
Abstract
It is well-established that different leadership styles are associated with followers’ mental health. However, little is known about the relative strength of the relationship of different leadership styles with followers’ mental health. So far, there is no meta-analysis comparing the incremental contribution of different leadership styles to mental health and studying potentially problematic construct proliferation. We included studies that compared at least two leadership styles in view of their relationships with followers’ mental health and directly estimated the relative contribution of seven leadership styles (i.e., transformational, transactional, laissez-faire, task-oriented, relationship-oriented, and destructive leadership, as well as leader-member exchange) to followers’ mental health. Using meta-analytical regression models, we compared the strength of the relationships between these leadership styles and followers’ overall mental health as well as positive (well-being and psychological functioning) and negative aspects of their mental health (affective symptoms, stress, and health complaints). Fifty-three studies with 217 effect sizes comprising 93,470 participants met the inclusion criteria. Transformational and destructive leadership were the strongest predictors of overall and negative aspects of mental health among followers. In contrast, the strongest predictors of positive mental health outcomes among followers were relations-oriented and task-oriented leadership, followed by transformational leadership. In sum, our results suggest that various leadership styles make unique contributions to explaining followers’ mental health and thus construct proliferation mostly does not pose a major problem when predicting relevant outcomes in this domain of leadership research. Our results are relevant for leadership development programs and for future organizational leadership models.
Keywords
To what extent do established leadership styles explain unique shares of the variance in followers’ mental health outcomes? Which leadership style has the strongest favorable association with followers’ mental health? And, in contrast, which leadership style has the strongest unfavorable association with followers’ mental health? These seemingly easy questions are currently hard to answer. Even though it is well-established that leadership affects followers’ cognitive and affective outcomes (Avolio et al., 2009; Kuoppala et al., 2008; Montano et al., 2017; Skakon et al., 2010), “leadership research has largely neglected research on employee health and well-being in favor of employee performance” (Inceoglu et al., 2018, p. 179). This limitation contrasts with the importance that followers’ health- and well-being-related states such as job satisfaction, perceived imbalance between efforts and job rewards or depression symptoms have on key organizational indicators including productivity (Böckerman & Ilmakunnas, 2012), absenteeism (Lidwall, 2016), or retirement intentions (Nexo et al., 2015).
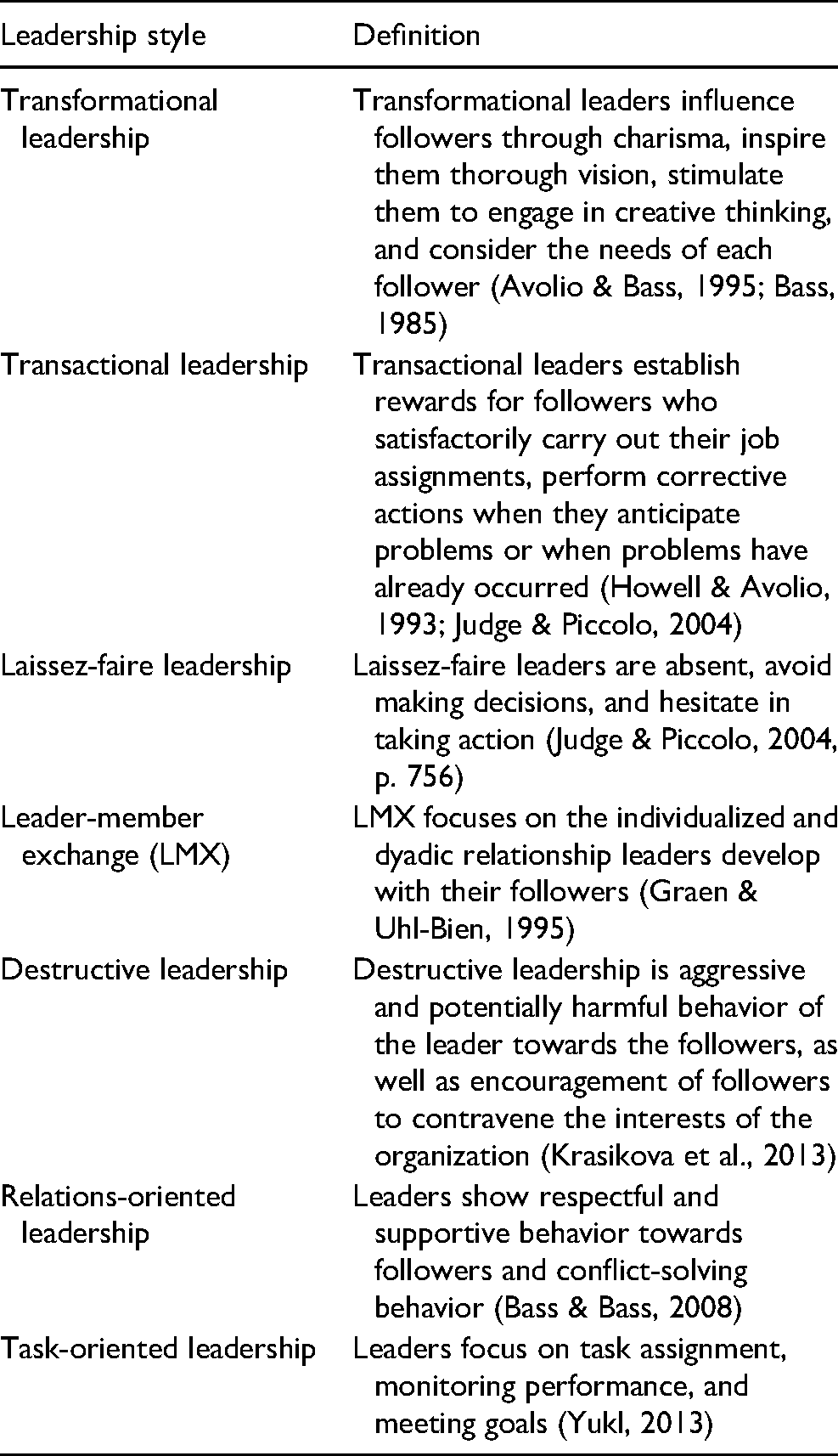
While previous meta-analyzes investigated the relation between leadership behavior and followers’ health-related outcomes (e.g., well-being or job-related stress; Avolio et al., 2009; Kuoppala et al., 2008; Montano et al., 2017), they do not allow drawing conclusions on the relative strength of these relationships: As the different leadership styles (i.e., the predictor variables in these meta-analyses) correlate substantially, the unique contribution of each leadership style in explaining followers’ mental health cannot be derived from the reported effect size estimates (see Derue et al., 2011). To address this problematic state of affairs, we present a meta-analysis focusing on the estimation of the unique and relative contributions of seven common leadership styles (i.e., transformational, transactional, laissez-faire, task-oriented, relationship-oriented, and destructive leadership, as well as leader-member exchange; see Table 1) in explaining followers’ mental health.
Definition of the Leadership Styles Investigated in the Present Meta-Analysis.
Following the approach of previous meta-analyses on the relative importance of different leadership styles for more prototypical leadership outcomes (e.g., job performance or job satisfaction; Piccolo et al., 2012), the current meta-analysis focuses on studies which compare at least two leadership styles. This approach allows not only the estimation of study- and sample-specific variance, but also the estimation of the unique explained variance in mental health-related outcomes (e.g., Judge & Piccolo, 2004). In contrast, previous meta-analyses examining the association between leadership styles and followers’ health mainly included primary studies focusing on only one leadership style and mental health (e.g., Kuoppala et al., 2008; Montano et al., 2017). Therefore, those meta-analyses could not indicate the unique and relative contributions of different leadership styles to followers’ mental health outcomes.
