
Abstract
Background
Balance training covers a range of different modalities and complexity levels for people with multiple sclerosis (MS). When evaluating the effects of balance training across different kinds of interventions, determination of the specific intervention content that predict effects are needed.
Objective
To investigate the effects of balance training on gait and dynamic balance outcomes.
Methods
Four databases were systematically searched. Randomized controlled trials involving people with MS (Expanded Disability Status Scale [EDSS] score ≤7.5) where at least 50% of the intervention targeted balance control were included. Interventions were categorized based on training types. Risk-of-bias was assessed using the Tool for the Assessment of Study Quality and Reporting in Exercise (TESTEX).
Results
A total of 18 included studies involved 902 people with MS (EDSS range from 0 to 7.5). Interventions evaluated with a balance composite score or a mobility test showed a moderate effect size (ES = 0.46 [95% confidence interval (CI) = 0.18 to 0.74]; p < .01) and a small overall ES (ES = 0.19 [95% CI = 0.01–0.36]; p = .04), respectively, across different training types. Stepping and gait speed outcomes showed no effect. Cognitive dual-task training showed a significant effect (ES = 0.81 [95% CI = 0.24 to 1.37]) on subgroup level, when evaluated with a mobility outcome measure. The median TESTEX score on study quality and reporting was 11 (maximum score = 15).
Conclusions
Improvements of balance were found across interventions when measured by balance composite scores and mobility tests, but not when measured by stepping or gait speed outcomes. Large training volume was positively associated with effect on balance. A definition of intensity in balance training is needed for evaluation of its impact on the effect of balance interventions.
Introduction
Multiple sclerosis (MS) is a chronic inflammatory and neurodegenerative disease of the central nervous system. 1 As the disease progresses, a wide range of impairments appear, including disturbances in gait and balance.1,2 About 50% to 80% of people with MS (PwMS) live with balance impairment, 2 resulting in decreased mobility, and increased fall risk.3 -5
Balance control is a complex motor skill derived from interaction of multiple subsystems 6 which includes motor, sensory, and cognitive balance components (Table 1). Neural lesions and degeneration due to MS affect signal conduction and integration involving peripheral nerves,7,8 spinal cord, and cerebral cortex. 9 Degeneration of neural pathways alters the integration of sensory inputs and hampers the execution of rapid, adequate motor output 10 causing deficits of balance control. 11 Furthermore, the cognitive processing of sensory inputs is also affected. This processing is influenced by, for example, limbic activity, 12 fatigue, 13 anticipation, 14 and divided attention.15 -17
Definition of Concepts.
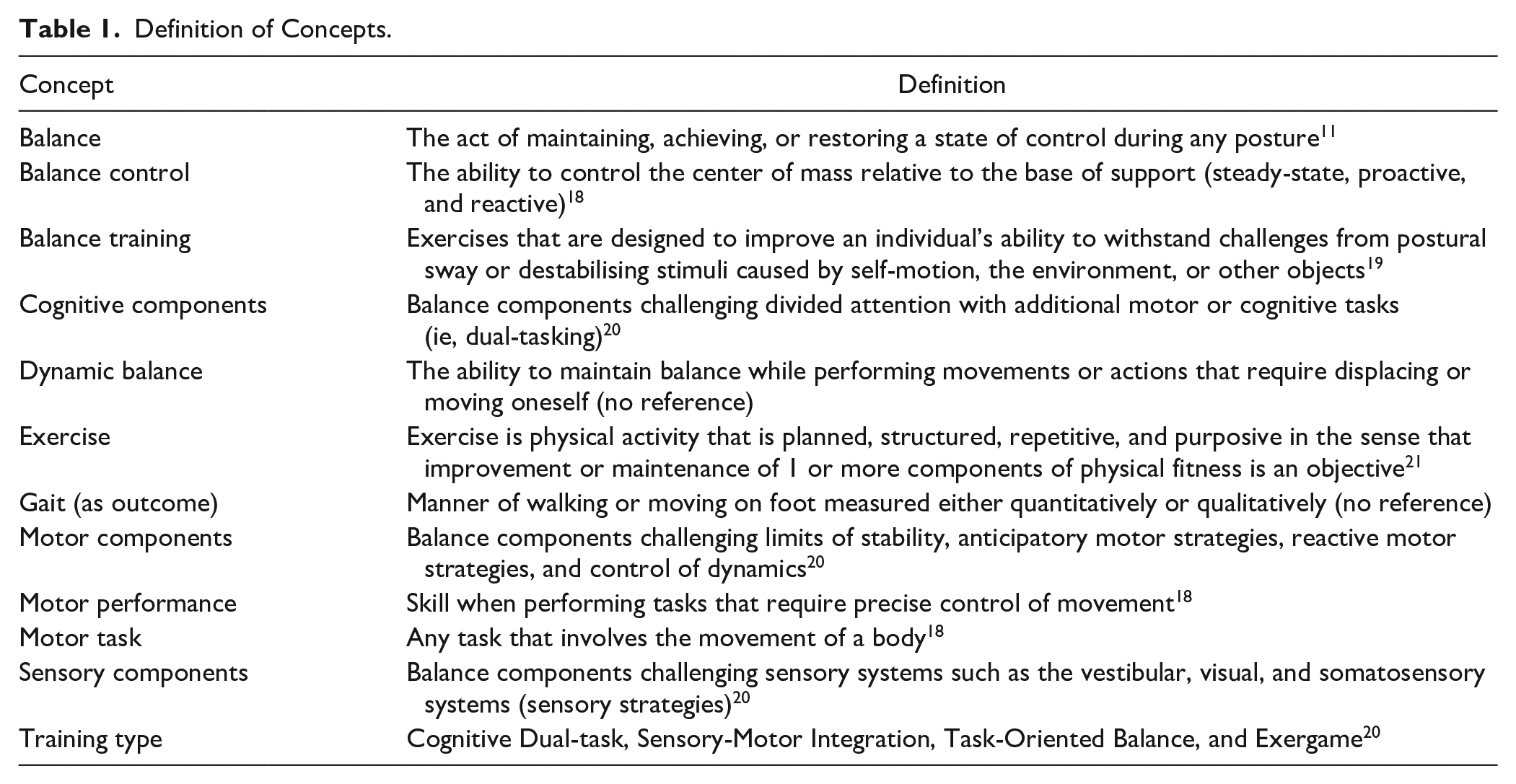
Balance training is defined as exercises focusing on controlling the center of mass relative to the base of support during different challenging activities. The causal effect from balance training is explained by neuroplasticity, defined as “the ability of the central nervous system to adapt in response to changes in the environment or lesions.” 22 The strive for an improved quality of performance when conducting a challenging motor task promotes reorganization in neural networks, 18 leading to improvement of balance. To enhance balance performance balance training should challenge the subsystems 6 underlying balance control and aim to enhance balance for at least 50% of the intervention, 19 where most exercises should focus on improving sensorimotor processes of balance control.
