
Abstract
Background
The decision of which arm to use to achieve a goal depends on energetic costs and performance abilities of each arm. Following a stroke, there is a reduction in the use of the more-impaired arm. Is it because the energetic costs of the more-impaired arm are increased, or because its use dictates a lower chance of success?
Objective
We sought to elucidate the impact of energetic cost and task success on the arm choice of stroke survivors.
Methods
Thirteen chronic stroke survivors and thirteen neurologically-intact subjects participated in an experiment where they reached towards visual targets in a virtual-reality environment. Energetic cost of reaching with their less-used arm (nondominant/more-impaired) was adjusted by amplifying the range of motion, while task accuracy requirement was independently modulated by changing target size.
Results
Reducing the energic cost of reaching increased the use of the less-used arms in both groups, but by a greater amount in the stroke survivors. In contrast, lowering task accuracy requirement altered arm choice similarly in the two groups. The time spent in decision-making (reaction time) reflected different impacts of energetic cost and task success on the arm choice of the two groups. Conversely, velocity changes were similar between the groups.
Conclusions
The impact of energetic cost on arm choice of stroke survivors is greater than neurologically-intact subjects. Thus, the reduction in the use of the impaired arm following stroke may be primarily due to a subjective increase in the effort it takes to use that arm.
Introduction
Following stroke, many survivors rely on their less-impaired arm to perform tasks that they would normally assign to their now more-impaired arm (“learned nonuse 1 ”). Prolonged nonuse of the impaired arm could create a vicious cycle, in which deteriorating central nervous system responsiveness, 2 atrophic changes in muscle, 3 and loss of cortical representation 4 reinforce one another, leading to further functional degradation.5,6
Despite its significance, it is not known how the upper limb motor impairment of stroke survivors leads to their learned nonuse. Direct measurements of learned nonuse hypothesis was mostly performed with primates,1,7,8 for which sensory (not motor) deficits were surgically induced. Relationship between motor impairment of stroke survivors and their learned nonuse has been examined by correlation analyses, which associated functionality scores of stroke survivors with their measured arm use.9 -12 In these observational studies, however, only a part of between-subject variability in the quantified nonuse (29%-38%) was explained by the functionality scores.11,12 Notably, hemiparetic persons often use their less-impaired arms even when their affected arms are capable of performing the task. 13
Arm choice of stroke survivors may be due to their perception of intrinsic (energy cost) and extrinsic (task goal) factors associated with a given task. Indeed, recent studies showed that expected energetic cost (energy expenditure) and task success can influence arm choice in both neurologically-intact subjects 14 and chronic stroke survivors. 15 However, the way expected energetic cost and task success impact arm choice may be substantially different for stroke survivors, as their impairment could affect how these two factors (energetic cost/task success) are considered and weighed in their decision-making process. For instance, arm choice of stroke survivors may be more sensitive to the expected energetic cost because of their weakness, 16 which could explain their reluctance to use more-impaired arms spontaneously even when they are capable. 13 On the other hand, stroke survivors may have an elevated sensitivity to task failures, suppressing the use of their more impaired arm. 1 We thus hypothesized that arm choice of stroke survivors would be more sensitive to the energetic cost than control subjects, as the use of their more-impaired arm would require a higher level of effort due to their weakness. We also hypothesized that the impact of required task accuracy would be greater for stroke survivors, as the decrease in the target size could make it more difficult for them to perform the task successfully due to their motor deficits.
Here, we used a virtual reality (VR) system to manipulate energetic cost and task accuracy requirements of a reaching task and measured how stroke survivors and healthy controls altered their choice of arm use. We found that the impact of the reduced energetic cost on arm choice of stroke survivors was indeed greater than control subjects. In contrast, the impact of task accuracy was similar in the two groups. Thus, the reduction in the use of the impaired arm following stroke may be primarily due to a subjective increase in the effort it takes to use that arm.
Methods
Participants
Twenty-six subjects including thirteen chronic stroke survivors (S1-S13; age: 49 ± 13 years; 5 female; Table 1) and thirteen right-handed neurologically-intact subjects (C1-C13; age: 33 ± 17 years; 7 female) participated in this study. The experimental protocol was approved by the Institutional Review Board at the Catholic University of America, and the written informed consent was obtained from all participants before their participation. Inclusion criteria for stroke subjects were: (1) chronic stroke (more than 6 months since stroke); (2) between the ages of 20 to 70 years old; (3) have residual motor control and have the ability to voluntarily initiate arm movements. Exclusion criteria were: (1) pain during upper limb movement; (2) musculoskeletal injuries (eg, bone fracture) or medical illness that could hinder their arm movements; (3) unable to give informed consent.
Stroke Subject Characteristics.
