
Abstract
Background
Coordination between arm movements and postural adjustments is crucial for reaching-while-stepping tasks involving both anticipatory postural adjustments (APAs) and compensatory movements to effectively propel the whole-body forward so that the hand can reach the target. Stroke impairs the ability to coordinate the action of multiple body segments but the underlying mechanisms are unclear. Objective. To determine the effects of stroke on reaching performance and APAs during whole-body reaching.
Methods
We tested arm reaching in standing (stand-reach) and reaching-while-stepping (step-reach; 15 trials/condition) in individuals with chronic stroke (n = 18) and age-matched healthy subjects (n = 13). Whole-body kinematics and kinetic data were collected during the tasks. The primary outcome measure for step-reach was “gain” (g), defined as the extent to which the hip displacement contributing to hand motion was neutralized by appropriate changes in upper limb movements (g = 1 indicates complete compensation) and APAs measured as spatio-temporal profiles of the center-of-pressure shifts preceding stepping.
Results
Individuals with stroke had lower gains and altered APAs compared to healthy controls. In addition, step onset was delayed, and the timing of endpoint, trunk, and foot movement offset was prolonged during step-reach compared to healthy controls. Those with milder sensorimotor impairment and better balance function had higher gains. Altered APAs were also related to reduced balance function.
Conclusions
Altered APAs and prolonged movement offset in stroke may lead to a greater reliance on compensatory arm movements. Altered APAs in individuals with stroke may be associated with a reduced shift of referent body configuration during the movement
Introduction
Stroke often results in arm motor impairments1,2 and deficits in anticipatory postural adjustments (APAs). 3 Evidence for the influence of stroke on arm motor function is mostly derived from studies in seated subjects, with minimal requirements for postural adjustments. In daily activities, however, tasks are often performed during standing where APAs are required to maintain body balance and stability while reaching. We addressed this relationship by evaluating reaching performance and APAs during whole-body reaching while taking a forward step in subjects with and without stroke. One challenge associated with stepping during reaching is the large whole-body displacement that should not be transferred to the endpoint position.
When reaching from sitting, addition of trunk motion did not affect the final endpoint position due to a compensatory synergy, that is, the arm-trunk coordination that neutralizes the effect of forward trunk displacement on the forward arm reach extent by adapting elbow and shoulder movement. 4 They also considered a second, transport synergy for trunk-assisted-reaching, described as the arm movement that contributes to the forward reaching extent. These synergies are particularly important during reaching tasks that involve multiple body segments having different amounts of inertia. 5 Having greater mass, the trunk moves slower than the arm, and therefore, trunk movement usually starts before endpoint movement.6,7 Anticipatory recruitment of high-inertial body segments may play an important role in whole-body reaching. APAs are important during the transition from standing to stepping forward to initiate gait characterized by changes in ground reaction forces that move the center-of-pressure (COP) 8 beneath the feet backward and toward the swing limb, 9 as well as by electromyographic (EMG) activity occurring prior to stepping. These preparatory changes in COP position produce the forces and moments necessary to propel the body forward and toward the stance leg before and during voluntary step initiation. Studies have identified differences in APA patterns after stroke, such as reduced APA magnitude prior to gait initiation.10,11 Although the timing of anticipatory trunk recruitment during seated reaching was preserved in individuals with stroke, 12 the altered APAs for voluntary stepping during standing reaching may also affect the timing of arm and trunk recruitment in these patients. APA characteristics during reaching when taking a voluntary step in stroke subjects and their relationship to reaching performance remains unclear.
The biomechanical explanation provides us with information about specific biomarkers of disordered movement, but they may be insufficient to signal true motor recovery due to disordered motor control mechanisms. 13 Therefore, the objective of this study was to estimate the relationship between altered APAs after stroke and whole-body reaching performance, while considering the multiple degrees-of-freedom (DFs) involved in the task. We hypothesized that APA patterns during whole-body reaching would be altered in individuals with stroke, resulting in reduced reaching performance. Whole-body reaching was examined by evaluating endpoint and step characteristics, and postural stability in multi-dimensional domains. After describing the impact of stroke on the task in the traditional biomechanical framework, we discuss how body balance and stability during reaching while taking a step in healthy subjects and individuals with stroke can be considered in the framework of the Referent Control Theory (RCT). 14
Methods
Participants
Eighteen right-handed individuals with chronic stroke (age: 61.4 ± 7.9 years; height: 174.0 ± 8.0 cm; weight: 82.8 ± 18.9 kg) and 13 age-equivalent right-handed healthy individuals (controls: age: 64.7 ± 10.2 years; height: 171.4 ± 11.1 cm; weight: 75.8 ± 12.3 kg) participated after signing consent forms approved by the Ethics Committee of Centre for Interdisciplinary Research in Rehabilitation of Greater Montreal (CRIR). We included individuals who had: (i) unilateral stroke >6 months previously; (ii) unilateral hemiparesis with ≥3/7 on Chedoke–McMaster Stroke Assessment Arm Scale. 15 We excluded individuals who had: (i) history of multiple strokes; (ii) cognitive impairment (Montreal Cognitive Assessment [MoCA] <20/30 16 ; (iii) no upper limb (UL) and/or lower limb (LL) proprioception (Fugl-Meyer Assessment [FMA] 17 ); (iv) UL pain; (v) marked apraxia or visuospatial neglect; or (vi) could not stand independently. Healthy controls with history of neurological disorders/physical conditions that could influence task performance were excluded. No participant required assistive devices for indoor ambulation. Two participants used a single-point cane only when coming to the lab for the experiment.
Study sample size, determined utilizing G*Power 3.1.9.4 18 accounting for the effect size reported previously 19 indicated 11 participants per group (effect size: 1.75; α-level: 5%; power: 95%) for the group comparison using the Mann–Whitney U test. However, recognizing the heightened variance in kinematic outcomes attributed to stroke heterogeneity, the sample size was increased to 18 individuals with stroke.
Clinical Evaluation
Motor and sensory impairments and balance were evaluated by an experienced clinician using reliable and valid clinical scales (Table 1). FMA was used to measure UL (66 pt) and LL (34 pt) motor impairment. MoCA evaluated cognitive function. Brief Balance Evaluations Systems Test (B-BESTest 20 ) evaluated balance function. Balance confidence was evaluated using the Activities-specific Balance Confidence Scale (ABC scale). 21
Demographics, Median (Interquartile Range).
