
Abstract
Stroke is a leading cause of death and disability. It is a complex and largely heterogeneous condition. Prognosis for variations in impairment and recovery following stroke continues to be challenging and inaccurate, highlighting the need to examine the influence of other currently unknown variables to better predict and understand interindividual differences in stroke impairment and recovery. The concept of “cognitive reserve,” a feature of brain function said to moderate the relationship between brain pathology and clinical outcomes, might provide a partial explanation. This review discusses the potential significance of cognitive reserve in the context of stroke, with reference to reduced burden of disability poststroke, health promotion, intervention and secondary prevention of cognitive impairment, ease and challenges of translation into clinical practice, prognosis and prediction of recovery, and clinical decisions and trial stratification. Discussions from the review aim to encourage stroke clinicians and researchers to better consider the role of premorbid, lifestyle-related variables, such as cognitive reserve, in facilitating successful neurological outcomes and recovery following stroke.
Introduction
Stroke is a serious condition characterized by a significant interruption in blood flow to the brain that can result in structural brain damage, and resultant impairments in movement, cognition, sensation, and language. 1 In 2013 alone, 25.7 million people globally were living with the consequences of stroke, and 10.3 million new cases of stroke occurred. 2 The condition has thus been recognized as the second leading cause of death and adult neurological disability globally, 2 and is considered a major international health care challenge. The magnitude of the problem highlights the importance of better understanding the factors that might contribute to successful stroke outcomes and recovery.
Recent decades have seen an increase in knowledge regarding potential determinants and biomarkers 3 of impairment and recovery following stroke (see Figure 1 and Appendix 1 for an overview). For example, demographic and stroke-specific factors such as age, sex, size, severity and location of infarct, initial impairment, structural and functional biomarkers (eg, corticospinal tract [CST] integrity),4,5 as well as acute treatment options, environmental conditions, acute level of consciousness and damage to key brain regions (ie, the anterior arcuate fasciculus and the development of aphasia)3,6-10 have all demonstrated prognostic value in predicting motor, cognitive, and/or language impairment and recovery following stroke. However, even after consideration for known predictors in complex statistical analyses, predictive models remain imperfect and fail to fully explain pervasive interindividual differences. The heterogeneity of stroke impairment and recovery thus highlights the need to examine the influence of other currently unknown variables to more accurately predict and understand interindividual differences in stroke recovery. The concept of cognitive reserve 11 might partially address this gap in knowledge (see Figure 1) and will be explored in this review, first with a theoretical overview of the concept, followed by a review of potentially important findings relevant to stroke researchers, clinicians, and survivors, which are rarely reported and poorly combined and integrated across current stroke literature. 12
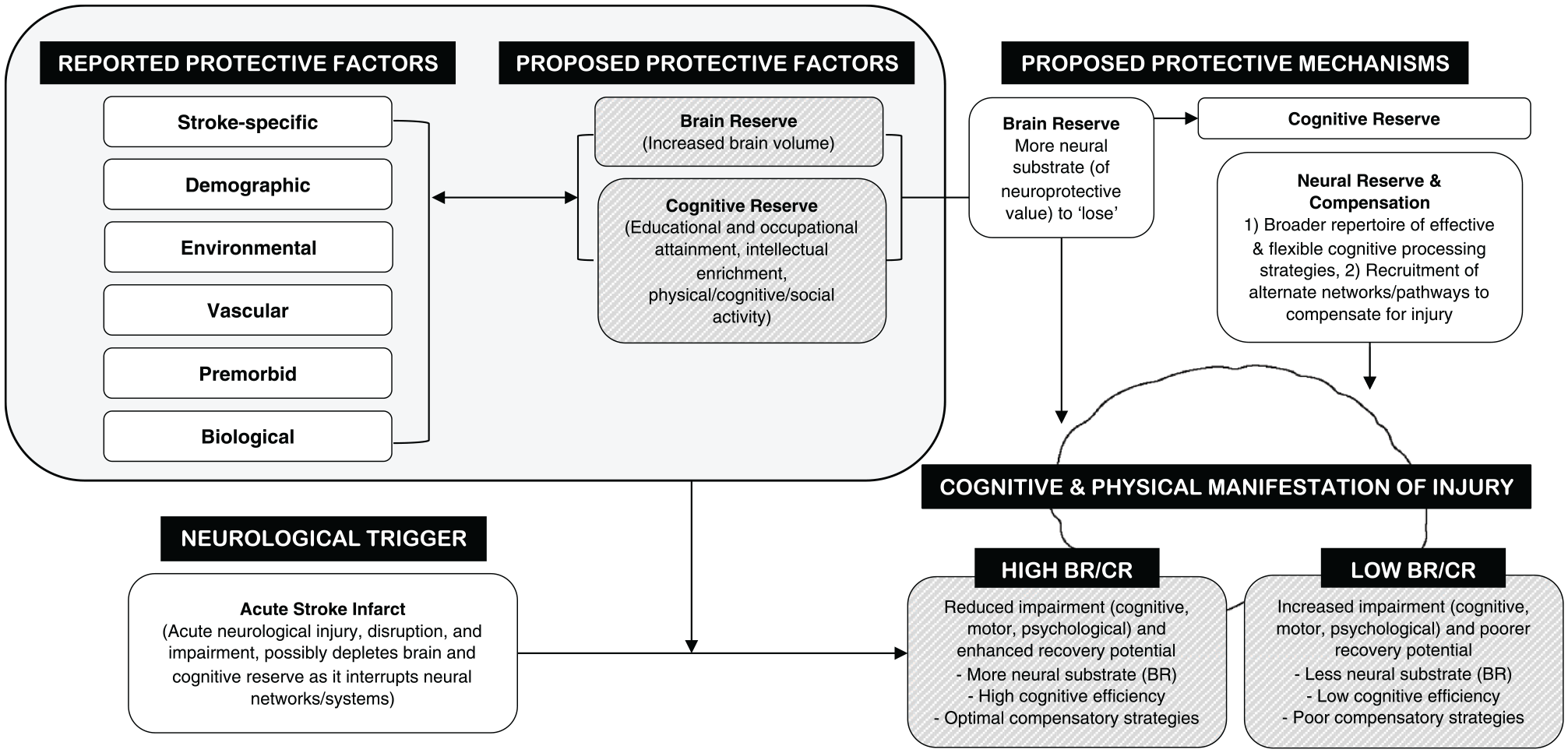
Reported (not exhaustive) and proposed protective factors (brain and cognitive reserve) and neural/cognitive mechanisms of brain/cognitive reserve and how they might influence impairment and recovery following stroke (figure modelled and adapted from Pinter et al 13 and Barulli and Stern). 14 See Appendix 1 for specific examples of the “reported protective factors” detailed in the figure. The figure is intended to highlight the gap in current knowledge and how brain and cognitive reserve might manifest clinically between patient groups. It is important to note that educational attainment (the most common “cognitive reserve” indicator in the literature) has been previously associated with some of the “reported protective factors” (eg, demographic factors, including socioeconomic status) 15 and that some “reported protective factors” likely demonstrate a degree of interrelatedness. BR, brain reserve; CR, cognitive reserve.