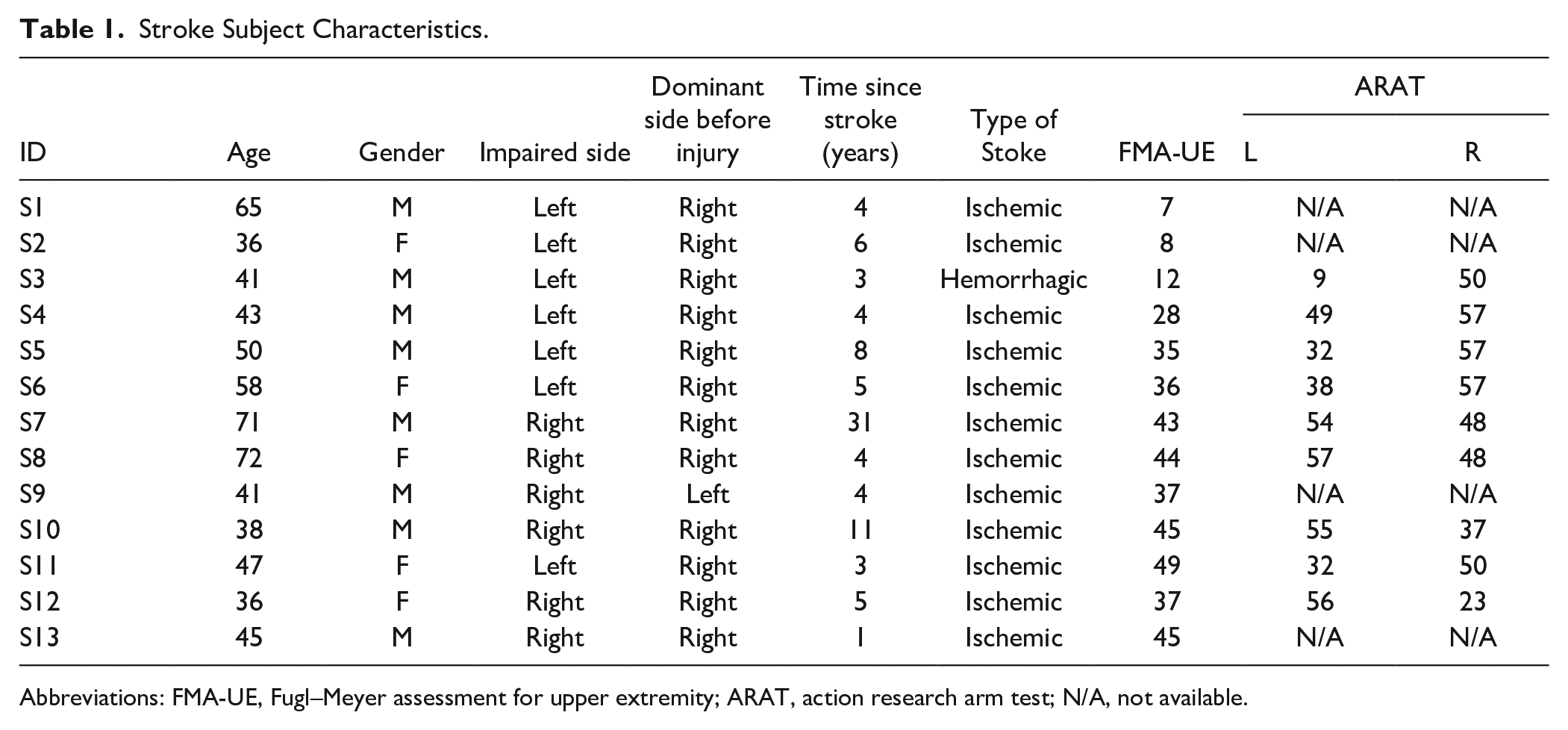
Abbreviations: FMA-UE, Fugl–Meyer assessment for upper extremity; ARAT, action research arm test; N/A, not available.
Experimental Setting
Subjects were instructed to perform reaching movements towards targets that appear in the VR environment using a head-mounted display (Oculus Rift; Facebook Technologies, LLC., CA, USA). A cube-shaped target appeared in a random order at one of the 26 possible locations within the workspace scaled to each subject from the anthropometric measurements (height: eye to waist level; width: between left and right shoulder; depth; between 40$ and 80% of maximum voluntary reach; see Figure 1A). Subjects held two controllers, one in each hand. They were told that they could use either their right or left arm to reach for the target.
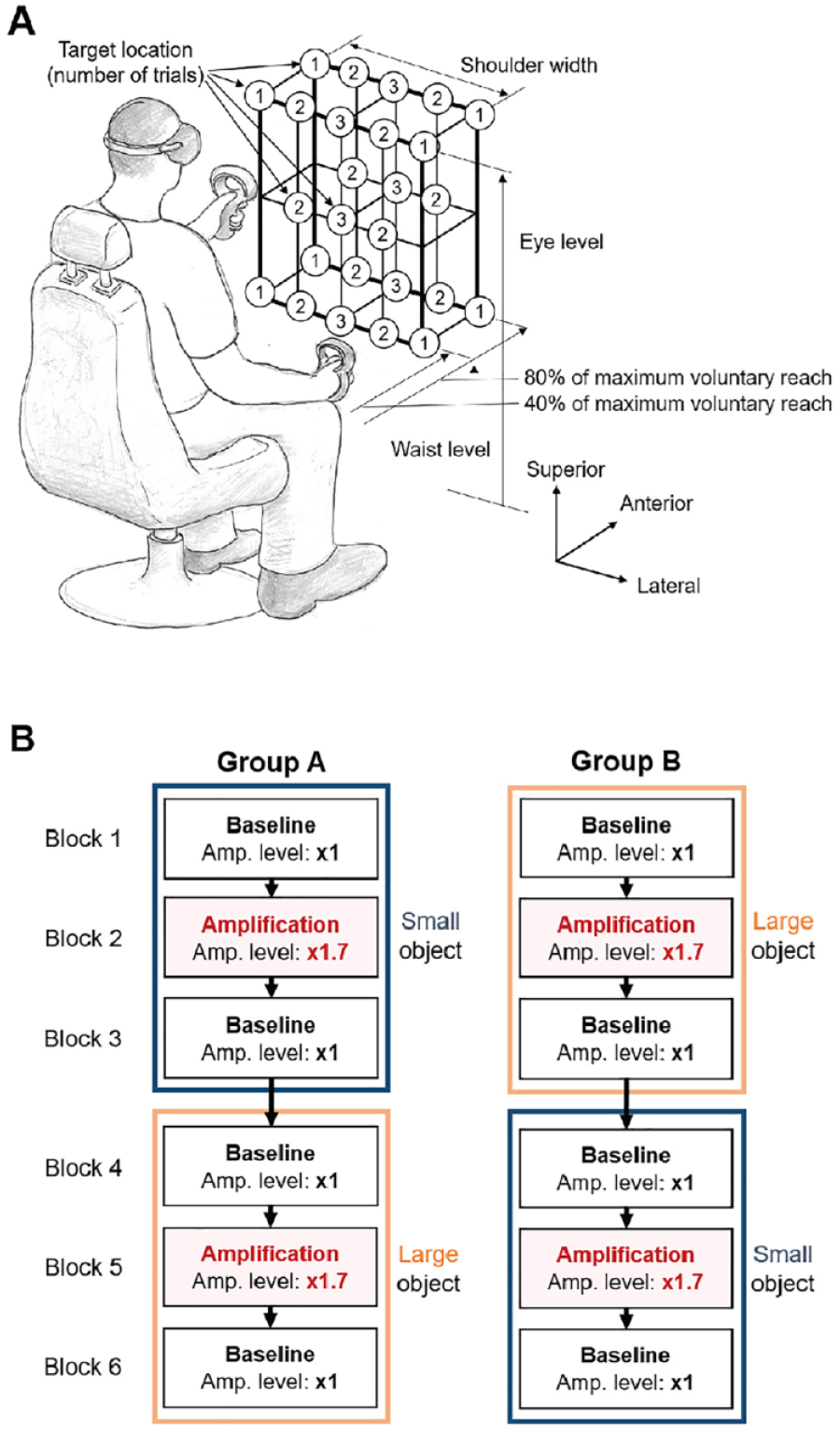
Experimental setting: (A) Target locations. (B) Protocol. Target locations were scaled to the range of motion of each subject. The amplification was applied to the more-impaired arm (stroke) or nondominant arm (control). The order of target size was randomized across subjects (crossover design).