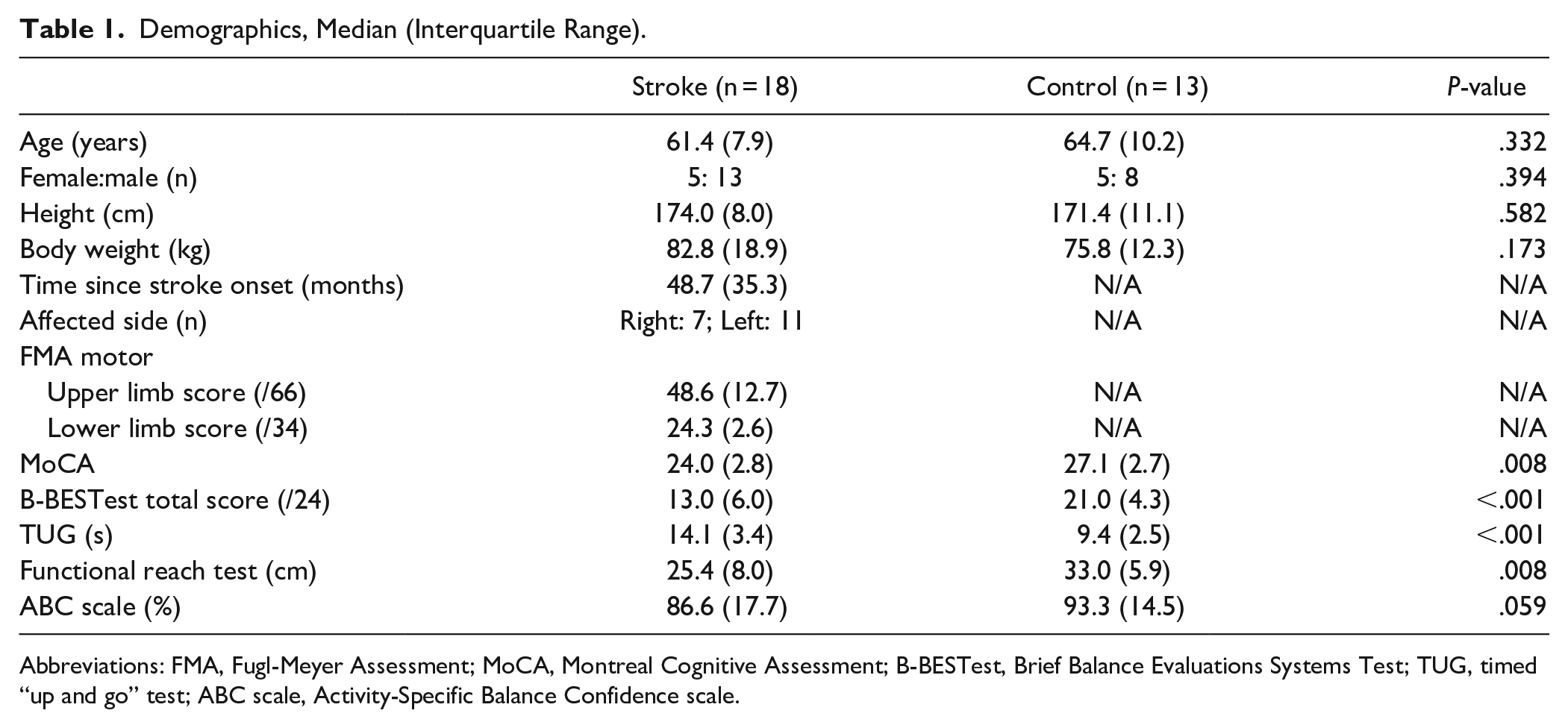
Abbreviations: FMA, Fugl-Meyer Assessment; MoCA, Montreal Cognitive Assessment; B-BESTest, Brief Balance Evaluations Systems Test; TUG, timed “up and go” test; ABC scale, Activity-Specific Balance Confidence scale.
Experimental Task
The more-affected and nondominant arms of individuals with and without stroke were tested, respectively. Subjects stood barefoot without assistive devices with 1 foot on each of 2 force platforms with feet shoulder-width apart and wore a ceiling-mounted safety harness to prevent falling. The target (light-emitting diode [LED]) was placed at 130% arm length measured from the acromion process to the index fingertip (endpoint) with elbow extended, at the height of the anterior superior iliac spine 22 on the tested side in the subject’s mid-sagittal plane. The endpoint starting position was standardized at the upper edge of the ipsilateral greater trochanter.
Before each trial, subjects visualized the target LED located on a retractable rod and then closed their eyes. On hearing a GO signal (beep), they reached with the arm as fast as possible to the remembered target to prevent visually guided corrective movements. The target was retracted with the GO signal to eliminate haptic feedback from touching the target. Since the target was placed beyond arm’s reach, subjects were forced to lean the trunk forward to reach the target (Stand-reach condition, n = 15 trials).
In another 15 trials, participants took an intentional forward step in each trial (Step-reach condition) with their preferred leg. Subjects were instructed to always step with the same leg. Before each experiment, subjects practiced reaching in both conditions with eyes closed (7-10 trials/condition). Since postural asymmetry can influence APAs, 6 subjects were encouraged to bear weight on both legs equally prior to trials by monitoring the vertical force applied on each platform. Rest periods of 5 minutes were provided between conditions to avoid fatigue. The order of conditions was randomized.
Data Recording and Analysis
Fourteen infrared light-emitting markers were positioned on the fingertip (endpoint), ulnar head (wrist), lateral epicondyle (elbow), and midsternum (trunk) and bilaterally on acromions (shoulders), ASIS (hips), patellae (knees), lateral malleoli (ankles), and first metatarsals (toes). One marker was placed on the target. Marker movements were recorded using a 3D motion capture system (Optotrak, NDI, Ontario, Canada; sampling rate 100 Hz, trial duration 7 seconds).
Ground reaction forces were recorded with 2 force platforms (OR6-5, AMTI, MA, USA) at 100 Hz. Net COP displacement was calculated to determine APA characteristics. 23 Onset of kinetic and kinematic data acquisition was synchronized by a computerized trigger system.
