
Abstract
Background:
Neurogenic overactive bladder (OAB) among survivors is burdensome. Low-frequency repetitive transcranial magnetic stimulation (rTMS) is a promising non-invasive intervention requiring comprehensive evaluation of its clinical and economic impact.
Objectives
To evaluate the efficacy, cost-utility, and stroke survivors’ experiences of rTMS for neurogenic OAB.
Methods
In this randomized, assessor-blinded, sham-controlled trial, 60 stroke survivors with neurogenic OAB received active rTMS (1200 pulses 80% resting motor threshold [RMT]) or sham (20% RMT) thrice weekly for 4 weeks at contralateral primary motor cortex. The OAB Symptom Score (OABSS), Incontinence Quality of Life (I-QOL), and Brief Resilience Scale (BRS)—were measured at baseline, week 4, and week 8. Repeated measures analysis of covariance evaluated effects. Cost-utility analysis used societal costs and quality-adjusted life years (QALYs). Focus groups involved 12 active-group participants.
Results
Active rTMS (n = 30; 60% male; mean age = 62.1 ± 9.5 years) significantly improved OABSS (mean difference [MD] = 1.81 points, 95% confidence interval [CI] [1.42-2.20], P < .001), I-QOL (MD = 17.48 points, 95% CI [14.18-20.79], P < .001), and BRS (MD = 0.25 points, 95% CI [0.09-0.41], P = .002), at weeks 4 and 8 compared to sham (n = 30; 47% male; mean age = 61.7 ± 8.3 years). Active rTMS was associated with lower societal costs (HK$1267.3 vs HK$1839.0) and higher QALYs (0.691 vs 0.571) than sham. Qualitative data indicated excellent tolerability, symptom relief, and acceptability.
Conclusions
Low-frequency rTMS is clinically effective, safe, acceptable, and potentially cost-saving for post-stroke neurogenic OAB. Larger trials with active comparators and extended follow-up are warranted.
Trial Registration
This trial was registered at http://ClinicalTrials.gov (reference number: NCT05557175) before the recruitment of the first participant.
Keywords
Introduction
Neurogenic overactive bladder (OAB), characterized by urinary urgency, frequency, and nocturia due to neurological injury such as stroke, affects 32% to 79% of stroke survivors.1,2 Its pathophysiology involves disruption of the neuromicturition pathways, impairing suprapontine inhibitory control and resulting in detrusor overactivity. 3 The condition significantly diminishes quality of life, elevates the risk of institutionalization, and exacerbates psychological distress. 4 Furthermore, neurogenic OAB imposes a substantial economic burden; estimated annual costs in the United States range from $65.9 to $82.6 billion, approximately 2 to 3 times higher than those associated with idiopathic OAB. 5
Current non-pharmacological interventions for OAB have notable limitations when applied to stroke survivors with neurogenic OAB. Behavioral therapies, such as prompted voiding and bladder training, often face implementation challenges in individuals with cognitive deficits, potentially leading to reduced adherence and frustration.6,7 While direct evidence linking these interventions to psychological distress in stroke survivors is limited, their feasibility is often compromised. Pelvic floor muscle training, although generally safe, may be contraindicated or less effective in patients with spasticity, poor motor control, or hypertonic pelvic floor muscles.7,8 Case reports have even described transient symptom exacerbation in some neurologically impaired individuals.7,8 In contrast, low-frequency repetitive transcranial magnetic stimulation (rTMS) offers a non-volitional, centrally mediated neuromodulatory approach. It does not rely on active patient participation or voluntary muscle contraction, thereby bypassing the risks associated with behavioral and pelvic floor training. By directly targeting the cortical-subcortical pathways involved in micturition control, rTMS represents a promising alternative strategy. 9
Non-invasive rTMS has emerged as a promising intervention for neurogenic OAB. By modulating corticospinal inhibition, it can reduce detrusor overactivity. 10 Building on evidence that low-frequency rTMS (1 Hz) modulates bladder function in neurologically impaired populations, we hypothesized that applying inhibitory low-frequency rTMS to the contralesional primary motor cortex (M1) would reduce its maladaptive hyperactivity—a phenomenon that occurs post-stroke due to a loss of transcallosal inhibition from the lesioned hemisphere. 11 By downregulating this contralesional overactivity, the intervention aims to restore interhemispheric balance, disinhibit the ipsilesional cortex, and normalize descending corticospinal control over the pontine micturition center, ultimately alleviating neurogenic OAB symptoms. 12 While a recent randomized controlled trial has demonstrated the efficacy of rTMS for post-stroke neurogenic OAB, 13 critical knowledge gaps remain regarding its cost-utility, its effect on stroke survivors’ resilience, and the lived experience of treatment. To address these gaps, this study aimed to: (1) compare the effectiveness of active versus sham rTMS on neurogenic OAB symptoms, quality of life, and resilience; (2) evaluate its cost-utility from a societal perspective; and (3) qualitatively explore stroke survivors’ experiences with the rTMS intervention.
