. From every vector, the mean point is calculated and considered as the reference one. Considering more than one measure helps overcoming periods of loss of skeletal tracking, the presence of noise, or small movements.
During the second stage, the limb length is calculated. Some users might find it difficult to take their limb to a complete extension, due to the effects of the disease. Therefore, the length



Determination of the areas of relevance
The type of exercises prescribed to RA patients mainly involve those related to the range of motion 3 (see Figure 4). These exercises are intended to improve and preserve the health of the joint as well as its range of movement. Every prescribed exercise is therefore going to focus on a specific limb or part of the body. Based on that, we define an area of relevance as the space range in which a certain joint is expected to be constrained during the exercise execution. In order to calculate these limits, during the training stage, the physical therapist is recorded while performing a correct execution of the exercises. The data gathered are post-processed to identify, in first place, the limbs or body parts involved in the exercise and the boundaries within which a safe and correct execution of the exercise is achieved.
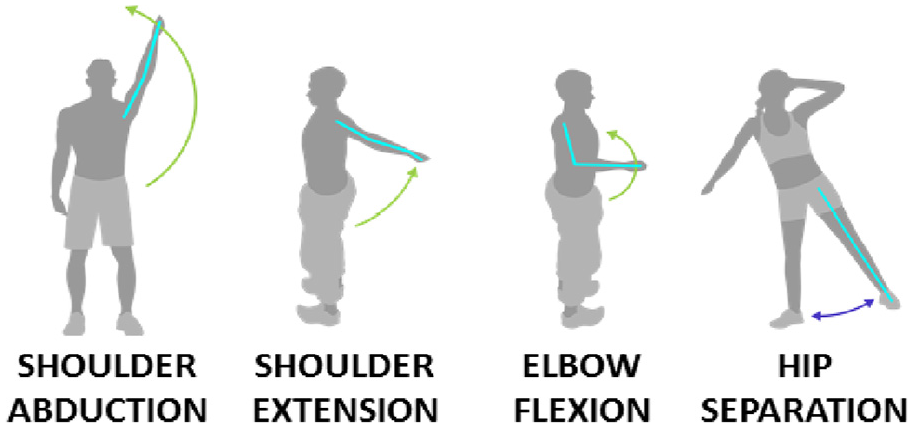
Exercises considered in ArthriKin.
The identification of the limbs or body parts involved in an exercise is carried out implementing an approach based on the space-time interest points (STIP) proposed in Laptev
24
that has been extensively used in computer vision systems for scene recognition. Similarly to what the STIP algorithm proposes, our system observes the skeleton joint positions during the exercise execution. From the obtained data, those joints showing a high variation in any or several dimensions (
Figure 5 represents the hand position in coordinates

Hand position in
As it can be observed from the
Despite dealing with 3D points, ArthriKin provides feedback to users in a two-dimensional (2D) space, by means of an arc that represents the trajectory (with the maximum and minimum points) that the patient should stick to (see Figure 6). This decision was adopted for the sake of feedback simplicity. For this reason, depending on the exercise, the patient should adopt a position facing the camera or sideways to it.

Trajectory to be followed by the patient represented as an arc.
The shoulder abduction exercise, depicted in Figure 6, for instance, has to be carried out facing the Kinect, which means that the area of relevance to be controlled is parallel to the device (in the
Exercise routine supervision therefore relies on having identified the limits that fall into a normal and correct execution of the exercise. The maximum and minimum point calculation should also be normalized so that they can be adapted to different users (i.e. different heights or arm lengths). This adaption process is especially important for those users in wheelchairs. Depending on the exercise, areas are extended to consider the space taken by the wheels. In the case of the shoulder abduction exercise, for example, the minimum point is adapted to consider the armrest of the chair.
Control of the exercise execution
The supervision of the exercise execution depends not only on the identification of the area of relevance for a given exercise, but also on performance (P) achieved. The area of relevance states the exercise safety limits, including the maximum and minimum point that should not be overpassed. On the other hand, the performance is used to monitor the degree of achievement and guide the user through the exercise execution by providing visual feedback using a color code (see Figure 10) or counting repetitions, whenever a trajectory described by the limb reaches a certain minimum. Figure 7 graphically identifies different levels of performance for the shoulder abduction exercise. Performance for the axes of interest is calculated as follows


where, for a given limb, such as an arm or a leg, the inner

Performance in
Yet, there are some exercises in which the performance depends on the angle formed by the extremity and the body torso, like in the shoulder or hip extension exercises (see Figure 8). The performance, although also stated in %, should be calculated considering that angle, as follows