Each trial began with the subject placing their hands on their lap. Once the system detected their hands at the starting position, a cube target was displayed at one of the 26 locations (shown in Figure 1A) with an auditory cue. At this point the subject decided which arm they wished to use for reaching to the target, and then performed the movement. The trial ended by the disappearance of the target once the handheld tool reached inside the target. At this point the subject returned their hand to their lap and after 3 seconds, the next trial started. The positions of the two hand-held controllers and the headset were recorded at 90 Hz.
In each experimental block, one of the two target cube sizes (small: 12 × 12 × 12 cm3; large: 24 × 24 × 24 cm3) and one of the two movement amplification conditions (no amplification: ×1; amplification: ×1.7) were used, which changed the level of task accuracy requirement and energetic cost associated with the task, respectively. Increase in the target size lowered the task accuracy requirement; under visual amplification, the displacement of the more-impaired (stroke) or nondominant (controls) arm from the initial position was amplified (by a factor of 1.7), thereby reducing the energetic cost associated with its movements. The arm movement was amplified regardless the direction of movement. Thus, the visual amplification did not necessarily adjust the task difficulty (or accuracy requirement) as the movements in the task-irrelevant dimension were amplified to the same degree with the movements towards the target. The amplification in our experiment was designed to only reduce the energetic cost associated with the movements of the amplified arm. The amplification level (×1.7) was determined from our previous study 17 and consequent pilot experiments, where the highest amplification level at which subjects did not experience difficulty in controlling the amplified hand movements.
Experimental Protocol
Participants completed six blocks of trials, each consisting of 50 reaching movements. Within each block, the target appeared 18 times at the center locations (6 at eye level, 6 at mid-level, and 6 at waist-level) within the sagittal plane, 24 times at the mid-lines between the center and shoulder lines (8 at eye level, 8 at mid-level, and 8 at waist-level), and 8 times at the boundaries defined at the shoulder width (4 at eye level and 4 at waist-level) (Figure 1A). At each level, a half of the targets appeared at approximately 40% of the maximum reaching distance of each subject, and the other half at 80% of his/her maximum reaching distance. More targets were assigned near the center line for which either arms can be used (ie, increased ambiguity). The eccentric locations (8 targets at the shoulder width) were included to prevent subjects from adopting a strategy of using the same arm to reach to all targets. Within each block, the target appearance order was randomized.
Subjects were randomly assigned to two groups, for which the experimental conditions were implemented in a crossover design (Figure 1B). Out of six blocks, visual amplification was implemented to the more-impaired (stroke) or nondominant (control) arm movements in the blocks 2 and 5, while the no amplification was implemented in the blocks 1, 3, 4, and 6. For one group (group A), the small targets were used in the first half (blocks 1-3), then the large targets in the second half (blocks 4-6); for the other group (group B), the large targets were used in the first 3 blocks and the small targets in the second 3 blocks. Subjects were not notified whether or how their less-used arm movements were amplified during experiments.
Data Analysis
Our primary outcome measure was the percentage use of the less-used arm (PULA), which was defined as the nondominant arm for control subjects, and the more-impaired arm for stroke subjects, computed for each block. In addition, kinematic analyses were performed to examine difference in the movement parameters between the conditions (amplification; target size). The following kinematic parameters were estimated from the movement data of the hand-held controllers of both sides; a) peak velocity (PV) of each hand, b) reaction time (RT), c) task duration time, d) path length ratio, and e) overshoot ratio for each reaching movement, which were computed in a similar way to our previous study 17 (see Appendix for details). All kinematic parameters were computed from the movement data in the VR environment. Trials with small RT values (<50 milliseconds) were excluded from the analysis.
The PULA and kinematic variables from both arms were compared between the two amplification conditions (baseline: C1; amplification: C1.7) and the target sizes (small; large) using a repeated-measures analysis of variance (rmANOVA). Here, kinematic variables of non-amplified arm (dominant/less-impaired) was compared to examine possible bilateral transfer in motor adaptation to amplification.
18
Significant level was set to P-value of .05 for all statistical tests, and the partial eta square (
We also examined the within-block changes in the arm use for each condition (target size/amplification). For each block, the average less-used arm use (PULA) was computed from the first 15 trials (“Early”: trials 1-15), the 15 trials in the middle (“Mid”: trials 19-33), and the 15 trials at the end (“Late”: trials 36-50), and the difference between these three phases was compared by rmANOVA.
Additionally, to test whether the degree of functional impairment of individual stroke survivors affect the degree of their motor adaptation, both Spearman’s and Pearson correlation tests were performed between the change in arm use (ΔPULA) of stroke survivors and the Fugl–Meyer Assessment for Upper Extremity score. To test whether changes in movement vigor measures (RT and PV) reflect the degree of motor adaptation (change in arm use), correlation tests were performed between the change in arm use (ΔPULA) and the changes in reaction time (ΔRT) and the changes in the peak velocity (ΔPV). For each correlation test, normality of the correlation was tested by the Shapiro-Wilk test on the independent variable. In case a nonlinearity was found, a nonparametric Spearman’s test was used instead of the Pearson correlation test. Additionally, the normal probability plot of the residuals was inspected. Linearity and homoscedasticity were examined from the scatter plot between the residual and the predicted value for each regression.
Results
All participants completed the task. Two stroke survivors with severe shoulder and elbow impairments (S1, S2; FMUE ≤ 8; Table 1) were found to use their more-impaired arms only reaching for the targets close to the initial position (less than 10% of the times), thus their data were excluded from the analysis. Reaching trials with the RT larger than 1000 milliseconds (“distraction”; 132 out of 7800 trials) or smaller than 100 milliseconds (“anticipatory action”; 28 out of 7800 trials) were excluded from analysis.
