
Abstract
Background
Previous studies have compared the effectiveness of constraint-induced movement therapy (CIMT) by different training doses. However, whether the dosing schedule, that is, intensive or distributed, influences the effectiveness of CIMT in children with unilateral cerebral palsy (CP) is unknown.
Objective
To investigate the effectiveness of intensive and distributed CIMT for children with unilateral CP.
Methods
Fifty children with unilateral CP were assigned to intensive or distributed CIMT group with a total of 36 training hours. The intensive CIMT was delivered within 1 week, and the distributed CIMT was delivered twice a week for 8 weeks. The outcomes were the Melbourne Assessment 2, Box and Block Test, Pediatric Motor Activity Log-Revised (PMAL-R), Bruininks–Oseretsky test of motor proficiency 2, ABILHAND-Kids and Parenting Stress Index—Short Form. The intensive group was assessed at the initiation of treatment (week 0), at the end of 1 week treatment (week 1), and 8 weeks after the initiation of treatment (week 8). The distributed group was assessed at week 0 and week 8.
Results
The within-group analyses demonstrated significant differences on all motor outcomes. There were no significant between-group differences at post-treatment, while the intensive CIMT demonstrated larger improvements than the distributed CIMT did on quality of use of the more-affected hand, as rated by parents on the PMAL-R at week 8.
Conclusions
The 2 dosing schedules of CIMT had similar effectiveness for children with unilateral CP. The intensive CIMT yielded additional improvement on parent rated motor quality of the more-affected hand at 8 weeks after the initiation of treatment.
Trial registration:
ClinicalTrials.gov (ID: NCT03128385)
Abbreviations
CIMT: Constraint-Induced Movement Therapy
CP: Cerebral Palsy
MA2: Melbourne Assessment 2
BBT: Box and Block Test
PMAL-R: Pediatric Motor Activity Log-Revised
BOT2: Bruininks–Oseretsky Test of Motor Proficiency 2
PSI-SF: Parenting Stress Index—Short Form
HO: How Often
HW: How Well
ANCOVA: Analysis of Covariance
Introduction
Cerebral palsy (CP), defined as non-progressive motor impairment caused by a deficit of the developing brain, is a common pediatric physical disability, with a prevalence estimated to range from 1.9 to nearly 3 per 1000 live births.1,2 Hemiplegia, 1 type of CP, presents with unilateral deficits. Typically, the upper extremity is more affected than the lower extremity, with impairment of muscle tone, sensation, strength, endurance, and range of motion.3,4 These unilateral deficits discourage children with CP from using their more-affected hand spontaneously in routine activities and further affect their participation in daily life. 5
A number of promising therapeutic models have been reported for children with CP, including constraint-induced movement therapy (CIMT), hand-arm intensive bimanual therapy (HABIT), goal-directed therapy, hybrid therapy, and virtual reality.6 -8 Previous studies suggest that CIMT is an effective model for improving the use of the more-affected hand.7,9 The CIMT model is derived from behavioral neuroscience research with primates 10 and commonly combines principles of shaping and motor learning strategies. 11 Thus, the use of part and whole practice methods, modification of tasks, practice on functional activities, active problem solving, and optimal practice schedules have been implemented in CIMT. 12 The key ingredients of CIMT are restraint of the less-affected hand and intensive practice of the more-affected hand. 11 Under these principles, a variety of CIMT programs have been developed and the method of delivering the dosage of CIMT has been modified to enhance its clinical feasibility.9,11,13
Currently, there are 2 major ways of delivering the dosage of CIMT, namely, intensive and distributed programs.9,14 -16 Intensive CIMT delivers the intervention within a daily session last long, with high frequency and a short program length, while distributed CIMT delivers the intervention within a relatively shorter session duration, with lower frequency and a longer program length. The arrangement of the training schedule of intensive CIMT is compacted, while that of distributed CIMT is dispersed. Different training schedules can be adopted to fit different family routines. In addition, the intensive CIMT program is generally a camp-based design that delivers intervention-embedded activities in novel themes, which helps improve the children’s motivation and engagement.17,18 The distributed CIMT program, on the other hand, is more practical for establishing individualized goals and is easier to embed in family routines in a natural environment, which allows for the integration of intervention programs into their daily activities based on children’s personal preferences. 19 Regarding the dosing schedules, the duration in a single practice session, frequency, and program length of intensive and distributed CIMT are different, so comparison of their effectiveness is warranted.