Considering the theoretical and practical implications of this research question, the first contribution of the present meta-analysis is to investigate whether and to what extent established leadership styles explain unique shares of the variance in followers’ mental health outcomes, as can be expected based on the theoretical differences between these styles. Given the current discussion on construct proliferation in leadership research (e.g., Banks et al., 2018; Bormann & Rowold, 2018; Hoch et al., 2016; Le et al., 2010), the often high correlations between leadership styles (e.g., between transactional and transformational leadership or between transformational and relations-oriented leadership), and the relevance of evidence-based leadership development programs (see Day, 2000, 2011), this is an important contribution to clarify the ability of different leadership styles to independently explain followers’ mental health. As the second contribution, we examine which leadership style has the strongest versus the weakest association (positive and negative) with followers’ mental health, i.e., we study not only whether, but to what extent established leadership constructs explain unique shares of the variance in followers’ mental health outcomes. To this end, we focused on primary studies that include a comparison of at least two different leadership styles in view of at least one mental health outcome. By doing so, we also study whether the principle “bad is stronger than good” (Baumeister et al., 2001) applies to the domain of leadership and follower health. Thus, we analyze whether destructive leadership as a “bad” leadership style has stronger associations with followers’ mental health outcomes than “good” leadership styles (e.g., transformational or relations-oriented leadership). Studying this question is relevant, because the basic principle (Baumeister et al., 2001) has been shown in various domains of human experience and behavior (e.g., negative vs. positive or neutral information receiving more attention, Ito et al., 1998, negative information being shared more in social contexts, Bebbington et al., 2017, and negative events being described with more elaborate language, Rozin & Royzman, 2001). Consequently, knowing whether mitigating “bad” leadership behaviors or fostering “good” leadership is a priority can once again inform leadership development programs (Day, 2000, 2011). As the third contribution, we investigate whether transactional and transformational leadership show an “augmentation effect” with regard to mental health (i.e., whether transformational leadership extends the assumed positive effect of transactional leadership). The augmentation effect is one of the most prominent tenets of the full range of leadership model (Bass & Avolio, 1993). Because the model has been among the most popular and most-studied leadership models for the last three decades, this is a highly relevant question.
The Present Research
We generally conceptualize mental health “as a continuum of neurophysiological and cognitive states related to thinking, mood and emotion, and behavior” (Montano et al., 2017, p. 329; see also WHO, 2001; for a comprehensive overview of mental health research, see Cooper et al., 2010). We further define positive mental health as full psychological functioning (i.e., the ability and capacity to flourish and being able to cope with stressful situations; Vaillant, 2003), and a positive sense of well-being (i.e., experiencing positive feeling states and subjective growth; McDowell, 2010). Negative mental health, in contrast, is defined as health states with potential clinical consequences including depressive symptoms, anxiety, frustration, negative affect, job-related stress, and similar outcomes (Mrazek & Haggerty, 1994).
To allow for an analysis of the absolute value that a particular leadership style explains with regard to mental health outcomes of different valences, we also consider the absolute magnitude of the associations between leadership styles and followers’ mental health irrespective of whether positive or negative health outcomes are involved. We refer to this magnitude as “overall mental health”. For this analysis, we do not consider the specific valence of the relationship (positive or negative) between a leadership style, for instance transformational leadership, and overall mental health outcomes, for instance well-being or anxiety.
Leadership can be understood as both, (i) a social influence process towards coordination of individual action, and (ii) a facilitating process of collective action to accomplish shared objectives (Yukl, 2013). In our meta-analysis, we will focus on (1) transformational/charismatic leadership theories (transformational leadership, transactional leadership, and laissez-faire), (2) leadership behavior theories (destructive leadership, and relations-oriented and task-oriented leadership), and (3) social interaction theories (leader-member-exchange [LMX]; for the definitions of these leadership constructs, see Table 1).
The concept of leadership styles is usually used to denote characteristic patterns of leader behavior (Fleishman et al., 1991). Although it is possible to classify the various leadership constructs according to levels of conceptualization (e.g., organization, groups or dyads; Yukl, 2013), the results of primary studies are usually based on instruments, which capture followers’ appraisals of typical behavioral patterns of leaders such as trustfulness, consideration or motivating behaviors. We, therefore, also conceptualize the leadership constructs that we included in our meta-analysis as leadership styles. In addition, one of the major aims of the present study is to assess potential construct proliferation regarding the associations of leadership and mental health (i.e., we test whether the constructs explain unique shares of the variance in mental health outcomes). To do so, we treat potentially overlapping constructs such as transformational leadership and relations-oriented leadership as separate constructs. By adopting this approach, we assume that each leadership style explains unique shares of the variance in followers’ mental health outcomes and, therefore, we are able to assess the extent of construct proliferation.
While the question of unique and relative contributions of different leadership styles to followers’ mental health has been unclear so far, large meta-analytic studies have consistently substantiated the following findings on the relationship between the most investigated leadership styles and followers’ mental health: First, important mental health outcomes such as stress, burnout, and depersonalization have been associated with lower levels of transformational leadership and LMX (Harms et al., 2017). Second, destructive leadership behaviors have been associated with increased levels of negative affect and perceived stress, and lower levels of well-being and positive affect (Schyns & Schilling, 2013). Third, recent meta-analytic evidence indicates that leadership behavior is also related to the leaders’ own mental health, with abusive supervision being associated with lower levels of leaders’ well-being (Kaluza et al., 2020).
More specifically, a previous meta-analysis focused on the associations of several leadership constructs and followers’ mental health (Montano et al., 2017). The study indicated medium to large reliability-adjusted correlations of different leadership styles with both negative and positive mental health outcomes (Montano et al., 2017). In particular, higher levels of transformational leadership, relations-oriented leadership, and LMX were related to less affective symptoms, burnout, job stress, and health complaints, and, at the same time, higher levels of well-being. On the contrary, destructive leadership was associated with increased affective symptoms, burnout, job stress, and decreased levels of well-being. In the current research, we generally build on the meta-analysis by Montano et al. (2017). However, as noted above, this meta-analysis is limited because it does not speak to the issues of (a) unique variance shares in followers’ mental health explained by single leadership styles and (b) the relative contribution of the respective styles to followers’ mental health. In other words, although the prior meta-analysis by Montano et al. (2017) reported substantial associations between several leadership styles and mental health outcomes, it did not clarify whether some leadership styles are more relevant for mental health than others. For example, both transformational leadership and LMX were found to be relevant antecedents of affective symptoms and work-related stress, yet the prior meta-analysis did not compare these leadership styles directly and, thus, could not clarify whether transformational leadership is a stronger antecedent of mental health outcomes than LMX. Moreover, it is even possible that some leadership styles in the prior meta-analysis are redundant given the high correlation between them (e.g., transactional and transformational leadership), which would point to construct proliferation in this domain. Thus, the present meta-analysis goes also beyond the study of single leadership styles of Montano et al. (2017) by addressing whether construct proliferation may actually account for the observed associations. In the next sections, we will derive a series of hypotheses on the seven leadership styles of our meta-analysis (transformational, transactional, laissez-faire, task-oriented, relationship-oriented, and destructive leadership, and leader-member exchange) and their associations with the three classes of followers’ mental health outcomes (i.e., positive, negative, and general health).
Relative Importance of Transformational Leadership and LMX for Overall and Positive Mental Health
We assume that transformational leadership and LMX are particularly relevant concerning the overall and positive mental health of followers. Transformational leadership (Avolio & Bass, 1995; Bass, 1985) influences followers through charisma, inspires them through vision (i.e., inspirational motivation), stimulates them to engage in creative thinking (i.e., intellectual stimulation), and considers the needs of each follower (i.e., individualized consideration). Thereby, transformational leadership is directly linked to the followers’ psychological needs (such as feelings of competence and relatedness; see Deci & Ryan, 2000; Inceoglu et al., 2018) and is proposed to increase followers’ necessary resources (e.g., motivation; Arnold, 2017; Stenling & Tafvelin, 2014; Walsh et al., 2014). Based on needs-based theoretical approaches generally (e.g., Hogan, 1982; McClelland, 1987) and self-determination theory specifically, we assume that the satisfaction of followers’ needs leads to optimal psychological functioning and well-being (Deci & Ryan, 2000). This link has been supported by various previous studies (e.g., Reis et al., 2018; Sheldon & Elliot, 1999; see Inceoglu et al., 2018). Hence, needs satisfaction should have a positive influence on overall mental health outcomes as well as positive mental health outcomes (Hobfoll, 1989, 2011).
LMX focuses on the individualized and dyadic relationship leaders develop with their followers (Graen & Uhl-Bien, 1995). As high quality exchange relationships are conceptualized as being tailored to the followers’ needs (Hooper & Martin, 2008), LMX should affect positive mental health outcomes by providing, for instance, an empowering work environment for followers (Schermuly & Meyer, 2015). Thus, followers should feel respected and supported (Sparr & Sonnentag, 2008) and report more resources, such as autonomy or trust (Gregersen et al., 2014). Hence, drawing on needs-based theories generally and self-determination theory specifically (Deci & Ryan, 2000), those resources again should positively affect overall mental health, as well as positive mental health outcomes (Epitropaki & Martin, 2005).