Impact of Energetic Cost and Task Accuracy Requirement on Arm Use: Difference and Similarity Between Groups
For both groups, the percentage use of less-used arm (PULA) significantly increased under the amplification (amplification: F1,21 = 101.76, P < .01,
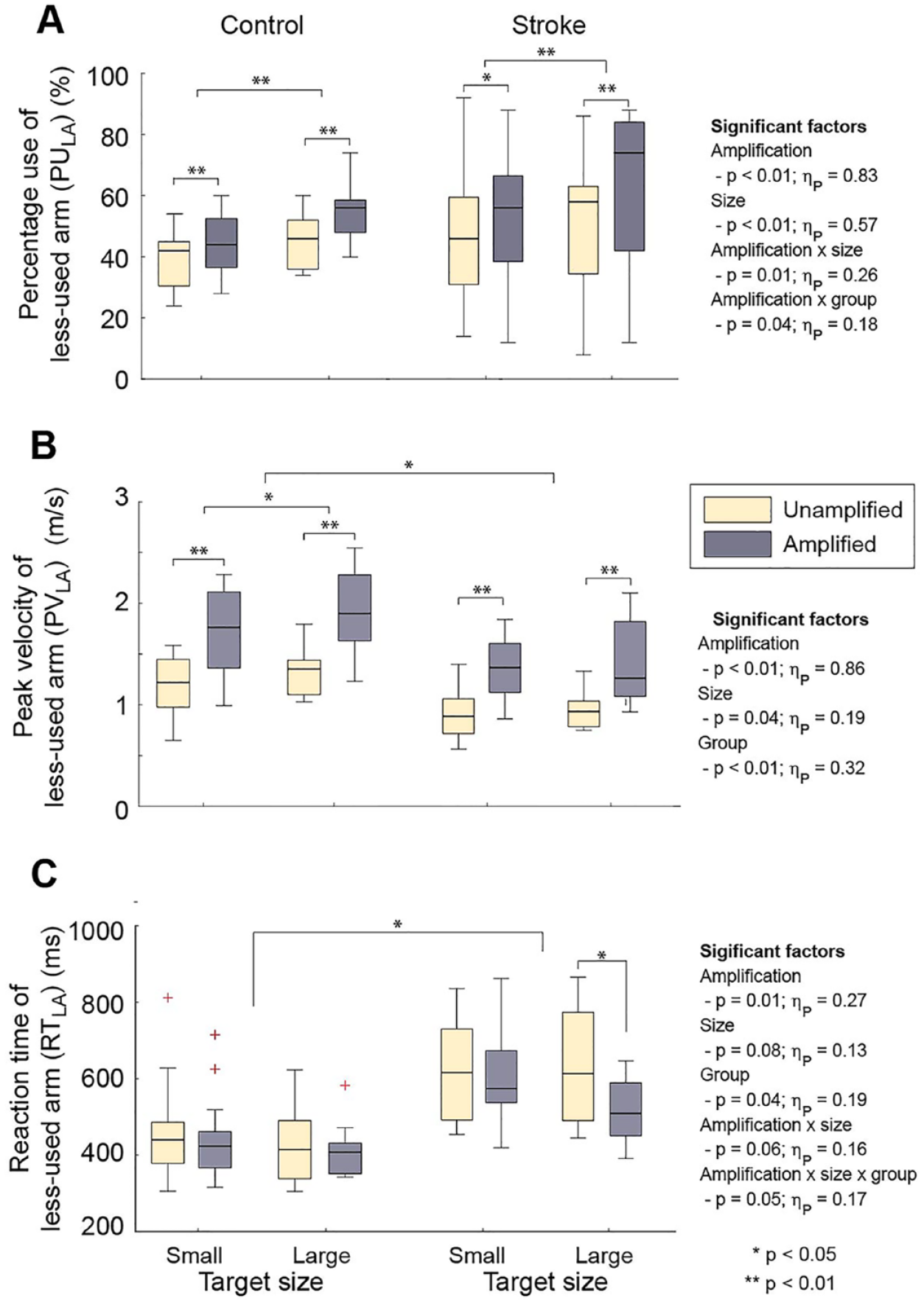
Arm use and kinematic parameters under experimental conditions (target size; amplification): (A) Percent use of less-used arm (PULA). (B) Reaction time of less-used arm (RTLA). (C) Normalized peak velocity of less-used arm. Here, the error bars are the 95% confidence interval, the bottom and top of the box are the 25th and 75th percentiles, the line inside the box is the 50th percentile (median), and outliers are shown as red crosses.
Mean (SD) Values of the Arm Use and Kinematic Variables.
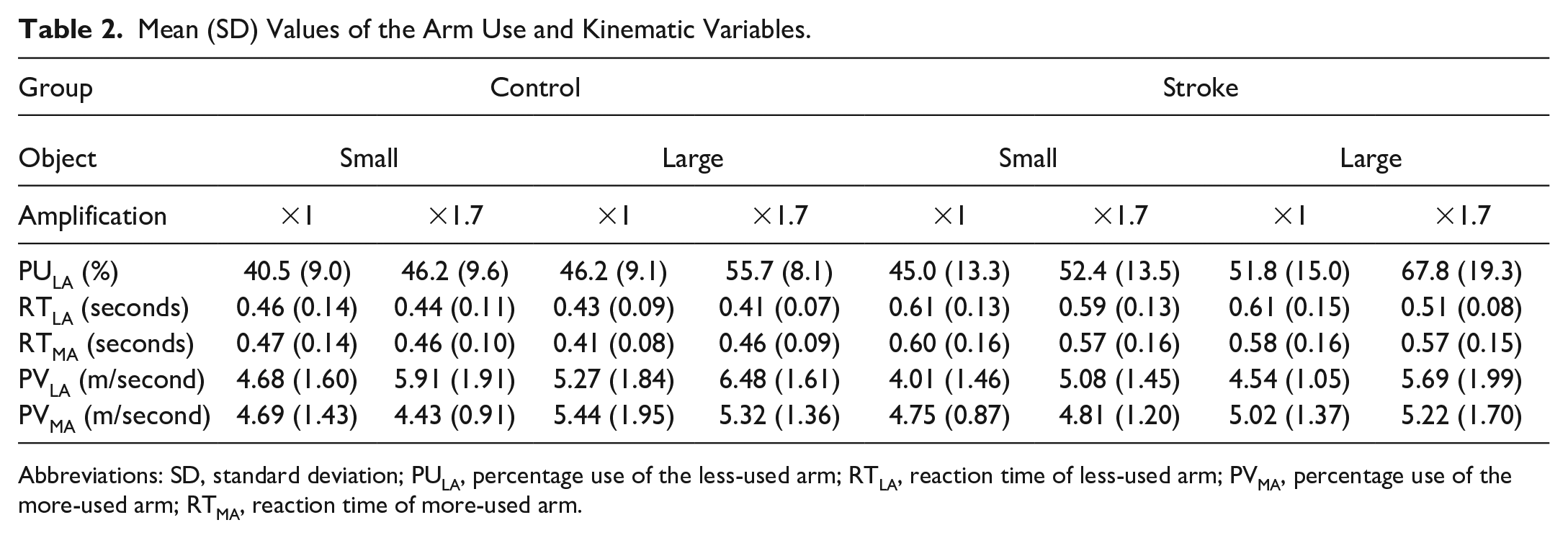
Abbreviations: SD, standard deviation; PULA, percentage use of the less-used arm; RTLA, reaction time of less-used arm; PVMA, percentage use of the more-used arm; RTMA, reaction time of more-used arm.