The influence of dosing schedule has been addressed in few previous studies. Deluca et al 20 investigated the effectiveness of CIMT while controlling the program length and frequency (ie, 6 hours per day for 21 days vs 3 hours per day for 21 days). Both dosages demonstrated positive and similar effects; however, the influences of dosing schedule were blurred due to the disparity in total training hours. To control the same total training hours, the pilot study from Wu et al 21 investigated the dosing schedules of CIMT (40 training hours over 2 or 4 weeks) for children with CP who had received botulinum toxin injections. Brandão et al 22 compared the efficacy of HABIT in 2 dosing schedules (90 vs 2 × 45 hours). Although both studies have investigated the influence of dosing schedules under the same number of training hours for children with CP, they did not recruit sufficient sample sizes (N ≤ 3 per group) or did not focus on CIMT models. A study with a larger sample size investigating the influence of the dosing schedule of CIMT is required to fulfill the current knowledge gap.
The purpose of this study was to compare the treatment effectiveness of different dosing schedules of CIMT with the same total number of training hours. The total number of training hours was 36 for each program, which was beyond the minimum recommended dose of 30 hours. 23 Specifically, the programs of intensive CIMT (ie, 36 hours within 1 week) and distributed CIMT (ie, 36 hours over 8 weeks) were adopted. Under the equivalent training hours, the intensive CIMT was delivered within 1 week and the distributed CIMT was delivered over 8 weeks. To ensure the equality of the 2 programs, all intervention activities were provided by certified occupational therapists with the same therapist-to-child ratio (1:1). Response to treatment was assessed with the International Classification of Functioning, Disability and Health: Children and Youth Version (ICF-CY) to indicate the effectiveness of the dosing schedules on the body function and activity level. 24 The treatment effects with the same number of intervention hours (36 hours) and the treatment effects over the same period (8 weeks after treatment initiation) were investigated.
Methods
Study Design and Procedure
A quasi-randomized trial design was used. The a priori sample size was determined based on previous studies.14,25,26 Given an error probability of α = .05 and a statistical power of 0.8, the sample size estimates were 48, 32, and 44 for the MA2, the BBT, and the Pediatric Motor Activity Log-Revised (PMAL-R), respectively. As the required sample size ranged from 32 to 48, we proposed to recruit at least 25 children for each intervention group to compensate for dropouts. Children were enrolled by researchers who were not intervention providers or assessors. Children were assigned to the intensive or the distributed CIMT group according to the time when they enrolled in the study. Children recruited in January to June were assigned to the intensive CIMT group, and the others were assigned to the distributed CIMT group. The intensive CIMT program was conducted during 1 week of the children’s summer vacation, and the distributed CIMT program was delivered for 8 weeks after recruitment. Before and immediately after the treatment, outcome measures were assessed by trained occupational therapists in the evaluation room. To reduce bias, the assessors were blinded to the purpose, expected results, and treatment allocation of the study. The study was approved by the university ethics committee (201701011RINC) and was registered in the ClinicalTrials.gov Protocol Registration and Results System under number NCT03128385.
Participants
Participating children were recruited from the CP associations, medical centers, and special education systems. The inclusion criteria of this study were (1) age of 5 to 13 years, (2) diagnosis of unilateral spastic CP, and (3) apparent disuse of the more-affected hand in spontaneous contexts, as reported by participants’ caregivers, school teachers or therapists. The exclusion criteria were (1) excessive muscle tone (Modified Ashworth Scale ≥2) at any joints of the upper extremities before treatment initiation, (2) severe cognitive, visual, or auditory disorders according to medical documents, parental reports, or the examiner’s clinical observation, and (3) injections of botulinum toxin type A or operations on the upper extremities within 6 months of the treatment.
Interventions
The 2 key components of CIMT are restraint of the less-affected limb and intensive training of the more-affected upper limb. 11 Shaping and repetitive task practices were applied during the training sessions. Shaping is a training method in which a motor or behavioral objective is approached in small steps by successive approximations. Repetitive task practice involves functional tasks that are performed continuously over a specific period. To ensure that the intervention quality was equivalent between the 2 programs, each child was assigned to a trained therapist to maintain a therapist-to-child ratio of 1:1 for both programs. Therapists were asked to finish standard 4-hour training before delivering each intervention. The types of target training movements included reach, grasp, release, carry and hold, and manual dexterity. Activities were graded and modified by considering the child’s preference and performance of the more-affected limb. The total amount of training for each program was 36 hours. The major difference between these programs was how the dosage was delivered across the different durations, frequencies, and lengths of practice.
