
Abstract
Background
Comparative therapeutic benefits of combined and single neurostimulation therapies including neuromuscular electrical stimulation (NMES), pharyngeal electrical stimulation (PES), repetitive transcranial magnetic stimulation (rTMS), transcranial direct current stimulation (tDCS), and traditional dysphagia therapy (TDT) remain unknown in post-stroke dysphagia (PSD) rehabilitation. Therefore, we performed the first network meta-analysis (NMA) to determine comparative effectiveness of combined and single neurostimulation and traditional dysphagia therapies for PSD.
Methods
A frequentist NMA model was performed with therapy effect sizes presented as standardized mean differences (SMD) and corresponding 95% confidence interval (95% CI) for therapy comparisons while netrank function ranked the therapies in R-Software. Meta-regression models for study characteristics were analyzed using Bayesian NMA Model.
Results
Overall, 50 randomized controlled studies with 2250 participants were included. NMES + TDT 3.82 (95% CI, 1.62-6.01), tDCS + TDT 3.34 (95% CI, 1.09-5.59), rTMS + TDT 3.32 (95% CI, 1.18-5.47), NMES 2.69 (95% CI, 0.44-4.93), and TDT 2.27 (95% CI, 0.12-4.41) demonstrated very large effect in improving swallowing function. NMES + TDT −0.50 (95% CI, −0.68 to −0.32, rTMS + TDT −0.44 (95% CI, −0.67 to −0.21), TDT −0.28 (95% CI, −0.46 to −0.10), and NMES −0.19 (95% CI, −0.34 to −0.04) demonstrated medium to small effect in reducing pharyngeal transit time (PTT). rTMS −0.51 (95% CI, −0.93 to −0.08) demonstrated medium effect in reducing oral transit time (OTT). No significant therapy comparison differences were found for reducing aspiration/penetration. The highest ranked therapy was NMES + TDT for better swallowing function and reduction of PTT, rTMS for reduction of OTT, and tDCS + TDT for reduction of aspiration/penetration. Therapeutic effects of the therapies were moderated by frequency, sessions, and duration.
Conclusion
Combined therapies including NMES + TDT, tDCS + TDT, and rTMS + TDT demonstrate better therapeutic effect for improved swallowing function and reduction of PTT, OTT, and aspiration/penetration for PSD.
Keywords
Introduction
Stroke is the leading cause of disability and the second cause of deaths worldwide. 1 Post-stroke complications including motor impairment, dysphagia, and eventually death continue to affect this population.2,3 Various rehabilitative strategies including traditional dysphagia therapy (TDT), neuromuscular electrical stimulation (NMES), pharyngeal electrical stimulation (PES), repetitive transcranial magnetic stimulation (rTMS), and transcranial direct current stimulation (tDCS) are currently used in the management of post-stroke dysphagia (PSD) to aid in effective swallowing, prevent aspiration/penetration, and improve quality of life.4,5 Various traditional dysphagia therapies were used in the current study including behavioral techniques utilizing oral and pharyngeal swallowing exercises, compensatory techniques utilizing posture adjustment and medications, and thermal tactile stimulation.4,5 Thus, identification of the most effective evidence-based therapies is crucial for better and improved dysphagia-related outcomes for PSD.
Current research findings reveal an increase in studies using combined neurostimulation and traditional therapies including NMES + TDT, tDCS + TDT, rTMS + TDT to complement single therapies including NMES, PES, tDCS, rTMS, and TDT in PSD rehabilitation.6,7 In addition, pairwise meta-analyses have revealed the effectiveness of combined and single neurostimulation and traditional dysphagia therapies including NMES + TDT, tDCS + TDT, rTMS + TDT, NMES, PES, tDCS, and rTMS in improving PSD when compared to TDT and sham therapy.6,7 Furthermore, a previous network meta-analysis (NMA) demonstrated that single non-invasive neurostimulation therapies including rTMS (SMD: 1.02 [95% confidence interval [CI], 0.61-1.43]), NMES (SMD: 0.82 [95% CI, 0.42-1.23]), and tDCS (SMD: 0.61 [95% CI, 0.09-1.13]) were effective in improving swallowing function in acute and sub-acute stroke patients while PES was not effective. 8 The use of combined neurostimulation and traditional dysphagia therapies may offer different functions working on the brain and oropharyngeal muscles that provide better cortical re-organization and improved swallowing musculature following a stroke than single therapies. An NMA is a statistical method that compares multiple treatments concurrently in a single analysis by combining direct and indirect evidence within a network of randomized controlled trials as compared to conventional pairwise meta-analyses. 9 Moreover, the treatments in an NMA can also be ranked in order of their effectiveness from the most effective to the least effective treatment ensuring better decision-making for clinicians. However, lack of evidence on the beneficial effects of combined and single neurostimulation and traditional dysphagia therapies demonstrates a gap that needs considerable attention, which was not addressed in the previous NMA. As such, the comparative benefits of combined or single neurostimulation and traditional dysphagia therapies remain unclear and unknown in the current stroke research and the management of PSD. Thus, an NMA on the comparative effectiveness of combined and single neurostimulation and traditional dysphagia therapies would provide comprehensive and useful evidence for clinical decision-making in PSD rehabilitation and further extend evidence on the current research findings and previous NMA.
The use of neurostimulation and traditional therapies is crucial in PSD rehabilitation ensuring effective and safe swallowing and improved survival for patients. Therefore, the aim of the current NMA of randomized controlled studies was to determine the comparative therapeutic effectiveness of combined and single neurostimulation and traditional dysphagia therapies including NMES + TDT, tDCS + TDT, rTMS + TDT, NMES, rTMS, PES, TDT, and sham therapy for PSD.