Theoretical Overview of the Reserve Concepts
What Is “Reserve?”
“Reserve” is a feature of brain structure and function said to moderate the relationship between brain pathology or injury and its clinical manifestation. 11 The concept was developed to explain pervasive differences in clinical outcomes between individuals with an equivalent or similar degree and/or severity of brain pathology or damage,11,16 most notably in those with Alzheimer’s disease. Two alternate forms of reserve are theorized—brain reserve and cognitive reserve. It is important to make this distinction, as brain and cognitive reserves are theorized, defined, and measured differently. 17
Brain Reserve
Brain reserve, also known as “brain reserve capacity” (BRC), 18 suggests that increased neural substrate (ie, increased brain size, and higher neuronal/synaptic count) is of neuroprotective value and can modulate cognitive performance. 19 The BRC or “threshold” model proposed by Satz 18 suggests that once pathological demand reaches an indefinite and individualized critical threshold (for example, once neural resources are depleted beyond that required to maintain some degree of effective cognitive performance), clinical expression of disease and/or injury occurs.
Cognitive Reserve
On the other hand, cognitive reserve is an active process, whereby better neurocomputational flexibility, such as a broader repertoire of, and/or more effective, cognitive processing strategies, may moderate the manifestation of pathology/injury, along with enhanced neural compensation (neuroplasticity).11,16 More specifically, the 2 features of cognitive reserve (neural reserve and compensation) may differentially work to (1) utilize, optimize, or strengthen preexisting and effective cognitive processing strategies to maximize performance when neural networks are compromised by neuropathology/injury (neural reserve), such as stroke and (2) recruit alternate neural networks or pathways not normally used by healthy individuals in order to compensate for neurologic disruption, such as an acute infarct (neural compensation)11,16 (see Figure 1 for a mechanistic schematic).
Engaging in complex mental/lifestyle activities across the life span, such as educational and occupational pursuits, and physical (eg, playing sports), cognitive (eg, reading), social (eg, attending recreational clubs), and leisure (eg, arts and crafts) activities, is generally thought to impart the brain with a “cognitive reserve” that can be drawn upon when needed 20 (see Table 1 for the most common cognitive reserve “indicators”). It is, however, important to note that cognitive reserve is a “latent” construct, meaning that what is measured (an observed score on a task or test) does not comprehensively represent the actual construct.21,22 There is a gap between the conceptualization of cognitive reserve as a dynamic construct and its operationalization, with cognitive reserve typically operationalized using static proxy indicators (eg, years of education) (see Table 1) thought to “boost” cognitive reserve development (see Figure 2 for a simplified conceptual model of methodological components needed to assess cognitive reserve in stroke populations in a research context).
Overview (Not Exhaustive) of the Most Commonly Used and Psychometrically Sound Indicators Used to Operationalize Cognitive Reserve Across the Literature. a
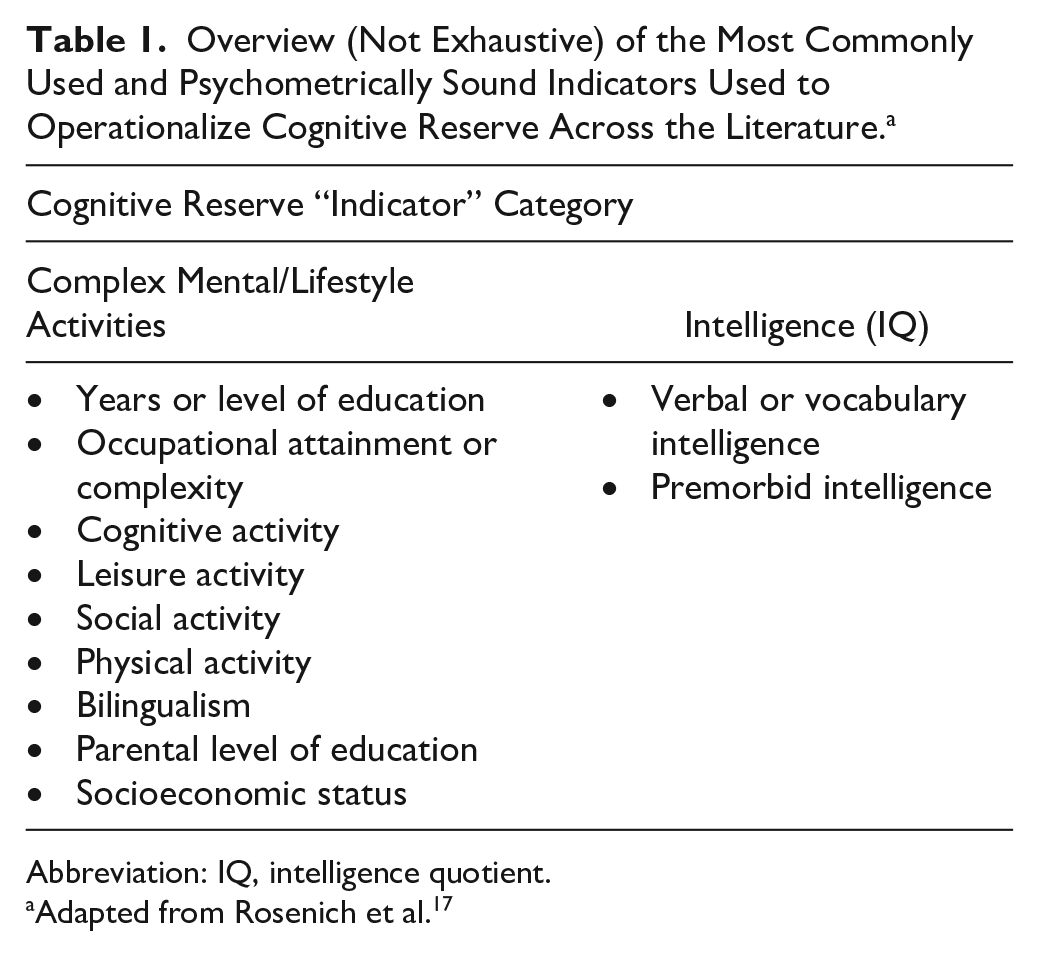
Abbreviation: IQ, intelligence quotient.