where


Performance calculation
The control of the exercise execution also involves the repetition counter. There are several issues that have to be addressed in order to count repetitions, such as dealing with situations in which low span of movements is achieved and assuring that a correct posture has been maintained throughout the execution of the exercise. Particularly challenging are those patients that workout from a wheelchair, mainly due to the armrest position. Moreover, it has to be checked that limbs are extended and performance in
The determination of the exercise performances is very important when monitoring the progression of the patient over time. The analysis of the resulting performance values can provide relevant information to detect patients going through an RA 25 and when assessing the benefits of certain exercise routines.
Natural interface interaction
RA is a disease whose prevalence increases with age, with an average onset at the age of 55. 26 This means that the majority of potential users of the proposed system will unlikely be familiar or confident with technology. In this sense, if this system is to be used without supervision, we must pursue users’ self-sufficiency when interacting with the system.
In this sense, ArthriKin has paid special attention to ease system interaction and keep the user experience as close as possible to interacting directly with a therapist. The natural interface interaction provided by the system is based on three main aspects: gesture control, voice commands, and visual representation of exercise trajectories.
Gesture control
The system is designed to be operated without any classical peripheral device (mouse or keyboard). The user will control the application by using a natural interface, thanks to the gesture control implemented in ArthriKin.
Hands are our natural interface when operating with an object. Similarly, the Graphical User Interface (GUI) of ArthriKin has been designed to be manually operated using the depth camera to detect when a hand is simulating a pressing action over a GUI button. Rather than using the mouse arrow to represent the location of the pointer, a hand is employed. The hand is gradually filled in purple as the hand pushes forward pretending to click a GUI button, as observed in Figure 9.
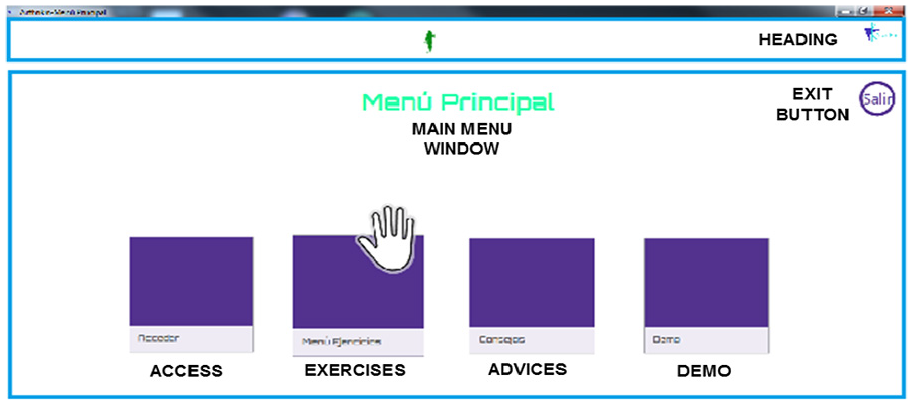
Natural interaction with the GUI by pressing buttons with the hand.
Voice commands
The system provides the user with voice command feedback, pretending to be a therapist. The following commands will guide the user through the exercise set up and execution:
Starting calibration. This message announces the start of the 5-s calibration process during which body and context features are gathered to adapt the exercise-execution model to the user.
Starting exercise. After this message, the user can proceed with the performance of the exercise. A visual representation of the articulation trajectory will also appear on the screen guiding the user through the execution.
Please, try to keep your arm parallel to the body. This message indicates that a deviation from the execution model has been detected. In order to prevent any harm, this message prompts the user to correct the body posture.
Please, try to keep your leg parallel to the body. Similar to the previous command, this one is intended to correct the position of the leg with respect to the body.
Repetition counter. Once a repetition is completed, a message is issued indicating the repetition number (i.e. one, two, three, etc.).
Exercise finished. Every exercise is configured to complete a number of repetitions. Once the repetitions have been achieved, a message announces the end of the routine.
Visual representation
The system provides real-time feedback to the user about the safe maximum and minimum points as well as the trajectory the arm or leg has to follow for a given exercise. In Figure 6, a green semicircle can be observed, with three bullet points indicating the maximum and minimum points and the current position of the hand.
It is worth mentioning that a color legend is also employed to provide the user with visual feedback about the performance or the deviation degree. Figure 10 shows the use of this color legend. The performance degree is represented using a color scale that ranges from red (at the minimum point) to green (at the maximum point). Then, the yellow color is employed to warn about a deviation from the area of relevance of the exercise. Similarly, the black color indicates that the exercise limits have been overpassed (either by the maximum or minimum points).