When outlining protocols for resistance and aerobic training, it is recommended to adhere to the frequency, intensity, type, time, volume, and progression principles, which encompasses Frequency (how often), Intensity (how hard), Time (duration), and Type (mode of exercise), Volume (amount of exercise), and Progression (how exercise is advanced). 23 Training volume can be calculated by multiplying Frequency/number of sessions by Time per training session and/or Duration of intervention. Of the mentioned parameters, intensity is significantly associated with improvement in resistance training and aerobic training. However, in balance training protocols, intensity is often conflated with training volume. This contrasts with its usage in resistance and aerobic training, where intensity is typically expressed as repetition maximum or as percent of maximum heart rate (%HRmax) or heart rate reserve (%HRmax-resting), respectively. 23 In these contexts, intensity represents a relative load, with the individual’s maximal capacity defining the absolute scale range. However, in balance training, there’s no established expression of intensity that accounts for the challenge to the balance control relative to the individual’s capacity. Yet, Farlie et al 24 has proposed a definition where “the degree of challenge to the balance control system relative to the capacity of the individual to maintain balance” can be considered as intensity.
Balance training is carried out in approaches ranging from static position training and functional training during ambulation to vestibular-ocular training, horse riding, Tai Chi, and exergaming. Therefore, the substantial diversity between these interventions poses a specific challenge when recommending 1 type over another.
A recent review indicates the importance of training volume in achieving effective results in diverse interventions that address balance in PwMS. 25 Balance training research performed in healthy elderly populations suggests that duration of training and level of challenge (intensity), optimally progressive, are critical factors for inducing beneficial training effects. This recommendation is asserted universally, disregarding divergent contributions from different types of balance training 26 and without a common understanding of what intensity in balance training is. Nevertheless, the impact of content in different balance training types to improve balance remains unclear.
A former review by Brincks et al 20 categorized interventions according to their specific targeting of motor, sensory, and cognitive components (Table 1). The number of components included in the training was suggested to reflect the level of intervention complexity. The review proposed an approach where complexity mirrors intensity, and revealed that several studies across training types challenged participants at a moderate level. The review also concluded that the effect on balance control was evaluated with many outcome measures, ranging from measurements of single properties (eg, sway area in standing) to functional composite scores such as the Bergs balance Scale. However, the review neither investigated whether an effect of balance training on balance control was evident nor if the level of complexity of an intervention impacted the effects of the balance intervention. Thus, the present systematic review aimed to investigate the effects of diverse balance training interventions on gait and dynamic balance outcomes and if intervention complexity impacts the effect of a balance training intervention in PwMS.
Methods
Protocol and Registration
This systematic review was preregistered in the international prospective register of systematic reviews (PROSPERO:CRD42020181093), the protocol is available at https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=181093. The review follows the guidelines presented in the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) statement. 27
Eligibility Criteria
Eligible study designs were randomized controlled trials (RCT) involving adults aged 18 years or older with a diagnosis of MS, an Expanded Disability Status Scale (EDSS) ≤7.5, 28 able to transfer from 1 seated position to another independently (eg, from a wheelchair to a chair), not considering disease duration and phenotype of MS. Planned and structured balance training interventions aimed at improving sensorimotor processes of balance control for at least 50% of the total intervention time, and which challenged at least 2 out of 6 balance subsystems (ie, biomechanical constraints, movement and sensory strategies, orientation in space, control of dynamics, and cognitive processing 6 ) were included.
Studies had to include non-training controls (usual care) or active control conditions that included exercise interventions that had no expected effects on balance control, for example, stretching or relaxation. Studies were eligible for inclusion if balance control was evaluated with outcomes reflecting postural stability (such as Berg Balance Scale, Functional Reach Test, Tandem Stand Test, Romberg’s Test, and measures of postural sway) or activities challenging balance during walking or functional mobility (such as Mini-Balance Evaluation System Test [BESTest], Six Spot Step Test, Functional Gait Assessment, Timed Up & Go, 25-Foot Walk Test, 10-Meter Walk Test, and 6-Minute Walk Test).
Searches, Information Sources, and Study Selection
This study is a continuation of our previous systematic review. 20 The review included 40 studies based on a literature search conducted in April 2020 (Figure 1). For the present review the literature search was updated in January 2023, and new studies were added to the sample of studies from the previous review. 20 The searches were conducted by librarians at the Karolinska Institutet University Library in the following databases: Medline (Ovid), EMBASE, Web of Science (Clarivate), and Cinahl (Ebsco). Search terms including Medical Subheadings, Emtree terms, and Cinahl headings were MS, postural balance, walking, gait, clinical trials, controlled trials, randomized controlled trials, and case-controlled trials. Full search strategy is available at https://www.crd.york.ac.uk/PROSPEROFILES/181093_STRATEGY_20200420.pdf. Screening process on newfound studies was performed by the same authors (J.B. and S.J.) as in the previous review. 20 Eligibility assessment for final inclusion of studies in the present review was conducted by 2 other authors (A.W. and J.C.).
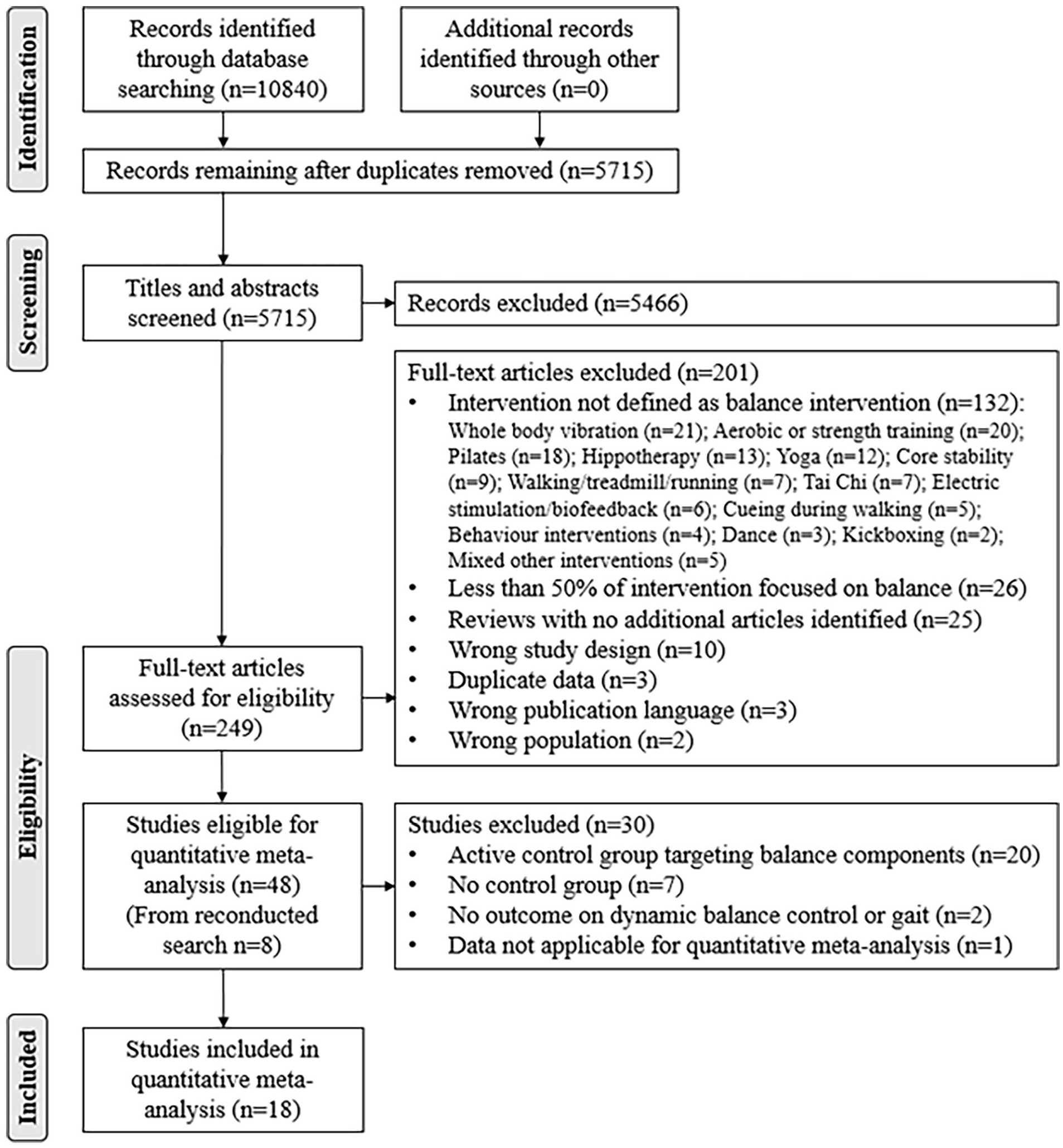
Preferred reporting items for systematic reviews and meta-analyses flow diagram on the search result and study selection process.