Additionally, two significant interactions were found; first, the impact of amplification on PULA was greater for stroke survivors (amplification × group: F1,21 = 4.55, P = .04,
Peak Velocity and Reaction Time
Kinematics of the less-used arm also changed significantly under different task conditions (ie, amplification and target size; Figure 2B; Table 2). The PV was significantly greater for control subjects (F1,21 = 10.06, P < .01,
The RT of the less-used arm also significantly decreased under amplification (F1,21 = 7.93, P = .01,
For the non-amplified arm (dominant/less-impaired side), the RT was longer for stroke survivors (F1,21 = 8.75, P < .01,
Kinematic Parameters: Path Length Ratio and Overshoot
Other kinematic parameters were also significantly affected by task conditions; the amplification significantly increased the overshoot of the amplified arm for both groups (F1,21 = 23.30, P < .01,
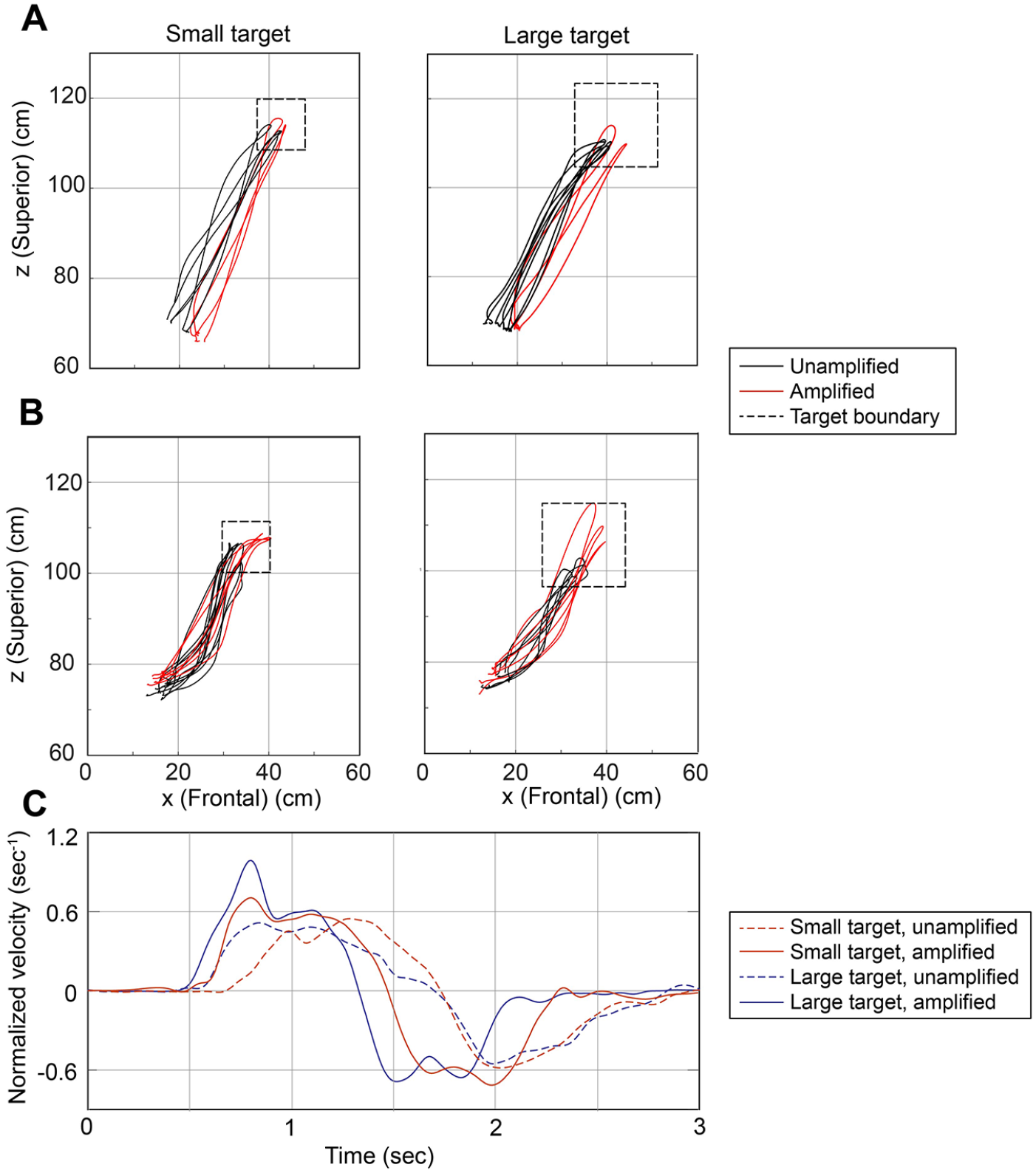
Representative cases of the movements (from blocks 1, 3, 4, and 5; A: control—C11; B: stroke—S10) and the velocity profiles (C) of the less-used arm of a stroke survivor (S10). The subject reached for a center target (T24) under four different experimental conditions. The movement trajectories of the control subject were straight (A), while those of the stroke subject were more curved (B). The movement overshoot of the stroke survivor was greater under amplification, especially when reaching for the large target. As shown in the representative velocity curves of a stroke survivor (S10) (C), the reaction time decreased and the peak velocity increased under amplification (dotted vs solid lines), and these changes were greater when reaching for the large target (blue lines).