Color legend devised to provide feedback about the performance achieved.
Activity record
ArthriKin is not only intended to support the RA patients in implementing a daily and safe exercise routine at home but it is also aimed at collecting, storing, and processing data about those routines. Relevant information can be inferred from that data, and it can eventually help the therapist and the doctor to adjust and personalize the treatment prescribed to every patient.
The system records information about patients, exercises, and detailed information about daily routine executions. XML files are employed to record information so that more advanced searches and data processing can be eventually supported. Currently, the system implements statistical functions that provide information about the maximum or minimum points reached or the average level of performance.
The system also offers the possibility of obtaining graphical representation of the stored information from where relevant conclusions can be easily spotted, such as a sudden reduction in performance due to an RA crisis or the steady improvement on flexibility based on the maximum achieved points, for example. Figure 11 shows the maximum, minimum, and mean point achieved during the execution of the shoulder abduction exercise in five different days. The graphical representation of results offers a flexible configuration from where to choose the exercise type and daily records of different patients.
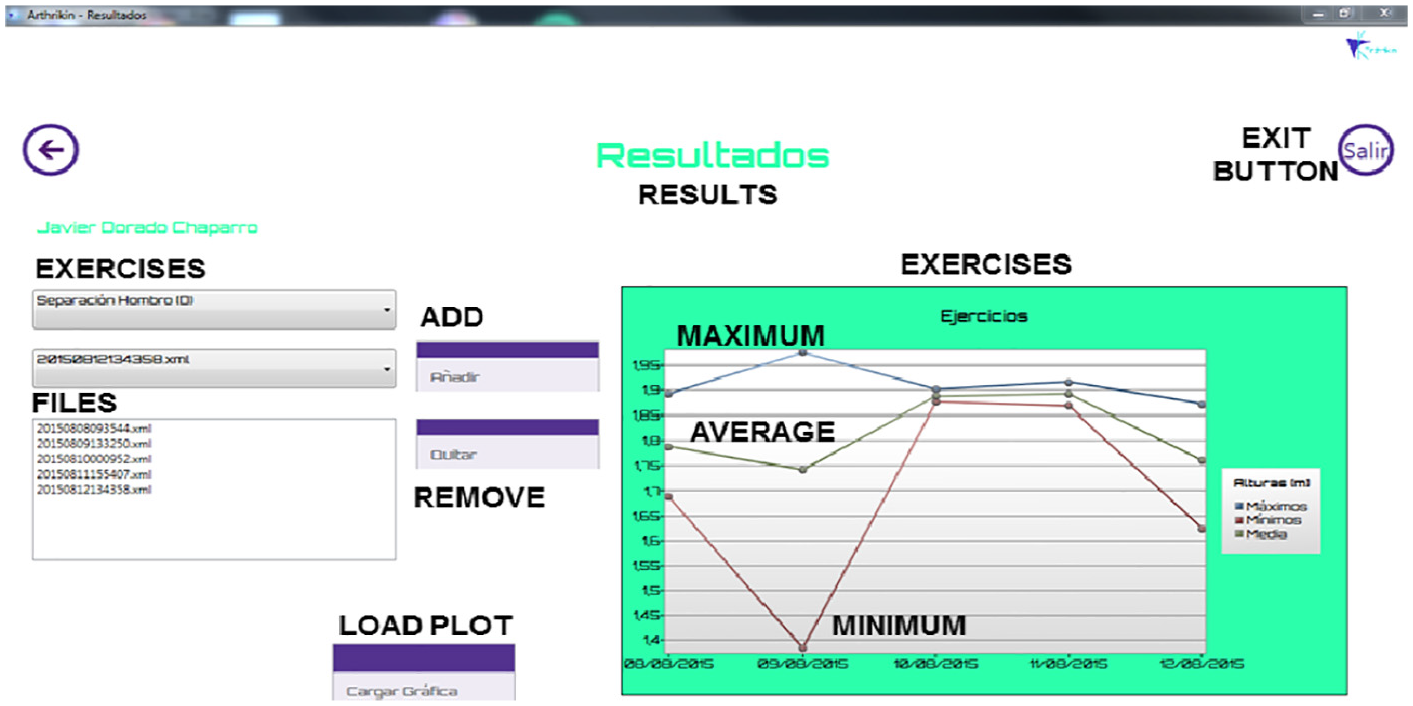
Representation of the activity record history.
Future work is intended to explore machine-learning techniques to determine whether some correlation exists between the data, the progression of the disease, and some other factors related to the patient state (stress, style of life, etc.).
System evaluation
The benefits derived from a continuous exercise program in people with RA have already been reported in previous works.5,27 Despite the fact that the proposed system has been initially devised for people with RA and the list of exercises is intended for RA rehabilitation, its application has the potential to be extended to supervise other types of rehabilitation routines. The preliminary approach adopted to evaluate the proposed tool presented in this article has therefore considered a more general scope than just evaluating the benefits of the intervention in people with RA.
The initial working hypothesis was that a computer-based tool with motion capturing, as ArthriKin, can be an efficient tool for at-home rehabilitation and remote assistance and supervision by a physiotherapist. To validate this hypothesis, we have analyzed the system suitability and efficacy on the basis of three different dimensions:
The physiotherapist motivation to use the system and be assisted by a computer-based tool.
The system accuracy when tracking the movements of the body during exercises.
The system usability when people use the tool.
Motivation evaluation
The physiotherapist motivation to use the proposed system is measured using a selection of 26 items from the Intrinsic Motivation Inventory (IMI) questionnaire. 28 This instrument has been previously used in rehabilitation contexts. 22 The original questionnaire comprised 45 items organized into seven subscales: interest/enjoyment, perceived competence, effort/importance, pressure/tension, perceived choice, value/usefulness, and relatedness. According to Ryan and Deci, 28 the intrinsic motivation per se is measured by the interest subscale although the perceived competence is considered to be related to it. The perceived choice is also considered a positive predictor of both self-report and behavioral measures of intrinsic motivation; however, pressure/tension is handled as a negative predictor. Effort is used in some questions, if relevant, so it is a separated variable. The value/usefulness subscale is related to the idea that people internalize and observe those experiences that they find useful for themselves. 29 Finally, the relatedness subscale is used in studies considering interactions between people.
Previous studies mention that the effects of the order of items appear to be negligible, and the inclusion or exclusion of specific subscales does not seem to have any impact on the others. Another important issue is the redundancy, because items within subscales overlap notably, although the fact of randomizing their presentation makes it less relevant for most participants.
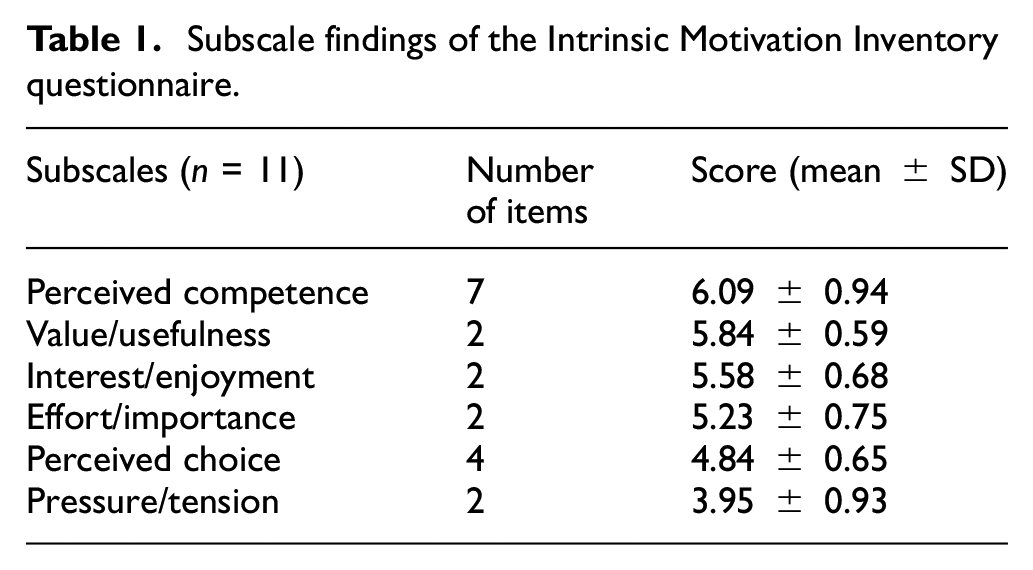
In order to evaluate the intrinsic motivation, we proposed an IMI questionnaire of 26 items to 11 physiotherapists who were previously introduced to the tool. The number of items of the each of the six subscales considered is shown in Table 1 (discussed later).
Subscale findings of the Intrinsic Motivation Inventory questionnaire.
Accordingly to the authors of self-determination theory, we randomized the IMI items. Each item was evaluated in a range between 1 (not at all true) and 7 (very true). There were 6 reverse score items, so if the physiotherapist for instance assigned a score equal to 1, the score was subtracted from 8 and therefore transformed into 7.
Accuracy evaluation
The evaluation of the proposed system based on Kinect has been carried out by comparing the obtained measurements with a high-accuracy 3D measurement system that is used as a gold standard. In this case, a Krypton K-400 dynamic measuring machine manufactured by Metris N.V. (nowadays Nikon Metrology N.V.) 30 has been used for this purpose. The main characteristics of this system are shown in Table 2.
Krypton K-400 (Metris M.V.) characteristics.