Adapted from Rosenich et al. 17
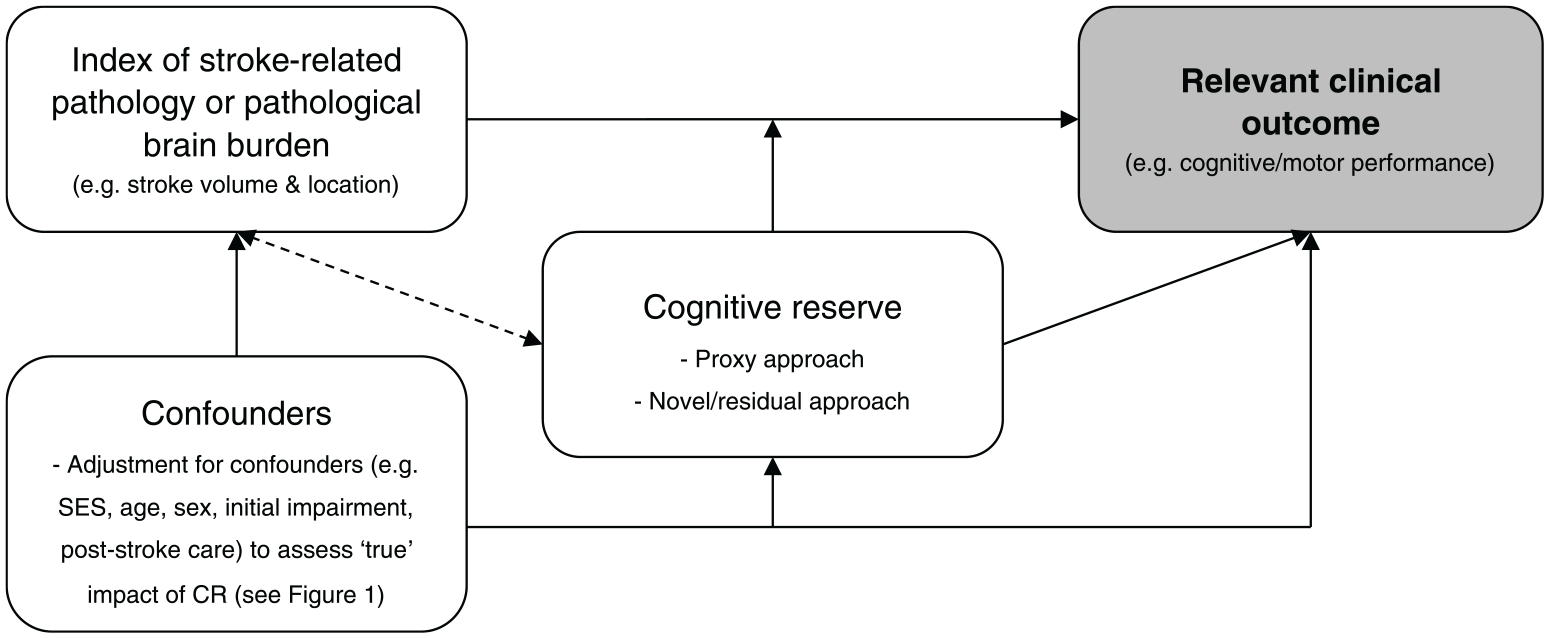
Simplified conceptual model of methodological components necessary to assess the cognitive reserve hypothesis in populations with stroke (figure adapted from the conceptual framework of cognitive reserve in cognitive aging detailed in Steffener et al 23 and Steffener and Stern 24 ). The model has been simplified and is not exhaustive but provides a starting point for researchers and clinicians considering the assessment of cognitive reserve in populations with stroke and is testable using statistical modeling. Stern 11 proposes 3 necessary components for any study assessing cognitive reserve: a measure of cognitive reserve, a measure of brain pathology, and a relevant clinical outcome measure in which the model attempts to “explain” (most commonly, cognitive performance). A measure of pathological/injury burden is crucial to show that any given cognitive reserve indicator modifies the relationship between pathology and performance, in line with cognitive reserve theory. 25 The arrows demonstrate some of the potential relationships/modifications (not exhaustive) between factors based on previous findings assessing cognitive reserve and clinical outcomes in neurological populations (not exclusively stroke): “confounders” → “index of pathology,” 26 “confounders” → “cognitive reserve,” 27 and “confounders” → “relevant clinical outcome”; 3 “cognitive reserve” → the relationship between pathology and outcomes, 28 “cognitive reserve” → “relevant clinical outcomes,” 29 and “cognitive reserve” → “index of pathology”; 30 “index of pathology”→ “cognitive reserve,”19,24 and “index of pathology” → “relevant clinical outcome.” 24 The bidirectional line between “index of pathology” and “cognitive reserve” is dashed to indicate that it is likely that injury/pathology influences cognitive reserve, however there is no information about this in stroke as of yet. SES, socioeconomic status’ CR, cognitive reserve.
The focus of this article will be on the applicability of cognitive reserve—being potentially modifiable—rather than brain reserve, in mediating neurological impairment and successful recovery.
Stroke “Recovery” and “Compensation” in the Context of Cognitive Reserve Theory
Poststroke changes to impairment and performance likely occur through a combination of spontaneous neural repair and experience-dependent processes, including substitution and neural compensation. 31 These processes are theoretically and technically distinct. 32 Mechanisms of stroke recovery that are most likely influenced by cognitive reserve may be mostly, but not exclusively, compensatory. Henceforth, the term “recovery” when used throughout this article refers to the cognitive/motor/psychological changes that occur poststroke that we believe are likely driven by “compensatory” rather than “spontaneous” mechanisms. Individual differences in neural compensatory mechanisms such as the “recruitment” and “retraining” of unaffected brain areas to maintain performance might partially constitute differences in cognitive reserve, as neural compensatory mechanisms parallel the mechanisms proposed by cognitive reserve theory.11,16 Importantly, however, the exact mechanism(s) through which cognitive reserve develops, and facilitates neuroprotection, remains a point of contention and has been subject to increased investigation. 33 Examples of the cognitive and neural mechanism(s) of cognitive reserve might include more effective/flexible cognitive processing, enhanced neuroplastic strategies (eg, increased synapto- and neurogenesis) 34 and the upregulation and expression of brain-derived neurotropic factor, known to facilitate neuroplasticity. 35 Additionally, it is currently unknown, but likely, that the nature and location of a stroke infarct is capable of modifying or dampening the neuroprotective benefits of both brain and cognitive reserve (see Figure 2). On the other hand, differences in spontaneous neurological “recovery,” including the resolution of cerebral edema and reperfusion, may be more dependent on immediate external factors such as access to healthcare and acute interventional therapies, and likely occur independently of cognitive reserve.