Data Management and Collection Process
Data extraction included study design and population, sample size, training and control intervention type, duration, volume, and outcome measures (Table 2). Interventions were grouped into 4 training types (Cognitive Dual-task, Sensory-Motor Integration, Task-Oriented Balance, and Exergame) based on the main focus and balance components (motor, sensory, and cognitive) challenged during the intervention. Categorization of training types and challenged balance components in the interventions was adapted from the previous review 20 presented in Table 2. Balance-related outcome measures were grouped into 4 Outcome categories based on type of outcome measure or the specific domain evaluated. The outcome categories were: Balance composite score (Berg Balance Scale and mini-BESTest); Mobility (Timed Up&Go and Six Spot Step Test); Gait speed outcomes (10-Meter Walk Test, 25-Foot Walk Test, and gait speed as a parameter measured in gait analysis); and Stepping (Four Square Step Test; Table 2). Two reviewers (A.W. and J.C.) completed the data extraction. Missing data were requested from authors of 7 studies29 -35 and obtained from 5 of them.30,31,33 -35 Data were considered missing if the author had not replied after 2 follow-up requests. Missing data on mean values and standard deviation from 1 study were calculated based on reported values on 95% confidence interval in the study. 32
Descriptive Data of the Included Balance Training Interventions in People With Multiple Sclerosis: Information on Training Category, Study Design, Study Population, Disease Characteristics, and Functional Mobility Level.
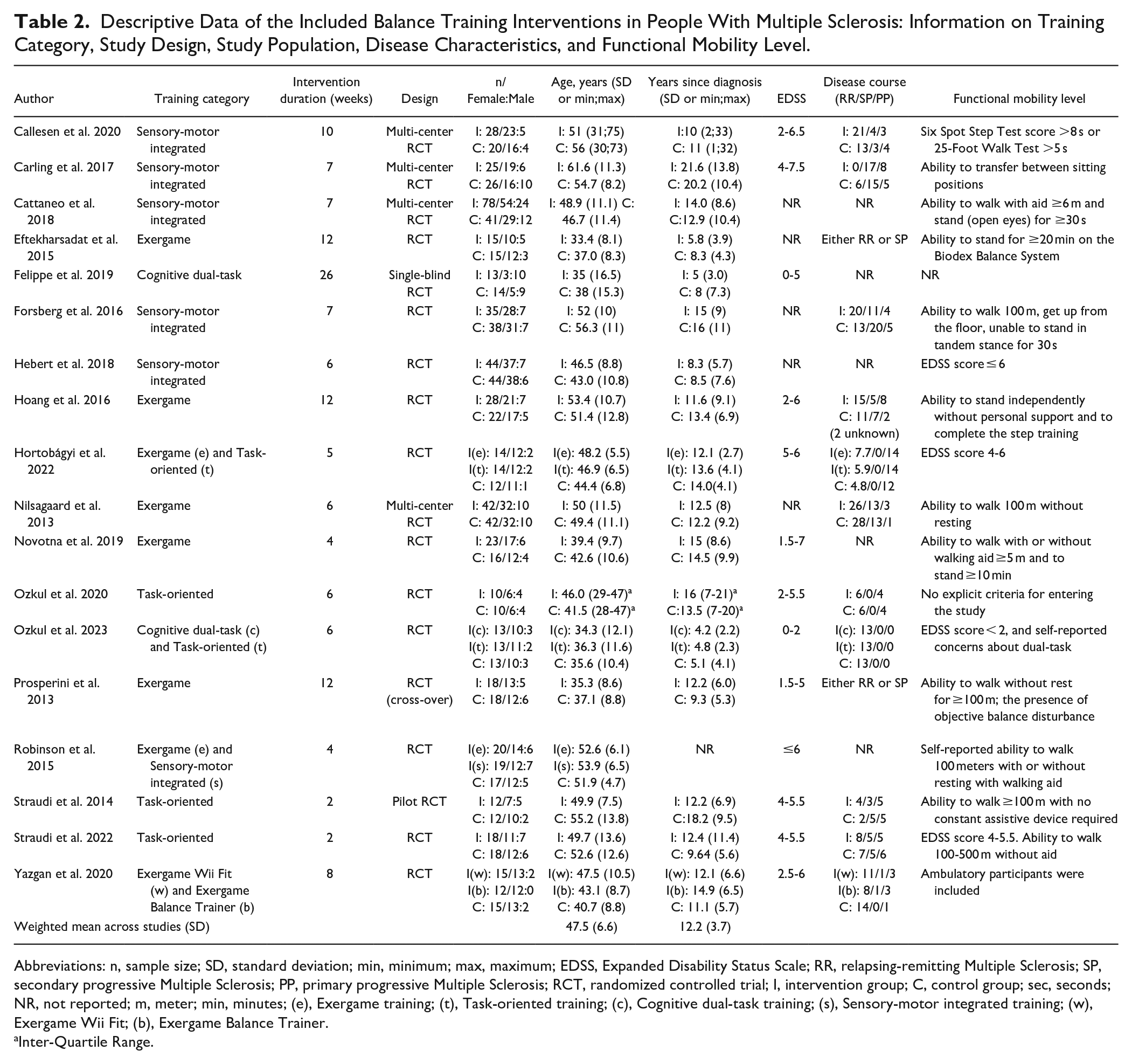
Abbreviations: n, sample size; SD, standard deviation; min, minimum; max, maximum; EDSS, Expanded Disability Status Scale; RR, relapsing-remitting Multiple Sclerosis; SP, secondary progressive Multiple Sclerosis; PP, primary progressive Multiple Sclerosis; RCT, randomized controlled trial; I, intervention group; C, control group; sec, seconds; NR, not reported; m, meter; min, minutes; (e), Exergame training; (t), Task-oriented training; (c), Cognitive dual-task training; (s), Sensory-motor integrated training; (w), Exergame Wii Fit; (b), Exergame Balance Trainer.