Significant group difference and interactions were found in the path length ratio (PLR) of the less-used arm. The PLR values of the less-used arms were significantly greater for stroke survivors (F1,21 = 6.54, P = .02,
Adaptation Over Time: Within-Block Changes in the Less-Used Arm Use
The less-used arm use was significantly different across the three phases (F2,22 = 3.23, P = .05,
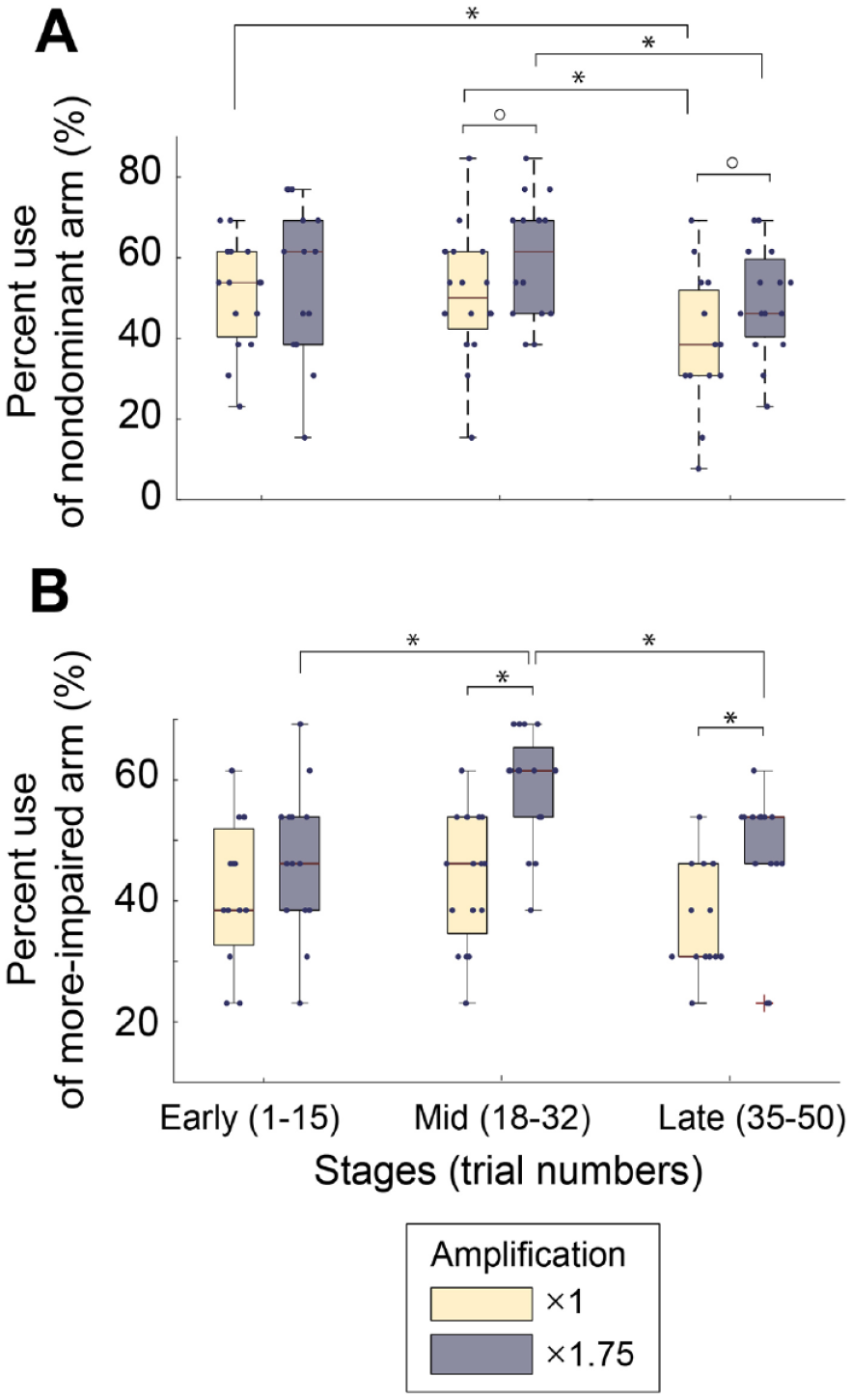
Within-block changes in the less-used arm use, when reaching for large targets; (A) Control; (B) Stroke. The nondominant arm use of control subjects generally decreased over time regardless of the amplification condition (A). In contrast, for stroke subjects, the increase in the more-impaired arm use by the amplification was the largest in the middle portion of the block (trials 19-33), which decreased at the late stage (trials 36-50) (B). However, even at the late stage, the more-impaired arm use of stroke survivors significantly increased under amplification.
Individual Differences in Adaptation: Reaction Time Versus Peak Velocity
Between the two factors examined (RT and PV), only the RT of stroke survivors explained between-subject variability in the use of their more-impaired arm; across task conditions (amplification/target size), the change in the use of less-used arm (ΔPULA) of stroke survivors was found to be significantly correlated with the change in their RT (r = −0.63; P < .01), but not with the change in their PV (r = −0.19; P = .41) (Figure 5B). On the other hand, the change in the PULA values of control subjects was not correlated with the change in either RT or PV (Figure 5A).