Cognitive Reserve as a Partial Explanation for Variability in Stroke Outcomes and Recovery: Current State of the Evidence
Few studies, with limited methodological approaches, have explicitly sought to assess the influence of cognitive reserve on impairment and recovery following stroke. Current preliminary evidence suggests that the concept likely affects cognitive and activity-based (motor and disability) outcomes and recovery poststroke; however, more work is needed to disentangle its exact contributions. The influence of cognitive reserve on mood is less clear; however, it should be acknowledged that poststroke impairments (eg, cognitive impairment) often reflect poorly on mood and are likely interrelated. 36
Cognitive Reserve and Cognition Following Stroke
Cognitive impairment is common following stroke and constitutes a substantial worldwide health burden that affects psychological well-being and independence in activities.37,38 The indirect effects of cognitive impairment on stroke recovery include reduced participation in rehabilitation and poor adherence to treatment guidelines. 38 While prevalence estimates vary due to study-specific differences (see Brainin et al 37 ), it is estimated that between 30% and 80% of all stroke survivors demonstrate some form of cognitive impairment, ranging from mild cognitive impairment in a single cognitive domain, to poststroke dementia. 39 Alarmingly, however, the prediction of cognitive impairment poststroke remains suboptimal, with limited evidence regarding which factors might dampen or facilitate this relationship. 40
Unsurprisingly, most evidence for cognitive reserve in stroke has used cognition as a primary outcome (see Table 2 for an overview of study characteristics and measures), in line with the original hypotheses set out by the cognitive reserve theory (see Figure 3 for a hypothesized model of cognitive reserve). For example, 2 important longitudinal studies reported that cognitive reserve (operationalized as years of education) preserves global cognition 28 and memory 41 poststroke and reduces the development of poststroke aphasia and dementia 41 independently of socioeconomic status (SES) in those with mild-to-moderate ischemic stroke. 41 Similarly, a recent cross-sectional study 42 demonstrated that those with higher cognitive reserve (operationalized as years of education) had significantly less cognitive deficits and functional disability (lower modified Rankin Score [mRS]) in the acute setting poststroke after statistical adjustment for age and lesion load. This study is particularly important as it includes a measure of stroke pathology (quantified as age and lesion load), in line with our conceptual model of cognitive reserve assessment (see Figure 2). Likewise, an autopsy study 43 that assessed a range of neuropathologic indices found that even very little educational attainment (M years = 3.9 ± 3.5) significantly modified the relationship between lacunar infarcts (quantified stroke pathology) and cognitive ability prior to death, independent of SES and other pathologies. This study provides compelling evidence for the cognitive reserve hypothesis by demonstrating that educational attainment (as a cognitive reserve indicator) independently modifies the relationship between pathology and outcomes.
Summary of Study Characteristics for Studies Assessing the Impact of Cognitive Reserve on Cognition in Stroke Populations.
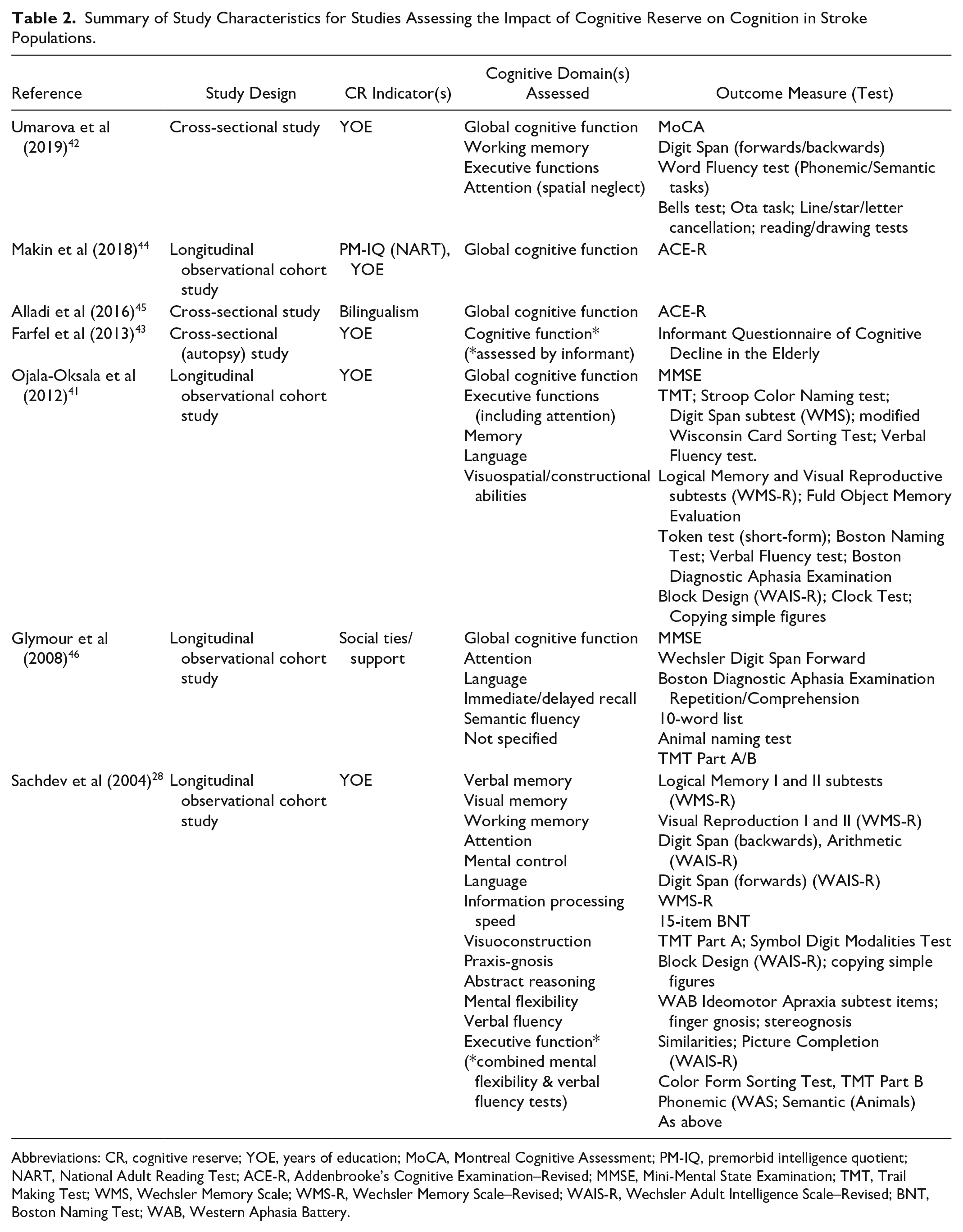
Abbreviations: CR, cognitive reserve; YOE, years of education; MoCA, Montreal Cognitive Assessment; PM-IQ, premorbid intelligence quotient; NART, National Adult Reading Test; ACE-R, Addenbrooke’s Cognitive Examination–Revised; MMSE, Mini-Mental State Examination; TMT, Trail Making Test; WMS, Wechsler Memory Scale; WMS-R, Wechsler Memory Scale–Revised; WAIS-R, Wechsler Adult Intelligence Scale–Revised; BNT, Boston Naming Test; WAB, Western Aphasia Battery.
