
Abstract
Objective:
We aimed to identify key aspects of the learning dynamics of proprioception training including: 1) specificity to the training type, 2) acquisition of proprioceptive skills, 3) retention of learning effects, and 4) transfer to different proprioceptive skills.
Methods:
We performed a systematic literature search using the database (MEDLINE, EMBASE, Cochrane Library, and PEDro). The inclusion criteria required adult participants who underwent any training program that could enhance proprioceptive function, and at least 1 quantitative assessment of proprioception before and after the intervention. We analyzed within-group changes to quantify the effectiveness of an intervention.
Results:
In total, 106 studies with 343 participant-outcome groups were included. Proprioception-specific training resulted in large effect sizes with a mean improvement of 23.4 to 42.6%, nonspecific training resulted in medium effect sizes with 12.3 to 22% improvement, and no training resulted in small effect sizes with 5.0 to 8.9% improvement. Single-session training exhibited significant proprioceptive improvement immediately (10 studies). For training interventions with a midway evaluation (4 studies), trained groups improved by approximately 70% of their final value at the midway point. Proprioceptive improvements were largely maintained at a delayed follow-up of at least 1 week (12 studies). Finally, improvements in 1 assessment were significantly correlated with improvements in another assessment (10 studies).
Conclusions:
Proprioceptive learning appears to exhibit several features similar to motor learning, including specificity to the training type, 2 time constant learning curves, good retention, and improvements that are correlated between different assessments, suggesting a possible, common mechanism for the transfer of training.
Introduction
Proprioception is the part of somatosensation that enables perception of body position and motion based on information derived from internal sensing structures.1,2 Proprioception has a substantial role in motor control, and loss of proprioception can result in sensory ataxia, impaired balance, and incoordination that are exacerbated in the absence of visual compensation.1,3 Beyond motor control, the somatosensory system plays a role in motor learning and functional recovery. 4 In post-stroke individuals, proprioceptive deficits predicted the possibility to benefit from constraint-induced therapy, 5 and finger proprioception and somatosensory system integrity predicted treatment-related hand function gains from robot-based therapy.6,7
Several systematic reviews have found that various forms of proprioceptive training improve proprioception in healthy subjects and patients with various medical conditions.8-11 However, these reviews have not analyzed the learning dynamics associated with proprioceptive training. Therefore, we are interested in 4 key aspects of learning that are well-known in motor learning literature: specificity, acquisition, retention, and transfer. It is currently unclear if this suite of motor learning features applies to proprioceptive learning.12,13
Specificity of motor learning refers to the observation that motor training effects depend on the training type. 14 The methods of proprioceptive training vary widely between clinical studies, and many studies have investigated the training effect on proprioception without explicitly using the term “proprioceptive training.” Consequently, previous systematic reviews defined proprioceptive training as an intervention or training program believed to influence proprioception.8,9 or an experimental program specifically oriented to enhance proprioception and balance. 10 However, many types of sensorimotor training programs, even if not specifically designed to challenge proprioception, might affect proprioceptive acuity.15,16 Therefore, we included a wide range of training programs and sought to examine the specificity of the training technique on measured changes in proprioception acuity.
A second well-known observation about motor learning is that the acquisition of a motor skill is well described by an exponential learning curve, often described by 2 time constants associated with fast and slow learning. 13 Many experiments confirmed that motor skill acquisition shows initial rapid improvement over a single session and later slower gains over multiple training sessions until reaching an asymptotic level,13,17 a process that has often been observed in motor rehabilitation. 18 Based on this perspective, we sought to investigate the temporal learning pattern in the acquisition of proprioceptive skills.
A third well-known feature of motor learning is retention, in which a motor skill gained during a training period is retained following the cessation of training for a period of time. It is currently unclear to what extent change in proprioception acuity is retained following training.
Finally, transfer refers to the application of a learned skill in a novel context. 14 Because of the complex neurophysiological processes related to proprioception, there is no single gold standard assessment technique to quantitatively measure proprioceptive acuity. Among the different assessment techniques, joint position reproduction (JPR) and threshold to detection of passive motion (TTDPM) have been widely used by clinicians and researchers.2,19 Estimation or discrimination of joint angle, such as active movement extent discrimination assessment and just-noticeable difference threshold, have also been used in some studies.20-23 Each assessment technique arguably assesses different aspects of proprioception involving different neurophysiological processes.2,19 Therefore, it is interesting to consider the extent to which training-related improvements manifest in different proprioceptive assessments.
In summary, through this systematic review, we aimed to answer the following questions related to the learning dynamics of proprioception training: (1) how do different types of training affect proprioceptive learning (specificity), (2) what is the temporal pattern of learning in proprioception (acquisition), (3) do proprioceptive training effects last after the intervention is completed (retention), and (4) does improvement in 1 proprioceptive task correlate with changes in other proprioceptive tasks (transfer)?
Methods
This systematic review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement 24 and registered on the PROSPERO International prospective register of systematic reviews (CRD42022327193).
Literature Search Strategy
A systematic literature search was performed using the database of MEDLINE (PubMed), EMBASE, Cochrane Library, and PEDro. Search terms include proprioception or kinesthesia (outcome) and training (intervention), and other relevant keywords related to them. The complete list of the search syntax used in each database is presented in Supplemental 1. The language was restricted to English, and only studies that recruited adults were included. The search period was from the database inception date to 2nd December 2021.
Eligibility Criteria
All prospective clinical studies on human subjects were assessed for eligibility. Inclusion criteria were as follows: (1) participants were adult subjects with or without specific medical conditions, (2) intervention was any kind of training program that may influence or enhance proprioceptive function, (3) at least 1 of the outcome measures was a quantitative assessment of proprioception not confounded by other sensory information, and (4) pre- and post-intervention results of the outcome measure were reported in the study. Since most of the quantitative outcome measures were the absolute errors of joint angle (°), a few studies presenting other forms of outcome measures were excluded for consistency. In addition, studies that included participants who underwent surgery during the study period were excluded because the change in outcomes might be affected by the surgical procedure.
Selection Process and Data Extraction
Initial search results were imported into Endnote X9 (Clarivate Analytics, Philadelphia, PA, USA), and duplicates were removed. Two authors (HGS and SJY) independently screened and assessed the eligibility of studies. The screening was performed based on the titles and abstracts, and then the full texts were retrieved and assessed for eligibility. In addition, the reference list of relevant articles was searched to identify additional eligible studies by the same authors. If 2 authors disagreed at any stage, a third author was consulted to make the final decision.
The following data was extracted from final study documents: publication year, author’s name, study design, population, intervention, comparator, duration of intervention, number of sessions, time frame of assessment, number of participants, method of outcome assessment, involved joint, and pre- and post-intervention results. The physiotherapy evidence database (PEDro) scale was used to assess the methodological quality of the studies with a comparable control group.25,26 The official score of the PEDro scale was adopted if it was provided on the PEDro site (https://pedro.org.au/). Otherwise, 2 authors (AF and CJ) independently evaluated the PEDro scale of each study and reached a consensus.
Data Synthesis
To incorporate the results of all included controlled and uncontrolled studies, within-group changes were analyzed primarily as the measure of the effectiveness of an intervention. The within-group change was calculated in 2 ways for each study group, proprioception outcome measure, and assessment time frame. First, the percentage of change between pre- and post-intervention was calculated by dividing the difference between the 2 results by the pre-intervention result. The results were averaged if the study had more than 1 result in the same proprioception assessment technique. Next, the mean % changes across the individual study groups were calculated according to the intervention types, time frames, disease entities, and involved joints. Second, the within-group standardized mean difference (SMD) was calculated using the following equation according to the previous recommendation 27 :
where the numerator is the difference between pre- and post-intervention means, and the denominator is the average standard deviation of both measures.