Methods
Study Design and Setting
This was a prospective, 2-arm, assessor-blinded, randomized sham-controlled trial, with an embedded cost-utility analysis and a qualitative component. The study was conducted at the Neuro-modulatory Laboratory in the Department of Rehabilitation Sciences at The Hong Kong Polytechnic University between January 2023 and January 2025. Ethical approval was obtained from the Institutional Review Board of The Hong Kong Polytechnic University (Reference No. HSEARS20210913002). The trial was prospectively registered on ClinicalTrials.gov (NCT05557175). All participants provided written informed consent prior to enrollment.
Sample Size Calculation
The sample size was calculated a priori using G*Power software (v3.1.9.7) based on an expected effect size (f) of 0.40 for the primary outcome (OAB Symptom Score [OABSS]), with 80% power and a 5% significance level (α = .05). 14 This analysis determined that 52 participants were required. To account for an anticipated 15% attrition rate, the sample was increased to 60 participants, with 30 allocated to each group. For the qualitative component, a sample of 12 participants from the active group was targeted to achieve thematic saturation, aligning with established recommendations for focus group sizes (6-15 participants). 15
Participant Recruitment and Eligibility
Participants were recruited using snowball sampling methods and through printed advertisements posted on noticeboards at The Hong Kong Polytechnic University, as well as via digital advertisements circulated in local stroke community WhatsApp groups. Interested volunteers contacted the research team by telephone and were subsequently invited for an in-person eligibility screening at the university. Following the week 8 follow-up, a subset of twelve participants from the active rTMS group were recruited via convenience sampling to participate in focus group discussions.
Eligible participants were stroke survivors aged 18 to 80 years who presented with moderate (OABSS 6-11 points) to severe (OABSS ≥12 points) neurogenic OAB symptoms. 16 Additional inclusion criteria required a Mini-Mental State Examination score of ≥24, indicating intact cognitive function, 17 and willingness to undergo randomization. Exclusion criteria comprised: (1) any contraindication to rTMS, as assessed by the 13-item TMS safety screening questionnaire, 18 (2) pregnancy or being within 6 months postpartum, (3) concurrent participation in other urinary incontinence-related research, (4) contraindications for magnetic resonance imaging (eg, metallic implants and claustrophobia), or (5) a history of urological cancer, significant prostatic pathology, or severe pelvic pain.
Randomization and Blinding
Randomization was performed by an independent research assistant using a computer-generated sequence. Allocation concealment was ensured with sequentially numbered, sealed, opaque envelopes containing assignment cards, which were prepared by the same assistant and opened only after baseline data collection. To maintain blinding, outcome assessors and the statistical analyst were provided with group codes labeled only as “Group A” and “Group B.” The assignment key remained concealed until all data analyses were finalized.
Interventions
Participants were randomly allocated to receive either active or sham low-frequency rTMS. The intervention was administered 3 times per week over 4 weeks, totaling 12 sessions. Each session lasted 20 minutes.
Active rTMS
Participants in the active rTMS group received low-frequency inhibitory stimulation administered via a 70-mm figure-of-eight, air-cooled coil (MagPro) targeting the contralesional M1. 19 The stimulation site was localized to the anterior-medial precentral gyrus, guided by the interhemispheric imbalance model of post-stroke recovery. According to this model, stroke reduces transcallosal inhibition, leading to pathological hyperactivity in the contralesional M1. Low-frequency rTMS is thought to downregulate this hyperactivity, thereby facilitating reactivation of the ipsilesional cortex and enhancing suprapontine inhibitory control over micturition reflexes.12,20 The motor hotspot was functionally defined as the scalp position that elicited the largest and most consistent visible contraction in the contralateral gluteal or lower abdominal muscles at the lowest stimulation intensity. This pragmatic approach leverages the well-documented synergistic activation between pelvic floor muscles and trunk/hip extensors.21,22 To verify accurate localization within the M1, a brief increase in stimulation intensity at this site reliably evoked motor-evoked potentials (MEPs) and visible twitches in the contralateral first dorsal interosseous muscle in all participants.18,23 The resting motor threshold (RMT) was then determined at this hotspot as the minimum intensity required to produce a MEP of ≥50 µV in at least 5 out of 10 consecutive trials in the target muscles. 19 The coil was positioned tangentially to the scalp with the handle oriented approximately 45° to the midline. 24 Each 20-minute session consisted of 1200 pulses delivered at an intensity of 80% of the participant’s RMT. 25
Sham rTMS
Sham rTMS was administered using the same coil, placement, orientation, and auditory feedback as the active treatment, but with stimulation intensity set to 20% of the RMT. This low-intensity active-coil sham is an established and well-validated control method in rTMS research.26,27 It generates negligible cortical electric fields (<50 V/m) and does not produce motor-evoked potentials, while preserving the scalp sensations (tingling and local muscle twitching) and audible click that are perceptually similar to active stimulation.18,28 Compared to alternative sham techniques—such as coil tilting or placebo coils—real-coil, low-intensity stimulation (10%-20% RMT) has demonstrated comparable rates of successful participant blinding in low-frequency rTMS protocols, with participants unable to reliably distinguish it from active stimulation.18,29,30
Outcome Measures
Outcome measures were assessed at baseline (week 0), immediately after the 4-week intervention (week 4), and at a 4-week post-intervention follow-up (week 8). At baseline, sociodemographic and clinical characteristics—including age, sex, occupation, education, employment status, stroke-affected side, and time since stroke—were collected.