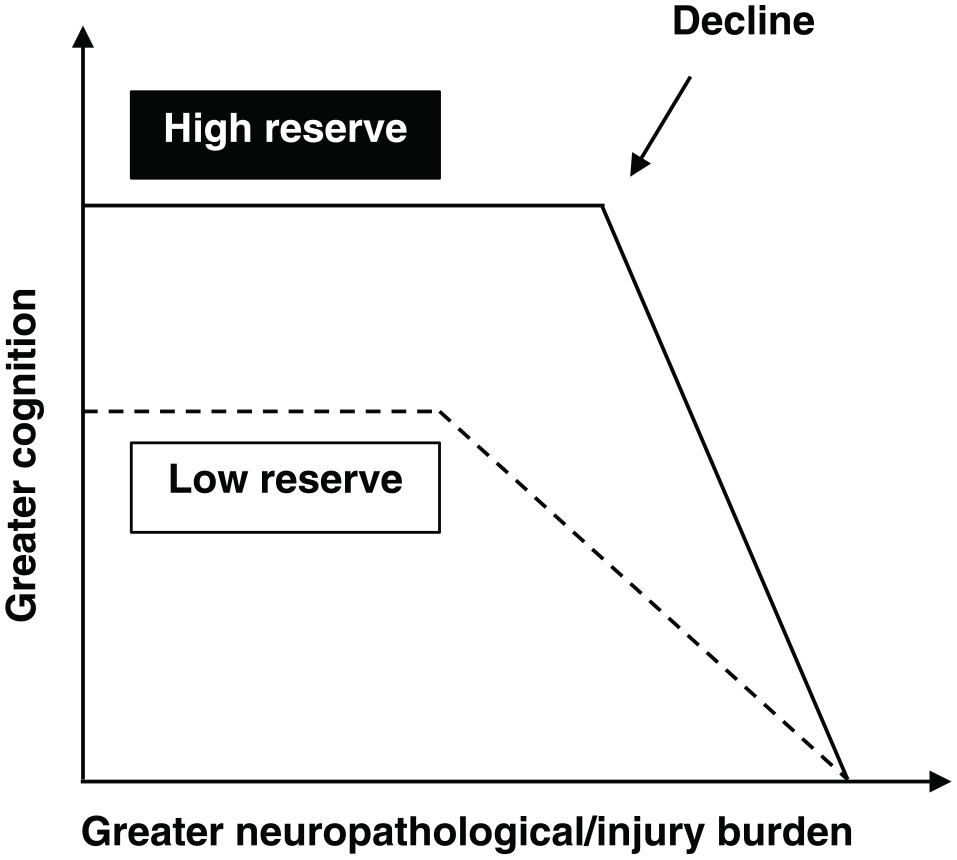
Hypothesized change in cognition over time as neuropathological/injury burden increases in those with high and low cognitive reserve (adapted from Stern 20 ). Those with higher cognitive reserve can withstand the effects of neuropathology or injury for longer without experiencing a decline in cognitive performance but decline faster as a result. The point of inflection (decline) occurs only after a critical threshold has been reached (ie, neuropathology or injury burden becomes so prominent, that the brain can no longer cope).
Other studies have demonstrated that both premorbid intelligence and years of education were associated with cognition poststroke. 44 Premorbid IQ was reported to be a stronger predictor of post-stroke cognition than vascular risk factors or stroke severity, suggesting that the variable should be considered in studies assessing cognition poststroke. Additionally, those with lower educational attainment had higher cognitive impairment at follow-up and were typically more functionally dependent (higher mRS) 1-year poststroke. Although the authors do not claim to have measured cognitive reserve, nor do they consider the relevance of their findings in the context of cognitive reserve, educational attainment and premorbid IQ are the most robust indicators of cognitive reserve to date. 17 Despite the lack of a comprehensive, multi-indicator cognitive reserve assessment and the study population being of milder stroke severity, this study highlights the predictive value of cognitive reserve for stroke impairment and recovery.
Finally, 2 studies took a less conventional approach to measuring cognitive reserve in stroke populations, by operationalizing the construct using indicators of bilingualism and social integration. Bilingualism as a cognitive reserve indicator has received extensive investigative attention in aging and neurodegeneration, 47 but little attention in stroke. One study with people with ischemic stroke found that a larger proportion of bilinguals (more than twice as many), compared with monolinguals, had intact cognitive function measured poststroke. 45 The cognitive and neural mechanisms of the “bilingual advantage” remain hotly contested, but include enhanced executive functioning, cognitive flexibility, and greater microstructural properties of white-matter pathways in regions supporting executive control relative to comparable monolinguals.48,49 Last, a novel study sought to determine whether social integration alters the course of cognitive recovery following stroke. 46 Baseline social ties and emotional support independently predicted cognition at 6 months poststroke and greater cognitive improvement from baseline to 6-month follow-up. The authors theorized that greater social ties might be an indicator of cognitive reserve that protects against cognitive impairment following stroke.
Cognitive Reserve and Disability Burden, Mortality, and Activities of Daily Living Following Stroke
Successful motor recovery and reduced disability following stroke is crucial for functional independence, safe performance of activities of daily living, and quality of life. 50 However, accurately predicting motor impairment, disability and an individual’s capacity for motor recovery following stroke is notoriously difficult. 51 Clinical assessment of motor impairment severity, genotyping, and the identification of molecular, neurophysiological, and neuroimaging biomarkers of structural (eg, Stinear et al 5 and Bigourdan et al 52 ) and functional network integrity (eg, see Grefkes and Fink 53 ) have increased the accuracy of predictive models.3,5,54 More specifically, differences in stroke-specific factors such as lesion location and the residual integrity of the CST seem to be particularly important in mediating motor impairment, disability and recovery following stroke. 51 However, even the “best” predictive models fail to fully explain the inter-individual variability observed clinically. This suggests that there is a proportion of physical/disability-related impairment and recovery that remains unexplained and unaccounted for in current prognostic models of outcomes and recovery. This difference might partially reflect differences in cognitive reserve and thus the ability of an individual to compensate for the injury. 11
A series of population-based, longitudinal cohort studies including 3804 people with mild-to-moderate ischemic stroke suggests that cognitive reserve is an important, independent mediator of activity-based impairment and outcomes poststroke.9,41,55-57 Those with higher cognitive reserve (operationalized as educational or occupational attainment) showed significantly higher odds of experiencing reduced disability, 56 functional burden (activities of daily living),9,57 fatigue, 57 and depression 57 following stroke. Last, higher cognitive reserve (operationalized as educational attainment) has also been independently associated with reduced long-term mortality, even after adjustment for age, sex, marital status, stroke severity, and white-matter lesions. 41 Interestingly, no association between cognitive reserve and cardiovascular risk factors (eg, hypertension, atrial fibrillation) and comorbidity burden was found in this study, highlighting the importance of cognitive reserve as a potential independent moderator of outcome and adverse clinical effects following ischemic stroke.