Kinematic data were interpolated (third-order spline function) and kinematic and kinetic data were filtered with a fourth order low-pass 10 Hz Butterworth filter. When trunk movement is involved in forward reaching, trunk movement usually continues after the end of endpoint movement. 12 Endpoint and trunk movement onset and offset were determined when the tangential velocity of the endpoint and ipsilateral acromion marker, respectively, exceeded or fell below 10% of their peak values for >50 ms. In each trial, the timing of all kinematic events was determined relative to endpoint movement onset. Endpoint performance, APA, stepping performance, and postural stability measures were computed.
Reaching Performance Measures
Changes in endpoint positions during the Step-reach compared to the Stand-reach condition indicated the extent of spatial adaptation of the endpoint to whole-body displacement. The arm-trunk gain (g) was used as an index of spatial adaptability describing the influence of whole-body displacement associated with taking a step on endpoint position. Differences in final endpoint (d) and hip (h) marker positions between conditions were calculated for the sagittal direction representing the largest changes in displacement for this task:

where d and h are final endpoint and hip position deviations, respectively in the Step- compared to Stand-reach conditions. In particular, g = 1 if d = 0 (ie, hip displacement associated with taking a step was completely neutralized and endpoint position remained the same as the Stand-reach condition), and g = 0 if d = h (ie, hip displacement in Step-reach condition was fully transferred to the endpoint position). The proportion of time from endpoint peak velocity to movement offset in the total movement time was calculated as the deceleration phase (%), where 50% indicated the same duration in the acceleration (movement onset to peak velocity) and deceleration (peak velocity to movement offset) phases. Timing of trunk movement onset, peak velocity, and movement offset were calculated, where endpoint movement onset was time 0. Mean trunk velocity during stepping (from step onset to step offset) was also calculated.
Anticipatory Postural Adjustment Measures
Initial standing posture symmetry was evaluated as the proportion of the mean vertical force on each force platform in the 2 seconds period before the GO signal. APA measures were computed separately for anterior-posterior (APAAP) and medio-lateral (APAML) directions. 24 For both directions, the baseline COP margin was computed as the mean ± 3SD of the COP positions in the 2 seconds period before the GO signal (Figure 1, dotted horizontal lines). 25 APA onset was defined as the time at which the COP deviated from the baseline margin towards swing leg or backwards (Figure 1, dotted vertical lines). 26 APA amplitude was defined as the maximal COP excursion (Figure 1, solid horizontal lines) from the baseline margin during APAs, normalized by the length and width of the base of the support (BOS), respectively for APAAP and APAML. Abnormalities of APA profiles were also characterized as multiple COP shifts prior to step onset.
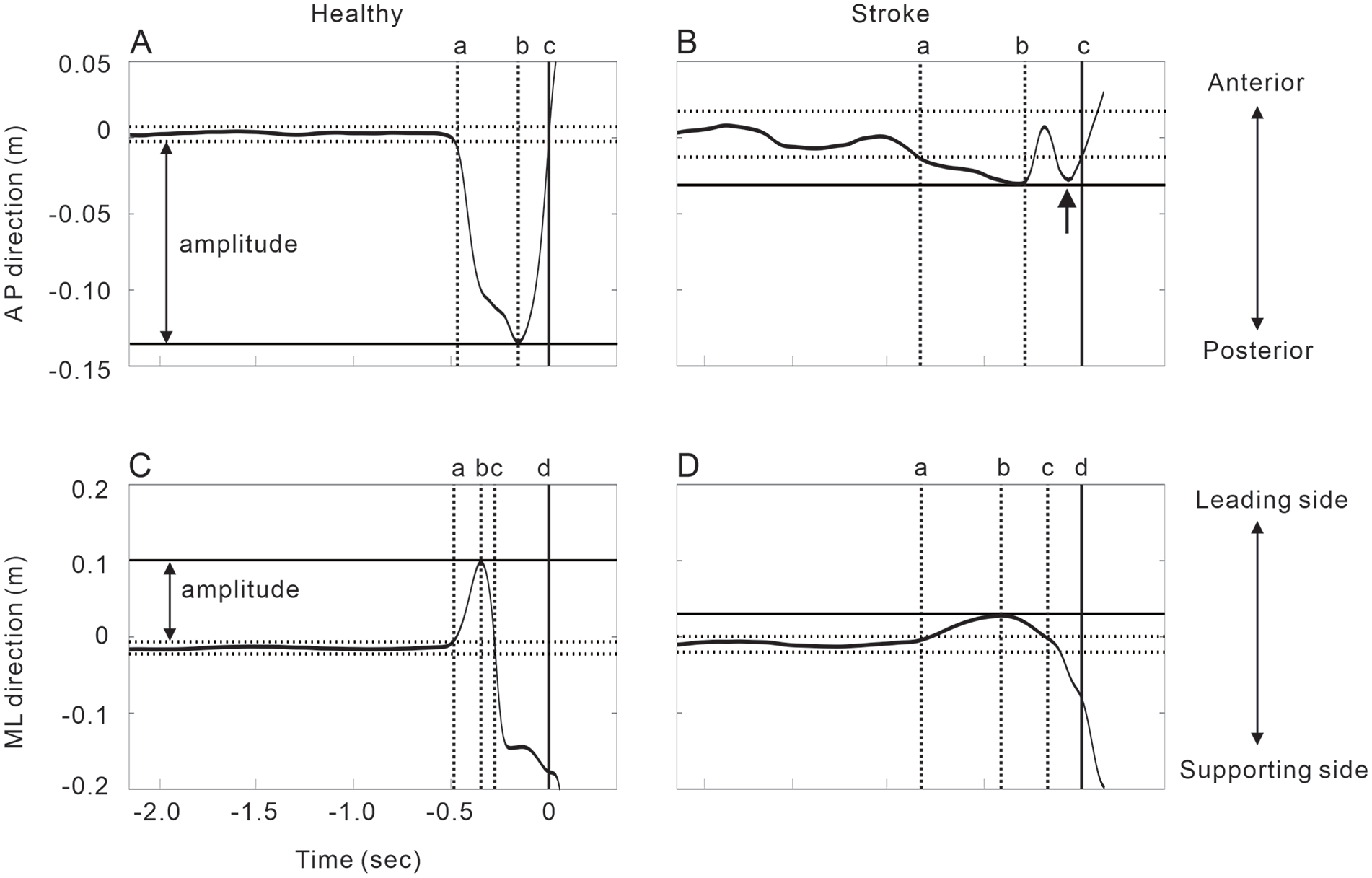
Examples of anticipatory postural adjustments during the Step-reach condition healthy and stroke subjects. The time 0 in the figure is adjusted to be the step onset time. (A) COP displacement in the anterior-posterior direction over time in a healthy subject. The COP first shifted backward (dotted vertical line: a), and then forward after reaching its peak (dotted vertical line: b). The COP position returned to the baseline margin (solid vertical line: c). (B) COP displacement in the anterior-posterior direction over time in an individual with stroke. After the backward shift of the COP reached its peak, there was a secondary backward shift of the COP (indicated with an arrow). Note that the amplitude of the COP shift is smaller and time required from APA onset (a) to step onset (c) is more prolonged compared to the healthy subject. (C) COP displacement in the medio-lateral direction over time in a healthy subject. The COP first shifted toward the leading leg (dotted vertical line: a), and then toward the supporting leg after reaching its peak (dotted vertical line: b). The COP position returned to the baseline margin (dotted vertical line: c) before the step onset (solid vertical line: d). (B) COP displacement in the medio-lateral direction over time in a stroke subject. There is no secondary peak of the COP displacement. Note that the amplitude of the COP shift is smaller and time required from APA onset (a) to step onset (d) is more prolonged compared to the healthy subject.