Because the sample size was small (≤20) in many study groups, SMDs were corrected for small-sample bias using the following formula27,28:
Since the standard errors of SMDs were necessary for pooling effect size, those were calculated using the following formula 29 :
where r is the correlation coefficient between pre- and post-intervention measures. If the study presented necessary data, r was calculated using the following equation 30 :
However, most studies did not report the standard deviation of the difference between pre- and post-intervention measures. According to the previous recommendation,31-33 a pre-post correlation of 0.5 was used for those studies. Pooled SMDs and 95% confidence intervals (CIs) across the study groups were analyzed using the random effects model with the restricted maximum likelihood estimator and Knapp-Hartung Adjustments for the between-study heterogeneity.
In addition, Pearson correlation analysis was used to investigate the extent to which an improvement in 1 proprioception assessment was correlated with any improvement in a different proprioception assessment. R software (version 4.1.2) with the {meta} package was used for all statistical analyses.
Classification of Training
Training type was classified broadly into proprioception-targeted training, non-targeted training, or no training. The classification took into account both the researchers’ intention in each study and the known aims specific to each training. The proprioception-targeted training was defined as a training program believed to specifically challenge or influence proprioception and related functions, such as balance, coordination, and sensorimotor performance. Non-targeted training was defined as a training program not specifically designed to challenge or influence proprioception; most of these were described as “routine,” “conventional,” or clearly had a primary purpose other than proprioception, such as strength, endurance, or flexibility training, while a subset was designed as control interventions in clinical studies. The “no training” category was defined as no intervention (as typically applied to the control groups) or intervention without training components, such as education, usual care, and daily activities.
Targeted and non-targeted training categories were further divided into subcategories according to their detailed types as described by the authors. The subcategories for the targeted training were “proprioceptive training” (when that term was used by the authors), balance/coordination training, proprioceptive neuromuscular facilitation (PNF)/manual therapy, popular low-impact activities (eg, Tai Chi, Yoga, and Pilates), training using vibrating devices, robot-assisted training, and other targeted training. The subcategories for the non-targeted training were routine or conventional training/rehabilitation, strengthening/resistance training, range of motion/flexibility training, and other non-targeted training. If a training program was difficult to classify into a subcategory or the number of study groups employing the training type was too small to be analyzed separately, it was classified as “other” training.
All authors discussed and agreed upon the classification definitions and subcategories of training. Two authors (HGS and SJY) independently performed the classification of training type in each study and reached a consensus. Information on the type of training used in each study is presented in Supplemental 2.
Results
An initial search identified a total of 5699 studies from 4 databases. After duplication removal and screening, 161 retrieved studies were assessed for eligibility. Twenty studies were also obtained from citation searching using previous reviews and retrieved studies. Among them, 15 retrieved studies were assessed for eligibility. Ultimately, 106 studies were included in this review. Figure 1 shows a PRISMA 2020 flow diagram that details the selection process.
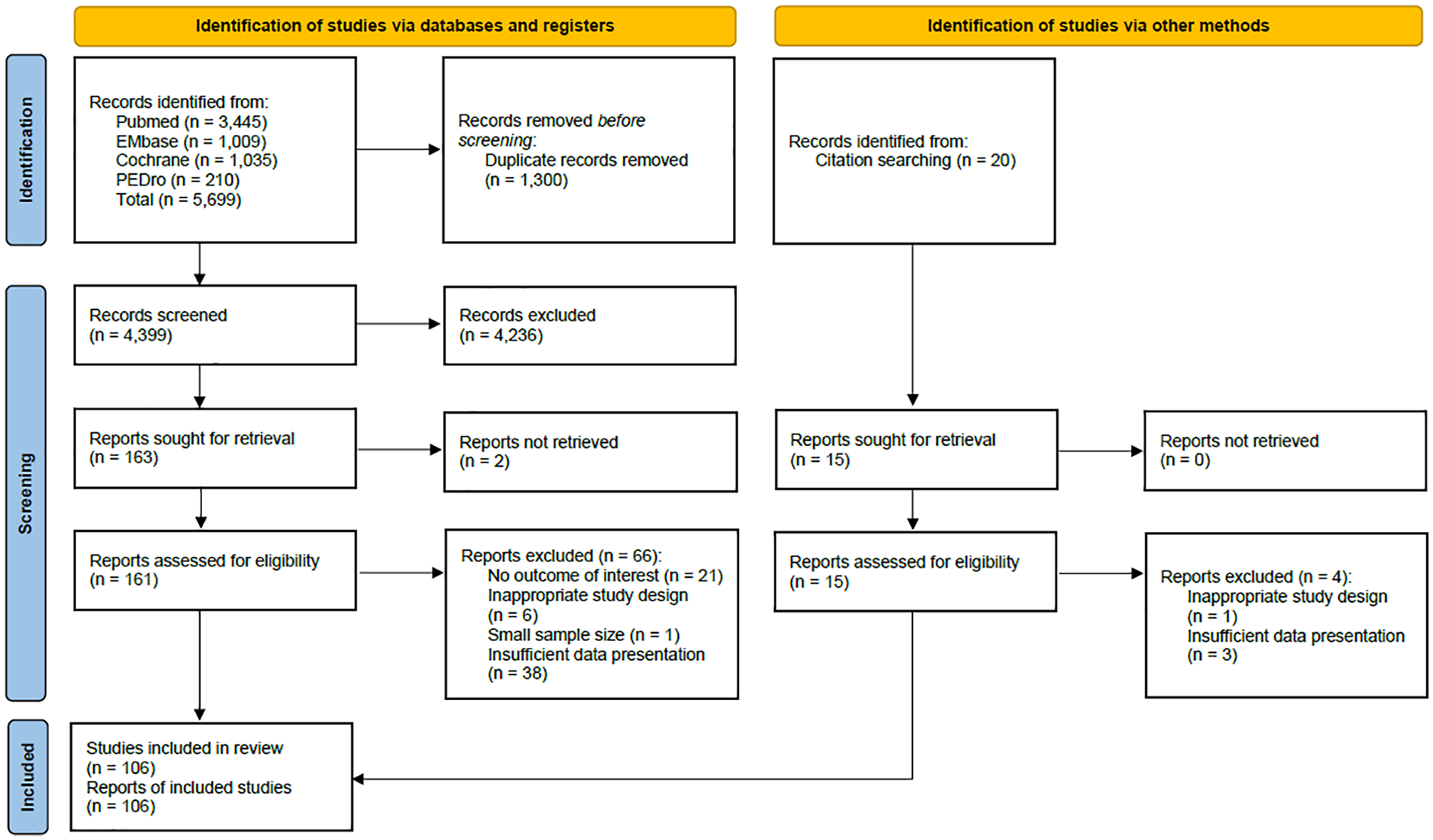
PRISMA 2020 flow diagram.
Characteristics of Included Studies
Among 106 included studies, 80 were randomized controlled trials (RCTs), 18 were pre-post studies, 3 were non-RCTs, and 5 were crossover studies. Based on the intervention type, the proprioception outcome measures, and the assessment time frame in each study, we identified 343 participant-outcome groups from the studies (ie, each group had a specific intervention, outcome, and assessment time frame). The number of participants in each group ranged from 6 to 75 subjects with an average of 16.9 ± 8.4. The most frequent medical condition was musculoskeletal disorders, and most evaluations were conducted at the end of the intervention. Active JPR was the most frequently used proprioception outcome measure and the knee joint was the most frequently evaluated joint. The PEDro scale was used to assess 88 studies that had scores ranging from 3 to 9 with a median of 6.