Four different exercises were proposed by a physiotherapist, considering the most commonly used exercises during a person-to-person rehabilitation session. These exercises, as depicted in Figure 4, were recorded simultaneously by the Kinect- and the Krypton-based systems.
The Krypton-based system employed three infrared (IR) cameras and IR light emitting diode (LED) markers (LED1, LED2, and LED3) placed in the measurement points. The measurement setup is depicted in Figure 12, showing the relative position of the Krypton and the Kinect systems, as well as the coordinate systems associated with them (

Measurement setup (position of the Kinect system in x′y′z′ coordinates: x′ = −374 mm, y′ = 171 mm, and z′ = −1714 mm).
Three IR LED markers were used for each exercise. Two of them (LED2 and LED3) were placed in the joints of interest for each exercise, according to Table 3. The remaining marker was placed in the origin of the Kinect coordinate system to capture the relative position between coordinate systems for post-processing purposes.
IR LED marker positions for each exercise.
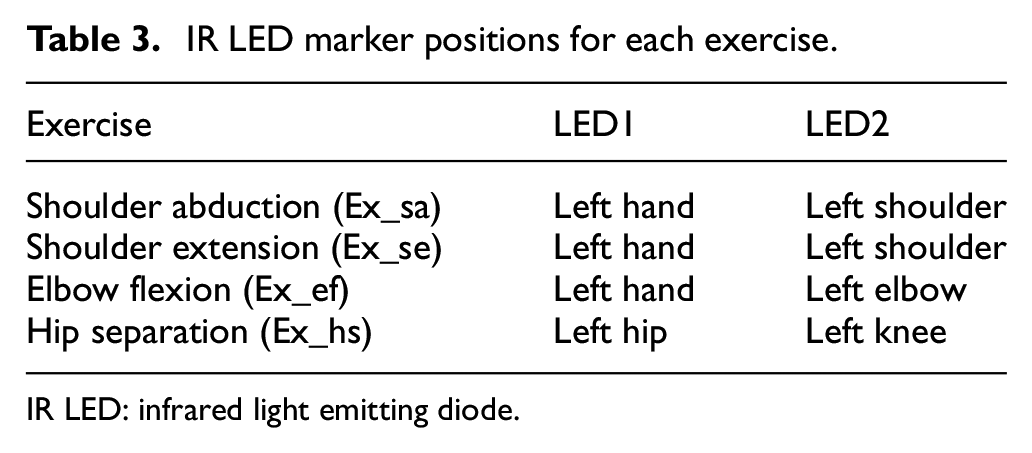
IR LED: infrared light emitting diode.
Once the measurements were captured for each exercise, the data obtained with the Krypton and Kinect needed to be post-processed in order to obtain the position errors. The post-processing stage was been carried out using Matlab and it consisted of the following steps:
Parsing of the Kinect XML files and the Krypton mat files.
Segmentation and synchronization of recordings.
Resampling to 150 Hz as common sampling frequency (Kinect works at 30 fps).
Transformation to a common coordinate system (Krypton coordinates
Error computation.
Usability evaluation
The guidelines established by ISO/IEC 9126-4 have been used to evaluate the usability of the system. The ISO 9241-11 standard provides a guide to understand usability. This standard defines usability as “the extent to which a product can be used by specified users to achieve specified goals with effectiveness, efficiency and satisfaction in a specified context of use.” As we can see in the definition, usability is not a one-dimensional magnitude, but rather a combination of different measures or factors. The ISO/IEC 9126-4 standard recommends that usability metrics should include the following three properties:
Effectiveness, defined as “the accuracy and completeness with which users achieve specified goals.”
Efficiency, which refers to “the resources expended in relation to the accuracy and completeness with which users achieve goals.”
Satisfaction, defined as “the comfort and acceptability of use.”
The effectiveness (

where
In addition, the number of errors that the participants had in the completion of the set of tasks was counted. Any omission, slips, or mistake in the execution of the task was counted as an error.
Regarding the efficiency assessment, it requires measuring the time that has been consumed to complete the task. Efficiency can be calculated based on time or as the overall relative efficiency.
Time-based efficiency