Stepping Performance Measures
Step onset, length, and duration were computed. Step onset relative to endpoint movement onset was defined as the time at which the stepping foot left the ground (ie, vertical force of the step side reached 1% baseline value). 27 Step length (m) and duration (seconds) were computed based on stepping foot toe marker displacement.
Postural Stability Measures
The margin-of-stability (MOS) was computed in both AP (MOSAP) and ML (MOSML) coordinates, considering the body as an inverted pendulum. 28 The center-of-mass (COM) position was estimated using segment inertial parameters. 5 The kinematic model included both sides of the thigh, shank, and foot, the trunk segment, and the pointing arm (hand, forearm, and upper arm). To compute MOS, the extrapolated COM position (xCOM) was estimated as the COM position projected on the ground, combined with its velocity, standardized by the pendulum length (distance between ankle marker and COM positions):

where vCOM is COM velocity, g is gravitational acceleration, and l is pendulum length:

where the BOS is the boundary position of the base-of-support. Positive and larger MOS indicate greater stability where the pendulum will not rotate over vertical, returning back to its current position, while negative and smaller MOS indicate greater instability where the pendulum rotates over the vertical, deviating from the current position. The MOS was calculated separately for AP and ML coordinates at both step onset and step offset. BOS position was estimated using the AP toe marker position for the MOSAP, while the ML ankle marker positions were used for the MOSML. Both MOSAP and MOSML were calculated for the stepping leg.
Statistical Analysis
Nonparametic tests were used for statistical analyses due to the small sample size. Mann–Whitney U tests estimated group differences in reaching performance, step performance, APAs, and postural stability measures. Spearman’s rank correlation coefficient (rs) estimated the relationships between reaching performance, step performance, APAs, and postural stability measures. Correlational analysis focused on 4 aims: The relationship between (1) Gain and APAs; (2) Gain and step performance; (3) APAs and clinical outcome; and (4) step performance and clinical outcome. The correlational analyses for the first 2 aims and last 2 aims were respectively performed in both subject groups and only in individuals with stroke. SPSS ver.21 (IBM, NY, USA) was used for statistical analyses, with significance levels of P < .05.
Results
Reaching Performance
Final hip positions at movement offset (ie, h in equation (1)) substantially differed between Stand-reach and Step-reach conditions in both individuals with (median difference: 349.32 mm; 95% confidence interval [CI]: 289.73, 398.06) and without stroke (median difference: 330.09 mm; 95% CI: 295.62, 392.97). Nevertheless, in controls, the final endpoint position difference (ie, d in equation (1)) was small (median difference: 91.41 mm; 95% CI: 39.48, 127.69), resulting in high gains (0.92 ± 0.04; Table 2). However, the final endpoint position in the Step-reach compared to the Stand-reach condition in individuals with stroke was substantially greater (median difference: 155.24 mm; 95% CI: 126.92, 182.04), despite similar hip displacement as controls, resulting in significantly lower gains (0.60 ± 0.04; Table 2).
Reaching Performance Measures in Individuals With and Without Stroke, Median (Interquartile Range).