Cognitive Reserve and Language Deficits Following Stroke
Language deficits such as aphasia affect approximately 20% to 40% of all people with stroke, 58 and negatively affect health-related quality of life. 59 A cross-sectional study 60 found that cognitive reserve (operationalized as educational attainment) was associated with significant reductions in the severity of language impairment following stroke, independently of age, sex, stroke volume, and SES. More specifically, higher cognitive reserve was associated with reduced errors on language tasks including written spelling to dictation, oral spelling to dictation, and written naming. Modest but significant associations between cognitive reserve and reduced errors were also found for auditory and written word comprehension, and oral reading of words and pseudowords. These results suggest that cognitive reserve might provide partial protection against (mostly) written language impairment following stroke. However, a limitation of this study is that the authors did not account for structural damage to the anterior arcuate fasciculus, an important, well known and extensively studied white-matter fiber tract, which, if damaged, is highly predictive of aphasia.8,61 Thus, replication of these findings after consideration for anterior arcuate fasciculus damage is required.
Cognitive Reserve and Psychological Well-Being Following Stroke
Less work has focused on understanding the role of lifestyle-related predictors on psychological outcomes following stroke, despite poststroke depression being common and associated with poor recovery. 62 We found no studies that directly assessed the impact of cognitive reserve (defined a priori) on psychological outcomes poststroke, but studies that have investigated the impact of prominent cognitive reserve indicators (ie, education) might shed light on the applicability of cognitive reserve to mood. It is, however, important to note that mood disturbances (most commonly, depressive symptoms) often co-occur with poststroke impairments (eg, cognitive impairment) and are likely inter-related. 36 A recent systematic review and meta-analysis 63 of 33 studies with 2664 participants reported a significant association between low education (<8 years) and poststroke depression in studies where depression was defined as a score of mild and above on a depression rating scale (eg, Beck Depression Inventory) (odds ratio [OR] 1.47, 95% CI 1.10-1.97, P < .01), but not when depressive symptoms were defined as severe or given a clinical diagnosis of major depressive disorder (OR 1.04, 95% CI 0.90-1.31, P = .60). While being less educated was also associated with increased risk of experiencing poststroke depressive symptoms (mean difference [MD] 0.68, 95% CI 0.05-1.31 P = .04), a stark heterogeneity in outcomes across studies and large confidence intervals were noted, with additional research needed to reach sound conclusions.
Discussion
The Significance of Cognitive Reserve for Stroke Impairment and Recovery: Practical and Clinical Utility
Cognitive reserve demonstrates clear applicability to stroke-related impairment and recovery worthy of further investigation. Exploring the role of cognitive reserve in stroke is significant for many reasons, which fall largely into 4 categories: (1) reduced burden of disability poststroke; (2) health promotion, intervention, and secondary prevention of cognitive impairment; (3) translation into clinical practice; and (4) more accurate prediction and prognosis of outcome and recovery, clinical decisions, and trial stratification.
Reduced Burden of Disability Poststroke
The global incidence/burden of stroke is increasing and set to drastically rise due to substantial ageing of the population.64,65 Cognitive reserve demonstrates great promise in reducing the burden of disability as a result of stroke, particularly because it is proposed to be modifiable across the lifespan. 20 Although cognitive reserve is likely one of many factors that contribute to reduced impairment following stroke, the concept might, at least in part, provide substantial protection against the impact of stroke on cognitive and behavioral abilities (see Nunnari et al 66 ), by facilitating a “reserve-preserve” relationship. That is, the higher an individual’s cognitive reserve, the better preservation of neural resources and cognitive and behavioral abilities one might expect. To decrease the global burden of disability as a result of stroke, future research should focus on improving understanding of major determinants of poststroke disability (particularly those that are modifiable and easily targeted, such as cognitive reserve) and causes of disparity and heterogeneity across individuals with similar clinical characteristics. 65
Health Promotion, Intervention, and Secondary Prevention of Cognitive Impairment
The results of this review provide further evidence for the need to engage in a brain-healthy lifestyle and protective activities, such as educational and occupational pursuits, and physical, cognitive, social, and leisure activities, throughout the lifespan. Interestingly, engagement in certain activities in different life stages (eg, in early-, mid-, and late-life) demonstrate differential effects on cognitive reserve development. Activities could, theoretically, be tailored to healthy or at-risk adults of all ages in health promotion campaigns and/or interventional trials aimed at “boosting” cognitive reserve to reduce brain impairment or secondary cognitive impairment as a result of stroke or other neurological diseases, such as Alzheimer’s disease. For example, childhood cognitive ability has been shown to independently influence adult cognition and cognitive reserve as measured by the National Adult Reading Test, 67 whereas physical and social activity in late-life partly mitigates the development of dementia. 68 Additionally, engaging in lifestyle activities in mid-life has been shown to be protective of late-life cognitive ability and structural brain health and integrity, independent of other cognitive reserve indicators such as education, occupation, and late-life activity, by increasing both cognitive and brain reserves, respectively. 69
Thus, rather than an entity that is fixed during development and remains static across the lifespan, cognitive reserve represents a dynamic aging process, with crucial implications for cognitive (and potentially motor and psychological) function in later life, 67 as well as before, during, and after neurological disease or injury. Cognitive reserve is thus a prime candidate for intervention in healthy and neurologically impaired populations, because it continues to develop with age, irrespective of pathological or injury burden. If individuals are adequately enabled to modify their cognitive reserve, depositing into their “brain bank” by pursuing complex mental activities across their life span, this might serve as valuable currency in the face of stroke or other neurological diseases. In particular, innovative approaches to increase cognitive reserve and reduce vascular- and lifestyle-related risk factors linked to stroke could be the target of self-management programs or novel e-health applications aimed at risk reduction. 37 Additionally, strategies to increase or maintain cognitive reserve before and/or following acute injury might help prevent exacerbated cognitive decline, including post-stroke cognitive impairment, or the manifestation of dementia. Dementia occurs in approximately 10% and 34.4% of first-ever mild and severe stroke survivors, respectively, within the first year poststroke, and in around 30% of stroke survivors after recurrent stroke.39,70,71 In fact, evidence suggests that those with higher cognitive reserve (higher educational attainment) are at a decreased risk of developing dementia following stroke and/or transient ischemic attack (see Mirza et al 71 and Malsch et al 72 ). It should also be mentioned that brain reserve might also be a suitable target for intervention. Physical activity, including aerobic exercise and strength training, has been shown to increase brain volume 73 and preserve cognition, 74 in healthy but inactive agers, 73 as well as people with stroke, 74 suggesting that brain reserve is more modifiable than previously thought. Future research should explore the benefits of combining aerobic exercise and/or strength training with a cognitive reserve “boosting” intervention on outcomes and recovery following stroke. Aerobic exercise and/or strength training in conjunction with a cognitive reserve “boosting” intervention might demonstrate synergistic or complementary treatment effects above and beyond standalone physical or cognitive interventions (eg, Bo et al 75 and Ploughman et al 76 ). However, the amount, sustainability, and maintenance of a brain and/or cognitive reserve “boosting” intervention, and which cognitive reserve factors would facilitate the greatest protection against impairment or decline remains unknown. Additionally, it should be noted that cognitive reserve “boosting” activities are highly correlated over the life course, 77 meaning that the most effective interventional strategies are likely those that emphasize risk reduction and prevention throughout the entire life course (comprising early-, mid-, and late-life), 77 not just prior to or immediately following disease/injury onset.