The summary of 106 included studies and 343 participant-outcome groups is presented in Supplemental 2 and corresponding references are provided in Supplemental 3.
Specificity of the Training Effect to Training Type
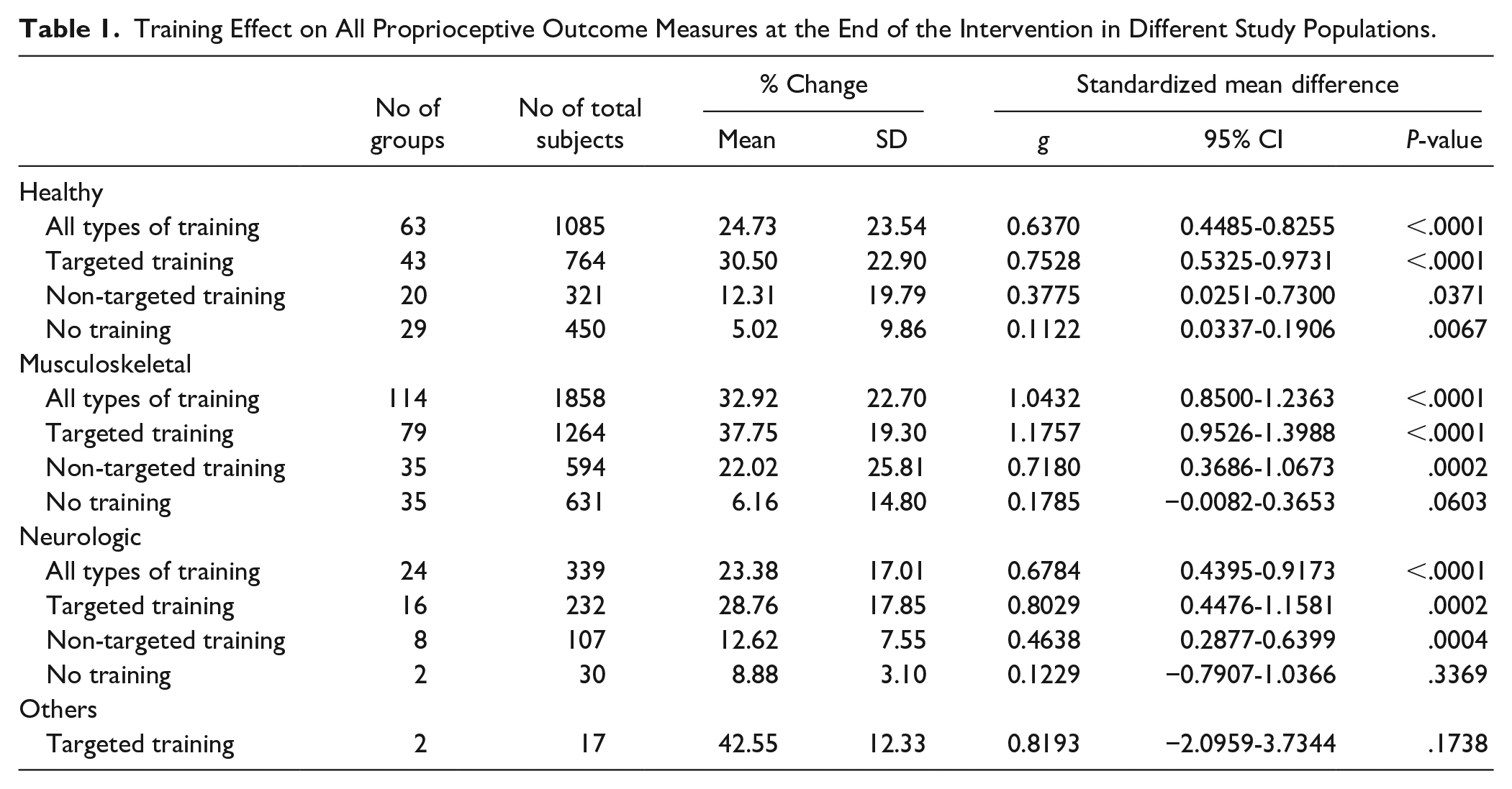
Proprioception-targeted training resulted in strong effect sizes for proprioceptive assessments that were significant for various populations (Table 1), and comparable between outcome measures (Table 2). Non-targeted training resulted in moderate effect sizes, while no training produced only small or nonsignificant effect sizes. Across outcome measures and participant types, proprioception-targeted training resulted in a mean improvement from 28.8 to 42.6%, non-targeted training from 12.3 to 22.0%, and no training from 5.0 to 8.8%. The effect size of targeted training was largest in patients with musculoskeletal diseases (g: 1.2). Proprioception-targeted training was employed in 68.3, 69.3, and 66.7% of the training groups in the healthy population, those with musculoskeletal diseases, and those with neurologic diseases, respectively; that is, there was little difference in training types across the disease population. When considering different proprioceptive outcomes (Table 2), the difference in effect size between targeted and non-targeted training was largest for the active JPR outcome measure (g: 1.03 vs 0.49).
Training Effect on All Proprioceptive Outcome Measures at the End of the Intervention in Different Study Populations.
Training Effect on Each Proprioceptive Outcome Measure at the End of the Intervention.