The intensive CIMT was delivered in a day camp with a group-based design (8-10 children) during the children’s regular summer vacation. The intervention camp, implemented in the classroom of the occupational therapy department, was arranged as an “Adventure Camp.” The treatment area was decorated as an adventure world, and each child was assigned the role of little warrior. The camp began with an opening ceremony to welcome the little warriors to a week of exploration and adventure. All upper limb activities were organized as a series of adventure-themed games.
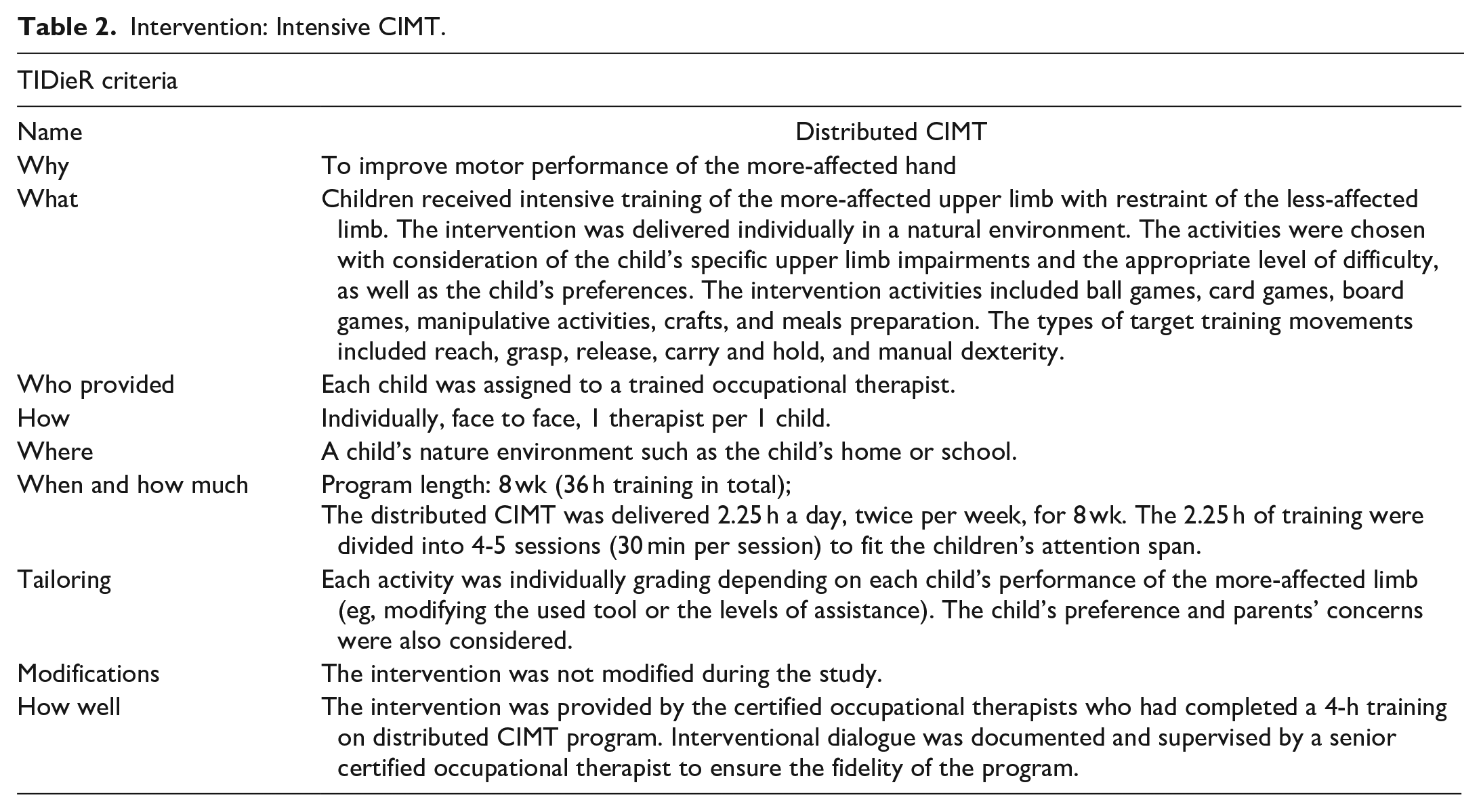
The distributed CIMT was delivered in a natural environment individually for 2.25 hours a day, twice per week, for 8 weeks. All activities were tailored and designed based on the child’s preference and parents’ concerns. The intervention took place in the child’s natural environment, such as home or school, allowing for the integration of training activities into their daily routines to increase generalization. The interventions were reported according to the template for intervention description and replication (TIDier) 27 and are shown in Tables 1 and 2.