Inter-Quartile Range.
Risk-of-Bias Assessment
Risk-of-bias was independently assessed by 2 blinded reviewers (A.W. and J.C.) using the Tool for the assEssment of Study qualiTy and reporting in EXercise (TESTEX) scale. 36 The TESTEX scale is considered a reliable tool specifically designed to facilitate the reviewing of exercise training trials. 36 The TESTEX scale consists of 12 items, of which 5 refer to the assessment of study quality (items 1 to 5), and 7 refer to the assessment of study reporting (items 6 to 12). The TESTEX scale ranges from 0 to 15. After blinded assessment (A.W. and J.C.), disagreements were discussed and resolved with the other review authors (S.J., J.B., U.D., and E.F.). In TESTEX scale item 2 (randomization), minimization was considered a valid randomization method, while cluster randomization was not. Furthermore, in TESTEX scale item 7 (intention-to-treat analysis), imputation of missing data was accepted as a valid intention-to-treat approach.
Synthesis of Results
Data from the included studies were descriptively summarized (Table 2). Random-effects meta-analyses based on data from functional balance outcome measures were conducted using IBM® SPSS® Statistics version 28.
Outcome measures capturing comparable aspects of functional balance control were pooled into specific outcome categories. Thus, interventions evaluated using multiple outcome measures could be included in meta-analysis within multiple outcome categories.
Post-intervention mean and standard deviation values of different outcome measures were used to calculate the intervention effect, as recommended by the Cochrane Handbook of Meta-analysis. 37 Values from midpoint measurements were used in studies with cross-over 38 and/or wait-list 39 RCT designs. Extracted baseline values were also displayed, although not used in the analysis. This was done to ensure full transparency regarding discrepancies between the original studies’ results and those reported in this review. The pooled effect was summarized using Hedges’ g statistics to allow for comparison across different outcome measures. Forest plots illustrated effect sizes (ES) with 95% confidence intervals (CIs) for individual studies and pooled effect.
Positive ES indicated improvement in favor of the intervention. An ES > 0.61 was regarded as large, >0.31 and ≤0.61 as moderate, and >0.14 and ≤0.31 as a small. 40 p-values <.05 were considered significant.
Heterogeneity was defined as Higgins’ I2 > 50%, and no or limited heterogeneity was defined as Higgins’ I2 ≤ 50%. 41
Funnel plots were created to assess publication bias in outcome categories, including at least 10 studies. 42
Univariate meta-regression analyses were conducted post hoc to investigate whether training volume and/or training complexity (number of balance components included in the training) were associated with ES. Training volume was log-transformed to account for a skewed distribution.
Additional adjusted meta-analyses were conducted where baseline values were retracted from the group-level post-measures. Standard deviations from post-intervention measures were used. This was done to adjust for potential misinterpretations that changes between post-intervention measures (intervention versus control) were caused by changes between groups when, in fact, they were due to a difference between baseline measures. Additional analyses are presented in the Supplemental Material.
Results
Study Selection and Characteristics
The updated search yielded 2932 new records. After removal of duplicates, 690 records were screened for inclusion based on title and abstract (Figure 1). From this, 8 full-text articles were added to the sample from the previous review, 20 resulting in a total of 48 studies eligible for the present review, of which, 18 studies were included for meta-analysis (Figure 1).
The studies included 902 PwMS with an EDSS score of 0 to 7.5 (Table 2). In the studies where the EDSS level was not reported,30,35,43 -45 it was noted that functional mobility levels of included PwMS matched the EDSS range of the other studies. The weighted mean age of PwMS samples across studies was 47.5 (SD = 6.6) years, ranging from 33.4 32 to 61.6. 31 The weighted mean disease duration (years since diagnosis) of PwMS samples across studies was 12.2 (SD = 3.7) years, ranging from 4.2 46 to 21.6 31 years (Table 2).
Training Types and Outcome Categories
Six studies applied the training type sensory-motor integrated training,30,31,43,45,47,48 8 applied exergame training,34,35,38,44,48 -51 2 applied cognitive dual-task training,32,46 and 5 studies applied task-oriented training.33,34,39,46,52 Three studies included interventions that comprised 2 different training types34,46,48 (Table 2).
The duration of the interventions ranged from 239,52 to 26 weeks 32 (Table 2), with a total delivered training volume ranging from 6 35 to 52 32 hours (Table 3). In cognitive dual-task training and sensory-motor integrated training, the median number of balance components challenged was 6.5, while the median number of components was 6 within the task-oriented training. The median number of components challenged in exergame training was 3 (Table 3).
Overview of Intervention Types, Outcome Categories, Balance Components Challenged in the Training, Training Volume in the Intervention, and the Corresponding Effect Size.
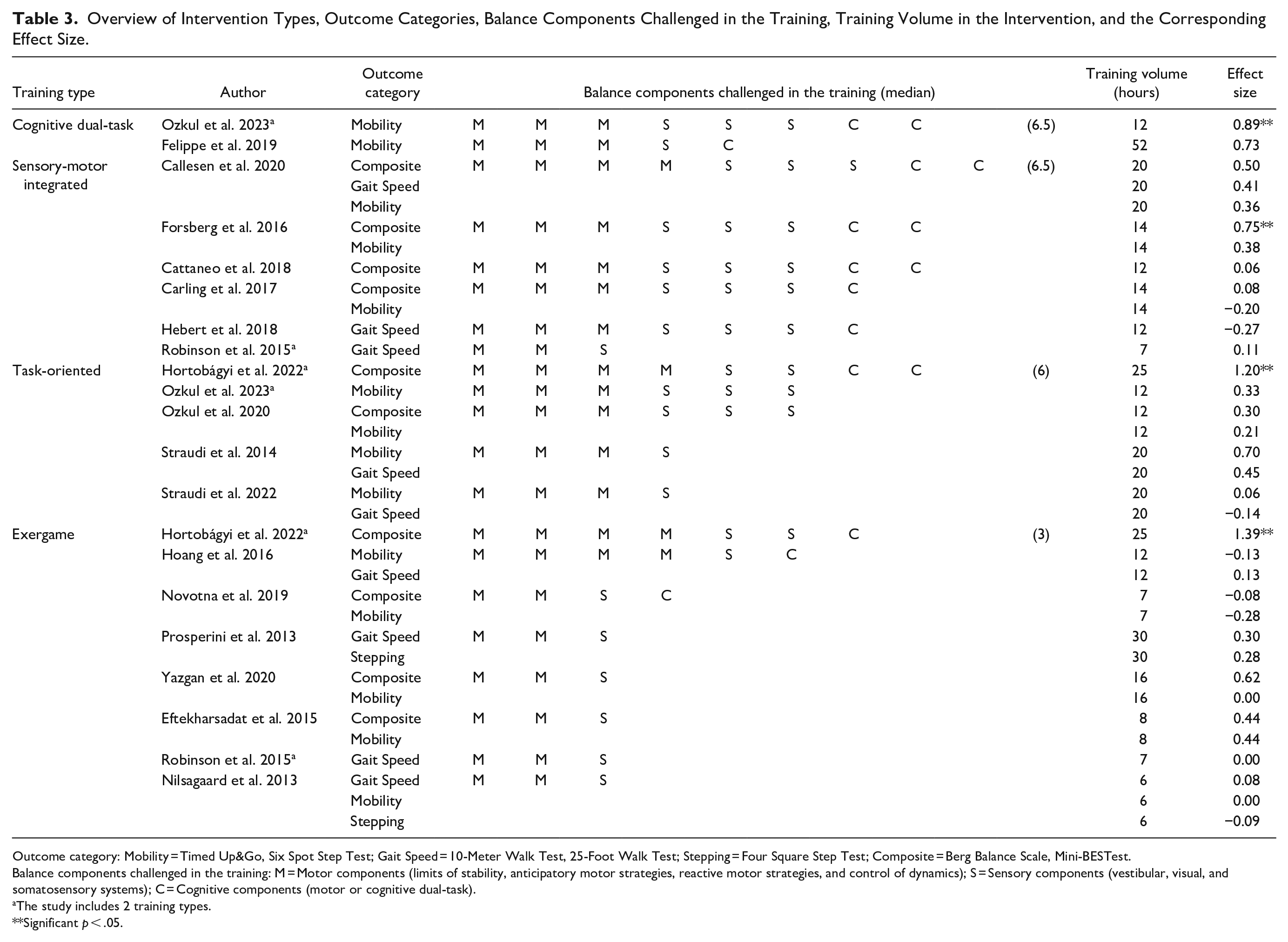
Outcome category: Mobility = Timed Up&Go, Six Spot Step Test; Gait Speed = 10-Meter Walk Test, 25-Foot Walk Test; Stepping = Four Square Step Test; Composite = Berg Balance Scale, Mini-BESTest.