Primary Measure
Neurogenic OAB Symptoms Severity
The OABSS, a validated and psychometrically robust instrument, was used to evaluate neurogenic OAB symptom severity. 31 It demonstrates excellent internal consistency (Cronbach’s α = .92) and test–retest reliability (intraclass correlation coefficient [ICC] = .95), 31 with good reliability also confirmed in the Hong Kong population (ICC = .82). 32 The established minimal clinically important difference (MCID) for the OABSS is a change of ≥3 points, as derived from anchor-based methods in stroke survivors with moderate-to-severe OAB. 33
Secondary Measures
OAB-Related Quality of Life
The Incontinence Quality of Life (I-QOL) questionnaire assessed OAB-related quality of life. 34 The I-QOL demonstrates excellent internal consistency (Cronbach’s α = .99) and test–retest reliability (intraclass correlation coefficient = .99). Its convergent validity is supported by strong correlations with the King’s Health Questionnaire (Pearson’s r = .76-.88). 35 The Chinese version used in this study also shows high internal consistency (Cronbach’s α = .82). 34 A change of ≥10 points on the I-QOL represents the established MCID for stroke survivors with moderate-to-severe OAB, as determined through anchor-based methods. 36
Resilience
The Brief Resilience Scale (BRS) measured resilience, comprising positively (items 1, 3, and 5) and negatively (items 2, 4, and 6) worded statements. 37 The BRS has demonstrated good internal consistency (Cronbach’s α = .71-.91) and acceptable test–retest reliability (intraclass correlation coefficient = .69) in the Hong Kong Chinese population. 37
Adherence
Adherence was calculated as the percentage of prescribed rTMS sessions attended, determined by dividing the number of sessions attended by the total prescribed (12) and multiplying by 100.
Economic Evaluation
An economic evaluation was conducted to assess the cost-utility of active versus sham rTMS for managing post-stroke neurogenic OAB. The analysis adopted a societal perspective, incorporating data from the Client Service Receipt Inventory (CSRI) 38 and the 5-Level EuroQol 5 Dimension (EQ-5D-5L) questionnaire collected at baseline and week 8. 39 Quality-Adjusted Life Years (QALYs) were derived using the Hong Kong value set. Total societal costs included direct intervention delivery, healthcare resource utilization, medications, transportation, and the value of informal care.
Qualitative Study
A qualitative component was integrated to explore the lived experiences of stroke survivors receiving active rTMS for neurogenic OAB. Following the week 8 follow-up, 12 participants from the active group were recruited via convenience sampling and assigned to 3 focus groups (4 participants each). Sessions were conducted face-to-face in a university setting, lasted 45 to 60 minutes, and were audio-recorded and transcribed verbatim. Only participants who received active rTMS were included to enable an in-depth exploration of the intervention experience, as those in the sham group did not receive the active treatment. 40 The complete qualitative methodology is described elsewhere. 41
Safety and Adverse Events
rTMS is a non-invasive neuromodulation technique with a well-established safety profile, particularly suitable for stroke survivors. Common side effects, such as transient mild headache or scalp discomfort, are typically self-limiting. 42 To ensure participant safety, eligibility was confirmed using a standardized 13-item rTMS screening questionnaire. 43 Throughout the trial, adverse events were actively monitored during and after each treatment session and systematically documented.