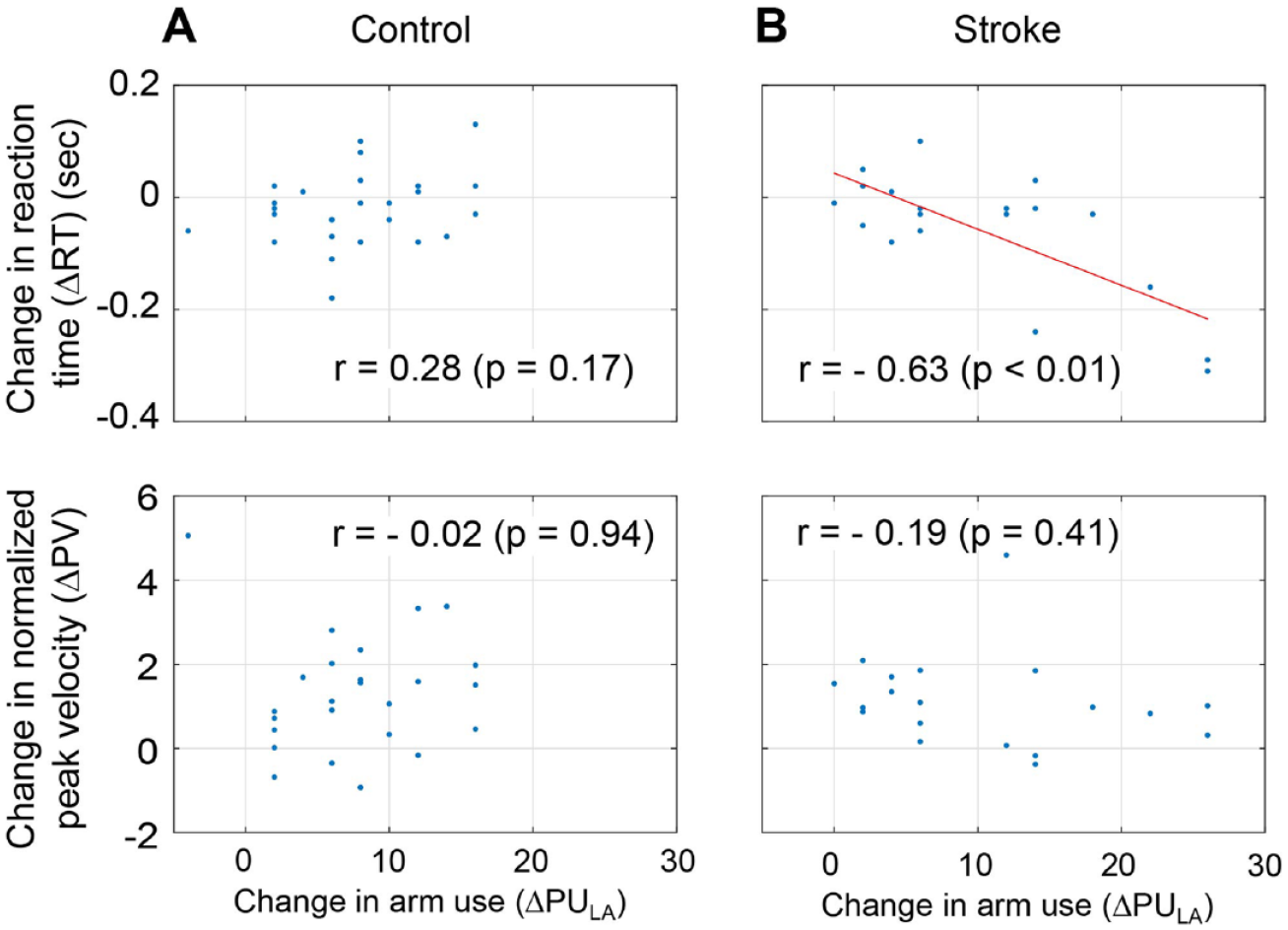
Correlation between the changes in movement parameters (reaction time and peak velocity) and the changes in the arm use (ΔPULA) across subjects for each group: (A) Control subjects. (B) Stroke survivors. No significant correlation was found for control subjects. In contrast, for stroke subjects, the change in the reaction time was found to negatively correlate with the change in arm use; for those with a bigger increase in the arm use, the reduction in their reaction time was greater.
Clinical functionality scores of stroke subjects were not significantly correlated with the changes in the use of their less-used arm (ΔPULA) for either small targets (r = 0.04; P = .89) or large targets (r = 0.40; P = .20).
Discussion
Both the expected energetic costs and the task’s accuracy requirements affect the choice of which arm to use to perform a task.
Following a stroke, the effort of using the impaired arm increases, while the ability to accurately control that arm decrease. Here, we altered the effort and accuracy costs independently and found that the stroke survivors responded more to the reduced effort costs (as compared to controls), while the impact of altering task accuracy requirements remained similar between the two groups.
Impact of the Expected Energetic Costs and Task Accuracy Requirement on Arm Choice of Stroke Survivors
The greater impact of energetic cost on arm choice in stroke survivors suggests the importance of weakness (paresis) in arm use post-stroke. Previous studies showed that weakness is the predominant impairment contributing to upper limb functional degradation following stroke (arm 16 : hand 19 ), thereby leading to learned nonuse of the more-impaired arms. 5 Our study provides evidence that increased energy expenditure associated with the use of the more-impaired arm may also be primarily responsible for reduction in its use following stroke, as the reduction in energy requirement led to a greater increase in the use of more-impaired arm of stroke survivors, when compared to control subjects. Our results suggest that the decision-making of stroke survivors is altered, and that their greater sensitivity to energy requirement could make them ‘underestimate’ the ability (or ‘utility’ 20 ) of their more-impaired arms. Thus, a greater sensitivity to effort costs could explain their unwillingness to use more-impaired arms, even when that arm is capable of performing the task. 13
Previous training studies21,22 have found that movement amplification in VR environment increases the use of the more-impaired arm of stroke survivors. In these studies, however, the goal-directed sub-movement components (ie, movement vector projected to the direction toward the target) were disproportionately amplified, thereby lowering task difficulty as well. It is thus difficult to discern whether the increase in arm use observed in these studies was due to energy reduction, or lower task difficulty. Our results show that reduction in reduction in energetic cost alone could promote the use of the more-impaired arm.
Conversely, task accuracy requirement had a similar impact on the use of the less-used arm for both groups; the change in the use of less-used arms due to the target size was similar for the control and stroke subjects. Unlike energy requirements, task accuracy did not preferentially promote the use of the less-used arms in stroke survivors. It is likely that, for stroke survivors, lowering task accuracy requirement could also have promoted the use of their less-impaired arms, which also exhibit functional deficits.23 -25 However, when combined with reduced energy requirements, lower task accuracy condition (bigger target size) induced a greater degree of change in arm use (ΔPULA = 16.0% ± 10.8%) than the higher task accuracy condition (ΔPULA = 7.4% ± 7.5%), particularly for stroke survivors. While this 3-factor interaction (size × amplification × group) did not reach significance for the arm use, a significant 3-factor interaction was observed in the movement characteristics (ie, RT and path length ratio), suggesting that the interactions between the task accuracy requirements and expected energy requirements in arm choice of stroke survivors may be fundamentally different from those of control subjects.