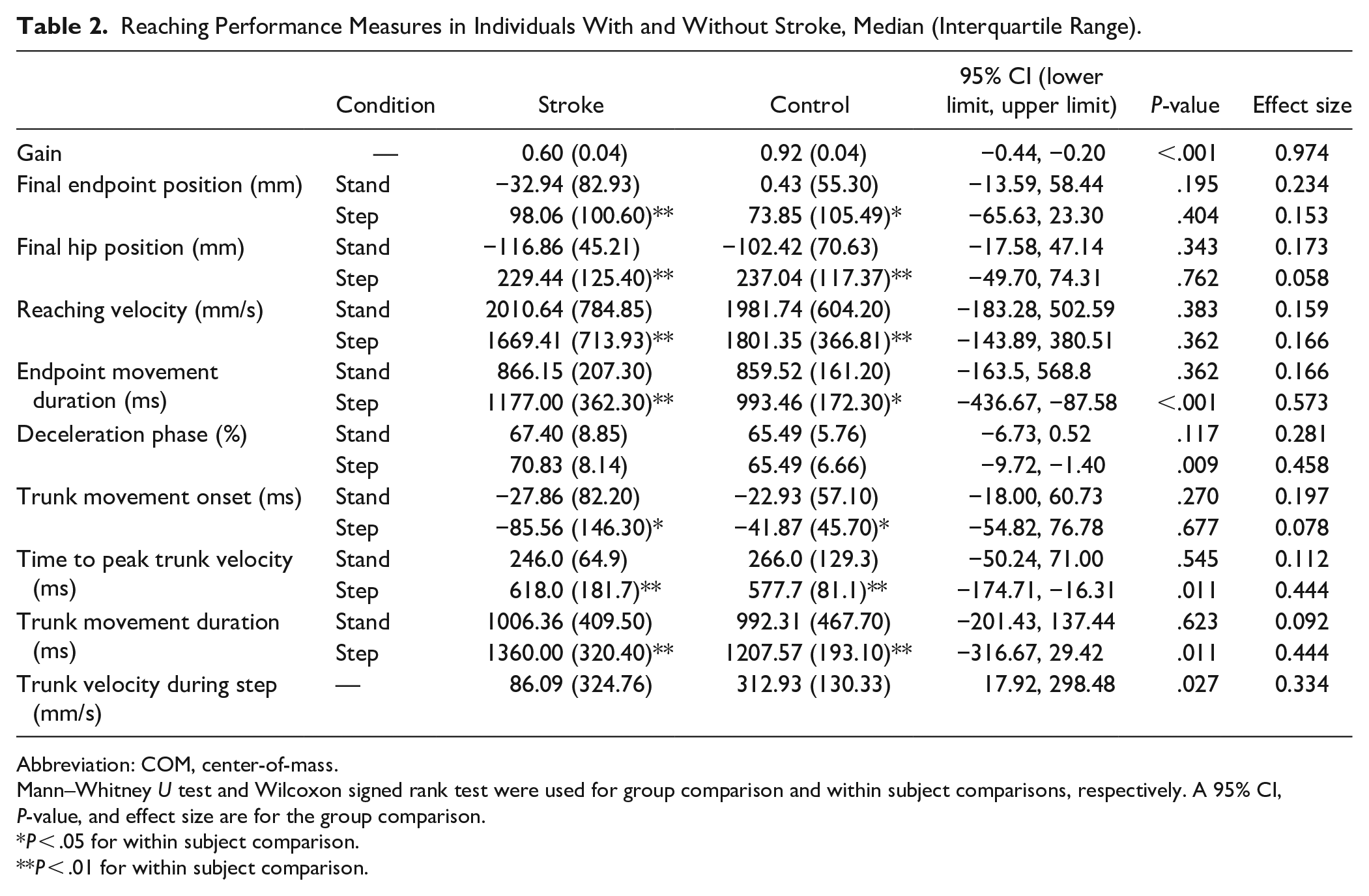
Abbreviation: COM, center-of-mass.
Mann–Whitney U test and Wilcoxon signed rank test were used for group comparison and within subject comparisons, respectively. A 95% CI, P-value, and effect size are for the group comparison.
P < .05 for within subject comparison.
P < .01 for within subject comparison.
Endpoint velocity in the Step-reach condition was significantly lower by 9.1% in controls and 17.0% in individuals with stroke than in the Stand-reach condition. Endpoint movement duration in the Step-reach condition was significantly longer by 15.6% in controls and by 35.9% in individuals with stroke than in the Stand-reach condition. Endpoint movement duration in the Step-reach condition was significantly prolonged by 18.5% in individuals with stroke, compared to controls (Table 2; Figure 2). In the Step-reach condition, trunk movement started significantly earlier than the endpoint movement and was more prolonged than in the Stand-reach condition. In the Step-reach condition, time to peak trunk velocity and trunk movement duration were more prolonged in individuals with stroke by 7.1% and 12.6%, compared to controls, respectively (Table 2; Figure 2).
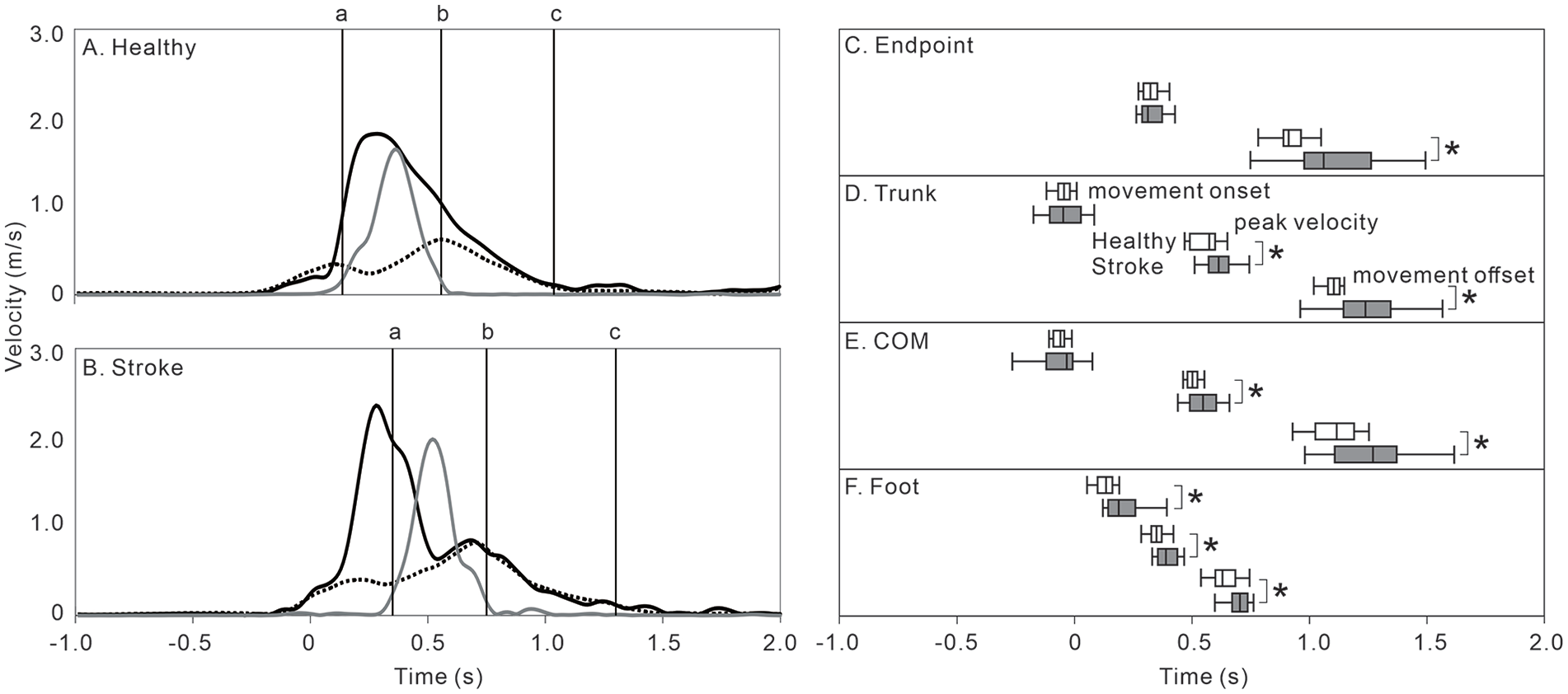
Velocity profile of the endpoint, trunk, and foot during the Step-reach condition in healthy and stroke subjects. (A) Velocity profile of the endpoint (solid black line), trunk (solid gray line), and foot (dotted black line) in a healthy subject plotted over time, where time zero in the figure is adjusted to be the endpoint movement onset. Foot movement onset (ie, step onset; vertical black line: a), foot movement offset (ie, step offset; vertical black line: b), and endpoint movement offset (vertical black line: c) are also shown. (B) Velocity profile of the endpoint (solid black line), trunk (solid gray line), and foot (dotted black line) in a stroke subject. Step onset (vertical black line: a) occurred long after the endpoint movement onset. (C-F) Movement onset (upper 2 boxes in each panel), peak velocity (middle 2 boxes in each panel), and movement offset (lower 2 boxes in each panel) timings in healthy (white box) and stroke (gray box) subjects. All timings are aligned such that time-zero is the time of endpoint movement onset.