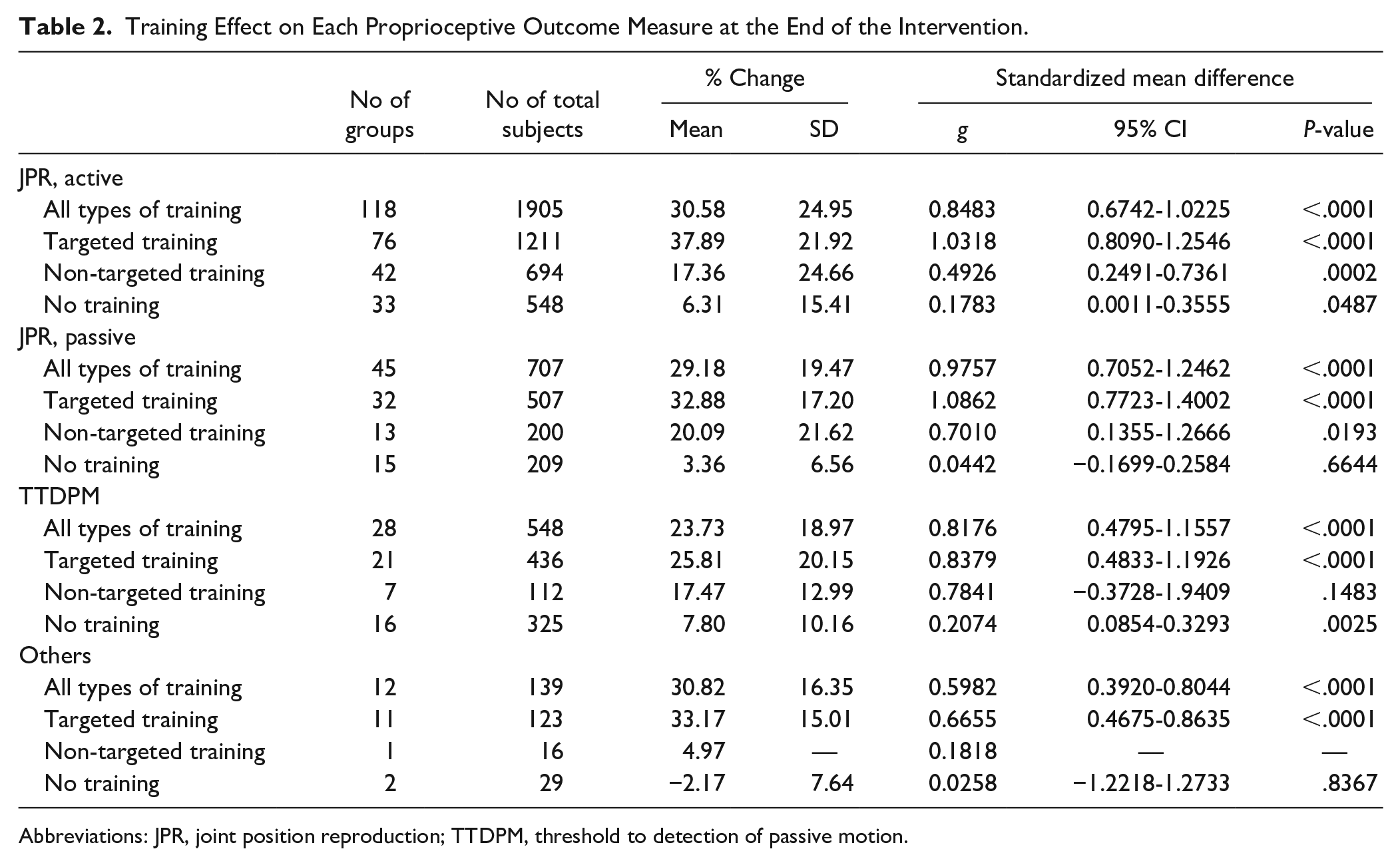
Abbreviations: JPR, joint position reproduction; TTDPM, threshold to detection of passive motion.
In terms of training types (Table 3), proprioceptive training, balance/coordination training, PNF/manual therapy, popular low-impact activities, and other specific/nonspecific training demonstrated a mean change of more than 30% with g of 0.8. Strengthening/resistance training showed a relatively large effect size (g: 0.86) compared to other non-targeted training subcategories, such as conventional training/rehabilitation and ROM/flexibility training.
Training Effect on All Proprioceptive Outcome Measures at the End of Intervention According to the Subcategories of Training.
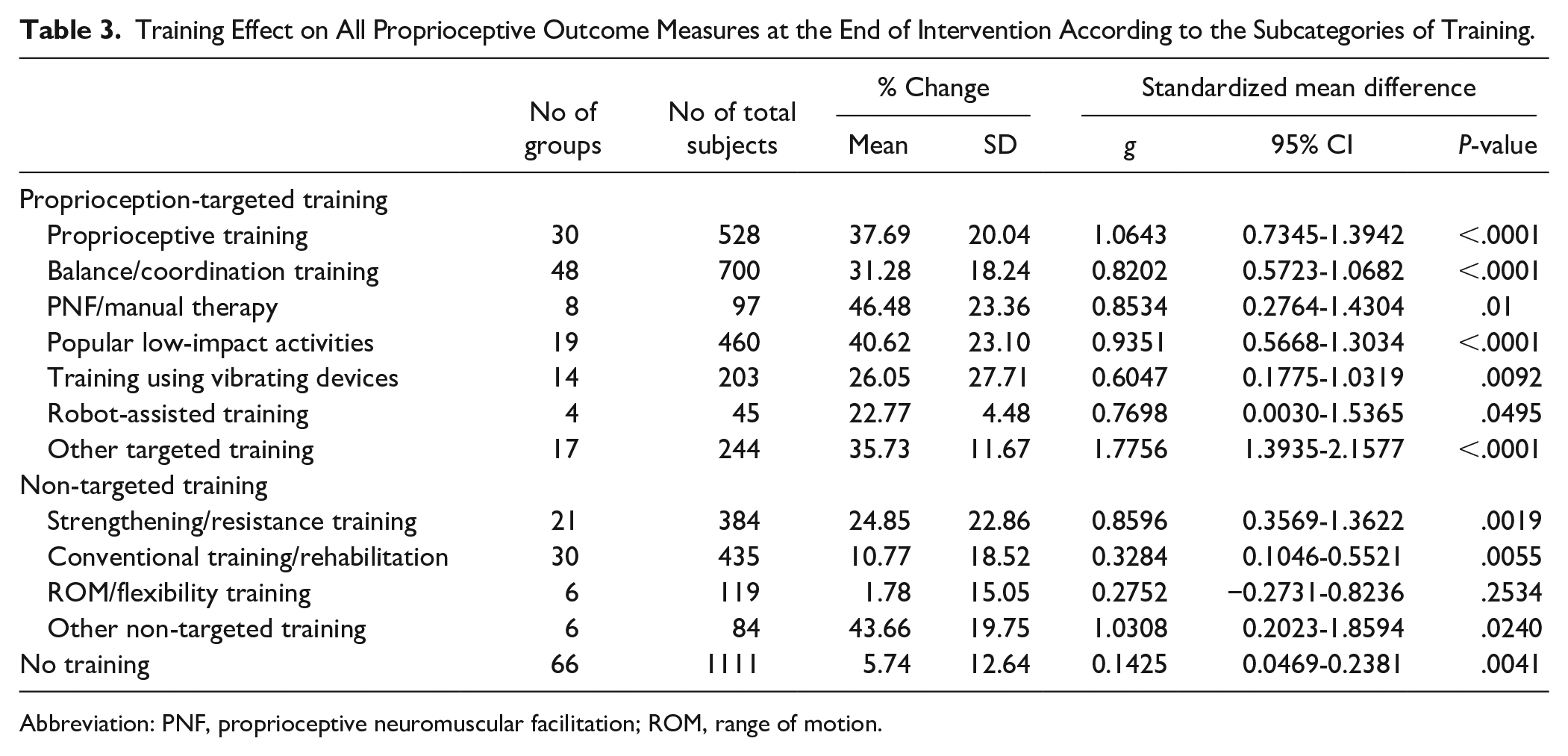
Abbreviation: PNF, proprioceptive neuromuscular facilitation; ROM, range of motion.
Effect sizes of proprioception-targeted training were comparable between body parts (Table 4). On the other hand, the effect size of non-targeted training was small or nonsignificant in the upper limb (g: 0.26) and neck/trunk (−0.17), but medium for the knee (0.79) and ankle (0.60).
Training Effect on All Proprioceptive Outcome Measures at the End of the Intervention in Different Body Parts.