Balance components challenged in the training: M = Motor components (limits of stability, anticipatory motor strategies, reactive motor strategies, and control of dynamics); S = Sensory components (vestibular, visual, and somatosensory systems); C = Cognitive components (motor or cognitive dual-task).
The study includes 2 training types.
Significant p < .05.
Two studies reported 3 outcome measures of functional balance,35,47 which enabled inclusion into 3 different outcome categories in the meta-analyses (Table 3). Further, 10 studies were included into 2 outcome categories,30,31,33,38,39,44,49 -52 and 6 studies were evaluated with 1 outcome measure of functional balance32,34,43,45,46,48 (Table 3).
Risk-of-Bias Assessment
The median TESTEX score of included studies was 11 (Table 4). Two studies (11%) reported activity monitoring in control groups35,46; 7 studies (39%) performed a valid intention-to-treat analysis31,39,43,44,48,50,52; and 9 studies (50%) reported that exercise load was adjusted to keep the relative intensity constant throughout the intervention period.31,32,34,38,46 -48,50,51 The remaining TESTEX items were reported in more than 50% of the included studies. All studies presented a training protocol enabling calculation of the intended exercise volume. Detailed information on individual study scores can be found in Table 4.
Item and Total Scores on Risk of Bias Assessment for Each Study Included in the Meta-analysis Based on the Tool for the assEssment of Study qualiTy and Reporting in EXercise (TESTEX) Scale: 1 Point Indicate That Criterion Has Been Met, Zero (0) Point Indicate That Criterion Has Not Been Met.
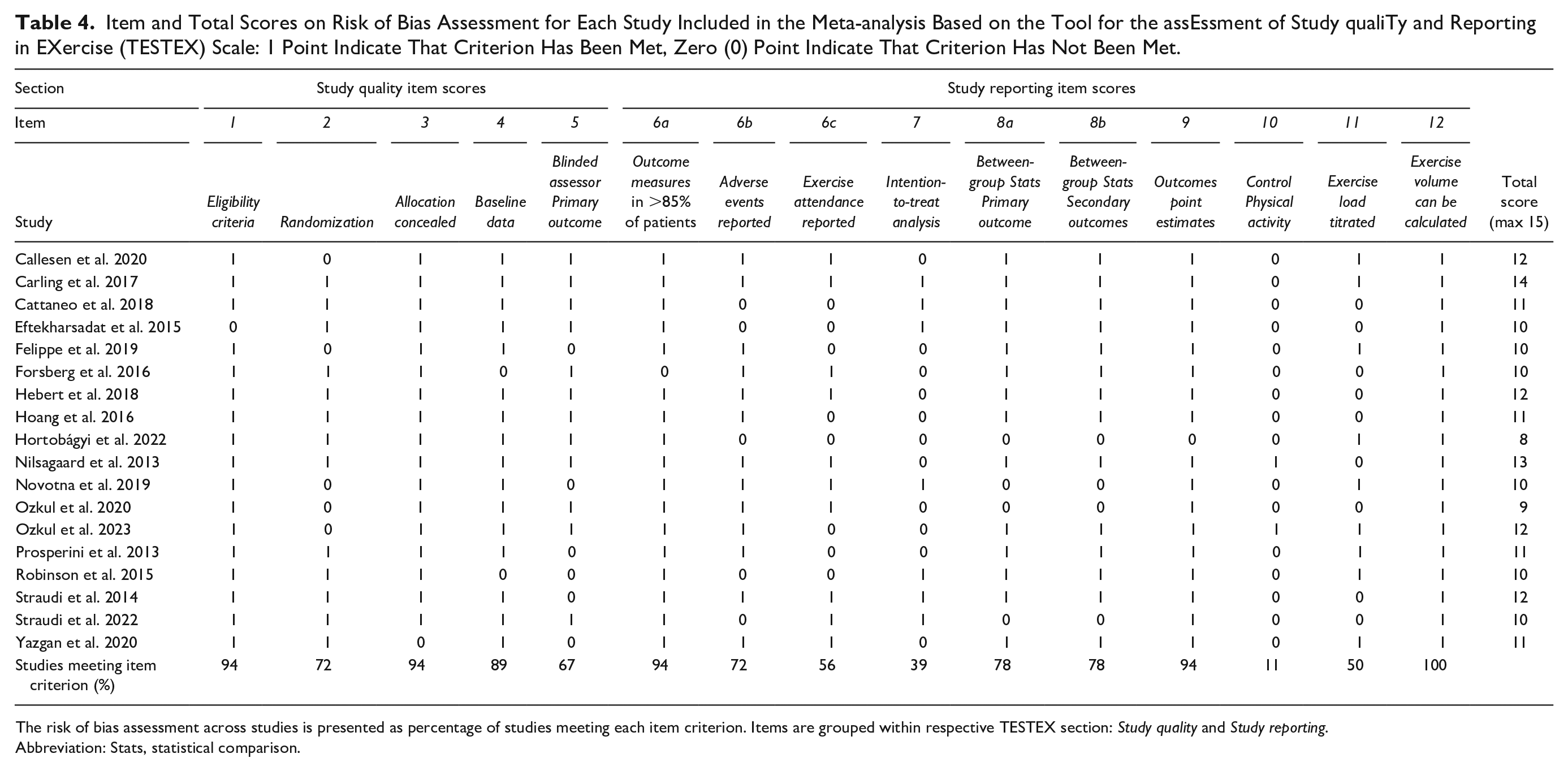
The risk of bias assessment across studies is presented as percentage of studies meeting each item criterion. Items are grouped within respective TESTEX section: Study quality and Study reporting.
Abbreviation: Stats, statistical comparison.