Anticipatory Postural Adjustments
Subjects stood symmetrically before movement onset, shown by the similarity of vertical force proportion on each leg (≈0.50) in both groups (Table 3). The COP trajectory typical for gait initiation29,30 was present in both groups, while multiple APAAP were observed significantly more often by 286.8% in individuals with stroke, compared to in controls. APA amplitudes in individuals with stroke were significantly reduced for both APAAP by 32.3% and APAML by 17.4%, compared to controls (Table 3). Similarly, APA velocities in individuals with stroke were significantly reduced for both APAAP by 50.0% and APAML by 38.5%, compared to controls (Table 3). There were no differences in APA measures between those who stepped with the paretic (n = 9) or the non-paretic leg (n = 9) in individuals with stroke.
Stepping Performance in Individuals With and Without Stroke, Median (Interquartile Range).
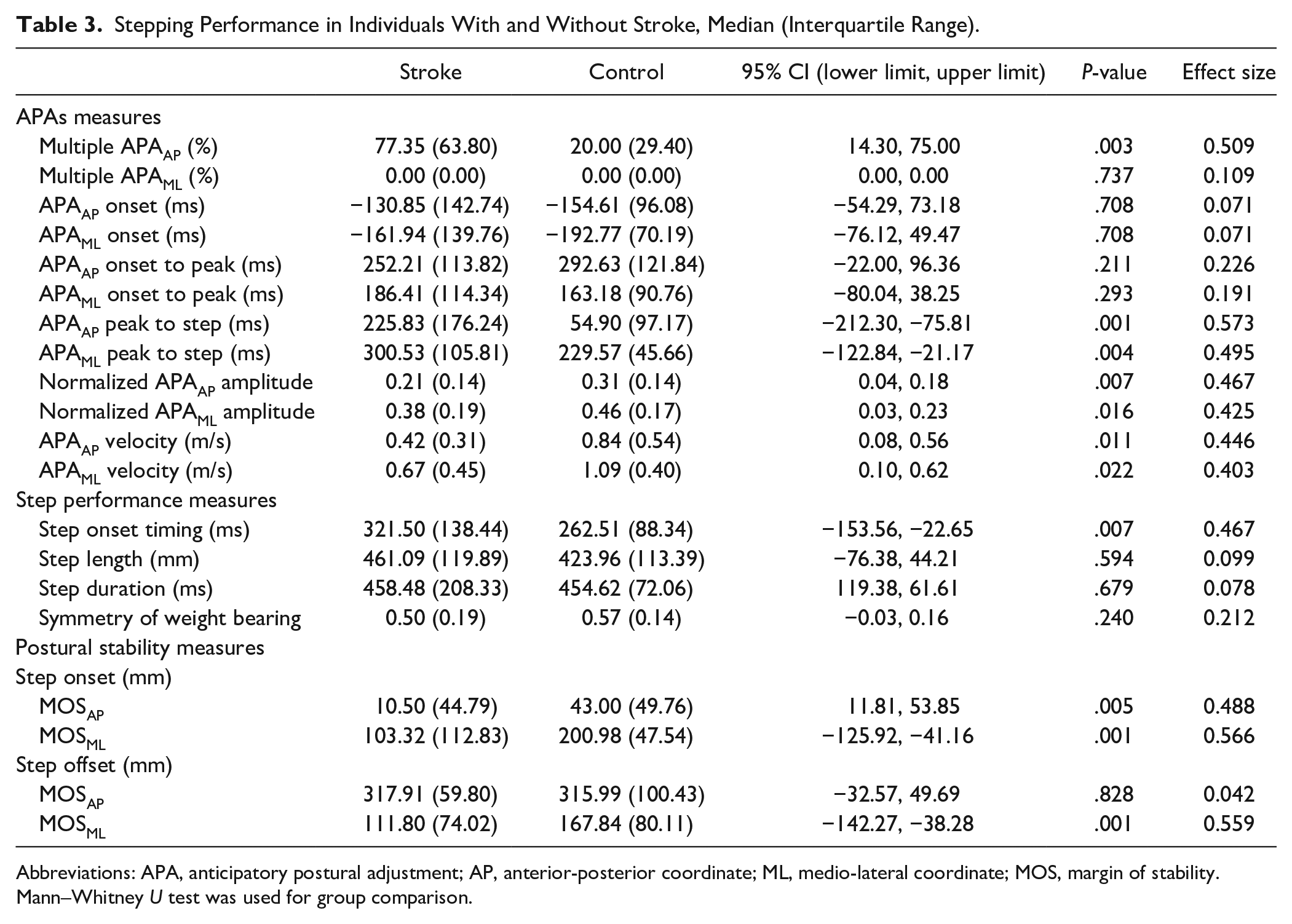
Abbreviations: APA, anticipatory postural adjustment; AP, anterior-posterior coordinate; ML, medio-lateral coordinate; MOS, margin of stability.