where
The overall relative efficiency
Finally, satisfaction was measured by questionnaires that are completed after each task (Task Level Satisfaction) and/or after the usability session (Test Level Satisfaction). In our case, we selected the Single Ease Question (SEQ) to evaluate each task and the System Usability Scale (SUS) to evaluate the user’s satisfaction with the system.
In order to evaluate the usability of the system, 20 volunteers with ages between 13 and 52 years participated in the study. Among the volunteers, there were 7 women and 13 men with different levels of education and different professions, each of whom had different experiences with technology. Each volunteer was asked to complete 15 tasks, and for each task, it was recorded the time needed to complete the task, the errors made, and whether they completed the task successfully. Volunteers were also asked at the end of each task about the level of difficulty they experienced completing it (SEQ). Finally, the participants were asked to complete a final satisfaction test (SUS).
Results and discussion
Motivation
The IMI questionnaire with 26 questions was completed by 11 physiotherapists and the mean values and standard deviations of the scores in each of the 6 subscales selected were calculated. These values are shown in Table 1.
As it can be seen, the standard deviation of each of the subscales is low, which means that a high level of agreement is found in the scores given by the different physiotherapists. Furthermore, it can be observed that all subscales are above 4, which corresponds the medium value of the scoring scale that goes from 1 to 7, except for the Pressure/Tension subscale which has a mean value of 3.95.
The best-rated subscale is perceived competence, indicating that physiotherapists felt they would be very capable of using the tool. Value/Usefulness also scored high, so it can be inferred that they find the tool very useful for the rehabilitation purpose. Furthermore, the score obtained in Interest/Enjoyment indicates that the use of the tool is interesting for them.
The score obtained in Effort/Importance and Perceived Choice subscales suggests that the professionals who took part in the study would make an effort to set up the tool and its use, in some cases for their own interest, but in other cases they would need some additional stimulus to adopt the new tool. This result is not surprising, since as in other sectors there are many people who are reluctant to use new technologies and embrace the changes they entail.
Finally, the Pressure/Tension subscale scored low, meaning that professionals believe they would not experience moments of pressure and tension while using the tool. In order to clearly illustrate the aforementioned results, Figure 13 shows a box plot of the motivation results by subscales.