Statistical Analysis
Analyses were conducted according to the intention-to-treat principle. For the week 8 endpoint, missing data from 3 participants (5%) were imputed using the last observation carried forward method. 44 The robustness of the results was confirmed via a sensitivity analysis employing multiple imputation by chained equations (20 imputations), which yielded virtually identical estimates (Supplemental Table S4). Primary efficacy outcomes—changes in OABSS, I-QOL, and BRS from baseline to weeks 4 and 8—were analyzed using repeated-measures analysis of covariance, with adjustment for the pre-specified covariates of age and sex. Effect sizes are reported as partial eta-squared (η²), interpreted as small (.01 ≤ η² < .06), medium (.06 ≤ η² < .14), or large (η² ≥ .14).45,46 Economic evaluation employed seemingly unrelated regression to estimate the difference in total societal costs (ΔC) and quality-adjusted life years (ΔE) between groups. QALYs were derived by converting EQ-5D-5L responses to utility scores using the Hong Kong value set, enabling the calculation of incremental net monetary benefit. Qualitative data from focus groups were transcribed verbatim by an independent service, with transcripts verified against audio recordings for accuracy. Further statistical detail is available in the Supplemental Methods.
Results
Participant Flow and Baseline Characteristics
Figure 1 presents the participant flow through the trial. Of 110 consecutively screened stroke survivors, 60 met the eligibility criteria for neurogenic OAB and were enrolled. Participants were randomly allocated to the active (n = 30) or sham (n = 30) rTMS group. Baseline sociodemographic and clinical characteristics, detailed in Table 1, were comparable between groups. Participants’ ages ranged from 37 to 78 years, with a mean age of 62.10 years (standard deviation [SD] = 9.54) in the active rTMS group and 61.67 years (SD = 8.29) in the sham rTMS group. The cohort comprised 32 males (53.3%) and 28 females (46.7%).

Flow of study participants through the trial.
Baseline Characteristics of the Study Participants.

Abbreviations: I-QOL, Incontinence Quality of Life Questionnaire; OABSS, Overactive Bladder Symptom Score; rTMS, repetitive transcranial magnetic stimulation.
Effectiveness of rTMS Interventions
The primary inferential analysis—comparing the active and sham rTMS groups at weeks 4 and 8, with adjustments for age, sex, and baseline scores—is detailed in Table 2 and Figure 2. These analyses demonstrate that active rTMS produced outcomes that were statistically superior and clinically meaningful across all efficacy measures when compared to sham stimulation.
Comparison of the Primary and Secondary Outcome Measures.
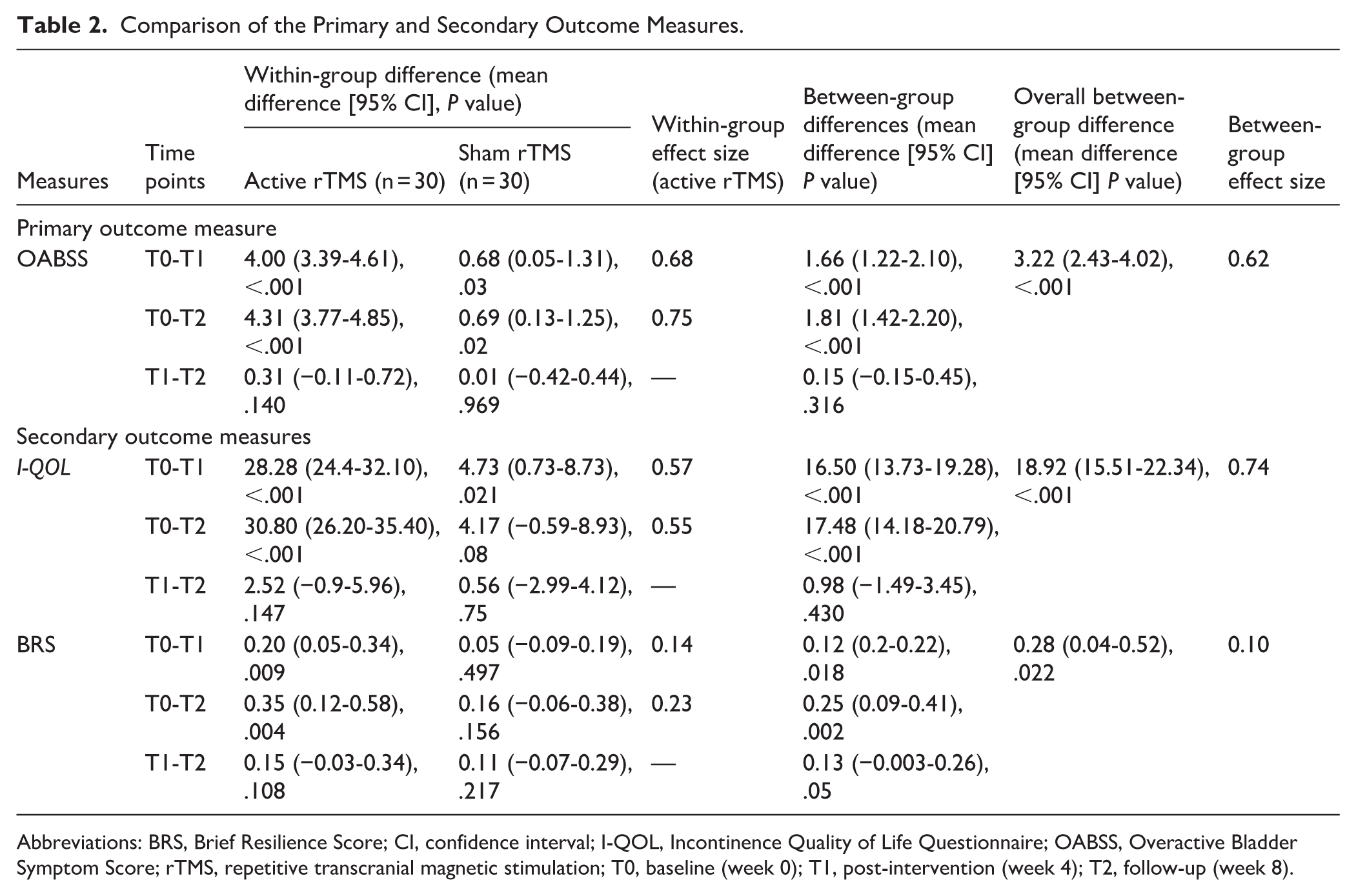