Mann–Whitney U test was used for group comparison.
Step Performance
Step onset timing was significantly delayed by 22.5% in individuals with stroke compared to controls (Table 3). Despite smaller APA amplitudes and velocities, step length, and step duration were similar between groups. There were no differences in step performance measures between those who stepped with the paretic or the non-paretic leg in individuals with stroke.
Postural Stability
Compared to controls, postural stability at step onset in individuals with stroke was significantly reduced for both AP and ML directions, as demonstrated by a reduced MOSAP by 75.6% and MOSML by 94.9%. However, postural stability at step offset in individuals with stroke was significantly reduced compared to controls only for the ML direction, as demonstrated by a 33.4% reduction in MOSML. There were no differences in postural stability measures between those who stepped with the paretic or the non-paretic leg.
Relationship Between Reaching Performance and Postural Measures
Normalized amplitude of APAs (APAAP: rs = .365, P < .05; APAML: rs = .435, P < .05) and APA velocity (APAAP: rs = .447, P < .05; APAML: rs = .415, P < .05) were moderately correlated with gain. Similarly, step onset timing was moderately correlated with gain (step onset: rs = −.483, P < .05).
Relationship of Reaching Performance and Postural Measures With Clinical Measures
In the stroke group, Gain was moderately correlated with UL motor impairment (FMA-UL score: rs = .470, P < .05) and balance score (B-BESTest: rs = .627, P < .05). Step onset timing was correlated with balance score (B-BESTest: rs = −.484, P < .05). Multiple APAs (rs = −.621, P < .05) and normalized APA amplitudes were correlated with LL motor impairment (FMA-LL score: rs = .671, P < .05).
Discussion
Evidence for impact of stroke on reaching performance has predominantly focused on arm motor function in seated subjects, neglecting the crucial role of APAs for reaching tasks during standing.1,2 This study fills this gap by investigating reaching performance and APAs during whole-body reaching while taking a forward step in individuals with and without stroke. There were significant differences in reaching performance, step performance, and postural stability between individuals with stroke and age-equivalent healthy individuals. Altered postural adjustments were related to reduced reaching performance highlighting the importance of the impact of stroke on postural mechanisms responsible for reduced reaching performance.
Aspects of coordination between arm reaching and voluntary stepping movements may be explained with the extension of the concept of arm-trunk synergies since the movement involves body segments with different amounts of inertia.
The Role of the Transport Synergy
The transport synergy refers to the contribution of arm movement to the forward reaching extent. When involved in arm reaching, trunk movement starts before endpoint movement. This anticipatory trunk movement allows smooth recruitment of body segments with different inertia. Similarly, when reaching movement is performed while taking a step, an anticipatory COP shift occurs to initiate whole-body displacement prior to endpoint movement onset (ie, APAs).
APA amplitudes and velocities in individuals with stroke were significantly reduced in both AP and ML directions compared to controls, consistent with previous studies reporting reduced APA amplitudes in subjects with stroke during seated reaching 31 and gait initiation.10,11 When taking a voluntary forward step, APAAP and APAML are important to evoke ground reaction forces that rapidly propel the body forward and onto the supporting leg, respectively.29,30 Smaller APA amplitudes without onset delay in individuals with stroke may be due to reduced force produced by ankle dorsiflexors for APAAP, and ankle plantarflexors, knee extensors, hip extensors and abductors for APAML.
Multiple APAs were observed for APAAP significantly more frequently in individuals with stroke, compared to controls. Multiple APAs can be considered as atypical APAs. 10 Multiple APAs were observed primarily in the AP direction, indicating that propulsive force was not generated smoothly in individuals with stroke. Therefore, the altered transport synergy during whole-body reaching in individuals with stroke can be characterized by reduced APA amplitude, velocity, and smoothness. The delayed step onset in stroke subjects due to the altered APAs would result in a delayed whole-body displacement, leading to poor synchronization of endpoint and whole-body movements during the transport synergy.
We focused exclusively on mechanical changes in APAs. However, EMG activity preceding step initiation are also affected by stroke. Successful step initiation necessitates a decrease in soleus and gastrocnemius muscle activity, coupled with an increase in tibialis anterior (TA) muscle activity to shift the COM forward. Furthermore, the engagement of hip abductors, such as the gluteus medius, is crucial for repositioning the COM onto the supporting leg. 32 Studies on individuals with stroke have revealed diminished amplitude and delayed onset in TA activity during step initiation. These alterations may be linked to challenges in reducing soleus muscle activity in the affected limb.11,33-35 Given the potential link between the observed changes in the arm transport synergy in our mechanical analysis and the previously documented EMG activity alterations, it is important to determine the relationships between modified APAs and diminished reaching performance after stroke using EMG-based APA measurements in future investigations.
Effects of Reduced Compensatory Synergy and Delayed Step Onset on Gain
The reduced gain in subjects with stroke can be attributed to the combination of 2 factors: (1) reduced ability to neutralize the effects of whole-body displacement associated with taking a step on the endpoint position; and (2) increased trunk displacement after the endpoint reaches the target due to delayed step onset. When healthy subjects take a reactive step induced by a postural perturbation during reaching, substantial changes of arm interjoint coordination occur to neutralize the effects of whole-body displacement associated with taking a step on endpoint position. 36 Individuals with stroke have reduced interjoint coordination during reaching from sitting 37 and standing. 19 In our study, the delayed step onset and prolonged trunk movement duration were significantly correlated with lower gains. The delayed step onset results in prolonged whole-body displacement even after the endpoint movement offset, increasing the demand of the compensatory synergy to neutralize the effect of whole-body displacement on the endpoint position. Therefore, the increased requirement for the compensatory synergy due to delayed step onset, in addition to the reduced ability to adjust interjoint coordination to maintain the endpoint position, may explain the reduced gain in individuals with stroke.