Box plot with the IMI results.
Accuracy
As an illustrative example, Figure 14 depicts the performance of the proposed system, in terms of accuracy, for the shoulder abduction exercise obtained by both systems (Kinect and Krypton) after the post-processing stage.
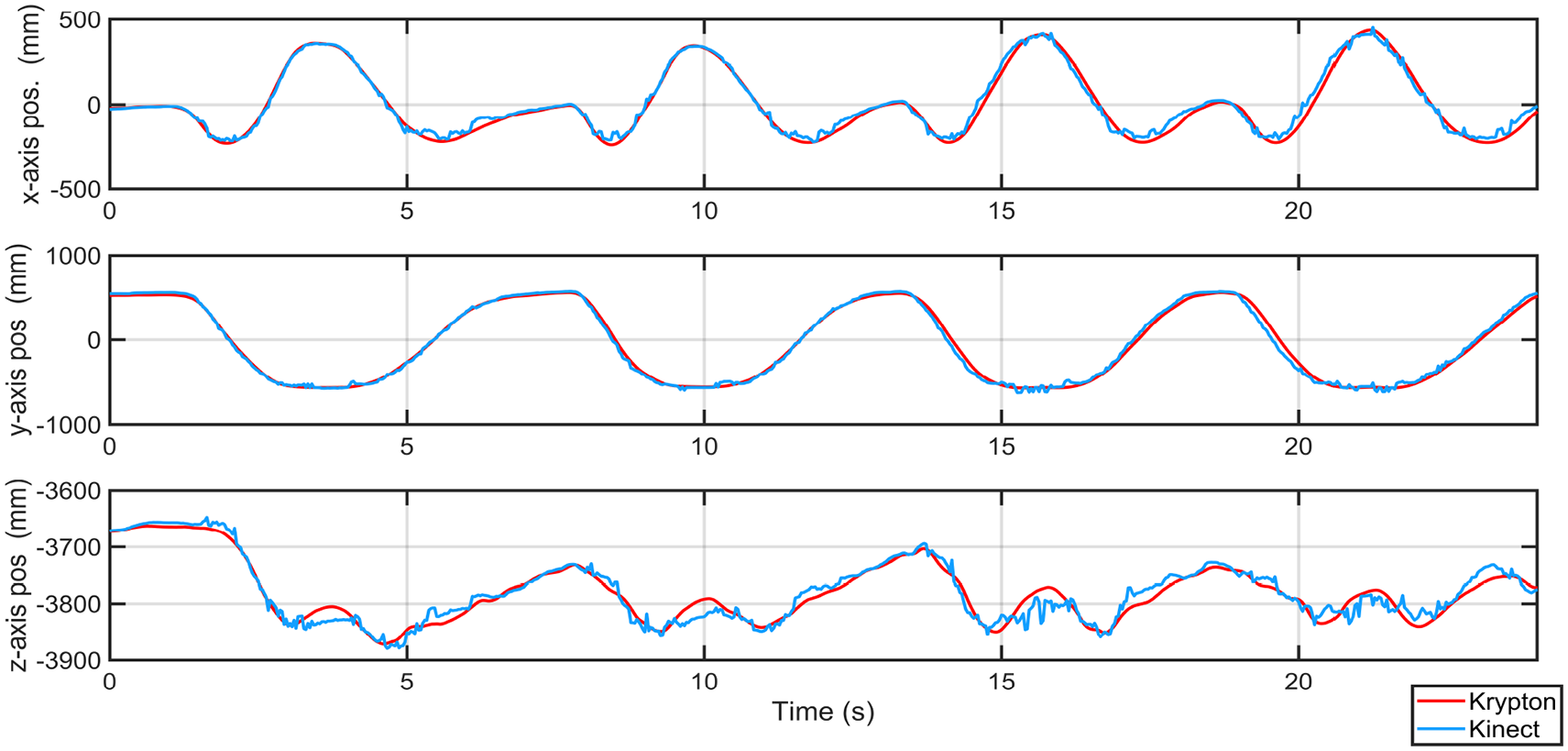
Left hand position measurements with Kinect and Krypton systems for the shoulder abduction exercise.
The assessment of the performance obtained with the Kinect-based system is based on the statistical analysis of the measurements and errors obtained from the comparison with the Krypton-based system. This statistical analysis is divided into the calculation of basic descriptive statistic values (root-mean-square error, mean absolute error, standard deviation) and the agreement between the two measurement techniques and reproducibility, which is evaluated by means of Pearson’s correlation coefficient and Lin’s Concordance correlation coefficient. This analysis is suitable for the validation of the Kinect-based system according to the study presented in Springer and Seligmann 31 for gait assessment. The results obtained for the different exercises are summarized in Table 4.
Statistical analysis (measures in mm).
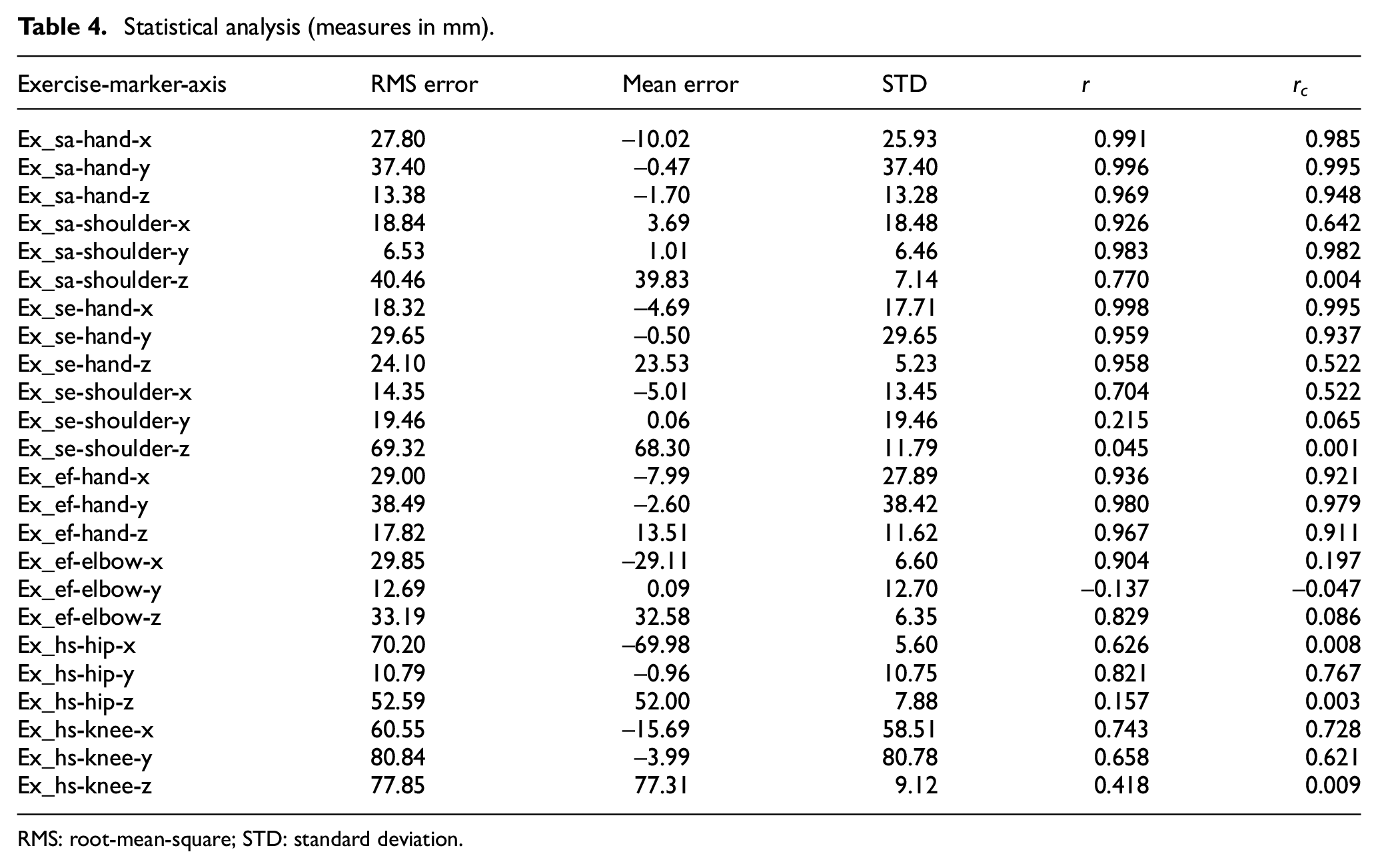
RMS: root-mean-square; STD: standard deviation.
The overall mean value of the root-mean-square (RMS) errors for all the exercises, joints, and dimensions is 34.93 mm. Correlation values for
In general, our results are in agreement with the work presented in Webster and Celik, 15 where the spatial accuracy of Kinect-based rehabilitation solutions is reviewed, and it is concluded that “the Kinect has been found, in general, to carry significant potential for a cost-effective motion capture system for rehabilitation.” Our results support the conclusions in Webster and Celik: 15 “Kinects ability to accurately capture upper extremity movements is consistently reported as sufficient for clinical use with regards to the elbow and wrist joint tracking; however, mixed results have been reported for the shoulder.” Similarly we have obtained less accurate results regarding the position of the hip. It should also be noted that the accuracy levels required depend on the type of exercise to be done as Zhao et al. 32 suggests, and the minimum accuracy level for a certain exercise has to be established with the participation of experts.