Abbreviations: BRS, Brief Resilience Score; CI, confidence interval; I-QOL, Incontinence Quality of Life Questionnaire; OABSS, Overactive Bladder Symptom Score; rTMS, repetitive transcranial magnetic stimulation; T0, baseline (week 0); T1, post-intervention (week 4); T2, follow-up (week 8).

(A) Mean Overactive Bladder Symptom Score for overactive bladder symptoms in the active repetitive transcranial magnetic stimulation group was significantly lower than in the sham- repetitive transcranial magnetic stimulation. (B) The mean Incontinence Quality of Life for overactive bladder-related quality of life in the repetitive transcranial magnetic stimulation group demonstrated a significantly greater improvement in the quality of life compared to the sham-repetitive transcranial magnetic stimulation group. (C) Mean brief resilience scale scores for resilience in the active- repetitive transcranial magnetic stimulation group show a significant improvement in resilience compared to the sham- repetitive transcranial magnetic stimulation group.
Primary Outcome: Neurogenic OAB Symptom Severity (OABSS)
Active rTMS produced significantly greater reductions in OAB symptom severity than sham, at week 4 (MD = 1.66 points, 95% confidence interval [CI] [1.22-2.10], P < .001) and week 8 (MD = 1.81 points, 95% CI [1.42-2.20], P < .001), corresponding to a very large effect size (partial η² = .62). While this between-group difference did not reach the commonly cited MCID of ≥3 points, 33 the active treatment group achieved a mean within-group reduction of 4.31 points from baseline to week 8 (95% CI [3.77-4.85], P < .001), exceeding this clinical threshold. This meaningful symptom improvement was further corroborated by very large effect sizes on secondary outcomes, including quality of life and resilience.
Secondary Outcomes
OAB-Related Quality of Life (I-QOL)
Active rTMS yielded significantly greater improvements in I-QOL scores compared to sham at week 4 (MD = 16.50 points, 95% CI [13.73-19.28], P < .001) and week 8 (MD = 17.48 points, 95% CI [14.18-20.79], P < .001), with a very large effect size (partial η² = .74). These observed gains exceeded the established MCID of ≥10 points.36,47
Resilience (BRS)
Active rTMS produced a statistically significant greater increases in resilience compared with sham at week 4 (MD = 0.12 points, 95% CI [0.02-0.22], P = .018) and week 8 (MD = 0.25 points, 95% CI [0.09-0.41], P = .002), with a medium effect size (partial η² = 0.10), consistent with clinically relevant enhancement of psychological resilience. Baseline-to-follow-up within-group changes are detailed in Supplemental Table S3.
Preliminary Cost-Utility
Supplemental Table S3 details the socioeconomic characteristics and support services received by participants. Notably, 63% (n = 38) of participants received care from unpaid caregivers, primarily spouses (50%), 82% (n = 49) had a monthly income of <HK$20 000, and 95% (n = 57) received government social support (eg, disability or old age allowance).