Notably, the time course of the behavioral adaptation under amplification was different between the groups. Under amplification, while the use of the less-used arm in the control group decreased over time within the block, the use of the more-impaired arm in the stroke group increased in the mid-stage, then decreased in the late-stage. We postulate that the stroke survivors could have increased the use of their more-impaired arm initially (up to mid-stage), as the reduction in energetic cost motivated them to use their more-impaired arm more. Such increase in arm use, however, may have caused fatigue, thereby leading to a significant reduction in the arm use in the late stage. But the more-impaired arm use in the late stage under amplification was still greater than that without amplification. Such fatigue-related behavioral changes should be carefully considered in stroke rehabilitation. 26
Time Spent in Decision-Making Was Indicative of Change in Arm Use of Stroke Survivors
The time spent in decision making (RT) in stroke subjects was significantly longer than that of control subjects, even when their movement vigor, represented by the PV, were not significantly different. The slower RT may be due to the impaired ability of stroke survivors to process information. 27
More importantly, RT of stroke survivors was a better indicator of the arm choice than the PV. Across stroke subjects, the change in RT accounted for a significant between-subject variability in the increase in arm use (r = −0.63; P < .01). Additionally, the patterns of change in RT mirrored the patterns observed in arm use: we found a greater increase in arm use of stroke survivors under amplification when they reached for large targets. Similarly, a significant reduction in RT of stroke survivors under amplification was observed when they reached for large targets, but not for small targets (Figure 2).
Thus, our results suggest that energetic cost reduction particularly affects “initiation” of the more-impaired arm in stroke survivors (indicated by changes in RT). Previously it was shown that initiation and invigoration of movements are two separate, sequential processes that involve distinct sets of neuronal actions, 28 mediated via striatopallidal pathways that modulate “motivation” for a specific action outcome. 29 It is possible that, during daily activities, altered decision-making of stroke survivors (ie, learned non-use) results from the physical impairments that have caused “chronic stress,” which alters striosome-circuit dynamics and leads to aberrant decision-making. 30 Reduction in energetic cost associated with the use of the more-impaired arm, facilitated by visually amplifying the movement range, appeared to have effectively increased the motivation for its use. The observed reduction in RT also indicates an increased level of attention/arousal associated with the use of more-impaired arm, which can affect the use of the paretic arm. 11
Implications
The results of this study show that stroke not only produces physical impairments, but also alters their decision-making processes that determines arm use. It appears that weakness/hemiparesis of chronic stroke survivors could be for the main factor in developing learned nonuse, making decisions more sensitive to the increased energetic cost of the more-impaired arm. This increased sensitivity makes stroke survivors underestimate the “utility” of their more-impaired arm, thereby suppressing its use even when the more-impaired arm can perform the task. 13 Learned nonuse following stroke thus is developed not only because of the physical impairments, but also because of their impaired ability to properly understand their impairments, evaluate their capacity, and make proper decisions.
We also provided evidence that the use of the more-impaired arms of stroke survivors can be promoted by reducing energetic costs associated with its use, which advocates for the use of assistive devices in rehabilitation trainings. Lowering task accuracy requirement alone may not be sufficient to promote the more-impaired arm use. However, task accuracy could impact the efficacy of assisted training, which was indicated by their significant interactions determining arm use. Thus, the task to be practiced should be carefully designed in their training and/or daily activities.
Our study showed that a reduction in the energetic cost associated with the use of the more-impaired arm in stroke survivors can directly affect their “readiness” to use the more-impaired arm, thereby promoting its use. The change in the “readiness” to use the more-impaired arm (RT) is a stronger predictor of its use than their movement vigor itself (PV). Similarly, when the level of energetic costs varied in neurologically-intact subjects, such energy-related changes in their decision-making were best explained by changes in RT. 31 For chronic stroke survivors who received constraint-induced movement therapy, an increase in the contingent negative variation (“readiness potential” of electroencephalography signals) correlated with their functional improvement, 32 which also emphasizes the importance of “readiness” to involve more-impaired limbs in daily activities. Therefore, to reverse the learned nonuse of chronic stroke survivors, the “readiness” to use their more-impaired arms should be promoted (via energy reduction/task redesign) and/or measured appropriately (eg, RT; contingent negative variation) to properly gauge their recovery.
Limitations
The number of subjects included in this study was small, which prevented other between-subject variables (eg, age) from being included in the analysis. While the statistical power of our main finding (ie, changes in the arm use) was found greater than 80% in post hoc analyses, a follow-up study with a larger number of subjects is warranted to confirm the findings of this study, and to examine potential impact of several important between-subject variables such as age, sex, clinical functionality scores, and concordance of lesion side (ie, dominant- or nondominant-side impaired). Our post hoc analysis showed that, while the impact of energy on arm choice was not significantly between two groups of stroke concordance (P = .22), we also observed different patterns of adaptation between the two groups; the impact of energy reduction was different between the two target sizes (4.4% for the small target; 19.2% for the large target) in the concordance group (dominant-side impaired), while the impact was similar between two sizes (10.4% for the small target; 12.8% for the large target) in the non-concordance group (nondominant-side impaired).
The control subjects were slightly younger than the stroke survivors tested in this study, which could have contributed to the observed between-group differences. Previous studies showed that, while older subjects make slower movements during reaching, their movement coordination patterns remain similar to that of younger subjects. 33 However, it is possible that the age of subjects could have affected their arm choice due to several age-related factors such as fatigue or changes in internal reward processing.34,35
It is possible that differences in the specific task conditions used in our experiment, that is, amplification levels and/or target sizes, may have been not large enough to induce behavioral changes (ie, arm use) in some subjects. In particular, the amplification did not impact the arm use of stroke subjects with severe arm impairments (S1, S2), indicating that the generalization of the findings of this study should be limited to stroke survivors with moderate-to-mild upper-limb impairments. Conversely, the amplification could have a disproportionately greater impact on some stroke survivors; while we clarified to stroke survivors (before testing) that this was not a training study to promote arm use but a research study that aimed to understand arm use following stroke, some subjects could have intentionally used their more-impaired arm once they recognize the amplification. On the other hand, it is possible that the difference in the target size used in this study was too small to induce significant changes in the arm use of stroke survivors. Further investigations on the between-subject differences in the motor adaptation, adopting various levels of amplifications or target sizes, are warranted to elucidate such possible between-subject differences in the motor adaptation of stroke survivors. Such studies will reduce the risk of a type-II error (an error of omission); for instance, it is possible that the impact of task difficulty for stroke subjects could be greater if a larger target size was used in the experiment.
Furthermore, it remains to be seen whether the behavioral changes observed in this study can lead to the meaningful changes such as the increased arm use in daily functional activities. Longitudinal training studies need to be carried out to confirm rehabilitative benefits of trainings with altered sensory feedback designed to motivate the use of more-impaired arm of chronic stroke survivors.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Disability, Independent Living, and Rehabilitation Research [grant number 90REGE0004].