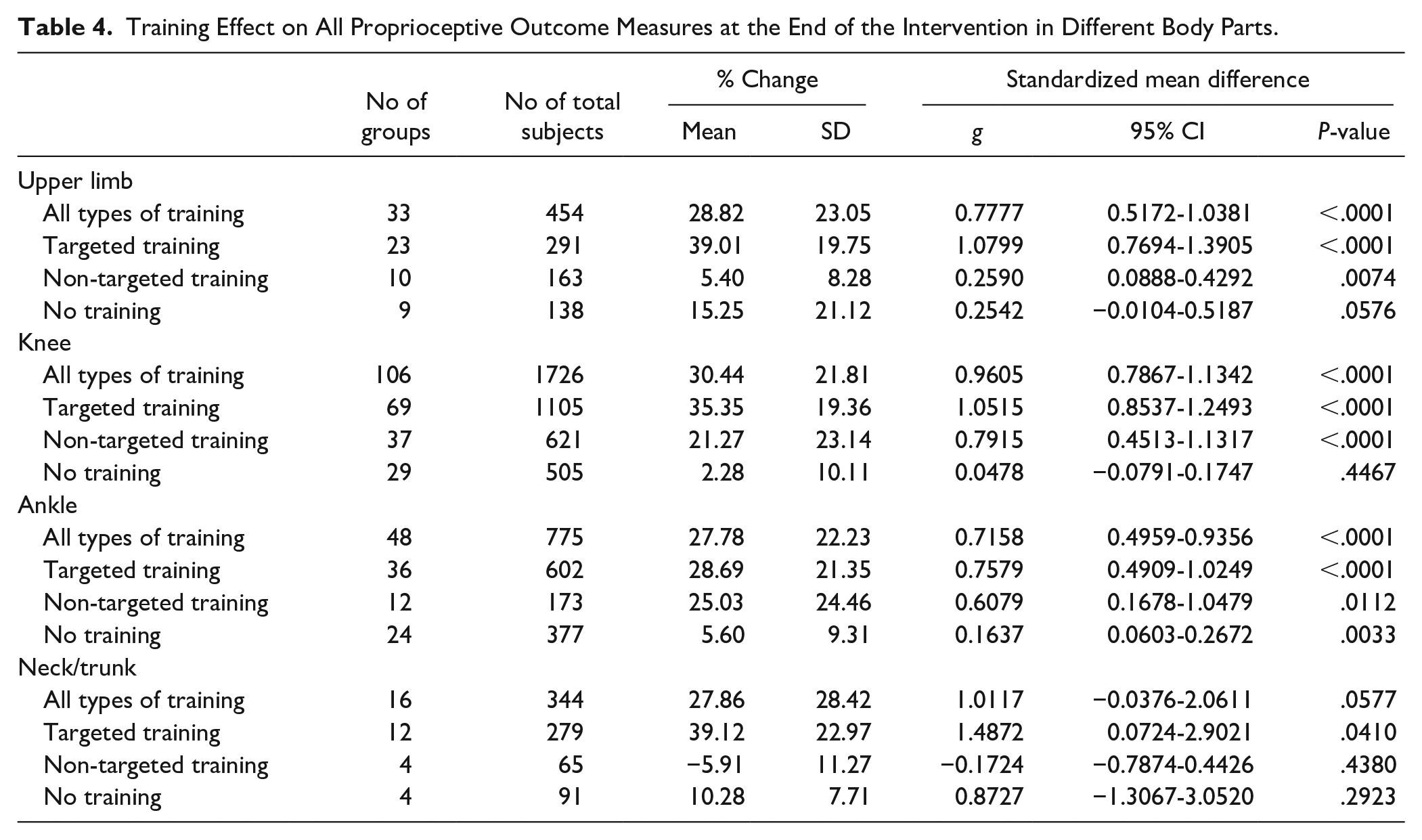
In summary, proprioceptive-targeted training produced the largest effect sizes in proprioceptive outcomes. The “no training” condition did not typically produce significant improvements, but non-targeted training often produced significant effects but with smaller effect sizes.
Time Course of Acquisition of the Training Effect
Ten studies, including 23 participant-outcome groups, evaluated the immediate effect of training after only 1 intervention session. Proprioception-targeted training produced a significant immediate effect: the mean % change was 29.0 ± 17.8, and g was 0.81 (95% CI 0.45-1.16, 15 groups, 308 subjects).
Four studies, including 9 participant-outcome groups (133 subjects), included an evaluation midway through a multi-session training protocol (Figure 2). The % changes were 29.9 ± 24.1 in the mid of the intervention and 43.9 ± 32.0 at the end of the intervention. That is, these groups exhibited on average approximately 70% of their final change at the midway point through the intervention. Effect sizes of incremental change were large across the first half (g: 1.02, 95% CI 0.27-1.77) and small in the second half (0.35, 95% CI 0.11-0.59).
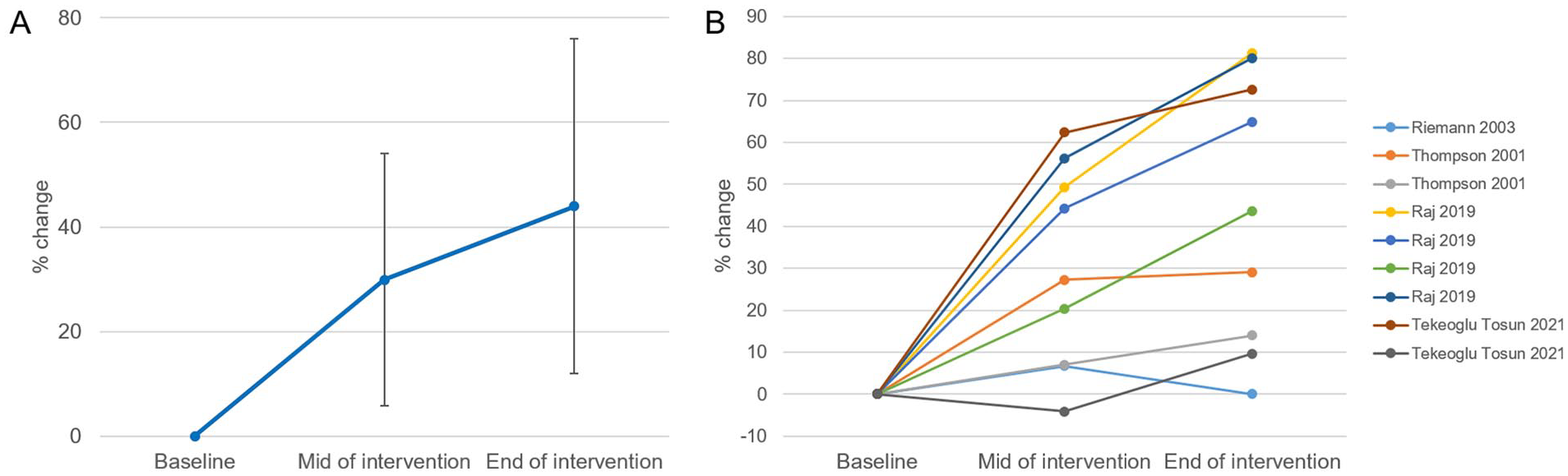
Time course of training effect on proprioceptive outcome measures. (9 participant-outcome groups, 133 subjects). Means and SDs (A), and the results of each group (B) are presented.
Retention of Training Effect
Twelve studies, including 37 participant-outcome groups, evaluated the training effect at least 1 week after the end of the intervention (Figure 3). All types of training (34 groups, 621 subjects) demonstrated a mean % change of 31.2 ± 32.7 and g of 0.88 (95% CI 0.44-1.30) at follow-up. Proprioception-targeted (17 groups, 310 subjects) and non-targeted (17 groups, 311 subjects) training showed mean % change of 23.7 ± 16.7 and 38.7 ± 41.8, and g of 0.82 (95% CI 0.22-1.41) and 0.96 (95% CI 0.26-1.67) at follow-up, respectively. After no training (3 groups, 73 subjects), the mean % change was −8.4 ± 27.6, and g was 0.41 (95% CI −2.3-3.1) at follow-up. The retention of training effect in each study group is presented in Supplemental 4.