Due to central characteristics of both leadership styles—such as individualized consideration and inspirational motivation for transformational leadership (Avolio & Bass, 1995) or high quality exchange relationships tailored to the followers’ needs for LMX (Graen & Uhl-Bien, 1995)— transformational leadership and LMX can be hypothesized to increase follower resources, such as empowerment or motivation (Schermuly & Meyer, 2015). Hence, they should both be associated with overall mental health, as well as positive mental health outcomes (Epitropaki & Martin, 2005; Hobfoll, 1989, 2011). Furthermore, in comparison with other leadership styles, transformational leadership and LMX are more concerned with the needs of the individual employee, which should be reflected in a stronger association of both leadership styles with mental health outcomes. In accordance with this theoretical argument, numerous findings from primary studies have emphasized the (relative) importance of transformational leadership and LMX for overall mental health and positive mental health outcomes (e.g., Arnold, 2017; Gregersen et al., 2014; Harms et al., 2017; van Dierendonck et al., 2004). Further, those findings are mirrored by a recent meta-analysis, in which transformational leadership and LMX showed some of the largest adjusted meta-analytic correlations across all mental health outcomes (affective symptoms, burnout, job stress, well-being, psychological functioning, and health complaints; Montano et al., 2017). Hence, we propose:
Relative Importance of Destructive Leadership for Overall and Negative Mental Health
However, leadership—and in particular destructive leadership—may also have harmful effects on mental health outcomes. Destructive leadership has been defined as aggressive and potentially harmful behavior of the leader towards their followers, as well as encouraging followers to contravene the interests of the organization (Krasikova et al., 2013). Such behaviors, which commonly include mockery, abusive language, continuous reproaching, blaming, hostile and rude manners (Tepper, 2000), are likely perceived as threatening and therefore stressful by affected followers (Harms et al., 2017). Experiencing stress results in a neuroendocrine response activation and increased affective symptoms (Contrada, 2010; Dallman & Hellhammer, 2010). Further, experiencing too much stress or prolonged periods of stress is detrimental for the followers’ mental health (see Harms et al., 2017). In addition, the power asymmetry between followers and leaders inhibits a direct response such as retaliation towards the leader (Marcus-Newhall et al., 2000). Thus, the effects of destructive leadership may be exacerbated by followers passing their experienced negative affect on to coworkers or private contacts (Carlson et al., 2012; Skarlicki & Rupp, 2010). Overall, destructive leadership should impair the availability of followers’ resources, and, consequently, increase the likelihood of negative mental health outcomes (Aasland et al., 2010).
Compared to other leadership styles, destructive leadership should have the most detrimental effect on followers, for instance, by increasing the likelihood of experiencing threatening or interpersonally stressful situations (Harms et al., 2017). This theoretical line of reasoning is supported by a recent meta-analysis, which reported one of the largest adjusted meta-analytic correlation for destructive leadership and negative mental health outcomes, thereby confirming its importance (Montano et al., 2017). Accordingly, we propose:
It was often argued and empirically shown that there is an asymmetry in the effects of positive and negative stimuli, whereby negative stimuli are weighted more heavily than positive ones (Baumeister et al., 2001; Kahneman & Tversky, 1979; Peeters & Czapinski, 1990; Rozin & Royzman, 2001). This in turn affects various fundamental domains of human experience and behavior (e.g., information processing and use of language, see Ito et al., 1998; Rozin & Royzman, 2001). Previous work (Duffy et al., 2002) emphasized the detrimental effects of negative interactions in the work context overshadowing the effects of simultaneous positive interactions with the same party (i.e., the supervisor). Building on this notion, we further posit that destructive leadership as compared to transformational leadership and LMX should have a stronger association with mental health. More specifically, given the saliency of hostile behaviors in destructive leadership, we hypothesize that followers who experience destructive leadership at work may have enhanced cognitive access to information on negative feelings, negative work-related memories, and negative health symptoms. Consequently, we propose:
Relative Importance of Transactional and Relations-Oriented Leadership for Overall, Positive, and Negative Mental Health
In our meta-analysis, we also consider transactional leadership and relations-oriented leadership and compare them to transformational leadership and LMX. Transactional leadership consists of (i) leaders establishing rewards for followers who satisfactorily carry out their job assignments (contingent reward), (ii) corrective actions of leaders when they anticipate problems (management by exception-active), and (iii) corrective actions of the leader when problems have already occurred (management by exception-passive; Howell & Avolio, 1993; Judge & Piccolo, 2004). Relations-oriented leadership encompasses respectful and supportive behavior towards followers and conflict-solving behavior (Bass & Bass, 2008).
As transformational leadership is assumed to build on transactional leadership (Avolio, 1999; Bass & Avolio, 1993), transformational leadership is thought to extend the assumed positive effect of transactional leadership (i.e., the so-called augmentation effect; Bass & Avolio, 1993), on followers’ mental health: While transactional leadership represents leaders’ contingent rewards and corrective actions, transformational leadership, in contrast, exerts its influence on followers through, for instance, inspirational motivation or intellectual stimulation and thereby may lead to improved follower well-being through social-cognitive (e.g., psychological empowerment) and motivational processes (e.g., need fulfilment; see Inceoglu et al., 2018). A similar effect could be assumed for LMX regarding relations-oriented leadership, given that LMX implies a high quality, individualized leader-follower relationship concerned with the exchange of resources between the leader and the follower, which may go beyond the more general consideration toward followers implied in the concept of relations-oriented leadership (see, for instance, Mahsud et al., 2010).
In addition, transformational leadership can also be considered a more comprehensive construct than relations-oriented leadership because transformational leaders, for instance, not only express individualized consideration by showing respect and concern for their followers, but also motivate and inspire followers by serving as role models or by providing meaning to the work’s assignments (for related meta-analytical evidence, see Derue et al., 2011). Consequently, we expect transformational leadership to show larger associations with followers’ mental health than relations-oriented leadership. When comparing LMX and transactional leadership, a similar reasoning should apply: LMX is considered to be more comprehensive than transactional leadership (see Graen & Uhl-Bien, 1995). This is because the exchange relation between the follower and the leader not only covers resources and goals, but also recognition and support, which should influence followers’ mental health. Hence, LMX is expected to explain more variance in followers’ mental health than transactional leadership. Prior meta-analytic findings support the conceptual overlap outlined above by showing that not only transformational and transactional leadership (Piccolo et al., 2012), but also transformational and relations-oriented leadership largely correlate (Derue et al., 2011). In summary, we propose:
Concerning transactional leadership (for our further reasoning on relations-oriented leadership, see Hypothesis 6), we, nonetheless, assume that it explains a unique share of the variance in followers’ mental health that also goes beyond transformational leadership. In particular, transformational leadership is assumed to augment the effect of transactional leadership (see Judge & Piccolo, 2004) and the “very term augmentation, meaning amplification or extension, suggests that there is something to amplify or extend” (Judge & Piccolo, 2004, p. 756). The meta-analysis by Judge and Piccolo (2004) indicated support for those theoretical assumptions and reported coherently unique variance for transactional leadership concerning performance-related criteria such as follower job satisfaction or leader job performance. Following Inceoglu et al.’s (2018) arguments, we assume that transactional leadership affects follower well-being positively through follower motivation, in particular due to its contingent reward component. Hence, we analogously propose:
Incremental Validity of Task-Oriented, Relations-Oriented and Laissez-Faire Leadership in Overall, Positive, and Negative Mental Health
Task-oriented leadership focuses on task assignment, monitoring performance, and meeting goals (Yukl, 2013). Laissez-faire leadership, in contrast to relations-oriented and task-oriented leadership, reflects the absence of leadership, as laissez-faire leaders “avoid making decisions, hesitate in taking action, and are absent when needed” (Judge & Piccolo, 2004, p. 756). From a theoretical point of view, relations-oriented and task-oriented leadership, as well as laissez-faire leadership should not incrementally add to followers’ mental health outcomes after taking into account transformational leadership, transactional leadership, and LMX. First, as outlined above, transformational leadership and LMX can be considered as more comprehensive leadership styles, which also encompass central aspects of task- and relations-oriented leadership, such as leaders monitoring and rewarding performance or showing respect and concern for their followers, respectively (Bass & Bass, 2008; Yukl, 2013). Prior meta-analytic evidence could be interpreted to support this notion, since the associations of transformational leadership and LMX with various mental health outcomes were found to be the largest (see Montano et al., 2017).