Methods
Search Strategy
The study protocol was registered with PROSPERO: CRD42021175299 and the Preferred Reporting Items for Systematic reviews and Meta-Analyses–Network Meta-analyses (PRISMA-NMA) statement was followed. 10 A comprehensive literature search was performed in Embase, PubMed, Ovid-Medline, CINAHL, Cochrane Library, Web of Science, and reference lists of published systematic reviews and meta-analyses were reviewed and identified potential studies were searched in Google with an initial search in March 2021 and follow-up search in July 2021 and August 2022. The following keywords were used with a detailed search strategy in the supplemental material (Supplemental Appendix 2): (Dysphagia OR swallowing disorder OR deglutition disorder OR oropharyngeal dysphagia) AND (traditional dysphagia therapy OR TDT OR neuromuscular electrical stimulation OR NMES OR pharyngeal electrical stimulation OR PES OR repetitive transcranial magnetic stimulation OR rTMS OR transcranial direct current stimulation OR tDCS AND (stroke OR cerebrovascular accident OR CVA). Corresponding authors were sent emails when there was missing data in the published studies to ensure that all potential studies were included.
Study Selection
The inclusion criteria were as follows: (1) adults with PSD ≥ 18 years old, (2) studies assessing effectiveness of NMES + TDT, tDCS + TDT, rTMS + TDT, NMES, rTMS, PES, TDT, and sham therapy, (3) randomized controlled studies, and (4) no language restrictions. The exclusion criteria were as follows: (1) irrelevant study design, (2) studies which combined stroke with other diseases, (3) duplicate studies, (4) non-relevant population studies, (5) systematic review or meta-analysis studies, (6) inappropriate data format studies including graphical presentations of longitudinal data, odds ratios, percentages, mean differences, and F statistics for repeated measures, and (7) studies that compared similar interventions including types of TDT or neurostimulation therapy, similar TDT or neurostimulation therapy on different parts or sites of swallowing musculature or brain (Figure 1).
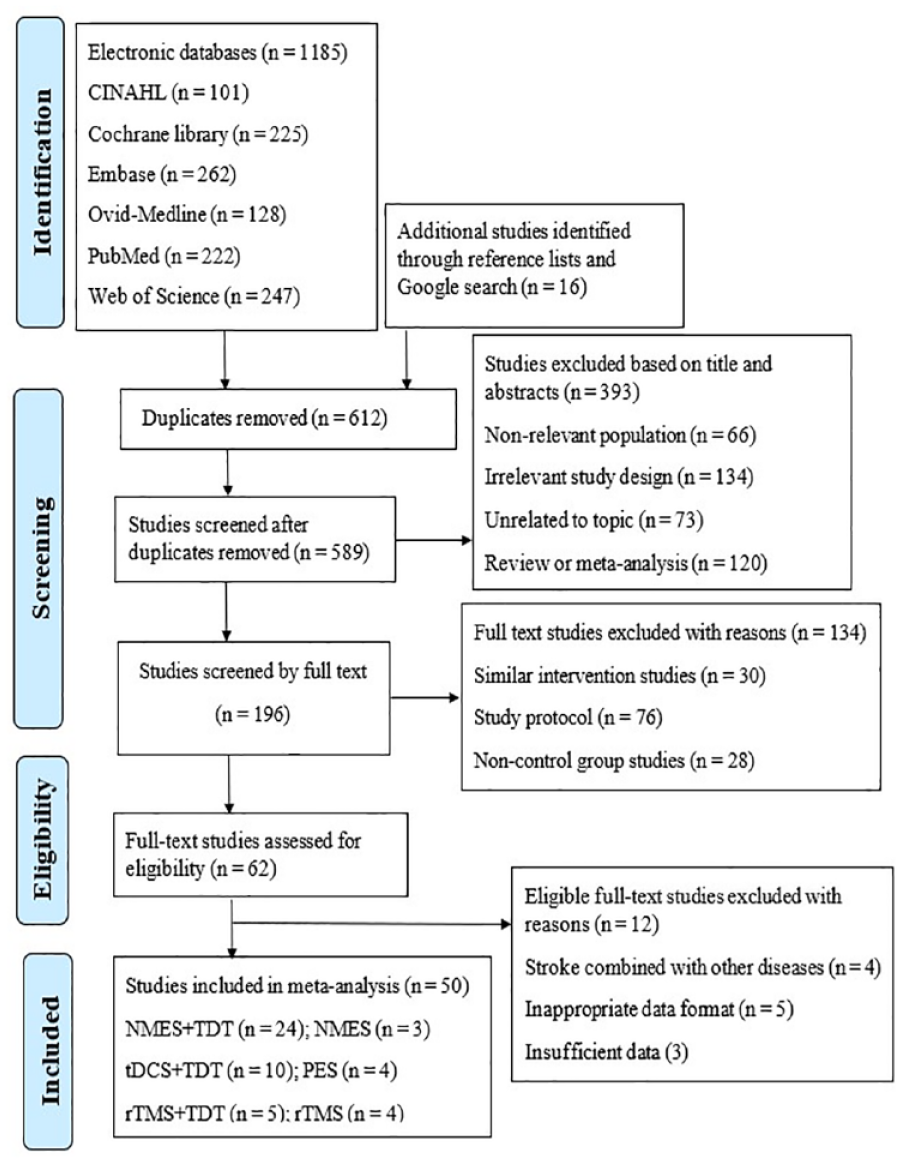
PRISMA flow chart for study selection.
Data Extraction and Study Outcomes
Two independent reviewers extracted the following data; (1) author and year of publication, (2) intervention comparison, (3) age, (4) gender, (5) type and phase of stroke, (6) sample size, (7) protocol of Sham therapy, TDT, NMES, PES, rTMS, rTMS + TDT, NMES + TDT, and tDCS + TDT, (8) study outcomes, and (9) follow-up time (Supplemental Appendix 2).