Intervention and longitudinal studies will be crucial to define when and how we can increase cognitive reserve, what cognitive reserve determinants are most important in providing protection in which clinical domains (eg, cognition vs motor function) and the magnitude of their protection, and the true extent to which cognitive reserve is modifiable, 78 particularly after injury. Although it is acknowledged that there are major barriers and costs to implementing population-wide health promotion or intervention strategies, 79 public policy should continue to promote universal education and support the maintenance of physically, mentally and socially enriched lifestyles into advanced age. While cognitive or physical training in late-life may not add appreciably to the cognitive reserve built over a lifetime, it is clear that the social isolation and unstimulating, sedentary environments experienced by many elderly, oftentimes in aged-care facilities, are capable of negatively impacting brain health. 80
Cognitive Reserve Measurement: Ease and Challenges of Translation Into Clinical Practice
Cognitive reserve is typically operationalized using one or more proxy variables thought to indirectly represent the construct (eg, engagement in complex mental activities) (see Table 1). Many proxies have been used to measure cognitive reserve previously, with distinct advantages and disadvantages noted for each approach. However, one of the most practical, informative, and psychometrically sound approaches is the use of multi-indicator cognitive reserve questionnaires, which can be administered quickly and easily at the bedside or over the telephone (where possible). Additionally, certain questionnaires, such as the Cognitive Reserve Index questionnaire (CRIq), 81 are available freely online and can be completed by proxy. Thus, the use of validated, multi-indicator cognitive reserve questionnaires, are highly recommended for use in clinical practice.
More Accurate Prediction and Prognosis of Outcome and Recovery, Clinical Decisions, and Trial Stratification
A major clinical challenge in the field of stroke rehabilitation and recovery concerns our ability to understand an individuals’ capacity or potential for recovery. 3 Cognitive reserve is likely one piece of the puzzle capable of complementing existing measures to help characterize or determine the trajectory of recovery following a condition as complex as stroke. Clinicians might find utility in using simple measures of cognitive reserve in concert with stroke severity ratings to gather greater insight into the prognosis for, and recovery of, neuropsychological and motor abilities or disability. It is imperative that the methods used to make predictions, particularly in the acute stroke setting, are simple and inexpensive. 82 Likewise, additional alternatives to stroke severity are needed to help guide clinical decisions and rehabilitation planning poststroke. 83 Cramer et al 84 identified 8 specific issues related to stroke rehabilitation and recovery that need to be addressed to move the field forward. One of the most relevant recommendations concerns the need to characterize intersubject differences that might affect treatment and rehabilitation response. A method that incorporates information regarding stroke severity, location, and impairment, as well as an estimate of premorbid functioning and engagement (ie, cognitive reserve), might be a more accurate, holistic, and person-centered approach. 83 An evaluation of cognitive reserve might provide clinicians in the acute stroke or post-acute rehabilitation setting with an easily measurable, additional tool to identify those at higher risk of cognitive (or potentially activity based) impairment. An assessment of cognitive reserve prior to discharge to postacute rehabilitation would provide crucial information regarding individual attributes and prior capacity and help define cognitive reserve profiles to optimize rehabilitation and training interventions. 85 This information could be used to help design and implement more appropriate rehabilitation plans, based on predicted susceptibility to deficits and the level of premorbid functioning to which a patient can realistically be expected to return. 83
Another recommendation from Cramer et al 84 concerned the need to better target and appropriately stratify patients into subgroups for treatment and clinical trials, to reduce intersubject variability. Stroke-specific and demographic factors, such as infarct location and volume, age, sex, and vascular risk factors introduce large intersubject variability in treatment response and recovery.6,7,9,10,86 However, premorbid factors such as cognitive reserve might also contribute to variability in therapeutic and rehabilitation response. A mismatch in cognitive reserve across study groups could lead to differences in outcomes and recovery that have nothing to do with the intervention or treatment of interest. 20 Thus, one approach might be to stratify patients into clinical trial groups according to their level of cognitive reserve at the point of study design and/or data analysis, in an attempt to better control for intersubject variability.
Limitations, Future Directions, and Conclusions
There are several limitations to this review. One common problem across studies is the gap between the conceptualization of cognitive reserve as a dynamic feature of brain function capable of moderating the effects of injury on performance and its operationalization as a static proxy (eg, educational attainment). Direct measures of cognitive reserve are currently unavailable, 21 and most studies included in this review used only a single proxy (eg, educational attainment) to operationalize cognitive reserve. It is thus unclear whether the results of these studies truly support a “cognitive reserve” hypothesis or represent other mechanisms through which socioeconomic markers affect health outcomes, including differences in health behaviors, vulnerability to stressors, and social support. 87 As a major marker of socioeconomic status, educational attainment is associated with access to resources to maintain good health and person-specific differences in the ability to prevent or manage chronic conditions (eg, hypertension) linked to accelerated cognitive aging and poor health outcomes. 21 Additionally, results might be confounded by the fact that education, a marker for both socioeconomic status and cognitive reserve, influences access to, and the quality of, stroke care, including access to specialized stroke units 88 and acute interventional therapies such as thrombolysis and thrombectomy, 89 thereby inadvertently affecting outcomes. The operationalization of cognitive reserve via the use of a single proxy (namely, years of education) is thus disadvantageous and an oversimplification of the construct. 21 Indicators are unspecific to the construct and likely linked to clinical and cognitive performance via multiple pathways, not just those claimed to represent cognitive reserve “mechanisms” (for a comprehensive discussion, see Jones et al 21 ). However, some studies took steps to overcome these limitations by measuring and statistically adjusting for SES-related factors capable of influencing health outcomes (eg, Booth et al, 28 Farfel et al, 43 and González-Fernández et al 60 ). These studies suggest that the role of cognitive reserve extends beyond just a socioeconomic effect and may provide more compelling evidence for the cognitive reserve hypothesis. Another limitation, which characterizes most of the studies included in this review, concerns the lack of neuropathological data and/or consideration for neuropathological burden. Given the challenges involved in acquiring neuropathological data, particularly in the acute stroke setting, many studies investigating cognitive reserve do not estimate the degree/severity of brain injury. However, a formal test of cognitive reserve theory should demonstrate that any given cognitive reserve indicator modifies the relationship between pathology (ie, infarct volume/location) and performance (ie, cognition), 25 in line with the concept’s original theoretical definition.11,16 It is also important to obtain neuropathological data as it is possible that the nature and location of the infarct could attenuate the neuroprotective benefits of cognitive reserve and deplete brain reserve. Thus, the acquisition of neuroimaging data to estimate the degree/severity of an infarct, and how it might influence the manifestation of cognitive reserve, is highly recommended.