Second, when considering the specific effects of laissez-faire leadership on followers’ mental health, the question is whether the absence of leadership explains unique variance in mental health outcomes after accounting for actually exhibited leadership (i.e., transformational leadership, LMX, and transactional leadership). Possibly, exhibited (i.e., active) and absent (i.e., passive) leadership behavior are two sides of the same coin—and so accounting for transformational leadership and LMX could already suffice for explaining the observed variance. In addition, transactional leadership accounts not only for active leadership behavior (i.e., contingent reward and management-by-exception, active), but also for passive (i.e., absent) leadership (i.e., management-by-exception, passive), potentially showing some overlap with laissez-faire leadership. Previous studies showed high multicollinearity for transformational, transactional, and laissez-faire leadership (for an overview, see Judge & Piccolo, 2004) and their effects “were substantially weakened when controlling for their mutual influences” (p. 764). This reasoning is partly supported by previous meta-analytic findings of Derue et al. (2011) showing that the variance in job satisfaction explained by laissez-faire leadership is lower than the corresponding proportion explained by other leadership styles involving a direct leader-follower interaction such as transformational leadership (3.8% vs. 21%).
Hence, in the present study we assume that transformational leadership, LMX, and transactional leadership explain the main variance share in followers’ well-being. We further assume that the effect size estimates of task-oriented, relations-oriented, and laissez-faire leadership are substantially lower in comparison to the direct effects of the prior leadership styles (i.e., transformational leadership, LMX, and transactional leadership). Further, in accordance with this argumentation, we do not expect unique shares of explained variance for the latter leadership styles (i.e., task-oriented, relations-oriented, and laissez-faire leadership) and therefore propose:
Methods
Study Protocol
With our meta-analysis, we build on the prior meta-analysis by Montano et al. (2017), as we adapted their study protocol, and updated the screening of studies. Since the previous database search of Montano et al. (2017) ended in July 2014, we updated the queries for original studies published in peer-reviewed journals to the period between August 2014 and September 2018 (in German, English, French, Italian or Spanish; search strings are provided in the Supplementary Material). The screening for new records was updated by querying in the databases PubMed, PsycINFO, PsycARTICLES, PSYNDEX, Econlit, and Business Source Premier (EBSCO Host). Further, we included only studies that reported correlations of at least two different leadership constructs and at least one mental health outcome in samples of employees. We pre-registered our meta-analysis in the PROSPERO database of systematic reviews. Fifty-three studies entered the analyses of the present study (see also Figure 1), including overall 217 correlations and 93,470 participants.
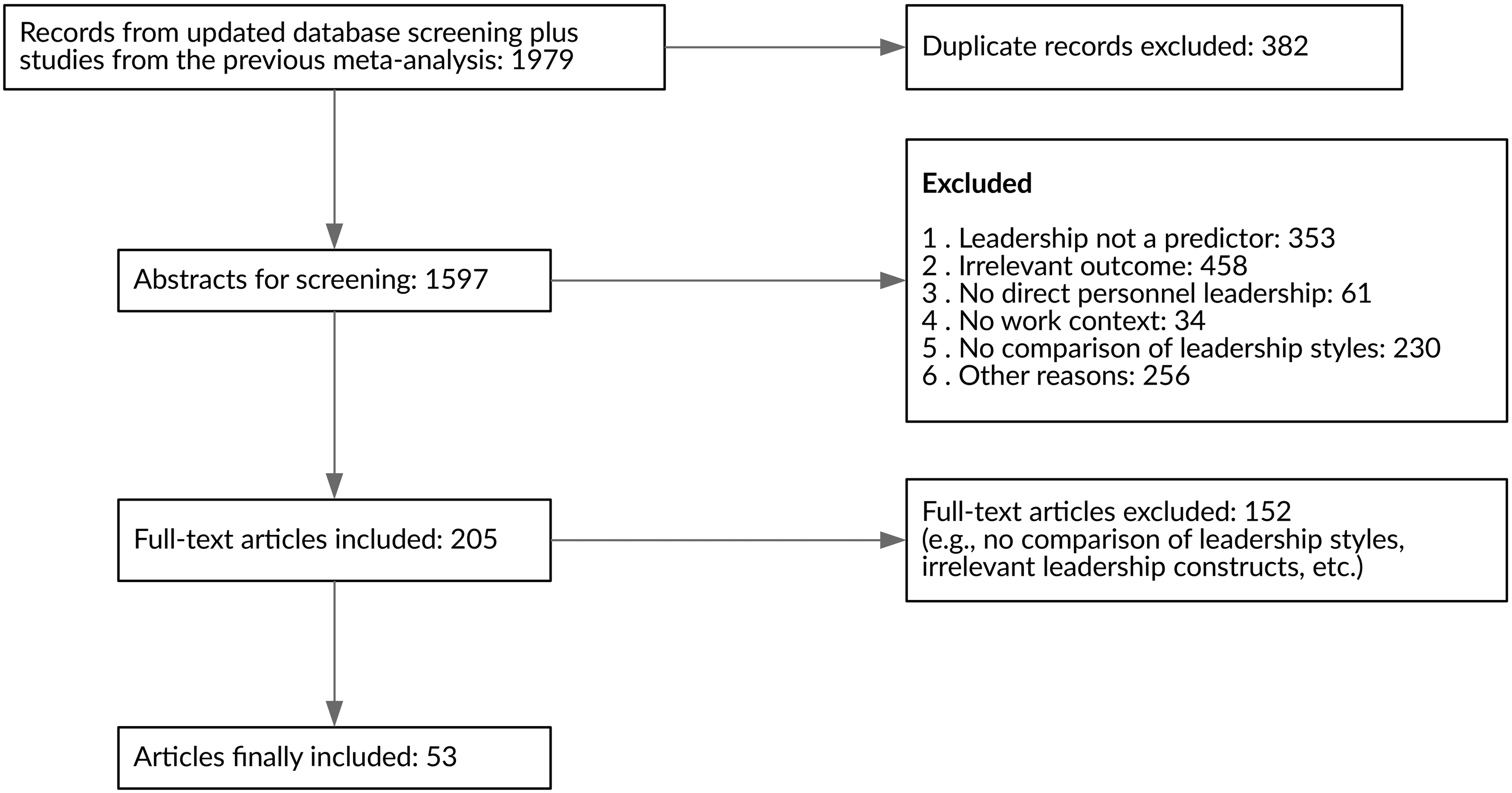
Flow diagram of included studies.
We base our conceptualization of leadership constructs and mental health outcomes on the previous meta-analysis by Montano et al. (2017) and considered the following seven leadership constructs: (1) transformational leadership, (2) transactional leadership, (3) laissez-faire leadership, (4) relations-oriented leadership, (5) task-oriented leadership, (6) destructive leadership, and (7) LMX. Other leadership constructs or theories including communication processes (Freedman, 2013), emotional interaction aspects of leader-follower dyads (Rajah et al., 2011), and cognitive processes (Lord & Shondrick, 2011) were also coded, but, due to the small number of respective studies, they were not included in the research hypotheses of this meta-analysis (Montano et al., 2017, also found only few related studies).
We classified mental health outcomes either as positive mental health states (i.e., well-being and psychological functioning; McDowell, 2010; Vaillant, 2003), or negative mental health (i.e., affective symptoms, burnout, stress, and health complaints; Mrazek & Haggerty, 1994). More specifically we considered affective symptoms (e.g., depressive symptoms, negative affect), burnout (including emotional exhaustion), work stress (e.g., job strain, distress, psychological stress), well-being (e.g., work-related well-being, positive affect), psychological functioning (e.g., empowerment, fulfillment, self-efficacy), and health complaints (e.g., overall health, fatigue, sleep problems). In addition to positive and negative mental health outcomes, we also analyzed overall mental health. Overall mental health refers to the absolute magnitude of all included associations, i.e., irrespective of the sign of the correlation coefficient. By taking into account the absolute value of the correlations (independent of the valence of the health outcomes), the analysis provides an estimate of the proportion of overall explained variance, i.e., the magnitude of the predictive ability of each leadership style for both positive and negative mental health outcomes. We classified mental health outcomes either as positive mental health states (i.e., well-being and psychological functioning; McDowell, 2010; Vaillant, 2003), or negative mental health (i.e., affective symptoms, burnout, stress, and health complaints; Mrazek & Haggerty, 1994).
Coding of Predictors and Outcomes
The coding of leadership constructs and mental health outcomes was performed by two graduate organizational psychologists who are not among the authors of the present study and who were blind to the research hypotheses. Both raters received a document including a general definition of the included leadership constructs and mental health outcomes. The coding of leadership constructs and mental health outcomes was performed satisfactorily (Cohen’s kappa 0.84 and 0.89, respectively; Landis & Koch, 1977). Raters resolved classification disagreements by discussion.