Usability
During the usability tests, each of the volunteers completed a set of 15 tasks with the ArthriKin tool to determine the usability of the system.
First of all, in order to assess the effectiveness of the system, it was analyzed for each proposed task whether it was completed or not and how many errors were made during completion. All users completed the proposed tasks, so the completion rate was 100%. Nevertheless, if we look at the error rate to be more accurate in terms of efficiency, 75% of users had less than 25% errors when performing all tasks, 20% of users obtained between 25% and 50% errors, and only one user was above 50% errors. Overall, an 18% error rate was achieved for all the tasks, which is a considerably low rate, and in spite of these errors, users were not prevented from successfully finishing all the tasks.
Regarding efficiency, it was necessary to know how long it took users to complete each task, if completed. The time-based efficiency calculation indicates the rate of goals achieved per second. This measurement is useful in the context of incorporating improvements to the tool and assessing the benefits in terms of efficiency. It is important to see that as Figure 15 shows, most users completed the assigned tasks in a similar amount of time. Figure 15 also illustrates the difficulties encountered by some users to complete certain tasks. This is visible by observing the number of outliers (e.g. task 4) and how far are their time values from the median (e.g. task 5). The overall relative efficiency is 100% in all tasks because all users managed to complete all tasks.
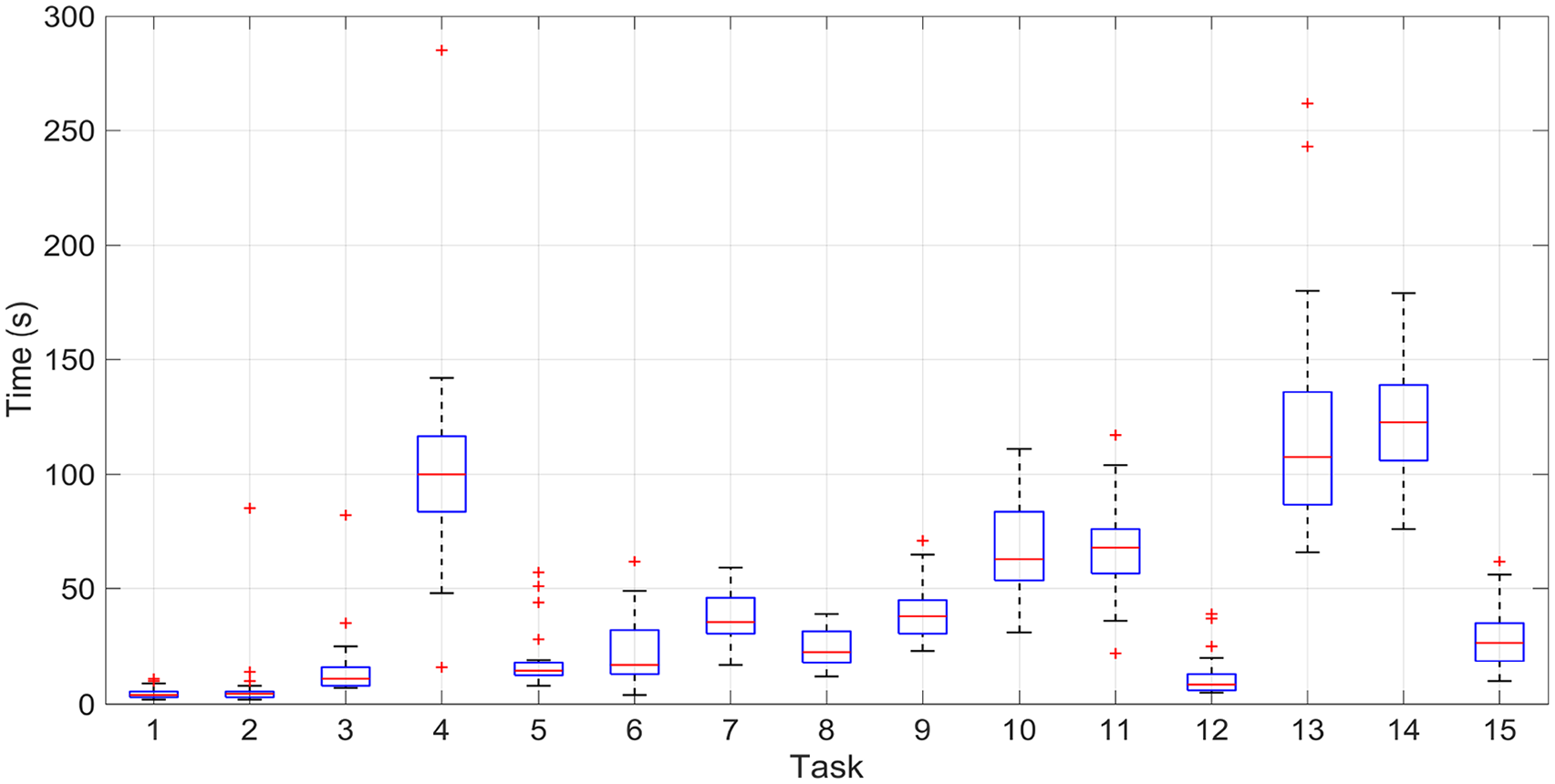
Box plot with the time per task measurements.
Finally, to complete the usability study, users were asked to complete two satisfaction tests to find out their opinions on the tool. Through the answers in the SEQ tests, it can be generally observed that users rated the tasks performed with high marks, which means that most of the tasks were easy for them to complete as Figures 16 and 17 illustrate.