The primary outcome was swallowing function measured using instrumental objective assessment tools including Video-fluoroscopic Swallowing Study, 11 Functional Dysphagia Scale (FDS), 12 Video-fluoroscopic Dysphagia Scale (VDS) 13 and non-instrumental subjective assessment tools including Functional Oral Intake Scale, 14 Dysphagia Outcome and Severity Scale, 15 Dysphagia Severity Rating Scale, 16 Gugging Swallowing Screen, 17 Swallowing Ability and Function Evaluation, 18 Swallowing Function score, 19 and Mann Assessment of Swallowing Ability. 20 The secondary outcomes were (1) pharyngeal transit time (PTT) measured by VDS and FDS, (2) risk of aspiration/penetration measured by Penetration Aspiration Scale (PAS), 21 VDS, and FDS, and (3) oral transit time (OTT) measured by VDS and FDS (Supplemental Appendix 2).
Quality Assessment of Included Studies
Two independent reviewers assessed the risk of bias of the included randomized controlled studies using the Cochrane Handbook for Systematic Reviews of Interventions Version 2.0. 22 The domains for the risk of bias include (1) the randomization process, (2) deviations from intended interventions, (3) missing outcome data, (4) measurement of the outcome, and (5) selection of the reported results. We rated each domain as low, some concerns or high risk of bias with the overall quality of each study assessed by checking and summing the five domains of risk of bias (Supplemental Appendix 21). Discrepancies among the reviewers were resolved through discussions with a third expert reviewer.
Statistical Synthesis and Analysis
Multivariate meta-analysis with the netmeta version 2.7-0 and GEMTC version 1.0-1 packages was performed in R-Statistical Software version 4.1.2 using post-treatment mean and standard deviation (SD) for the experimental and control groups.23 -26 The pooled effect sizes were presented as standardized mean differences (SMDs) for continuous outcomes including swallowing function, PTT, aspiration/penetration, and OTT for each pairwise intervention comparison.24 -26 Studies that presented median and inter-quartile range for the experimental and control groups, a formula developed by Wan et al 27 and Hozo et al 28 was used to calculate mean and SD.27,28 The frequentist NMA model was employed to determine relative effectiveness and ranking of combined and single rehabilitative therapies including NMES + TDT, tDCS + TDT, rTMS + TDT, NMES, rTMS, PES, TDT compared to sham therapy.24,25 The pooled treatment effect sizes of the therapy comparisons were generated using post-treatment mean and SD scores from the raw data to estimate direct, indirect, and network evidence.24,25 The generalized DerSimmonian-Laird method was used to estimate the τ2, which was used as the measure of heterogeneity for all the outcomes.24,25 We generated network maps (Figures 2 and 3) and presented SMDs of credible intervals and corresponding 95% CI for each pairwise intervention comparisons. For effect size interpretation, SMDs were interpreted as small: 0.20, moderate: 0.50, large: >0.80, and very large: >1.3.25,29 The transitivity assumption was followed by including (1) participants with dysphagia secondary to stroke, (2) ischemic and hemorrhagic types of strokes, (3) acute, sub-acute, and chronic phases of stroke, (4) interventions including neurostimulation therapies (NMES, PES, rTMS, and tDCS) and TDT, and (5) randomized controlled studies. The full design-by-treatment interaction random-effects model and the network node-splitting methods assessed the global and local consistency and inconsistency, respectively. 30 The comparison-adjusted funnel plots and Egger’s regression method were used to assess publication bias. 25
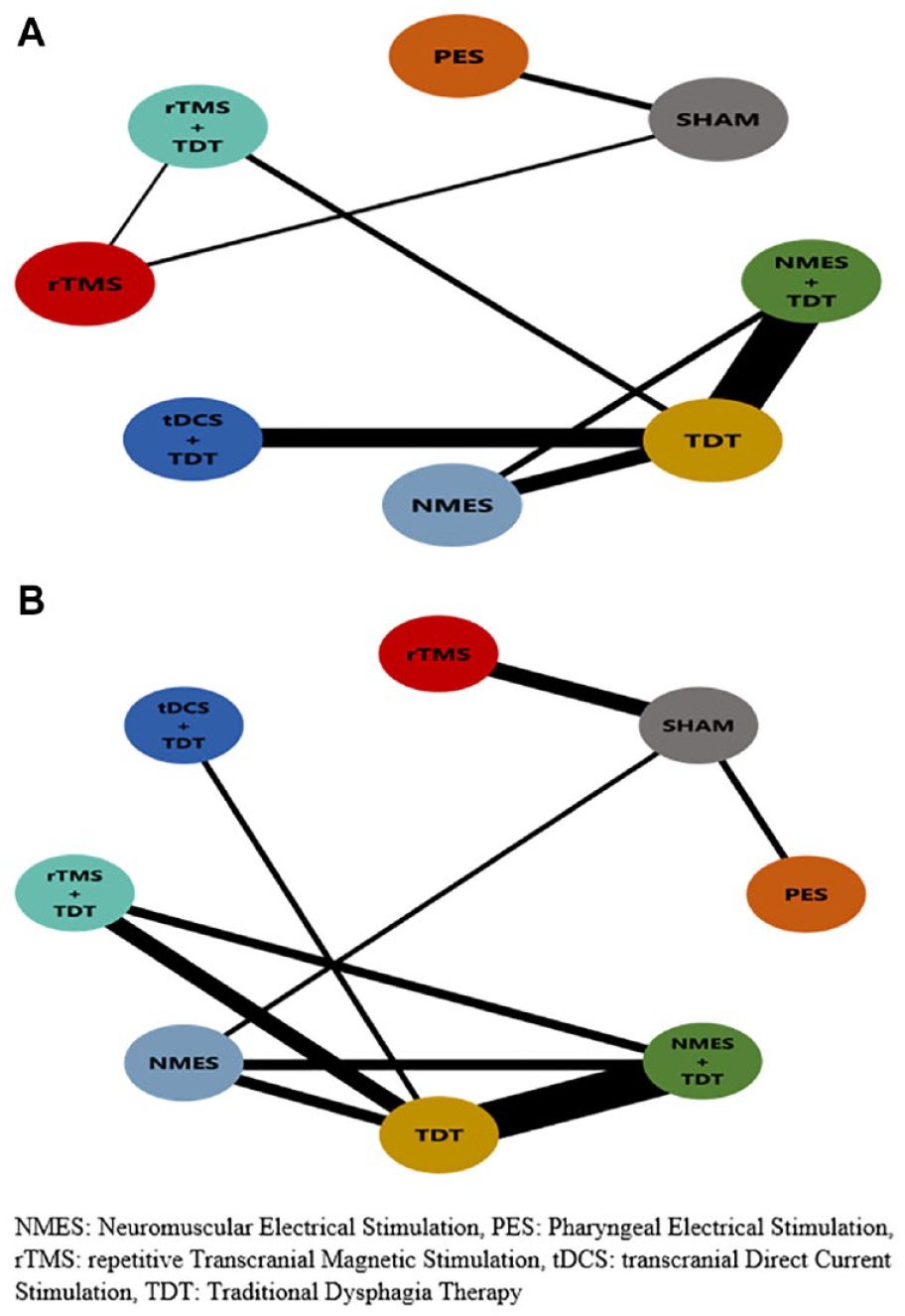
Network maps for swallowing function and pharyngeal transit time.