Statistical Analysis
The present investigation focuses on the comparison of leadership styles regarding their association with mental health outcomes. Thus, the overall approach of the statistical analysis is to estimate the extent to which each single leadership style explains variance of the meta-analytic associations. Hence, contrary to the usual meta-analytic studies, in which the effect sizes Ti reported in i studies are aggregated in a meta-analytic overall estimate θ, we compare the contribution of each leadership style to the variance of the overall estimate. To accomplish this, we consider each leadership style Xj, j = 1, …, p, as a predictor of the meta-analytic overall estimate θ. The approach can be described in terms of a meta-analytic multilevel model with three levels of variation as described in detail in Konstantopoulos (2011). The first level corresponds to the usual within-study variance of the reported effect size Ti around the true estimate θi:




The logical implications of our research hypotheses led to the definition of 12 linear-mixed regression models, which were estimated in the random-effects specification via restricted maximum-likelihood (Kalaian & Raudenbush, 1996; Viechtbauer, 2005). The correspondence between model specification, hypotheses, and expected results is provided in Table 2. Since most research hypotheses concern the relative contribution of particular leadership styles to the variance of effect sizes, the goodness-of-fit of the models can be used to compare how much of the heterogeneity is explained by the different leadership styles. In the context of likelihood-based inference, the goodness-of-fit estimated by the Akaike’s Information Criterion (AIC) is an appropriate statistic, which takes into account model complexity, with lower AIC values indicating a better model (see the next paragraph for an example of how the AIC statistic is being used in the present study). Furthermore, we also provide the Q-statistic of the test of moderators corresponding to the null hypothesis H0: βjs = 0 (see equation 4).
Model Specification, Research Hypotheses and Expected Results.
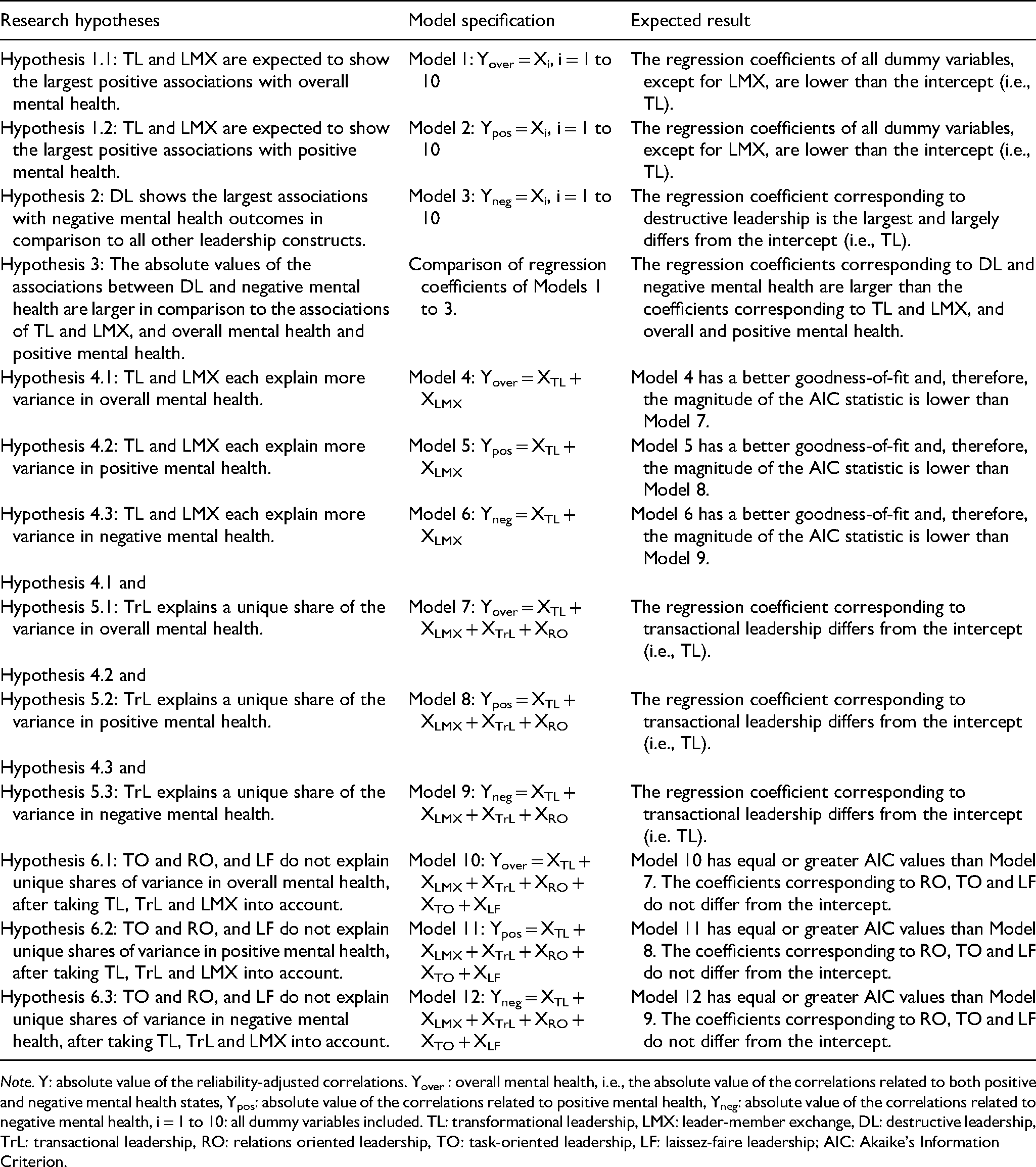
Note. Y: absolute value of the reliability-adjusted correlations. Yover : overall mental health, i.e., the absolute value of the correlations related to both positive and negative mental health states, Ypos: absolute value of the correlations related to positive mental health, Yneg: absolute value of the correlations related to negative mental health, i = 1 to 10: all dummy variables included. TL: transformational leadership, LMX: leader-member exchange, DL: destructive leadership, TrL: transactional leadership, RO: relations oriented leadership, TO: task-oriented leadership, LF: laissez-faire leadership; AIC: Akaike’s Information Criterion.
The raw reported correlations rraw and the sampling error vraw were adjusted for measurement unreliability of the predictor and outcome variables by using the formulae radj = rraw / (αpred αout) and vadj = vraw / (αpred αout), respectively, where αpred and αout are the average Cronbach’s alpha of the predictor and outcome variables (Borenstein et al., 2009). In addition, as the effect sizes considered in the present study are correlations whose variance Vr is proportional to (1 - r2)2, it is necessary to perform the meta-analysis on the basis of Fisher’s z-transformation to avoid the explicit dependence of Vr on the effect size r (Borenstein et al., 2009). To this end, the correlations r are transformed to Fisher’s z by the formula z = 0.5 ln[(1 + r) (1 – r)] with variance Vz = 1/(n – 3) and sample size n. The linear-mixed meta-analytic regressions are performed on Fisher’s z score and the estimates are converted back to correlation units by applying the hyperbolic tangent function r = exp(2z – 1) / exp(2z + 1). For longitudinal studies, the correlations at baseline were considered to reduce losses of study participants because of sample attrition and to ensure a common time point of reference for comparison of effect sizes between longitudinal and cross-sectional studies. We report meta-analytic regression models based on the reliability-adjusted correlations and sampling error. The corresponding models of the raw unadjusted effect sizes are provided in the Supplementary File.
To illustrate our analytical approach, we describe Model 12 in detail in the following. It tests Hypothesis 6.3, i.e., the assumption that task-oriented leadership, relations-oriented leadership, and laissez-faire leadership do not explain unique shares of variance in negative mental health outcomes, after accounting for transformational leadership, transactional leadership, and LMX. In Model 12, the reliability-adjusted correlations of negative mental health states are regressed on transformational leadership, which is represented by the intercept, and the dummies corresponding to LMX, transactional leadership, relations- and task-oriented leadership, and laissez-faire leadership. Thus, if Hypothesis 6.3 holds, the AIC statistic of Model 12 should be greater than the corresponding AIC statistic of Model 9, since it is not expected that the inclusion of task-oriented leadership, relations-oriented leadership, and laissez-faire in Model 12 has an additional contribution to explained variance beyond Model 9. Therefore, the corresponding AIC values of Model 12 are supposed to be greater (i.e., worse goodness-of-fit) and the regression coefficients in Model 12 should not differ from the intercept representing the effect size of transformational leadership.