The economic evaluation showed that active rTMS incurred lower mean total costs (HK$1267.3, 95% CI [1148.2-1386.5]) and generated higher QALYs (0.691, 95% CI [0.364-1.000]) than sham (HK$1839.0, 95% CI [1654.2-2023.8]; 0.571, 95% CI [0.251-0.890]). This resulted in active rTMS dominating sham (lower cost and higher effectiveness), with a cost-saving of HK$572 per stroke survivors and 0.120 additional QALYs (Table 3; Supplemental Figure S2). However, the lack of an active comparator (eg, standard pharmacotherapy) precludes formal cost-effectiveness conclusions.
Costs Associated With Active rTMS and sham rTMS Groups.

Abbreviations: MTR, mass transit railway; rTMS, repetitive transcranial magnetic stimulation.
The costs for all resources are denominated in Hong Kong Dollars (HK$) for the year 2024.
Qualitative Findings
Twelve participants from the active rTMS group participated in focus group discussions (mean age = 60.12 ± 7.22 years; 58.3% male). Four key themes emerged from the qualitative analysis (Table 4): (1) perceived improvement in neurogenic OAB symptoms, (2) a favourable safety profile, (3) a sense of fulfillment derived from treatment, and (4) experienced social benefits. Representative participant statements included: After completing the first week of treatment, I improved a lot in the whole month. (P1) The rTMS treatment session is very fine; everything goes well. (P11) Now, I can hold my urine better. I feel more relaxed, happier, it’s good. (P8) Now I can go out on the street or to other places without worrying too much. (P2)
Overview of Themes and Subthemes Generated From Participants’ Experiences With the rTMS Intervention.

Abbreviations: OAB, Overactive Bladder; rTMS, repetitive transcranial magnetic stimulation; UUI, urgency urinary incontinence.
Safety of rTMS
The rTMS intervention was well-tolerated in both groups. A total of 3 mild, transient adverse events were reported: 2 headaches in the active group and 1 in the sham group. All resolved spontaneously within 24 hours without requiring analgesia or leading to sequelae. No serious adverse events, seizures, or treatment discontinuations occurred. The per-session adverse event rate was low (0.56% for active; 0.28% for sham), confirming an excellent safety profile consistent with the established use of rTMS in stroke populations. Supplemental Figure S1 illustrates the intervention setup, depicting coil placement over the right M1 and modeled electric field distributions for both active and sham conditions.
Adherence
Adherence was excellent, with all participants completing the full 12-session rTMS protocol, resulting in a 100% completion rate during the 4-week intervention period. Follow-up was also high, with a 95% retention rate at the 8-week endpoint; 3 participants were lost to follow-up due to scheduling conflicts (Supplemental Table S1).
Discussion
This randomized, assessor-blinded, sham-controlled trial demonstrates that low-frequency rTMS targeting the medial precentral gyrus (M1 cortex) is a safe and effective intervention for neurogenic OAB in stroke survivors, yielding statistically and clinically significant improvements in symptom severity, quality of life, and resilience. While the between-group difference in OABSS (1.81 points) did not reach the conventional MCID of ≥3 points, this statistically robust result (partial η² = .62) represents a meaningful clinical effect. 33 The active rTMS group’s mean within-group improvement of 4.31 points from baseline did surpass this threshold, indicating substantial symptom relief for treated stroke survivors. This is strongly corroborated by the marked gains in I-QOL MD = 17.5 points, exceeding its MCID of ≥10) and qualitative reports of reduced urgency and improved bladder control. From an economic perspective, active rTMS was dominant over sham, associated with lower societal costs and higher QALYs (incremental cost −HK$572; incremental QALY +0.120). These preliminary cost-utility findings are promising, though formal cost-effectiveness against standard care remains to be established. The experiences of stroke survivors were overwhelmingly positive, with focus group data highlighting themes of enhanced control, regained confidence, and high treatment acceptability.