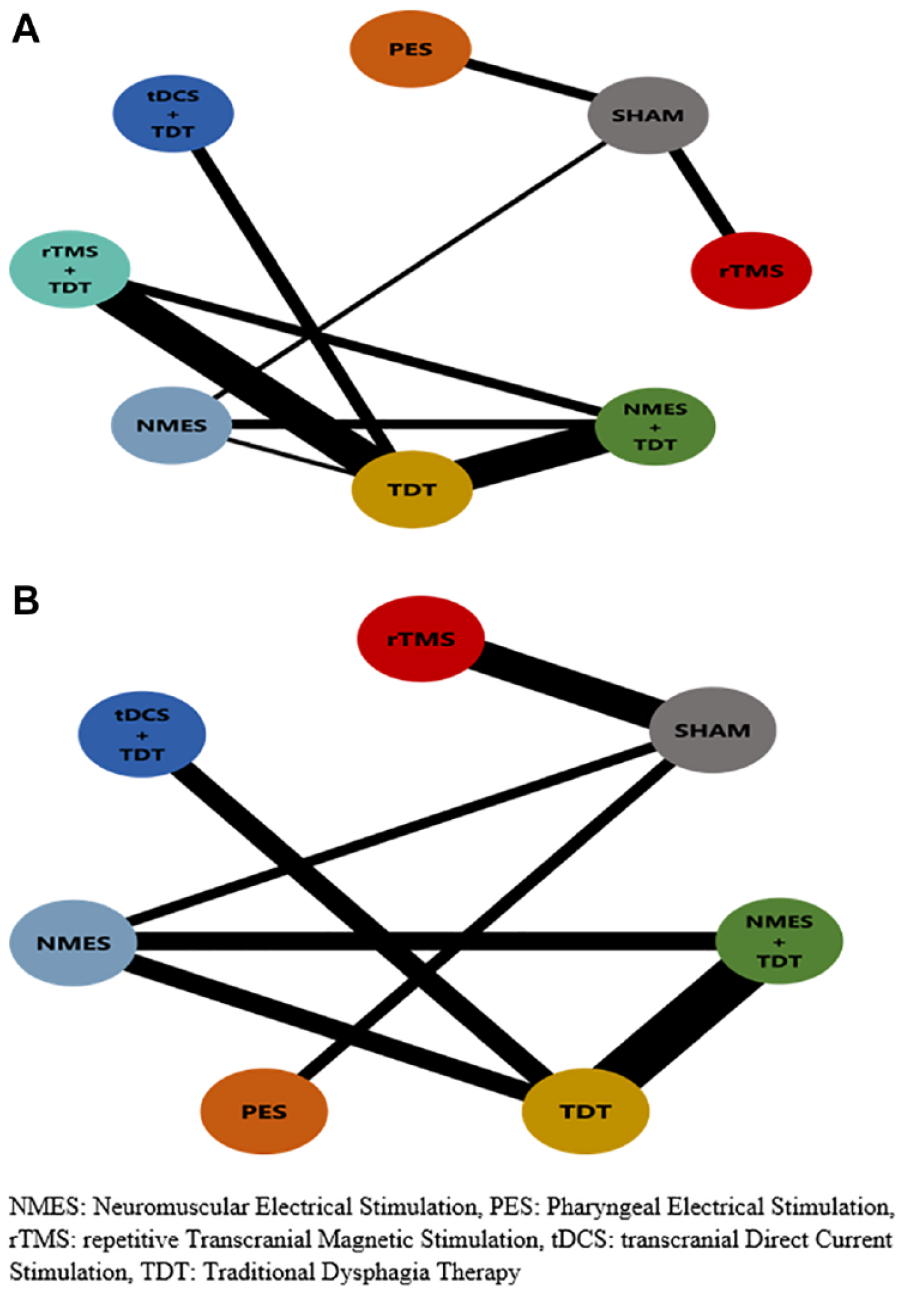
Network maps for aspiration/penetration and oral transit time.
Treatment Ranking
Treatment ranking among NMES + TDT, tDCS + TDT, rTMS + TDT, NMES, rTMS, PES, TDT compared to sham therapy was estimated using the netrank function. 31 The netrank P-scores, which range between 0 and 1, demonstrate that neurostimulation and traditional therapies with higher P-score numbers indicate the probability of being ranked as the most effective intervention. The interventions were further categorized: (1) best quartile: ≥0.75-1.00, (2) second quartile: ≥0.50-<0.75, (3) third quartile: ≥0.25-<0.50, and (4) least quartile: 0-<0.25.
Moderator Analysis
A Bayesian hierarchical model using the mixed treatment comparison (MTC) model was used for moderator analysis as the frequentist method cannot perform this analysis.23,25 Thus, meta-regression models assessed the influence of participants’ characteristics including (1) age, (2) gender, (3) type of stroke, (4) phase of stroke, and (5) sample size and interventional characteristics including (1) frequency per week, (2) total number of sessions, and (3) total duration the intervention on our generated evidence. A 10-point change in the deviance information criterion (DIC) between the adjusted NMA model from the initial unadjusted NMA model indicated significant moderator effect of the given study covariate.