Future studies should continue to assess the impact of cognitive reserve on stroke impairment and recovery, irrespective of injury burden (see Table 3 for a summary box of high-priority future directions). Future studies should use more comprehensive, well-validated cognitive reserve assessments and adjust for confounding SES-health markers (eg, access to resources, stress, life course factors). Researchers should also prioritize the acquisition and analysis of imaging data related to neurological injury burden/severity, perhaps initially by making use of routine clinical scans where possible (see Umarova et al 42 ) (see Table 3). These steps will help determine the true effects of cognitive reserve in moderating impairment associated with increased pathological burden. Other cognitive reserve indicators, including engagement in cognitive, physical, and social activity, have demonstrated additive and independent weighting on the cognitive reserve construct (eg, Ikanga et al 90 ), and should be investigated as markers of cognitive reserve in people with stroke. 66 The use of multi-indicator assessments and the development of novel cognitive reserve measurement methods (eg, Reed et al 91 ) might help reduce the confounding effects of SES-related factors, better address the gap between the conceptualization/operationalization of the construct and provide stronger support for the cognitive reserve mechanism. Additionally, many of the studies included in this review were cross-sectional, and longitudinal studies will be needed to assess the effects of different cognitive reserve indicators on the degree and trajectory of impairment and recovery following stroke. Likewise, intervention studies will be needed to define when and how we can increase both brain and/or cognitive reserve and the extent to which brain and/or cognitive reserve can be modified and maintained across the lifespan and following injury. 78 Last, additional work should continue to focus on understanding how cognitive reserve might provide an additional level of neuroprotection above and beyond the influence of other, well-known recovery predictors, as the neural mechanisms that underlie the reported associations remain relatively unexplored and are ill-specified. 92
Summary Box of High-Priority Future Directions and Recommendations for Research Exploring CR in Stroke Populations.
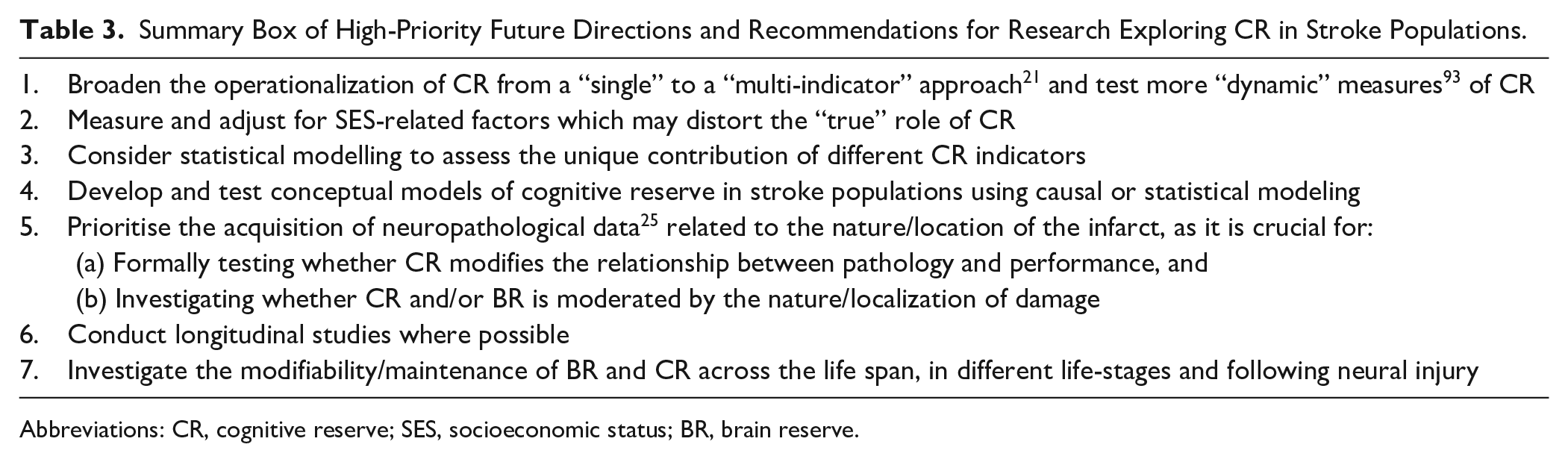
Abbreviations: CR, cognitive reserve; SES, socioeconomic status; BR, brain reserve.
In conclusion, although cognitive reserve is likely only one of many factors proposed to modify cognitive and/or motor impairment, disability, and recovery poststroke, the preliminary findings discussed in this review stress the importance of considering premorbid, life course–related characteristics (eg, cognitive reserve) when considering impairment and capacity for recovery poststroke.9,13,66 The role of cognitive reserve in facilitating reduced impairment and successful recovery from stroke represents an area of therapeutic promise and should be considered in future research and/or trials focused on understanding the nature and trajectory of impairment and/or recovery following stroke.
Supplemental Material
SupplementalMaterial_Appendix1 – Supplemental material for Cognitive Reserve as an Emerging Concept in Stroke Recovery
Supplemental material, SupplementalMaterial_Appendix1 for Cognitive Reserve as an Emerging Concept in Stroke Recovery by Emily Rosenich, Brenton Hordacre, Catherine Paquet, Simon A. Koblar and Susan L. Hillier in Neurorehabilitation and Neural Repair
Footnotes
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: ER is supported by a Research Training Program (RTP) scholarship (Australian Federal Government, Department of Education & Training) and a Commonwealth Scholarship for SA (Australian Federal Government, Department of Education & Training). BH is supported by a National Health and Medical Research Council (NHMRC) fellowship (1125054).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.