The regression coefficients in all models express the average differences between transformational leadership and the specific leadership style being compared. Furthermore, since the research hypotheses are stated in terms of the relative contribution of the leadership styles to the effect-size magnitude, all correlations of positive or negative mental health outcomes entered the models also as absolute values. All calculations and the estimation of meta-analytical models were performed with the programming language and statistical environment R (Version 3.6), especially the package “metafor” (Viechtbauer, 2010).
Results
A total of 23 distinct comparisons of leadership styles were identified in the included studies, yielding 217 correlations and a total of 93,470 participants. Most comparisons in the primary studies include transformational and transactional leadership, relations- and task-oriented leadership, and destructive leadership (see Table 3). Furthermore, negative mental health states are more frequently investigated in the primary studies than positive ones (151 vs. 66 correlations). The results of the mixed meta-analytic regressions concerning the research hypotheses are reported in Tables 3 and 4.
Linear-Mixed Meta-Analytic Regressions Corresponding to Models 1 to 3.
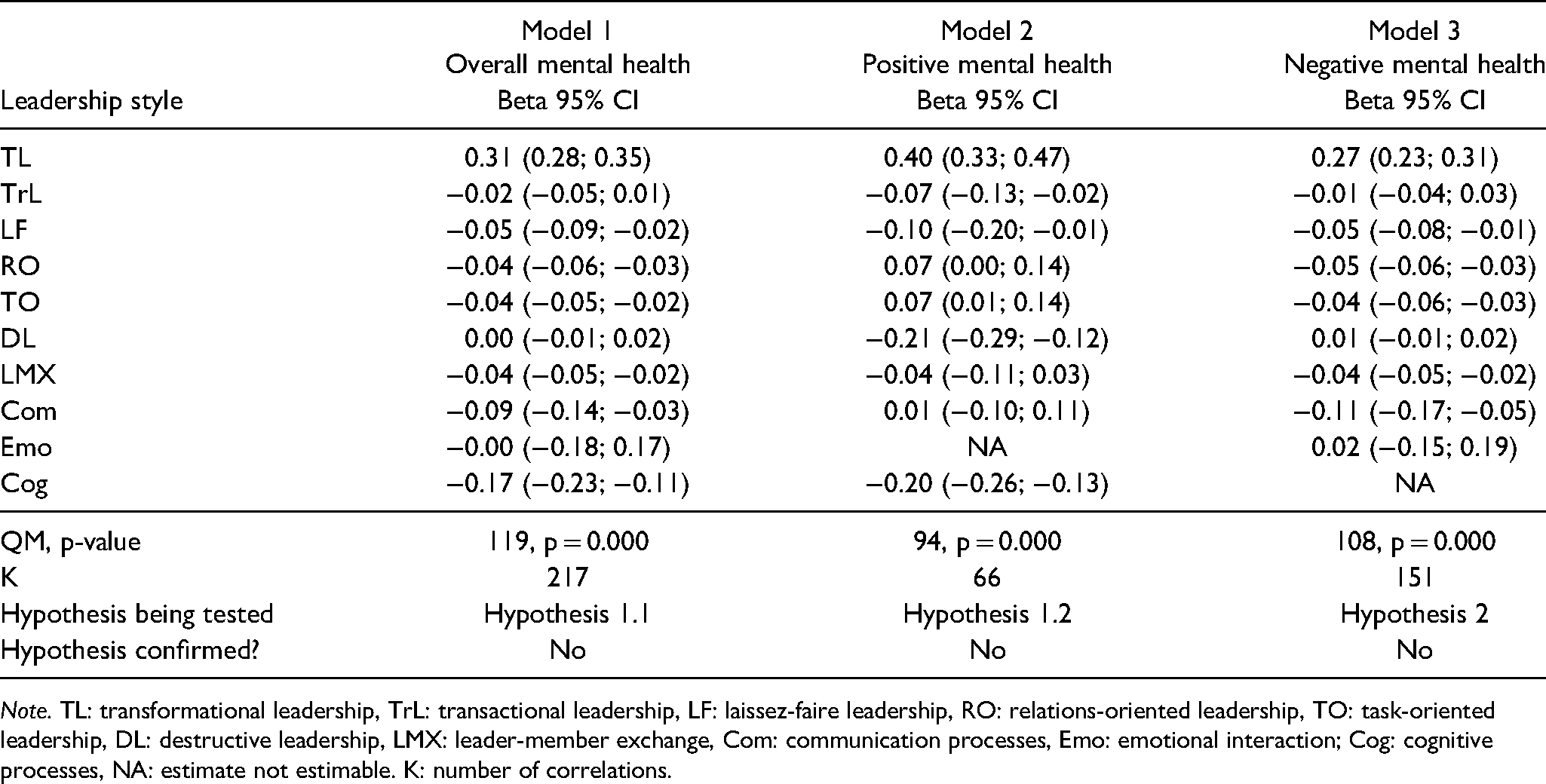
Note. TL: transformational leadership, TrL: transactional leadership, LF: laissez-faire leadership, RO: relations-oriented leadership, TO: task-oriented leadership, DL: destructive leadership, LMX: leader-member exchange, Com: communication processes, Emo: emotional interaction; Cog: cognitive processes, NA: estimate not estimable. K: number of correlations.
Linear-Mixed Meta-Analytic Regressions Corresponding to Models 4 to 12.
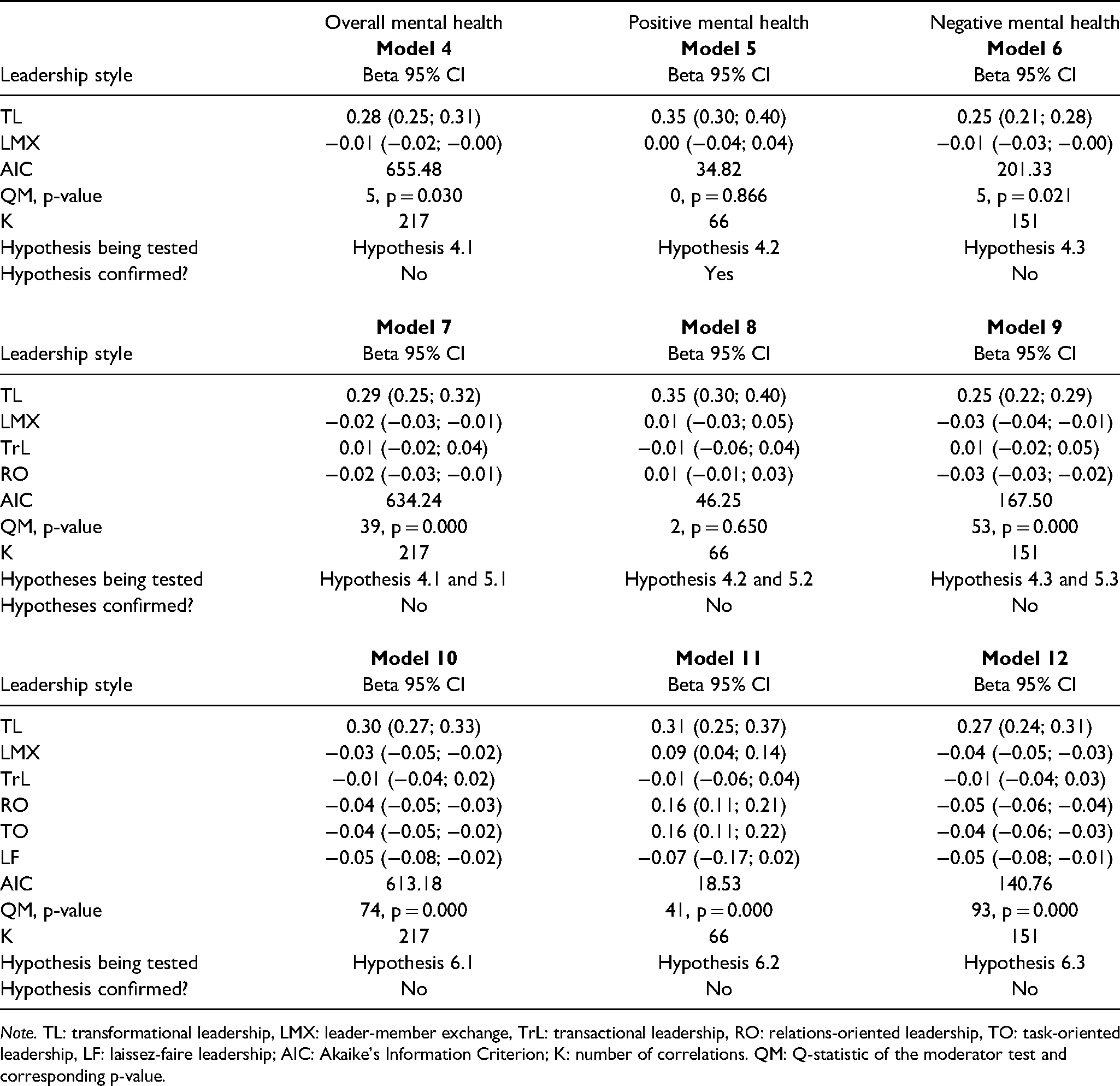
Note. TL: transformational leadership, LMX: leader-member exchange, TrL: transactional leadership, RO: relations-oriented leadership, TO: task-oriented leadership, LF: laissez-faire leadership; AIC: Akaike’s Information Criterion; K: number of correlations. QM: Q-statistic of the moderator test and corresponding p-value.