Synthesis of Results
Effects on Balance Composite Scores
Nine studies that included the training types exergame, sensory-motor integrated, and task-oriented, used a balance composite score for evaluation of the intervention effect30,31,33,34,43,44,47,50,51 (Table 5).
Meta-analysis of the Effect of Balance Training on four Outcome Categories in Subgroups of Training Types.
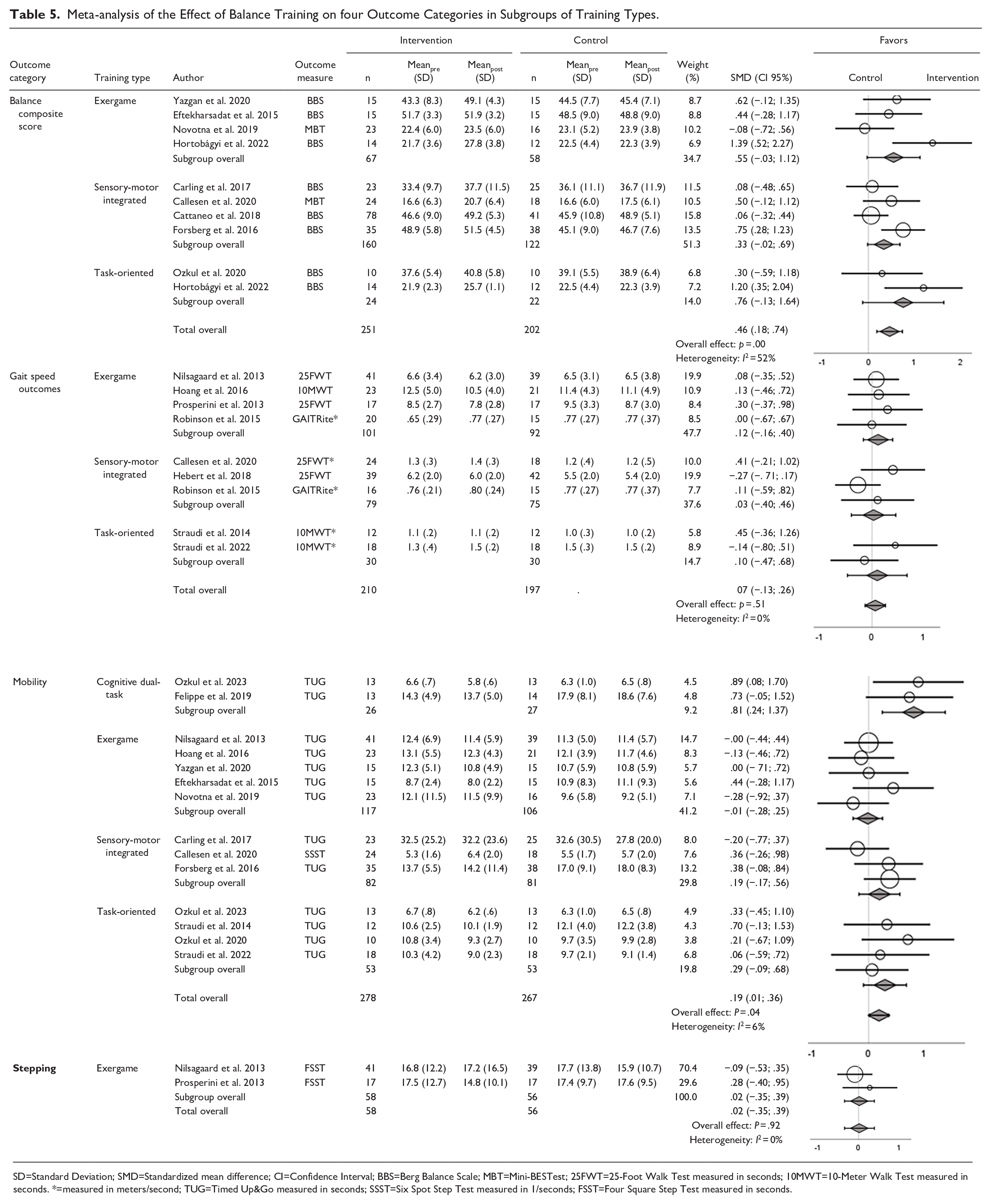
SD=Standard Deviation; SMD=Standardized mean difference; CI=Confidence Interval; BBS=Berg Balance Scale; MBT=Mini-BESTest; 25FWT=25-Foot Walk Test measured in seconds; 10MWT=10-Meter Walk Test measured in seconds. *=measured in meters/second; TUG=Timed Up&Go measured in seconds; SSST=Six Spot Step Test measured in 1/seconds; FSST=Four Square Step Test measured in seconds.
Overall ES, across exergaming, sensory-motor integrated training, and task-oriented training showed a moderate effect on balance composite scores, with a considerable heterogeneity (ES = 0.46 [95% CI = 0.18 to 0.74]; p = .00, I2 = 52%; Table 5).
On subgroup level, ES were considered moderate for exergame (ES = 0.55 [95% CI = –0.03 to 1.12]) and sensory-motor integrated training (ES = 0.33 [95% CI = –0.02 to 0.69]), and large for task-oriented training (ES = 0.76 [95% CI = –0.13 to 1.64]). None of the 3 training types reached significance.
Effect on Gait Speed Outcomes
Eight studies that included the training types exergame, sensory-motor integrated, and task-oriented applied gait speed as an outcome measure35,38,39,45,47-49,52 (Table 5). No overall or subgroup level effect was found in the meta-analysis (ES = 0.07 [95% CI = –0.13 to 0.26]; p = .51, I2 = 0%; Table 5).
Effects on Mobility
Thirteen studies that included the training types cognitive dual-task, exergame, sensory-motor integrated, and task-oriented, evaluated the effects of balance training on mobility30 -33,35,39,44,46,47,49,51,52 (Table 5). Overall, the meta-analysis showed a small significant effect of the interventions on functional balance when evaluated with a mobility test (ES = 0.19 [95%cCI = 0.01 to 0.36]; p = .04, I2 = 6%; Table 5).
At subgroup level, ESs were considered small for sensory-motor integrated (ES = 0.19 [ 95% CI = –0.17 to 0.56]) and task-oriented training (ES = 0.29 [CI 95% = –0.09 to 0.68]), and large for cognitive dual-task training (ES = 0.81 [95% CI = 0.24 to 1.37]), with the latter being significant.
Effects on Stepping
Two studies that included the training type exergame applied an outcome category related to stepping for evaluation of the intervention effect35,38 (Table 5). No effect was shown (ES = 0.02 [95% CI = –0.35 to 0.39]; p = .92, I2 = 0%).
Correlation Analyses
Visual inspection of weighted scatter plots (Figure 2) indicated an association between training volume and ES when measured by the outcome categories Balance composite score and Mobility. No association was found between Number of components in the training and ES. Analyses were conducted with studies pooled across training types. Corresponding meta-regressions showed significant associations between training volume and ES for the outcome categories Balance composite score (β = 1.05 [SE = 0.31]; p < 0.01) and mobility (β = .47 [SE = 0.21]; p = .03; Supplemental Material).