Confidence in Network Meta-Analysis
The confidence rating of the intervention comparisons in the current NMA was assessed using the Confidence in Network Meta-Analysis (CINeMA) guideline 32 consisting six domains including within-study bias, reporting bias, indirectness, imprecision, heterogeneity, and coherence. The within-study bias is the percentage of contribution matrix of each study based on the individual study risk of bias and is rated as low, moderate, and high risk of bias. Reporting bias results are assessed based on the suppression of negative study findings, publication bias, time-lag bias, and omission of unfavorable study results. Indirectness is the representativeness of the study settings, populations, interventions, and outcomes among the included studies. Imprecision represents clinical important difference of the therapy comparison based on the treatment effect and the 95% CI. Heterogeneity measured by the τ2 is the difference of the genuine variations between studies. Incoherence refers to statistical intransitivity when the direct and indirect evidence are not in agreement and coherent. Reporting bias, indirectness, imprecision, heterogeneity, and incoherence are rated as no, some, and major concerns. The overall CINeMA confidence rating for each therapy comparison is denoted as very low, low, moderate, and high.
Sensitivity Analysis
Sensitivity analysis was performed to assess the robustness of the study findings based on the risk of bias.24,25 High risk of bias studies were excluded for each outcome and the analysis was performed again. The results from the sensitivity analysis using the P-score were assessed for consistency by comparing with the results of the P-score of the initial analysis.
Results
Demographic Characteristics
Overall, 50 randomized controlled studies (Supplemental Appendix 22) published between 2006 and 2022 were identified and included from 1201 studies that were retrieved from the electronic databases, the Google search and reference lists (Figure 1). In all, we identified 2250 participants with the sample size ranging from eight to 162 in the included studies with 1368 participants being males and 894 being females. The mean age in the experimental groups ranged from 55.3 to 87 years and ranged from 55.6 to 81 years in the control groups. The primary diagnosis of the participants was stroke in acute, sub-acute, and chronic phases. Regarding type of stroke, 34 studies comprised of both ischemic and hemorrhagic types while 16 studies comprised of ischemic type (Supplemental Appendix 2).
Interventional Characteristics
The following dysphagia therapies were identified including NMES + TDT, tDCS + TDT, rTMS + TDT, rTMS, PES, NMES, TDT, and sham therapy. The protocol of combined neurostimulation and traditional dysphagia therapies including NMES + TDT, tDCS + TDT, and rTMS + TDT included frequency of the intervention per week ranging from 3 to 10 times, the number of sessions ranged from 6 to 40 sessions, and the total number of hours ranged from 2.6 to 44 hours. The protocol of single neurostimulation and traditional dysphagia therapies including rTMS, PES, NMES, TDT, and sham therapy included frequency of the intervention per week ranging from one to 5 times, the total duration of the intervention per day ranged from 10 to 30 minutes, the number of sessions ranged from one to 20 sessions, and the total number of hours ranged from 20 minutes to 10 hours. The study duration in the current NMA ranged from one week to eight weeks for post-treatment with no long-term follow-up (Supplemental Appendix 2).
Assessment of NMA Assumptions
The results of the full design-by-treatment interaction random-effects model showed that swallowing function (P = .125), OTT (P = .253), aspiration/penetration (P = .470) revealed no inconsistency while PTT (P < .04) showed some inconsistency. Similarly, the results of the network node splitting models for swallowing function, aspiration/penetration and OTT revealed no inconsistency while PTT showed some inconsistency between direct and indirect estimates (Supplemental Appendices 7-10).
Comparative Effectiveness of Combined and Single Neurostimulation and Traditional Dysphagia Therapies on Primary Outcome: Swallowing Function
NMES + TDT 3.82 (95% CI, 1.62-6.01), tDCS + TDT 3.34 (95% CI, 1.09-5.59), rTMS + TDT 3.32 (95% CI, 1.18-5.47), NMES 2.69 (95% CI, 0.44-4.93), and TDT 2.27 (95% CI, 0.12-4.41) demonstrated very large effect for better swallowing function compared to sham therapy. There were no therapy differences for rTMS 0.86 (95% CI, −0.71 to 2.42) and PES 0.53 (95% CI, −0.71 to 1.78) compared to sham therapy (Table 1; Supplemental Appendix 3). There was no evidence of publication bias for swallowing function (P = .818) (Supplemental Appendix 11).
Network Evidence Estimates for Swallowing Function (Upper Triangle) and Pharyngeal Transit Time (Lower Triangle).
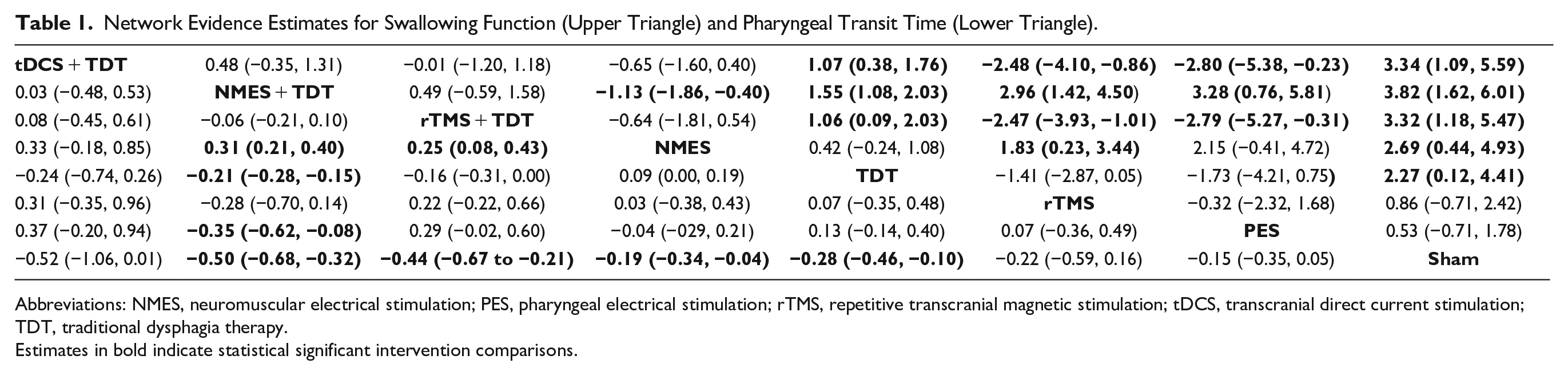
Abbreviations: NMES, neuromuscular electrical stimulation; PES, pharyngeal electrical stimulation; rTMS, repetitive transcranial magnetic stimulation; tDCS, transcranial direct current stimulation; TDT, traditional dysphagia therapy.