These outcomes are consistent with established neuromodulatory principles. Specifically, the reduction in bladder overactivity aligns with evidence that low-frequency rTMS decreases corticospinal excitability, a mechanism previously shown to mitigate detrusor overactivity in other neurological disorders. 48 The larger effect sizes observed in our trial compared to prior work by Chen et al, 13 (0.81-1.05 for OABSS) may be attributed to our use of a higher pulse count per session (1200 vs 600), which plausibly induces more robust and sustained modulation of the cortico-subcortical networks disrupted in post-stroke OAB.49,50 These clinical gains support our mechanistic hypothesis. Inhibitory rTMS applied to the contralesional M1 is posited to reduce pathological interhemispheric inhibition, thereby facilitating the disinhibition and functional recovery of the ipsilesional motor network. This cortical rebalancing is likely to strengthen descending inhibitory control over the pontine micturition center, a pathway substantiated by evidence from both motor recovery and bladder neuromodulation studies.10,13,50,51
The rTMS protocol targeted the medial region of the primary motor cortex (M1), consistent with neuroanatomical mappings of pelvic floor muscle (PFM) and gluteus maximus control to this area.22,52 Mechanistically, low-frequency stimulation is hypothesized to modulate key brainstem centers, such as the pontine micturition center or periaqueductal gray, thereby reducing excessive excitatory drive to sacral parasympathetic nuclei and subsequent detrusor overactivity.13,53 This aligns with the understanding that stroke disrupts suprapontine inhibitory control, leading to the high prevalence (32%-79%) of OAB in survivors.1,2 The intervention’s proposed effect of inversely modulating corticospinal projections to the detrusor muscle further supports this pathway.10,54 Methodologically, the trial utilized a non-invasive approach for cortical targeting, capitalizing on the functional synergy between the PFM and gluteus maximus. The motor hotspot was identified via visible gluteal contraction, with accurate M1 localization confirmed by eliciting motor-evoked potentials in the contralateral first dorsal interosseous muscle.21,55 This pragmatic method enhanced stroke survivors’ comfort and clinical feasibility by avoiding more invasive or complex assessments.
Neuroanatomically, the M1 cortex contains a distributed representation of the pelvic floor musculature. 22 This suggests that modulating M1 activity via rTMS could directly influence pelvic floor function and related bladder control. In the context of post-stroke neurogenic OAB, the proposed mechanism involves applying low-frequency rTMS to the contralesional M1. This is hypothesized to reduce pathological interhemispheric inhibition from the contralesional hemisphere, thereby facilitating the recovery of the ipsilesional cortex and rebalancing the cortico-subcortical networks governing micturition.10,54 In this study, we posit that such neuromodulation may have altered cortical excitability—potentially decreasing the RMT and increasing MEP amplitude—which subsequently translated into the observed clinical improvements in OAB symptom severity.
The trial outcomes suggest that rTMS modulates cortico-subcortical networks, potentially compensating for stroke-induced disruptions in neuromicturition pathways—a mechanism supported by existing neurophysiological evidence. 56 The intervention demonstrated high feasibility, with 100% adherence and a low rate of mild, transient adverse events, consistent with the established safety profile of rTMS in stroke populations. 57 The use of validated psychometric tools (OABSS, I-QOL, and BRS)31,34,37 strengthens the internal validity of the findings, with observed effect sizes indicating a robust clinical impact. By integrating efficacy, cost-utility, and the experiences of stroke survivors, this study addresses a key gap in prior neuromodulation research for OAB, 13 positioning low-frequency rTMS as a comprehensive and promising non-invasive therapy for neurogenic OAB in stroke rehabilitation.
The active rTMS group demonstrated both lower costs and higher Quality-Adjusted Life Years (QALYs) than the sham group, indicating that the intervention was dominant (more effective and less costly) in this comparison. However, from a health policy perspective, establishing cost-effectiveness requires a direct comparison with current standard care options, such as pharmacotherapy or behavioral training. 58 Therefore, while the observed dominance over sham is a promising and economically favorable preliminary result, it primarily supports the feasibility of rTMS and justifies future, definitive cost-effectiveness analyses against established treatments. Such future evidence could directly inform healthcare policy and resource allocation by identifying interventions that optimize clinical outcomes relative to economic investment. Given Hong Kong’s relatively high GDP per capita, the healthcare system may possess the capacity to invest in innovative, potentially cost-saving interventions like rTMS should subsequent comparative studies confirm its value.
The qualitative data revealed that participants experienced multiple clinical benefits from the rTMS intervention, including a reduction in core neurogenic OAB symptoms—specifically urinary frequency, urgency, and urgency incontinence—alongside improved quality of life and increased confidence. Participants generally reported positive experiences regarding the safety of the procedure. While some participants reported mild side effects, such as headaches and scalp discomfort, that disappeared before the next treatment session (24 hours), these were generally mild and transient, and did not interfere with their ability to complete the treatment sessions.59,60 The convergence of these positive qualitative findings with the results of the RCT and cost-utility analysis strengthens the overall evidence base and confidence in the study’s conclusions.