Although the small sample size did not allow subgroup analyses, the side of the brain lesion may have influenced motor planning and execution. Following stroke in right-handed individuals, there is a lesion-side-specific difference in the utilization of the paretic arm. Specifically, individuals with left hemisphere lesions are more engaged with their paretic arm compared to individuals with right hemispheric lesions.38–41 Endpoint error during reaching is greater in individuals with right hemispheric lesions who tend to use their paretic arms only when movement is predicted to be successful. 41 These characteristics may be related to the hemisphere-dependent control mechanisms of reaching. In right-hand dominant individuals, the left hemisphere may specialize in regulating movements through predictive mechanisms optimized for consistent and stable mechanical conditions. In contrast, the right hemisphere may provide position- and velocity-dependent reactions stabilizing posture and movement in case of sudden perturbations. 42 Respectively, for whole-body reaching, the arm transport synergy predominately provides responses to anticipated perturbations (ie, APAs), whereas the compensatory synergy contributes to stability of posture and endpoint trajectory during unexpected perturbations. Therefore, left and right hemispheric lesions may respectively reduce transport and compensatory synergies. Further studies with larger sample sizes and APA measurement using EMG are necessary to elucidate the hemisphere-specific impact of stroke on whole-body reaching.
Postural Stability During Whole-Body Reaching When Taking a Step
For whole-body reaching, the system needs to transfer stability from 1 standing position to another. MOS at step onset was significantly reduced in both AP and ML directions in individuals with stroke, suggesting that they had reduced postural stability in both directions when initiating a voluntary step. MOS at step offset was only reduced in the ML direction in individuals with stroke, suggesting that they were able to regain postural stability in the AP direction. These results are consistent with previous studies demonstrating that individuals with stroke have difficulty in maintaining postural stability particularly in the ML direction during gait.43,44
Interpreting the Results in the Context of Referent Control of Motor Actions
In healthy subjects, final endpoint position and endpoint trajectory were maintained despite the involvement of additional DFs while taking a step during reaching. Similar results were found when healthy subjects make an unintentional (sudden) step during reaching tasks. 36 This suggests that the intact central nervous system (CNS) has a greater capacity of preserving motor equivalence and equifinality than previously thought. The control of motor equivalent actions can be explained by the RCT, an extension of the equilibrium-point hypothesis. 45 RCT proposes that the CNS can specify a referent body configuration (R) that represents a common, threshold body posture at which muscles begin to be activated or deactivated. In this context, reaching while stepping is initiated by a referent shift of the endpoint and foot positions. By shifting R, the CNS transfers balance and stability (body equilibrium) in the environment. The actual body motion, Q, deviates from R due to gravity and external forces. Movement results from the tendency to minimize the difference between referent (R) and actual (Q) endpoint and foot positions (see Asatryan 45 for details).
In our study, the timing of the peak trunk velocity and trunk movement offset were delayed in individuals with stroke (Figure 2C-F). During arm reaching, the shift in the referent endpoint position ends at around peak endpoint velocity, 46 implying the feedforward nature of referent control. A similar control strategy may underlie referent shifts in the referent body configuration, R, during a single step. Shift in R during a single step ends around the time to trunk peak velocity. Delayed timing of peak trunk velocity and reduced trunk velocity during stepping observed in our study may indicate a reduced rate of R shift in individuals with stroke. Reduced APA amplitude and velocity may also indicate that the shift in R was delayed in individuals with stroke.
Clinical Implications
It is important to understand both UL sensorimotor performance and balance function during functional reaching from standing in individuals with stroke, a task that can be used to assess higher-order motor control. Our study revealed a decrease in amplitude, velocity, and smoothness of APAs among individuals with stroke. Altered APAs after stroke lead to a delayed stepping onset and may be due to a deficit of the damaged CNS to appropriately shift R. This deficit may also underlie the decrease in paretic leg muscle activation, and in particular, the activation of TA, 33 further compounding the problem. Fear of falling has also been related to prolonged APAs during gait initiation in older adults. 47 Therefore, training programs that target ankle EMG patterns, muscle weakness, balance function in both AP and ML directions, and fear of falling may prove beneficial in optimizing APAs during whole-body reaching while taking a step.
Limitations
APA assessment during whole-body reaching relied on kinetic measurements obtained from force-platforms. To gain a more comprehensive understanding of altered APAs in individuals with stroke, additional investigations employing EMG are necessary. The restricted sample size precluded subgroup analyses to explore potential influences of lesion location on APAs and reaching performance. Considering that prior research indicated distinct roles of brain hemispheres in adjustments of reaching movements, further studies with larger sample sizes including EMG-based APA measurements may be indicated to investigate the hemisphere-specific influence of stroke on whole-body reaching. Results generalizability is limited since our study only included individuals with chronic stroke exhibiting relatively good balance function. Further studies in individuals with acute stroke and those with poor balance function are necessary to investigate if findings apply to different patient populations.
Conclusions
This study examined reaching performance and postural adjustments involved in whole-body reaching while taking a forward step in individuals with stroke. Individuals with stroke had altered APAs during the task, characterized by reduced amplitude, velocity, and smoothness of anticipatory center of pressure shift. Altered APAs were associated with decreased reaching performance. A deficit in the ability of the damaged CNS to specify the referent body configuration provides a potential explanation based on motor control theory. The study provides insights into the potential mechanisms underlying the reduced performance of whole-body reaching after stroke. Therapeutic interventions should address both arm and postural movements in order to improve whole-body reaching performance in individuals with stroke.
Footnotes
Acknowledgements
We thank all participants who volunteered for the study.
Author Contributions
Yosuke Tomita: Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Software; Validation; Visualization; Writing—original draft; Writing—review & editing. Aditi A. Mullick: Methodology; Project administration; Writing—original draft; Writing—review & editing. Anatol G. Feldman: Conceptualization; Formal analysis; Funding acquisition; Methodology; Project administration; Resources; Supervision; Writing—original draft; Writing—review & editing. Mindy F. Levin: Conceptualization; Formal analysis; Funding acquisition; Methodology; Project administration; Resources; Supervision; Writing—original draft; Writing—review & editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Y.T. is supported by Kakenhi (Grant-in-Aid for Early-Career Scientists No. 22K17637). Research was supported by a grant from National Science and Engineering Research Canada (NSERC) to A.G.F. No. RGPIN/0498-2019; M.F.L. was supported by a Tier 1 Canada Research Chair in Motor Recovery and Rehabilitation.
Research Data Availability
Data will be made available on request.