Estimates in bold indicate statistical significant intervention comparisons.
The results of the netrank function scores revealed that NMES + TDT (0.95), tDCS + TDT (0.79), and rTMS + TDT (0.79) were the best, the second was NMES (0.58), the third was TDT (0.43), the least were rTMS (0.22) and PES (0.19) for swallowing function (Supplemental Appendix 3).
Comparative Effectiveness of Combined and Single Neurostimulation and Traditional Dysphagia Therapies on Secondary Outcome: PTT
NMES + TDT −0.50 (95% CI, −0.68 to −0.32), rTMS + TDT −0.44 (95% CI, −0.67 to −0.21), TDT −0.28 (95% CI, −0.46 to −0.10), and NMES −0.19 (95% CI, −0.34 to −0.04) demonstrated medium to small effect in reducing PTT compared to sham therapy. There were no therapy differences for tDCS + TDT −0.52 (95% CI, −1.06 to 0.01), rTMS −0.22 (95% CI, −0.59 to 0.16), and PES −0.15 (95% CI, −0.35 to 0.05) (Table 1; Supplemental Appendix 4). There was no evidence of publication bias for PTT (P = .176) (Supplemental Appendix 11).
The results of the netrank function scores revealed that NMES + TDT (0.87), tDCS + TDT (0.80), and rTMS + TDT (0.77) were the best, the second was TDT (0.52), and the third were rTMS (0.41), NMES (0.31), and PES (0.28) for PTT (Supplemental Appendix 4).
Comparative Effectiveness of Combined and Single Neurostimulation and Traditional Dysphagia Therapies on Secondary Outcome: Aspiration/Penetration
rTMS + TDT −2.65 (95% CI, −7.68 to 2.38), tDCS + TDT −2.15 (95% CI, −7.35 to 3.05), NMES + TDT −2.11 (95% CI, −7.04 to 2.81), TDT −1.41 (95% CI, −6.11 to 3.31), NMES −1.40 (95% CI, −6.37 to 3.55), rTMS −0.79 (95% CI, −2.67 to 1.08), and PES −0.20 (95% CI, −1.90 to 1.49) revealed no therapy differences compared to sham therapy for reducing aspiration/penetration (Table 2; Supplemental Appendix 5). There was some evidence of publication bias for aspiration/penetration (P = .009) (Supplemental Appendix 11).
Network Evidence Estimates for Aspiration/Penetration (Upper Triangle) and Oral Transit Time (Lower Triangle).
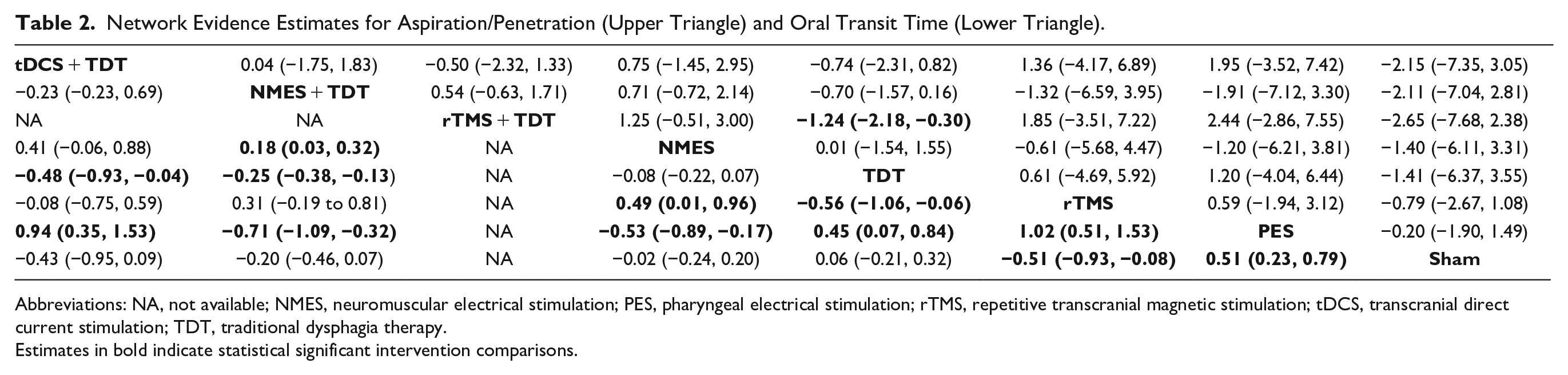
Abbreviations: NA, not available; NMES, neuromuscular electrical stimulation; PES, pharyngeal electrical stimulation; rTMS, repetitive transcranial magnetic stimulation; tDCS, transcranial direct current stimulation; TDT, traditional dysphagia therapy.
Estimates in bold indicate statistical significant intervention comparisons.
The results of the netrank function scores revealed that rTMS + TDT (0.84) was the best, the second were NMES + TDT (0.67) and tDCS + TDT (0.66), and the third were rTMS (0.45), NMES (0.43), TDT (0.39), and PES (0.32) for aspiration/penetration (Supplemental Appendix 5).