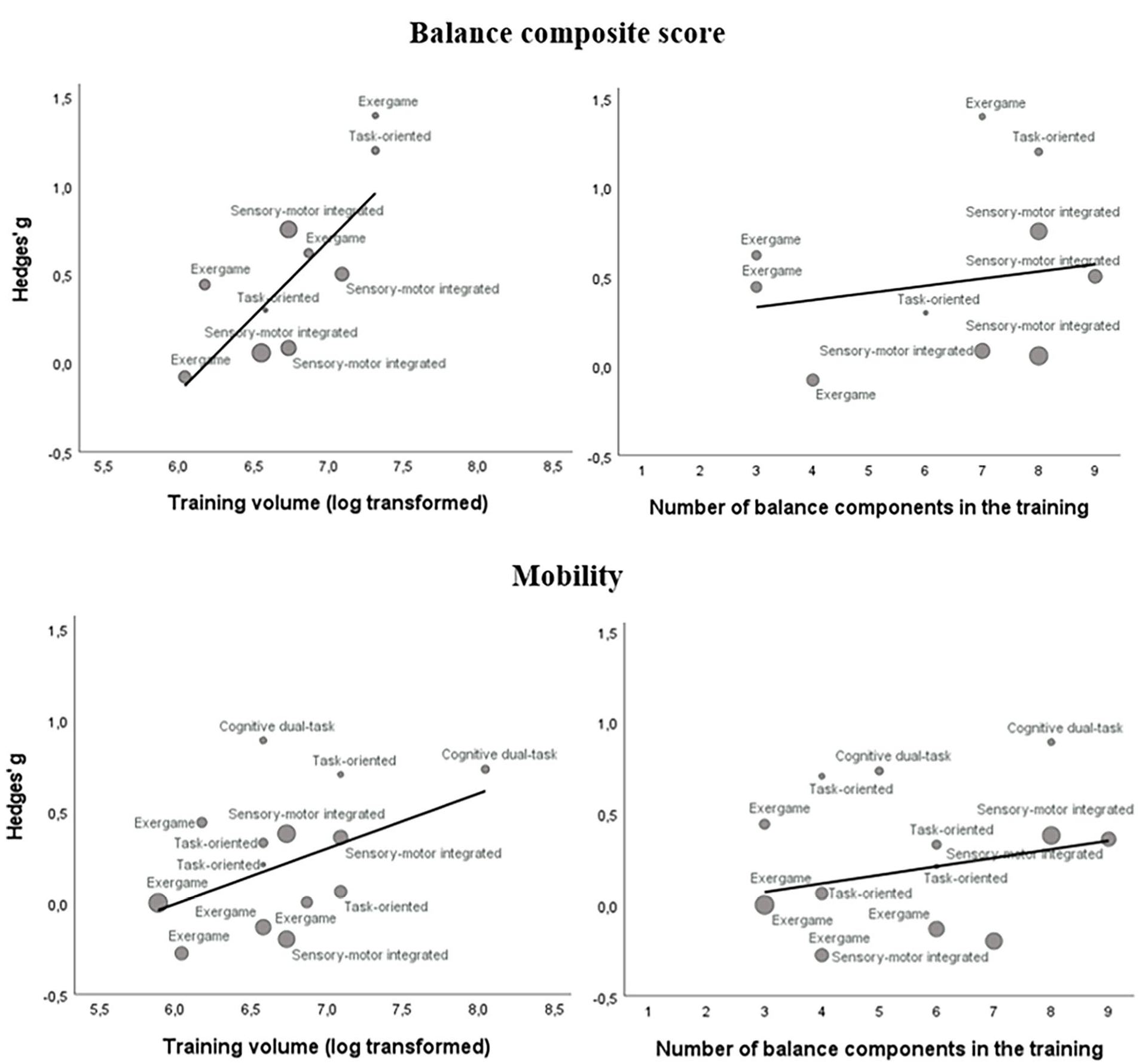
Bubble plots on training volume (log transformed) and number of balance components in the training of all included studies labeled with training types (cognitive dual-task, sensory-motor integrated, task-oriented, and exergame) and grouped within the respective outcome categories Balance composite score and Mobility. The bubble size indicates the study weight.
Publication Bias
The outcome categories Balance composite score and Mobility showed symmetric distribution in Funnel plots, indicating no publication bias (Supplemental Material).
Discussion
This systematic review and meta-analysis evaluated the effect of diverse balance training interventions on balance and gait outcomes and the association between intervention complexity and exercise effect in PwMS. Balance training interventions displayed small to large ES when evaluated with balance composite scores and mobility tests. In contrast, effects of balance training on gait speed and stepping, that are considered less complex outcomes, showed no effects. Training volume was significantly associated with training effect, irrespective of training type. Contrary to our expectations, intervention complexity derived from the number of balance components included in the training did not emerge as a significant predictor. Notably, interventions employing a task-oriented training approach tended to yield the most favorable outcomes.
In the present review, balance training was constrained to interventions that in more than 50% of the session time directly target balance, with exclusion of interventions like resistance training,53,54 aquatic exercise,55,56 and aerobic training. 57 Compared to previous reviews with broader criteria regarding types of interventions,25,58 this review included studies with a primary focus on balance. However, various kinds of training can be argued to impact neural pathways associated with postural balance 25 and therefore likely capable of enhancing balance. This makes investigation of exposures that particularly impacts balance difficult.
Similarly to the association between intensity and physiologic gains in resistance and aerobic training, it is expected that intensity also matters in balance training. However, in the absence of an expression of intensity based on the relative level of challenge, the complexity of the applied interventions (based on the number of balance components included in the training) was proposed as a proxy for intensity in our previous review. 20 It was hypothesized that interventions with a higher level of complexity would have a larger effect on balance compared to interventions with a lower level. This hypothesis was not confirmed in any outcome category and may be explained by an uncertainty of how challenging the respective balance interventions were relative to the participants capacity.
The categorization of training types was derived from the descriptions of interventions in the studies included. Of note, it is uncertain whether the authors of the included studies would concur with the categorization applied in present review and/or if the applied categories accurately capture the actual intervention content. Despite this uncertainty, the meta-analysis results suggest a more pronounced effect from task-oriented training compared to exergame and sensory-motor integration training, when assessed by composite scores (ES = 0.76 [95% CI = –0.13 to 1.64]) and mobility tests (ES = 0.29 [95% CI = –0.09 to 0.68]). This observation aligns with existing recommendations stating the importance of specificity in training. 59
Furthermore, while an intervention may target a multitude of balance components, it may not be perceived as more challenging. If intensity in balance training is compared to intensity in aerobic or resistance training, achieving large effects often demand near-maximal loading, this would translate into a high level of challenge in balance training.
In contrast to the proposed intensity measure that considered intervention content, the quantity of training sessions was associated with ES measured by a balance composite score or a mobility test, irrespective of the training type. This result is in line with the review by Corrini et al, 25 which reported a significant association between effect and session time and a near-significant association with total training volume. In support, a review by Gunn et al 58 demonstrated an association between the effect of balance training and exercise volume (minutes/week). Associations in these reviews are, however, derived from studies with a broader definition of balance training.
Despite the attempt to detect characteristics, such as intensity, of balance training interventions that were associated with effect, this review did not succeed in doing so. Due to confusion related to the reporting of intensity in balance training, the authors of this review encourage further discussion on how intensity is best defined and implemented in future balance training studies.