Hypothesis 1
As can be observed from Table 3, the regression coefficients β obtained in Model 1 for overall mental health reveal that LMX has a lower effect size than transformational leadership (β = −0.04, 95% CI [-0.05; −0.02]). At the same time, however, the coefficients of transactional leadership, destructive leadership, and the emotional interaction of leaders and followers in Model 1 include zero and, consequently, the corresponding effect sizes are not statistically different from transformational leadership. Hence, the results do not support Hypothesis 1.1, given that the regression coefficients in Model 1 do not indicate that transformational leadership and LMX show the largest positive associations with overall mental health. On the other hand, even though the effect sizes of transformational leadership and LMX regarding positive mental health do not statistically differ (Model 2, β = −0.04, 95% CI [-0.11; 0.03]), the coefficients of relations-oriented (β = 0.07, 95% CI [0.00; 0.14]) and task-oriented leadership (β = 0.07, 95% CI [0.01; 0.14]) indicate somewhat larger effect size estimates in comparison to transformational leadership and, as a logical consequence, also to LMX. Therefore, Hypothesis 1.2 is not supported as the effect size estimate of transformational leadership is not the largest in comparison to all other leadership styles.
Hypotheses 2 & 3
Similarly, Hypothesis 2 stating that destructive leadership shows the largest associations with negative mental health is not supported since the regression coefficient of destructive leadership in Model 3 is not statistically different from transformational leadership (Table 3, β = 0.01, 95% CI [-0.01; 0.02]). The comparison of the regression coefficients of Models 1 to 3 indicates that the association between destructive leadership and negative mental health is not larger than the associations of transformational leadership and LMX with overall mental health and positive mental health. Moreover, since the confidence intervals of the intercept estimates overlap, the difference between the effect size estimates of destructive leadership and transformational leadership for negative mental health (β = 0.01, 95% CI [-0.01; 0.02]) does not suggest that destructive leadership as a negative stimulus is being weighted more heavily than other types of leadership styles perceived as positive stimuli (see Table 3). On the contrary, the largest differences between transformational and destructive leadership are being observed for positive mental health (Model 2, β = −0.21, 95% CI [-0.29; −0.12]). Thus, Hypothesis 3 is not supported by the results.
Hypothesis 4
Concerning Hypothesis 4, the estimates in Table 4 indicate that transformational leadership and LMX explain more variance than transactional leadership and relations-oriented leadership, but only for positive mental health, and neither for overall nor for negative mental health. This can be observed by comparing the AIC and QM statistics of Models 5 and 8 (regarding positive mental health), in which there is no indication that the addition of transactional and relations-oriented leadership as predictors improves the model fit beyond transformational leadership and LMX, respectively (AIC: 34.82 vs. 46.25 and QM 0 [p = 0.866] vs. QM 2 [p = 0.650] in Model 5 and Model 8, respectively). Thus, our results support only Hypothesis 4.2. However, in contrast to Hypotheses 4.1 and 4.3, model fit of overall and negative mental health outcomes actually improved (e.g., AIC from 201 in Model 3 to 167 in Model 7) after considering transactional and relations-oriented leadership in the regression models (Table 4).
Hypotheses 5 & 6
By the same token, the coefficient estimates of transactional leadership in Models 7 through 9 (see Table 4) indicate that transactional leadership does not explain a unique share of the variance, since there are no differences from the intercept (i.e., transformational leadership, β = 0.01, 95% CI [-0.02; 0.04], β = −0.01, 95% CI [-0.06; 0.04], and β = 0.01, 95% CI [-0.02; 0.05], Models 7 to 9, respectively). Consequently, there was no evidence for Hypothesis 5. Finally, concerning Hypothesis 6, the AIC estimates of Models 10 through 12 in comparison to Models 7 through 9 reveal that the inclusion of task-oriented, relations-oriented, and laissez-faire leadership improves model fit for overall (Hypothesis 6.1), positive (Hypothesis 6.2), and negative mental health (Hypothesis 6.3). Moreover, the regression coefficients of those leadership styles in Models 10 through 12 reveal a unique contribution to explained variance, contrary to the assumptions of Hypothesis 6 (see Table 4). In particular, since model fit improved largely in Models 10 through 12 after the inclusion of task-oriented leadership (AIC 615.56, 15.45 and 141.81, respectively), it seems that the largest contribution to explained variance is associated to this leadership style rather than to relations-oriented or laissez-faire leadership.
Discussion
Our results indicated partial support for Hypothesis 1.1, stating that transformational leadership and LMX show the largest effect sizes for mental health, and supported Hypothesis 4.2, stating that transformational leadership and LMX explain more variance in positive mental health outcomes than transactional and relations-oriented leadership. However, most of our hypotheses were not supported. The main reason for the mostly unexpected results was the surprisingly low share of explained variance attributable to LMX (i.e., previous sources would have pointed in a different direction, see, for instance, Harms et al., 2017; Montano et al., 2017). This surprising result, however, simultaneously demonstrates the value of our approach of moving beyond the assessment of single leadership constructs and their respective relationships with followers’ mental health (see, for instance, Montano et al., 2017), because focusing on single leadership constructs can lead to potentially ambiguous findings. In contrast, directly comparing leadership styles to each other regarding the unique variance that they explain in followers’ mental health clarifies this.
Even in the absence of supported hypotheses, our findings still revealed a clear overall pattern: First, transformational and destructive leadership are the strongest predictors of overall mental health, with laissez-faire, relations- and task-oriented leadership, and LMX each showing incremental contributions to explained variance, albeit with lower effect size estimates (Tables 3 and 4). Second, relations- and task-oriented leadership were the strongest predictors of positive mental health outcomes, followed by transformational leadership (Table 4). At the same time, destructive leadership and, to a lesser extent, laissez-faire leadership showed the strongest negative links with positive mental health outcomes (Table 3). Third, transformational and destructive leadership explained the largest shares of variance regarding negative mental health outcomes, albeit with an opposite direction of associations, namely, negative for transformational leadership and positive for destructive leadership. Laissez-faire, relations- and task-oriented leadership, and LMX explained unique shares of the variance in followers’ negative mental health outcomes as well. Fourth, transactional leadership did not explain incremental variance in followers’ overall mental health as well as in positive or negative mental health.
Although the findings confirm the importance of transformational leadership for enhancing positive mental health and reducing negative mental health outcomes, destructive leadership is on a par with the predictive power of transformational leadership. Furthermore, other leadership constructs revealed an important incremental contribution to explained variance, especially laissez-faire leadership, relations- and task-oriented leadership, and LMX. The incremental contribution of transactional leadership, however, was very low, thereby providing additional support to the notion that there is a substantial conceptual overlap with transformational leadership (cf. Judge & Piccolo, 2004). This overlap might also prevent the hypothesized augmentation effect, at least in view of mental health outcomes (Bass & Avolio, 1993; see also below).
Theoretical Implications
Concerning the theoretical implications of our research, we would like to stress the following four aspects. First, we go beyond extant meta-analyses studying either the associations of transformational and transactional leadership with classical leadership outcomes (i.e., followers’ satisfaction and performance; e.g., Dumdum et al., 2013; Gottfredson & Aguinis, 2016; Lowe et al., 1996; Wang et al., 2011) or focusing on construct proliferation in view of these criteria (Hoch et al., 2016), by studying the association of seven leadership styles with followers’ mental health. Even though the behavioral components of the different leadership styles may show signs of construct proliferation (e.g., Banks et al., 2018; Bormann & Rowold, 2018; Hoch et al., 2016) and even though the related leadership styles are often highly correlated, especially transformational leadership, relations-oriented leadership, and LMX, our findings indicate that they are not interchangeable with regard to followers’ mental health. In contrast, all included leadership styles—with the exception of transactional leadership—explained incremental variance beyond transformational leadership with regard to followers’ mental health. Given the conceptual overlap and the often considerable empirical association between these styles, this result is noteworthy and relevant both from a theoretical and an applied perspective.