The findings of this trial should be interpreted within the context of its limitations. As a preliminary RCT, the single-site recruitment and moderate sample size may affect the generalizability of the results. The 8-week follow-up period is insufficient to evaluate the long-term durability of rTMS effects for a chronic condition such as neurogenic OAB. Several methodological choices, while justified, present avenues for refinement in future studies. For instance, the non-invasive localization of the M1 hotspot, although practical, lacks the precision of Electromyography (EMG)- or functional Magnetic Resonance Imaging (fMRI)-guided methods and could be influenced by co-contraction of adjacent muscles. The lack of formal blinding assessment means the potential influence of unblinding on subjective outcomes (OABSS, I-QOL, BRS, and qualitative reports) cannot be entirely ruled out. Furthermore, while the OABSS is a validated measure, future trials would benefit from incorporating condition-specific tools, such as the Neurogenic Bladder Symptom Score, to more comprehensively capture the spectrum of neurogenic bladder dysfunction. While our randomization achieved a reasonable balance, the lack of stratification by sex is a limitation. Given known pathophysiological differences in urological health between men and women, future studies should prioritize sex stratification to enable powerful subgroup analyses. Although missing data were minimal (5% at final follow-up) and a sensitivity analysis using multiple imputations confirmed the primary results, future studies with larger samples should preferentially employ multiple imputations or full information maximum likelihood as the primary approach. Despite these limitations, the internal validity of our findings is strengthened by the randomized sham-controlled design, high adherence, robust effect sizes on key outcomes, and convergent findings from our quantitative and qualitative data.
Conclusion
This randomized, sham-controlled trial demonstrates that low-frequency rTMS applied to the contralesional M1 cortex is a promising, non-invasive intervention for neurogenic OAB after stroke. Compared to sham, active rTMS yielded statistically significant and clinically meaningful improvements in quality of life (I-QOL gains exceeding MCID) and resilience, along with significant reductions in symptom severity on the OABSS. While the between-group difference in OABSS did not meet the conventional MCID of ≥3 points, the within-group improvement in the active arm surpassed this threshold, supported by very large effect sizes and qualitative reports of substantial symptom relief. From a societal perspective, active rTMS was dominant (lower costs and higher QALYs), well-tolerated, and associated with perfect adherence and uniformly positive stroke survivors’ experiences. These multidimensional findings support low-frequency contralesional M1 rTMS as a safe, acceptable, and potentially cost-saving treatment for post-stroke neurogenic OAB. Confirmatory trials with larger samples, active comparators, and extended follow-up are now warranted.
Supplemental Material
sj-docx-1-nnr-10.1177_15459683261432087 – Supplemental material for Clinical Efficacy and Preliminary Cost-Utility of Low-Frequency Repetitive Transcranial Magnetic Stimulation Versus Sham Stimulation for Neurogenic Overactive Bladder in Stroke Survivors: A Randomized Controlled Trial
Supplemental material, sj-docx-1-nnr-10.1177_15459683261432087 for Clinical Efficacy and Preliminary Cost-Utility of Low-Frequency Repetitive Transcranial Magnetic Stimulation Versus Sham Stimulation for Neurogenic Overactive Bladder in Stroke Survivors: A Randomized Controlled Trial by Mohammed Usman Ali, Kenneth N.K. Fong, Georg S. Kranz, Jingjing Li, Crystal Kwan and Priya Kannan in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
We would like to extend our appreciation to all study participants. We appreciate the contribution of Dr Jack Zhang, Mr Mohammad Jobair Khan and Ms Liu Zhaoxue.
Ethical Considerations
Ethical approval was obtained from the Institutional Review Board of the Hong Kong Polytechnic University (Ref No.: HSEARS20210913002. The study protocol was prospectively registered on ClinicalTrials.gov (NCT05557175).
Consent to Participate
Written informed consent was obtained from all participants.
Author Contributions
Mohammed Usman Ali: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Project administration; Resources; Software; Validation; Writing—original draft; and Writing—review & editing. Kenneth N.K. Fong: Conceptualization; Data curation; Investigation; Methodology; Project administration; Software; Supervision; Validation; and Writing—review & editing. Georg S. Kranz: Data curation; Formal analysis; Investigation; Methodology; Software; Supervision; Validation; and Writing—review & editing. Jingjing Li: Data curation; Formal analysis; Investigation; Methodology; Software; Validation; and Writing—review & editing. Crystal Kwan: Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Resources; Software; Validation; and Writing—review & editing. Priya Kannan: Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Resources; Software; Supervision; Validation; and Writing—review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Hong Kong Polytechnic University (Dean’s Reserve, Faculty of Health and Social Sciences (Department of Rehabilitation Sciences)). Ref No. ZVSV.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting this study’s findings are available from the corresponding author* upon reasonable request.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.