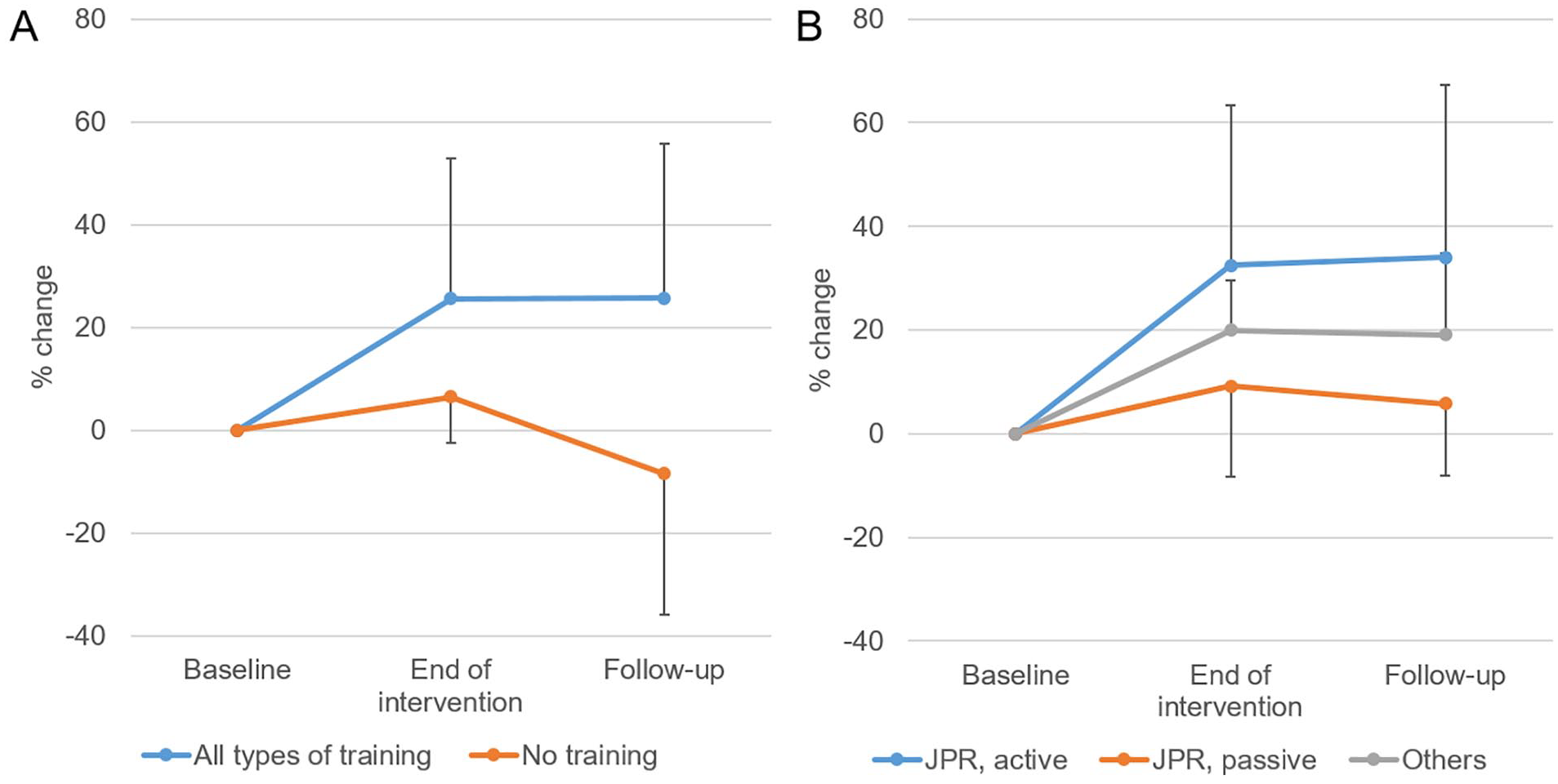
Retention of training effect on proprioceptive outcome measures. (A) The results of all types of training and no training were from 26 participant-outcome groups with 496 subjects and 3 groups with 73 subjects, respectively. (B) Among the training groups, 16 groups with 301 subjects, 5 with 113 subjects, and 5 with 82 subjects were evaluated by active JPR, passive JPR, and other outcome measures, respectively. Values are means and SDs.
Transfer of Training Effect to Different Proprioceptive Skills
Some studies evaluated proprioceptive improvements with multiple assessments. There were 5 studies (11 groups, 137 subjects) that evaluated both active and passive JPR, 4 studies (9 groups, 126 subjects) that evaluated both active JPR and TTDPM, and 6 studies (16 groups, 238 subjects) that evaluated both passive JPR and TTDPM in our review. The correlation was significant between the % changes of active JPR and TTDPM (r = 0.85, P < .01), and passive JPR and TTPDM (r = 0.7, P < .01), and neared significance for active and passive JPR (r = 0.58, P = .06). The beta coefficients in the regression equations were 0.4 between active and passive JPR and 0.63 between active JPR and TTDPM, representing greater changes after training in active compared to passive proprioceptive assessments (Figure 4). Baseline performances were also correlated between active and passive JPR and between passive JPR and TTDPM (see Supplemental 5).
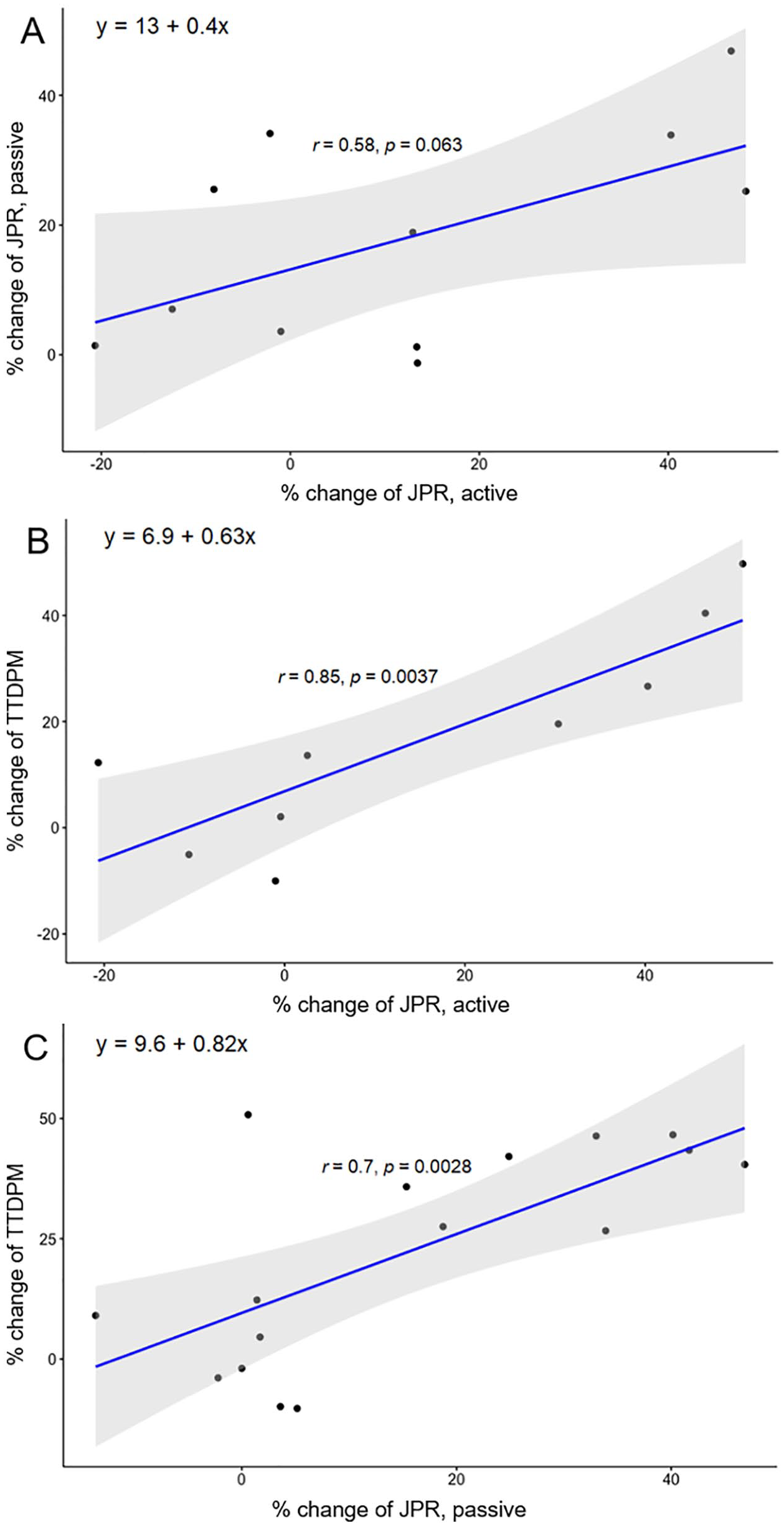
Transfer of training effect between proprioceptive outcome measures. The correlations were analyzed between the % changes of active and passive JPR (A), active JPR and TTDPM (B), and passive JPR and TTDPM (C). The shaded areas represent 95% confidence intervals.