Comparative Effectiveness of Combined and Single Neurostimulation and Traditional Dysphagia Therapies on Secondary Outcome: OTT
rTMS −0.51 (95% CI, −0.93 to −0.08) demonstrated medium effect in reducing OTT compared to sham therapy while sham therapy was better than PES 0.51 (95% CI, 0.23-0.79). There were no therapy differences for tDCS + TDT −0.43 (95% CI, −0.95 to 0.09), NMES + TDT −0.20 (95% CI, −1.46 to 0.07), NMES −0.02 (95% CI, −0.24 to 0.20), and TDT 0.06 (95% CI, −0.21 to 0.32) (Table 2; Supplemental Appendix 6). There was no evidence of publication bias for OTT (P = .324) (Supplemental Appendix 11).
The results of the netrank function scores revealed that rTMS (0.91) and tDCS + TDT (0.86) were the best, the second was NMES + TDT (0.70), the third were NMES (0.41) and TDT (0.25), and the least was PES (0.002) for OTT (Supplemental Appendix 6).
Confidence Rating of Evidence and Sensitivity and Moderator Analyses
The confidence rating of the direct, indirect, and network evidence for swallowing function, PTT, OTT, and aspiration/penetration was determined by the CINeMA guideline. The confidence rating of the included outcomes in the current NMA ranged from very low to moderate (Supplemental Appendices 12-14).
The results of the sensitivity analysis revealed similar P-scores to the initial P-scores of the included interventions for all the outcomes (Supplemental Appendix 16). Therefore, the current NMA results would be considered as being robust.
The findings of the meta-regression demonstrated a minimal change of the DIC from the initial unadjusted model to the adjusted model of demographic and interventional characteristics (Supplemental Appendices 17-20). However, the findings revealed that frequency, number of sessions, and duration of the therapies were significant moderator variables due differences of the initial and adjusted SMDs of the therapy treatment effects. Age, gender, type of stroke, phase of stroke, and sample size were not significant moderator variables in the current NMA.
Discussion
Effectiveness of Neurostimulation and Traditional Dysphagia Therapies on Swallowing Function, PTT, OTT, and Aspiration/Penetration
To our knowledge, this is the first NMA to provide comprehensive evidence on the comparative therapeutic effectiveness of combined and single neurostimulation and traditional dysphagia therapies including NMES + TDT, tDCS + TDT, rTMS + TDT, NMES, rTMS, TDT, PES, and sham therapy in patients with PSD. The current NMA findings demonstrated that combined and single neurostimulation and traditional dysphagia therapies including NMES + TDT, tDCS + TDT, rTMS + TDT, NMES, rTMS, and TDT were effective for better swallowing function and reduction of PTT and OTT post-treatment. The results of the current NMA are consistent with results of previous pairwise meta-analyses and NMA.6,8,33 Chiang et al 8 in their NMA demonstrated that single non-invasive neurostimulation therapies including rTMS, NMES, tDCS, and PES were effective in improving swallow function for PSD immediate post-intervention. However, these findings were confounded by combination of swallowing therapies with non-invasive neurostimulation therapies and the therapeutic effects could not be attributed to the use of single non-invasive neurostimulation therapies alone. Hence, we further categorized the neurostimulation and traditional dysphagia therapies into combined and single therapies including NMES + TDT, tDCS + TDT, rTMS + TDT, NMES, rTMS, TDT, and sham therapy to provide more comprehensive evidence on the dysphagia therapies in PSD. NMES and PES stimulate peripheral nerve fibers and muscles promoting recovery of the cortical control of swallowing, tDCS and rTMS stimulate the brain increasing brain hemispheric neuronal excitability, and TDT including swallowing behavioral interventions maintains the power and tone of the swallowing musculature.34,35 It is worthwhile to note that as regards to therapy ranking, combined neurostimulation and traditional dysphagia therapies including NMES + TDT, tDCS + TDT, rTMS + TDT were mostly superior compared to single therapies.
The current NMA findings suggest that the therapeutic effects produced by combined neurostimulation and traditional dysphagia therapies promote and induce better cortical plasticity and reorganization of the central nervous system and neural activation of oropharyngeal muscles leading to better swallowing function and reduction of PTT and OTT.35,36 Additionally, the activation of oropharyngeal muscles ensures improved precision, safety, performance, and coordination of the bolus movement from the oropharyngeal phases into the esophageal phase. In the current NMA, PES alone had the lowest therapy ranking suggesting limited therapeutic effect in improving PSD complications. Compared to other combined and single therapeutic modalities, the results of the current NMA imply that the therapeutic effect induced by PES alone becomes easily out-weighted by the disabilities of the central nervous systems in patients with PSD. Thus, use of combined neurostimulation and traditional dysphagia therapies including NMES + TDT, tDCS + TDT, rTMS + TDT could be suitable therapies in the management of PSD ensuring safe transportation of the bolus through the oral, pharyngeal, and esophageal phases of the swallowing.
Regarding aspiration/penetration, incomplete laryngeal protection occurs due to decreased and blunted epiglottic movement when the bolus reaches the pharynx while vocal fold paralysis leads to impaired upper airway protection during swallow. 37 Furthermore, decreased laryngeal elevation and decreased anterior displacement of the hyoid bone results in abnormal hypolaryngeal movements causing aspiration/penetration in PSD patients. 37 Evidence from previous research findings have also revealed fluid penetration and aspiration status as important risk factors for all-cause mortality when conducting instrumental swallowing evaluations in patients with PSD. 38 Our study reported no difference in reducing aspiration/penetration among the combined and single neurostimulation and traditional dysphagia therapies possibly due to limited number of included studies for aspiration/penetration in the current NMA. Thus, more future studies are needed to address this issue and further investigation towards the mortality rate, incidence of aspiration pneumonia, and nutritional status among patients with PSD will be essential.