Meta analysis on subgroup level showed a moderate to large ES for balance training delivered as either exergaming (ES = 0.55 [95% CI = –0.03 to 1.12]), sensory-motor integrated training (ES = 0.33 [95% CI = –0.02 to 0.69]), or task-oriented training (ES = 0.76 [95% CI = –0.13 to 1.64]), when evaluated with a balance composite score. These subgroup results were not significant but tended to be. The outcome category balance composite score was derived from Bergs Balance Scale in 7 studies (8 interventions),30,31,33,34,43,44,51 and from the Mini-BESTest 60 in 2 studies.47,50 The Berg Balance Scale assesses mainly the ability to sustain static position under escalating level of difficulties but does not include gait components, balance reactions, or dual-tasking. Such absence of an ambulation component may explain the somewhat uniform effects observed across training types despite content diversity in the interventions. Based on this, measurements that include ambulation components are recommended.
When the subgroup effect of different training types was measured by a mobility outcome, where 13 out of 14 interventions utilized the Timed Up & Go test, exergame failed to demonstrate an effect, while training with a more functional approach exhibited ESs ranging from 0.19 in sensory-motor integrated training to 0.81 in cognitive dual-task training. The result in the present review likely reflects the importance of task-specificity when designing training, as stationary training does not show an effect on outcome measures that capture balance while moving around. 59 However, it’s important to note that these results are derived from a limited number of studies within each subgroup, with only the effects from cognitive dual-task training32,46 reaching statistical significance.
When assessing the effect of balance training on gait speed, all training types yielded negligible and insignificant results. This might be explained by the hypothesis that balance training enhances adaptive and reactive strategies by controlling subtle yet precise movement. Improvement of balance may not significantly manifest in outcomes assessing habitual movement patterns prioritizing speed and force over adaptation and precision. Moreover, balance exercises may not impose sufficient loads on peripheral structures to impact the prerequisites for achieving high gait speed.
The most prominent finding from the risk-of-bias assessment was that only 2 studies (11%) reported activity monitoring in the control groups.35,46 This introduces the risk of making false conclusions on causal effect of the interventions as the activity type and level in the control groups are unknown. Uncertainty of how balance is impacted by different types of training affecting pathways associated with balance makes reporting of activity in the compared groups essential in future studies.
Clinical and Research Implications
The meta-regression results from the present review align with a prior review 25 recommending interventions with high training volume to ensure a sufficient stimulus for achieving training effect. Our results recommend the use of outcome measures encompassing multiple balance components evaluating adaptive, reactive, and ambulation properties, such as the Mini-BESTest 61 to detect effect on balance performance in general and not just specifically for PwMS. Moreover, gait tests only assessing maximal walking speed (eg, 25-Foot Walk Test) may not capture potential improvements related to balance that would be captured by more complex gait outcomes (eg, Six Spot Step Test). Inconsistent and insufficient reporting of both intervention content and applied progression model, poses a challenge to comparability, when attempting to identify the key elements of balance training. Furthermore, a persistent absence of standardized methods applied to measure and report intensity and quality in balance training hinders the collective understanding and development of balance training interventions. Consequently, specific contributions of factors such as difficulty level, type of sensory stimuli, and cognitive processing requirements to the enhancement of functional balance remain unclear. Future balance training research in PwMS should therefore provide detailed descriptions of the applied interventions to advance the field.
The recognized knowledge gap regarding the effects of balance training and its association to dose, intensity, and training type is not restricted to balance training in PwMS, but is generalizable to various patient groups. However, since the effects of balance training partly might be explained by cognitive adaptation and learning, the cause of balance impairment in different patient groups may restrict the generalizability of effects.
Strengths and Limitations
This review included 18 studies, representing 4 different balance training types, and involving more than 900 PwMS. Further, this is the first meta-analysis making the ambitious attempt to apply a definition based on a minimum of balance training content that specifically focuses on improving balance. In addition, this review defined intensity in balance training without confusing this with training volume parameters, that is, duration, frequency, and session time. However, a limitation is that certain training types only applied a few studies (ie, cognitive dual-task training was only applied in 2 studies32,46). The limited number of studies prohibited the assessment of additional covariates in the meta-regression. Consequently, it was not possible to determine whether the observed effect across all studies and within the respective training types depended on intervention duration and/or disability status.
The meta-analysis used ES that is a dimensionless measure of effect allowing pooling across outcome measures. However, the size of an effect relies on ratio between effect and sample distribution which complicates interpretation. The small ES found, might reveal a trend toward an effect, but it is hard to translate or make a useful interpretation of the results to outcome measures and functional tests used in clinical contexts.
Due to notable discrepancies between the calculated effects in our primary analysis and those reported by the individual studies, a supplementary meta-analysis was performed, using post-test values adjusted for baseline values (see Supplemental Material). Of note, in both methodological approaches, the analysis found the composite scores to be superior in detecting a change in balance control and that measures of mobility that evaluate more elements than speed alone are recommendable. These findings therefore add support to the validity of the main analyses.
Conclusions
In this review, balance training was categorized into the training types: cognitive dual-task; exergame; sensory-motor integrated; and task-oriented balance training. The training types demonstrated comparable beneficial effects on balance when measured by multi-dimensional balance composite scores and mobility tests but not in terms of gait speed.
Intervention complexity determined from the number of balance components challenged in the training was not associated with an effect on balance. However, dynamic and cognitively challenging balance training tended to improve complex mobility, in contrast to exergame training. Interventions employing a task-oriented training approach tended to yield the most favorable outcomes.
Training volume across training types was associated with effect on balance. However, a definition of intensity in balance training is needed for evaluation of its impact on the effect of balance interventions.
Supplemental Material
sj-docx-1-nnr-10.1177_15459683241273402 – Supplemental material for Effects of Balance Exercise Interventions on Balance-Related Performance in People With Multiple Sclerosis: A Systematic Review and a Meta-Analysis of Randomized Controlled Trials
Supplemental material, sj-docx-1-nnr-10.1177_15459683241273402 for Effects of Balance Exercise Interventions on Balance-Related Performance in People With Multiple Sclerosis: A Systematic Review and a Meta-Analysis of Randomized Controlled Trials by Andreas Wallin, Sverker Johansson, John Brincks, Ulrik Dalgas, Erika Franzén and Jacob Callesen in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
We acknowledge the great work of librarians Emma-Lotta Säätelä and Sabina Gillsund, Karolinska Institutet University Library, in structuring and documenting the search strategies.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
Author Contributions
Andreas Wallin: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Project administration; Visualization; Writing—original draft. Sverker Johansson: Conceptualization; Methodology; Writing—review & editing. John Brincks: Conceptualization; Methodology; Writing—review & editing. Ulrik Dalgas: Conceptualization; Methodology; Writing—review & editing. Erika Franzen: Conceptualization; Methodology; Writing—review & editing. Jacob Callesen: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Project administration; Supervision; Writing—original draft.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ulrik Dalgas has received research support, travel grants, and/or teaching honoraria from Biogen Idec, Bristol Myers Squibb, Merck Serono, Novartis, Bayer Schering, and Sanofi Aventis, as well as honoraria from serving on the scientific advisory boards of Biogen Idec and Genzyme. All other authors declare no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.