Discussion
This systematic review aimed to investigate proprioceptive training using 4 key aspects of motor learning: specificity, acquisition, retention, and transfer. We found that training effects were larger for proprioceptive-targeted training versus non-targeted training. Acquisition was consistent with a 2 time-constant process with 1 fast and 1 slow time constant. Retention, across a minimum of a week, was excellent. Finally, the transfer of learning effects between different proprioceptive skills might occur. Now, we discuss these results and directions for future research.
Nature of Proprioception and its Assessment
Proprioception requires both sensory signals from peripheral mechanoreceptors, such as muscle spindles, Golgi tendon organs, and other receptors located in the joints and skin, and central processing to integrate the sensory information to determine body segment positions and movements in space.1,19 Corollary discharge, a central signal related to motor output, also contributes to the sensation of movement or position during active movements. 1 A recent neuroimaging study showed pure position sense-related activity in the right parietal and frontal cortices, including dorsal and ventral frontoparietal networks. 34 It was also reported that several brain regions beyond the primary somatosensory cortex, such as temporoparietal, supplementary/premotor, and insular cortices, were associated with accurate proprioception.35,36 Therefore, proprioception is not a simple passive reception of a sensory signal but rather a perception involving a complex array of information sources and central mechanisms for attention control, movement planning, and sensory processing that are shaped by memory and learning.
Due to the fundamental nature of proprioception being that stimuli originate from within the body and the complex neurophysiological processes described above, it is challenging to assess it objectively and quantitatively. Currently, 2 main assessments of proprioception have been utilized: the detection of position and the detection of motion. 2 These are JPR and TTDPM, which were also the most common outcomes in this systematic review. JPR has several subtypes, such as active or passive, ipsilateral or contralateral, and using memory or not, which have very different requirements for motor command and control, interhemispheric communication, and working memory. 37 Therefore, improvement in JPR after training may be due to improvements in these factors in addition to pure proprioception. On the other hand, TTDPM may more directly reflect proprioceptive sensitivity with less cognitive and no motor system involvement. Nevertheless, we cannot exclude the possibility that cognitive functions, such as perceptual decision-making, attention, and explicit awareness, and assessment familiarity due to repetition may be involved in improving proprioceptive assessments. Although often insignificant and minor compared to other training groups, some improvement observed in the no training group may represent the effect of assessment familiarity. It is essential to recognize these limitations of current proprioceptive assessments for interpreting the results of this study.
Specificity of the Training Effect
Proprioceptive-targeted training produced the largest effect sizes in proprioceptive outcomes compared to non-targeted training or no training. This suggests that it is possible to optimize proprioceptive training paradigms, although it remains unclear how to do this. Potential insight can be gained by considering the training effect according to the subcategories of training.
Among the subcategories of training, proprioceptive training and balance/coordination represent the most widely used training types in the literature and showed the largest effect size. Although there was a wide variety of training methods described as “proprioceptive training” in the literature, most of them targeted proprioception in the leg joints and incorporated static or dynamic balance training components. Balance involves other sensory systems (ie, the vestibular system and vision), therefore these “proprioceptive training” approaches are not purely proprioceptive. Only a few studies had training tasks with an eye-closed condition to further challenge proprioceptive function.38-40 Therefore, there was little difference between the actual methods of proprioceptive and balance/coordination training in the literature, and they resulted in a similar effect on proprioception.
Only 1 study investigated the effect of proprioceptive training on the upper limb in patients with diabetic polyneuropathy. 41 In this study, the proprioceptive training included duplicating wrist position tasks, similar to active JPR. This study found an even larger effect size with a mean % change of 58.2 and g of 2.30. For proper evaluation of training effects and better outcomes, a more precise definition of proprioceptive training will be needed in future investigations.
PNF/manual therapy and popular low-impact activities also showed a large effect size on proprioceptive acuity. The actual training methods of PNF/manual therapy varied from study to study, with the exception of the application of specialized manual techniques by therapists. One study even included proprioceptive training like TTDPM and JPR tasks performed manually by the therapist. 42 Therefore, their effect on proprioception should be considered individually in each study. Although popular low-impact activities also included various forms of exercise, such as Tai Chi, Yoga, Pilates, Taijiquan, and dance, these activities may train similar mechanisms of proprioception as all these activities require sensorimotor coordination and balance. Although a relatively extended intervention period, up to 24 weeks, likely influenced the group-level effect size, long-term application may be a fundamental advantage of these popular low-impact activities.
Among the non-targeted training, strengthening/resistance training demonstrated a relatively large effect size. Although its primary purpose is not the improvement of proprioception, several studies have described possible mechanisms by which strengthening/resistance training may influence proprioception.43-45 Neural adaptations induced by resistance training, such as motor unit facilitation, enhanced motor unit synchronization, and Golgi tendon organ inhibition, may affect proprioception. 43 In patients with knee osteoarthritis, increasing muscle strength may enhance proprioceptors’ sensitivity outside the knee capsule and alleviate joint pain by attenuating the loading forces, which may also result in proprioceptive improvement. 44 In volleyball players with infraspinatus muscle atrophy, shoulder strengthening training induced greater joint stability and may have increased the efficiency of mechanoreceptors, including muscle spindles, thereby contributing to better shoulder motion detection and position sense. 45 Therefore, strengthening/resistance training may improve proprioceptive acuity through a general mechanism as well as joint- and disease-specific mechanisms. 46
The difference in training effect between targeted and non-targeted training was particularly remarkable when active JPR was the outcome measure. This result suggests that the specificity of training may matter more in active rather than passive proprioception tests. Active tests involve fusimotor drive and muscle spindle feedback during active movement control, 19 and motor activity evokes corollary discharge affecting sensation of limb position. 1 These unique features could be additional training targets for further improvement. For example, a recent study revealed that neuroplastic changes occurred in interactions between the primary motor and somatosensory cortices during the skill learning process. 47 Therefore, a training program that adequately targets sensorimotor integration may lead to an additional improvement in a proprioception task requiring motor activity. However, as discussed in the previous section, it is important to consider whether observed improvements in either the motor command or sensorimotor integration associated with proprioceptive tasks are solely related to enhancements in proprioception.