Box plot with the SEQ results by user.

Box plot with the SEQ results by task.
If we analyze the evaluations of the results of the SUS, we see that the results are also positive since 60% consider the application as Excellent, 30% as Good, 5% as OK, and the other 5% as Poor, as it can be extracted from Table 5.
Individual’s SUS score.
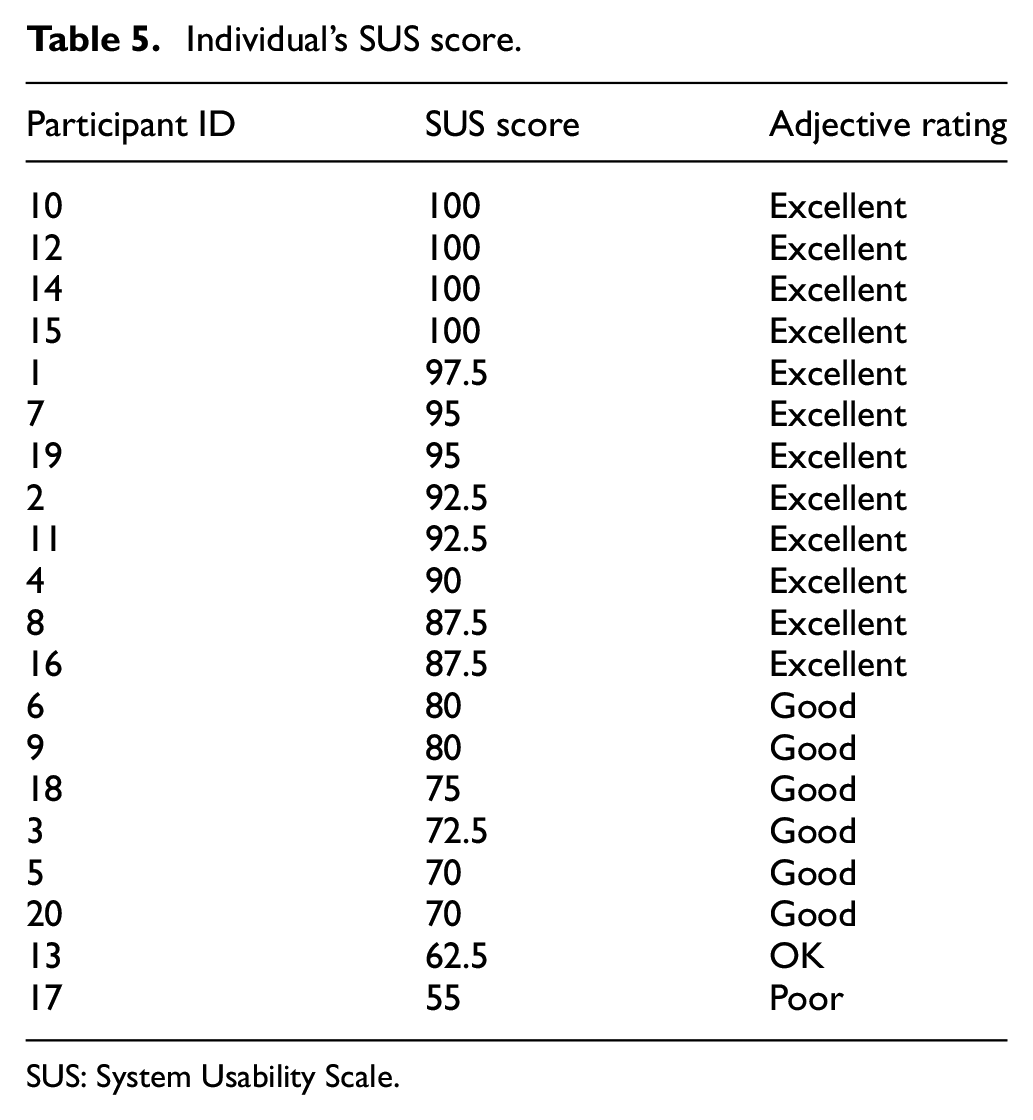
SUS: System Usability Scale.
Conclusion
This article has presented ArthiriKin, a rehabilitation system based on computer vision for patients suffering RA. The system is aimed for at-home rehabilitation, providing supervision and feedback for the user and a friendly natural interface for interaction. Furthermore, the performance during exercise routines is recorded to allow the remote supervision of physiotherapists. Calibration and performance metrics are adapted to the user, providing online feedback to the user while performing the exercises. The resulting system has been evaluated by means of a high-accuracy measurement system that is used as a gold standard: the Krypton K-400 dynamic measuring machine (Metris M.V.). The accuracy obtained with the Kinect-based system is considered to be sufficient considering the computing errors and correlation indexes obtained. Motivation and usability have also been analyzed. Motivation has been analyzed from the perspective of therapists to determine their willingness to use and recommend this tool. Overall, the tool is highly perceived by professionals (highly considered in terms of usefulness) who show medium–high interest in the tool and therefore in their willingness to adopt it as a working tool. In terms of usability, the high rate of completion (100%) and low error rate (18%) lead us to conclude that the proposed system is effective and also efficient because of its high efficiency rate (100%). In terms of user satisfaction, most of the participants (90%) are positively satisfied with the system usability and easiness of use.
This work therefore demonstrates the viability of a system based on a low-cost depth camera to support at-home rehabilitation for RA patients, but it can easily be extrapolated to any other condition benefiting from daily exercise. The system assessment yields a sufficiently low error for supervising the correct execution of the most commonly used exercises for this type of rehabilitation. Particularly important is the performance of the supervising algorithm, capable of working in real time, instantaneously detecting and notifying deviations.
These evidences lead us to conclude that the proposed system could have a potential impact in improving the quality of life of people suffering from RA. Patients count on an external supervisor detecting wrong positions or incorrect exercise performance in real time. Besides, performance data is collected assisting the specialists in the evaluation of the progression of the patient as well as the detection of crisis.
Footnotes
Handling Editor: Xing Chen
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has been partly funded by the Spanish Ministry of Economy and Competitiveness under project PLATINO (TEC2017-86722-C4-4-R) and by the Regional Government of Castilla-La Mancha under project SYMBIOT (SBPLY/17/180501/000334) which is partially funded by the European Social Fund. Mr Cantarero is funded by the Spanish Ministry of Education, Culture and Sport within the framework of the National FPU Program (ref. FPU 16/06205). Xavier del Toro Garcia has received financial support from the European Regional Development Fund (Fondo Europeo de Desarrollo Regional, FEDER).