Second, as transactional leadership did not explain incremental variance in followers’ mental health, our results did not support the assumption of an augmentation effect, which would have been reflected in transformational leadership building on transactional leadership and extending its effect (Bass & Avolio, 1993). Thus, at least in relation to mental health outcomes, this augmentation effect does not seem to exist (see, however, Judge & Piccolo, 2004, for support of the augmentation effect in the domain of performance-related outcomes). Because the augmentation effect is a central tenet of the full range of leadership model (Bass & Avolio, 1993), future research is desirable that clarifies why transactional leadership explains incremental variance in followers’ performance (Judge & Piccolo, 2004), but not in followers’ mental health.
Third, another important result of the present study concerns the predictive power of laissez-faire and, especially, destructive leadership. The potential detrimental effects of these leadership styles concern not only increasing levels of affective symptoms, burnout, and health symptoms, but also a substantial reduction of positive mental health outcomes. However, the mediating processes accounting for the observed correlations likely differ for both negative leadership styles: Whilst destructive leadership may evoke negative feelings such as distress (Glasø et al., 2018), shame, fear, and nervousness owing to one’s leader’s mockery, abusive language, and continuous reproaching, laissez-faire leadership would rather evoke negative feelings such as distress, anger or irritability owing to the consequences of the leader’s lack of decision making and action (Skogstad et al., 2007). Nonetheless, the results (see Tables 2 and 3) indicate larger associations for destructive leadership than laissez-faire leadership, and equally strong associations for destructive leadership and transformational leadership for overall and negative mental health outcomes.
Fourth and finally, the finding that destructive leadership as a negative stimulus does not seem to be more strongly associated with followers’ mental health outcomes than leadership styles with a positive valence (such as transformational leadership) is meaningful: At least in the current domain, it indicates that “bad” is not necessarily stronger than “good” (Baumeister et al., 2001; Rozin & Royzman, 2001). Thus, although the principle of bad being stronger than good has been found in various domains of human experience and behavior (e.g., negative vs. positive or neutral information receiving more attention, Ito et al., 1998; negative information being shared more in social contexts, Bebbington et al., 2017; the use of more elaborate language to describe negative events, Rozin & Royzman, 2001; and the effects of negative interactions in the work context overshadowing the effects of simultaneous positive interactions, Duffy et al., 2002), it does not necessarily generalize to all domains. Although destructive leaders may be perceived as especially negative (Rozin & Royzman, 2001), non-destructive leaders acting for instance in transformational or relations-oriented ways may induce a positivity bias as part of an encompassing positive-negative asymmetry (Peeters & Czapinski, 1990). In other words, followers may respond especially positively to a leader showing a positive leadership style because in this social situation they may “[…] achieve at least some of the scarce positive life outcomes possible in a world with a much larger potential for negative outcomes” (Peeters & Czapinski, 1990, p. 38).
Practical Implications
Our results suggest that leadership development programs can be optimized to favorably impact followers’ overall mental health by focusing on the core behavioral characteristics associated with transformational leadership (e.g., Kelloway et al., 2000; for an overview, see Day, 2011). By additionally taking into account the contribution of task-oriented and relations-oriented leadership to positive mental health, leadership trainings may also address the importance of an adequate balance between a clear definition of goals and work tasks and the building and maintenance of trustful, respectful, and considerate relationships with followers. At the same time, given the large influence of destructive leadership or laissez-faire on mental health, leader development programs should also explicitly address potential antecedents and the detrimental consequences of those types of leader behaviors, and provide some guidance on appropriate policies and strategies to hinder or restrain their occurrence.
Building upon leadership development programs, organizations could define ideal versus negative leadership prototypes as a foundation for normative and explicit leadership models. These prototypes could either mirror the ideal prototype of a visionary, considerate, motivating, trustful, and authentic leader that could be the normative reference for fostering the enactment of more effective and desirable forms of leadership in organizations (i.e., a prescriptive norm). Alternatively, they could depict the negative prototype of a neglecting, absent, or aggressive leader, which may help organizations to define unacceptable forms of norm deviance among leaders (i.e., a proscriptive norm). By creating such normative and explicit leadership models, organizations may advance social norms hindering forms of laissez-faire leadership and destructive leadership (see Schyns & Schilling, 2013).
Limitations
In the following, we will discuss the most important limitations of our study: First, the analyses focused on the leadership styles investigated most frequently and simultaneously in the included primary studies. In the future, empirical studies may focus on a different set of leadership theories (for a review, see Dinh et al., 2014) to be more comprehensive and improve the understanding of the interplay of different organizational factors in the enactment and experience of leadership in organizations. Moreover, except for five studies that were written in German, we included only studies that were written in English. Future cross-cultural meta-analytical studies are desirable that are conducted by authors from different countries who can also understand and assess studies written in further languages (e.g., Chinese). Future studies could also study further potential contextual boundary conditions such as the leaders’ hierarchy level or the type of organization that we did not consider in our analysis.
A second limitation concerns the unequal distribution of comparisons of leadership styles and mental health constructs in the included studies, which prevents a more detailed analysis of comparisons among the leadership constructs. However, concerning the main research hypotheses of our study, this limitation does not have consequences for our conclusions since the variance estimate is the within-study variance for all comparisons in the models. Third, most studies focused solely on negative mental health outcomes (i.e., 151 vs. 66 correlations), respectively and, therefore, the estimates of variance pertaining to positive mental health outcomes are in comparison somewhat larger (Table 3). However, the relative contribution of leadership styles to mental health found in this meta-analytic study mirrors the main findings of the Global Leadership and Organizational Behavior Effectiveness (GLOBE) project, a large cross-national study involving the comparison of different leadership attributes. According to the GLOBE findings, some of the most desirable leadership attributes included being trustworthy, just, honest, encouraging, and motivational, which usually characterize, for instance, transformational or relations–oriented leadership behavior (Avolio & Bass, 1995; Bass & Bass, 2008). By contrast, being a loner, asocial, non-cooperative, irritable, ruthless, and dictatorial (i.e., mirroring destructive leadership behavior; Krasikova et al., 2013) were considered as the most undesirable leadership attributes (Dorfman et al., 2004).
Fourth and finally, the present investigation is limited regarding potential mediation processes at the junctions between leadership and mental health outcomes, which is due to the primary studies that could be included in our analysis. Inceoglu et al. (2018) proposed a framework on mediators for different leadership styles and followers’ well-being and outlined five general mediator-categories, namely social-cognitive, motivational, affective, relational or identification mediators. We encourage future research on mediators of leadership and mental well-being, which would allow investigating the relative importance of different leadership styles for the proposed mediators and followers’ resulting mental health.
Conclusions
The results obtained in the present meta-analysis indicate that transformational, relations-oriented, and task-oriented leadership have the most favorable, whereas destructive leadership and laissez-faire leadership have the least favorable association with followers’ mental health. Even though the behavioral components of the different leadership styles may show signs of construct proliferation, our findings emphasize that most included leadership styles—except for transactional leadership—contribute to explained variance beyond transformational leadership in regard to followers’ mental health. Moreover, the included leadership styles revealed specific relations with positive versus negative mental health outcomes: Whereas transformational and destructive leadership were the strongest predictors of overall mental health, relations- and task-oriented leadership were the best predictors of positive mental health outcomes. Leadership development programs may benefit from an explicit focus on behavioral leadership patterns inducing a favorable impact on followers’ mental health, and, at the same time, eliminating the detrimental impact arising from destructive leadership.
Supplemental Material
sj-pdf-1-jlo-10.1177_15480518221114854 - Supplemental material for A Meta-Analysis of the Relative Contribution of Leadership Styles to Followers’ Mental Health
Supplemental material, sj-pdf-1-jlo-10.1177_15480518221114854 for A Meta-Analysis of the Relative Contribution of Leadership Styles to Followers’ Mental Health by Diego Montano, Joyce Elena Schleu and Joachim Hüffmeier in Journal of Leadership & Organizational Studies
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
J
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.