With regard to interpreting the specificity of the training effect, it is also necessary to consider the characteristics of the population. This study showed a relatively large effect of training in the population with musculoskeletal diseases, regardless of training type, compared to the healthy and neurologic disease populations. Considering that all but 1 group (diabetic polyneuropathy) in the neurologic disease population had central nervous system disorders (stroke, Parkinson’s disease, and multiple sclerosis), this result suggests that it is difficult to improve proprioceptive acuity by training when the central nervous system is damaged. Although maladaptive central nervous system reorganization in chronic musculoskeletal disorders may contribute to altered joint control and pain, 48 this does not appear to significantly affect proprioceptive learning. The small effect size in the healthy population might be attributable to a ceiling effect, as many study groups included young adults and athletes.
Temporal Features of Acquisition of Proprioceptive Acuity
Although the number of relevant studies was limited, our review suggests both immediate and cumulative effects of training on proprioceptive acuity. These appeared similar to fast and slow learning, as observed in motor skill learning. 13 However, the mechanisms underlying the acquisition of proprioceptive acuity have not been fully elucidated yet and may differ from motor learning, which already has a vast amount of related research.13,49 The cortical somatosensory map is highly plastic even in the adult brain and changes actively to suit behavioral demands and compensate for injury. 50 Several studies have reported that a short-term intervention, such as a repetitive motor task,51,52 tactile coactivation, 53 or regional anesthesia, 54 induced neuroplastic changes in the somatosensory areas with relevant behavioral or symptomatic changes. In addition, prolonged sensory experience and task training for weeks to months induce somatosensory map plasticity. 50 Hebbian plasticity in response to use or training has been suggested as the underlying mechanism of this map plasticity. 55 The acquisition of proprioceptive acuity after training reported in our review may have a similar underlying mechanism of neuroplasticity in the somatosensory areas. Since most previous studies have focused on tactile sensation, further investigation of proprioceptive learning mechanisms is warranted.
Retention of Proprioceptive Acuity After Training
Our review demonstrated that the training effect on proprioception was maintained at follow-up evaluation after the end of training. The retention of the training effect probably occurs in proprioception for at least several weeks to months. The primary motor cortex and striatum are known to play essential roles in the consolidation of motor skills. 13 A previous study reported that consolidation of somatosensory memory also occurred associated with motor learning, and improved proprioceptive acuity was retained for up to 10 days after 5 days of wrist-reaching movement training. 56 It has also been reported that the somatosensory cortex is involved in motor memory consolidation. 57 Although these studies investigated somatosensory learning accompanied by motor learning, they suggested that consolidation and retention similar to that observed in motor learning may occur in proprioceptive learning. Further research on the retention of the training effect specific to proprioception across a more extended period, as well as on the neural substrates involving the consolidation of somatosensory learning will be needed.
Transfer of Training Effect Between Different Proprioceptive Assessments
From the motor learning perspective, transfer refers to the application of a learned skill in a novel context. 58 More specifically, transfer can be defined as the improved capability for performance in 1 task as a result of practice on some other task. 14 In this systematic review, we were unable to find any studies that provided training specific to only 1 proprioceptive task and assessed another proprioceptive task with a different nature. As an alternative, we tried to investigate the transfer of training effect in proprioception tasks by analyzing the correlation between changes in different proprioceptive assessments. However, the training methods were not specific to 1 proprioceptive task but rather general training to challenge or influence proprioception and related functions. Therefore, it is unclear whether the observed correlation is a transfer of learning from 1 proprioceptive task to another or whether training affects multiple aspects of proprioception and enhances them together. In addition, strong correlations of baseline performances between active and passive JPR and between passive JPR and TTDPM may suggest that common mechanisms are involved in these assessments, potentially indicating a mechanism for the transfer of training effect. Because the joint receptors, such as Ruffini and Golgi-type mechanoreceptors, are thought to be selectively stimulated during TTDPM and passive JPR at a slow angular velocity, 59 the correlation between the changes of these 2 passive tasks was predictable. On the other hand, the reason for the high correlation between the changes of active JPR and TTDPM seems unclear. A marginally insignificant correlation between active and passive JPR may imply different neurophysiological processes under the active and passive proprioceptive tasks, although low statistical power due to the small sample size should be considered.
The characteristics and mechanism of motor learning transfer to the contralateral limb, or cross-education, have been extensively studied and discussed.60-63 A few studies in this review have also investigated the transfer of training effect on proprioception to the contralateral body part. El-Gohary et al 64 reported a 41.7% improvement in active JPR of the non-dominant knee after proprioceptive training on the dominant leg. Wang et al 65 reported 32.1 and 17.3% of improvement in joint angle discrimination and active JPR of the contralateral wrist after robot-aided visuomotor wrist training. They also suggested that the neural mechanism underlying proprioceptive learning transfer relies on interhemispheric connections via the corpus callosum. There are callosal connections between the secondary somatosensory cortices, which are important for somatosensory signal integration, as well as homotopic regions of the primary somatosensory cortices.66,67 It has also been reported that tactile perceptual learning was transferred to the untrained contralateral hand. 68 Thus, various forms of transfer seem to be in play during proprioceptive training, and further research is required to clarify their characteristics and mechanisms.
Study Limitations and Future Directions
First, although a total of 106 studies were included in this review, most were small studies with the median number of participants in each group being 15. In addition, the training methods were diverse even in the same subcategory, and heterogeneity was also large in the outcome. To obtain clear evidence, large-scale clinical trials on each topic of proprioceptive learning are needed. Second, the majority of the disease groups covered in this review were musculoskeletal disorders, and research on neurological disorders was limited. In the case of musculoskeletal diseases, it should be considered that the performance of the proprioception task may have been improved indirectly due to pain relief or joint stability improvement as a result of the training. Third, although the effect of assessment familiarity observed in the no training group was minimal, this effect could be more significant when proprioceptive assessment methods are included as a training component. However, because only 6 groups from 4 studies included proprioceptive assessment methods in their training,41,42,69,70 this should have only a minor effect on the overall results. Fourth, few studies have included evaluation in the middle of the intervention. Although the results of these studies suggest a second time constant in the learning curve for proprioception training, long-term studies with repeated evaluations during and after intervention are required to confirm an apparent learning curve.
We could not draw clear conclusions about important questions, such as which form of proprioception-targeted training was most effective, which populations can benefit most, what the specific values of the two-time constants are, how long retention lasts, and the mechanisms of transfer. These are all important directions for future research.
Supplemental Material
sj-docx-1-nnr-10.1177_15459683231207354 – Supplemental material for A Systematic Review of the Learning Dynamics of Proprioception Training: Specificity, Acquisition, Retention, and Transfer
Supplemental material, sj-docx-1-nnr-10.1177_15459683231207354 for A Systematic Review of the Learning Dynamics of Proprioception Training: Specificity, Acquisition, Retention, and Transfer by Han Gil Seo, Seo Jung Yun, Andria J. Farrens, Christopher A. Johnson and David J. Reinkensmeyer in Neurorehabilitation and Neural Repair
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by NIH R01HD062744 and NIDILRR 90REGE0010.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.