The goal of dysphagia rehabilitation through use of rTMS, tDCS, NMES, PES, and TDT in stroke patients is promoting brain cortical neuroplasticity ensuring effective swallowing and prevention of aspiration/penetration.33 -36 Our study findings showed that frequency, number of sessions, and duration of the combined and single neurostimulation and traditional therapies as significant moderator variables in the current NMA. A recent systematic review has revealed that frequency, duration, intensity, and repetitions of the dysphagia therapies as important dysphagia exercise dose-determining factors to ensure better dysphagia-related outcomes. 39 Currently, there are no standard guidelines on the frequency, duration, intensity, and repetitions of the dysphagia therapies which can be seen as a limitation in the PSD rehabilitation. 39 As such, future studies exploring the impact of frequency, duration, intensity, and repetitions for dysphagia therapies to established standardized optimal doses are needed to address this shortfall. Our results showed that PES had the least number of sessions, frequency, and duration among the interventions, which may also likely explain partly its inability to improve PSD complications. As such, future RCTs assessing the effectiveness of neurostimulation and traditional therapies on PSD should explore and establish standard and optimal doses that can be useful in clinical settings and assessment of dose-effects of the therapies. The current findings also suggest that combined and single neurostimulation and traditional dysphagia therapies could be used for better swallowing function and reduction of PTT, OTT, and aspiration/penetration in acute, sub-acute, and chronic phases and hemorrhagic and ischemic types of stroke. Additionally, future RCTs with detailed demographic characteristics and dose-determining factors of neurostimulation and traditional dysphagia therapies are recommended to help further determine the therapeutic effects on dysphagia severity, type, and phases of stroke and dose-effect in PSD management. Overall, the current NMA revealed that combined neurostimulation and traditional dysphagia therapies are preferable for better swallowing function and reducing PTT, OTT, and aspiration/penetration and can be useful in all phases and both types of stroke. Nevertheless, the relevance and application of these combined and single neurostimulation and traditional dysphagia therapies for PSD could be tailored to individual patients and interventional characteristics and needs in clinical practice.
Strengths and Limitations of the Study
The current NMA has notable strengths. First, the current NMA provides comprehensive evidence on the comparative effectiveness of combined and single neurostimulation and traditional dysphagia therapies from 50 included randomized controlled studies with 2250 participants. Second, we ensured that all eligible randomized controlled studies were included without any language restrictions using rigorous scientific methodology following the PRISMA-NMA guidelines. Third, we performed moderator analysis to assess the effect of the demographic characteristics including age, gender, phase of stroke, type of stroke, and sample size and interventional characteristics including frequency per week, total number of sessions, and total duration the intervention on the estimated evidence and conducted sensitivity analysis by excluding high risk of bias studies to assess the robustness of the study findings. Fourth, the current NMA is an advancement of the previous NMA as more dysphagia therapies including NMES + TDT, tDCS + TDT, rTMS + TDT, and TDT and outcomes including PTT, OTT, and aspiration/penetration were assessed in the current NMA analysis. Some study limitations need to be considered when interpreting the current NMA findings. First, heterogeneity was observed in the four outcomes and inconsistency in some intervention comparisons but transitivity assumption through the full design-by-treatment interaction random-effects model and the moderator analysis were used to address heterogeneity and inconsistency. Second, most studies had smaller sample sizes and limited follow-up time, as such future RCTs with larger sample sizes and longer follow-up periods are needed to further determine the short and long-term benefits of these neurostimulation and traditional dysphagia therapies in PSD. Third, the confidence rating of the evidence for the outcomes was rated very low, low, and moderate because most of the included studies were single-blinded RCTs with limited information on blinding and allocation concealment and thus, future rigorous RCTs are needed to address this issue. Fourth, various types of TDT were used in the current NMA that may demonstrate different therapeutic effect on the PSD rehabilitation and more studies are required to determine the specific effects of these TDT interventions. Lastly, use of non-instrumental subjective assessment tools might lead to over-estimation of treatment effects due to subjective response of the participants.
Conclusions
The current NMA findings demonstrate that the combined and single neurostimulation and traditional dysphagia therapies of NMES + TDT, tDCS + TDT, rTMS + TDT, NMES, rTMS, and TDT are effective therapies for better swallowing function and reducing PTT and OTT. In addition, the combined and single neurostimulation and traditional dysphagia therapies of tDCS + TDT, NMES + TDT, NMES, TDT, rTMS, and PES revealed no difference in reducing aspiration/penetration. In summary, depending on the available neurostimulation and traditional dysphagia therapies, use of combined neurostimulation and traditional dysphagia therapies including NMES + TDT, tDCS + TDT, and rTMS + TDT demonstrate to be the better therapies for improving swallowing function and reducing PTT and OTT. Moreover, more plausible evidence is needed to further determine better combined or single neurostimulation and traditional dysphagia therapies for reducing aspiration/penetration in clinical settings.
Supplemental Material
sj-docx-1-nnr-10.1177_15459683231166940 – Supplemental material for Comparative Effectiveness of Combined and Single Neurostimulation and Traditional Dysphagia Therapies for Post-Stroke Dysphagia: A Network Meta-Analysis
Supplemental material, sj-docx-1-nnr-10.1177_15459683231166940 for Comparative Effectiveness of Combined and Single Neurostimulation and Traditional Dysphagia Therapies for Post-Stroke Dysphagia: A Network Meta-Analysis by Kondwani Joseph Banda, Ko-Chiu Wu, Hsiu-Ju Jen, Hsin Chu, Li-Chung Pien, Ruey Chen, Tso-Ying Lee, Sheng-Kai Lin, Shih-Han Hung and Kuei-Ru Chou in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
The findings and conclusions are those of the authors, who are responsible for its contents. We thank the Community Elderly Health Care Foundation, TMU, and University System of Taipei Joint Research Program, USTP-NTUT-TMU-110-03 for their assistance.
Author Contributions
KJB, KCW, and KRC contributed to the literature search. KJB and KCW contributed to data collection, data analysis, and visualization. KJB and KRC wrote the original draft. HC and KRC contributed to validation and editing of the manuscript. HJJ, LCP, RC, TYL, SKL, and SHH contributed to validation and review of the manuscript. KRC contributed to conceptualization and supervision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
All the related data have been provided in the tables, figures, and supplemental material.
Supplementary Material
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.