Intervention: Intensive CIMT.
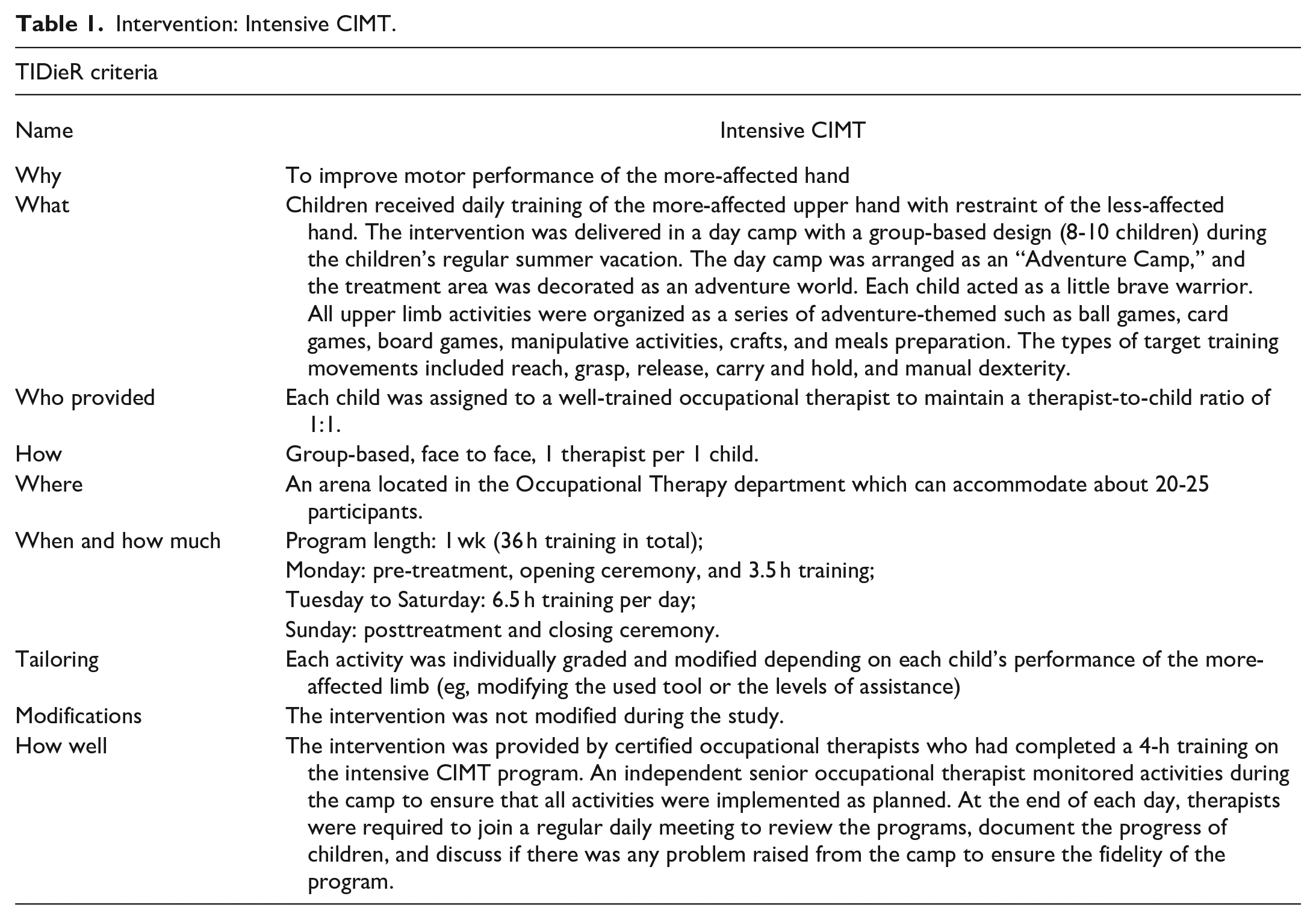
Intervention: Intensive CIMT.
Primary Outcomes
The primary outcome measures were focused on the child’s unilateral motor performance from objective and subjective perspectives. The Melbourne Assessment 2 (MA2), the Box and Blocks Test (BBT), and the Pediatric Motor Activity Log-Revised (PMAL-R) were used to present the comprehensive improvements in the body function and activity domains of the ICF-CY. The MA2 was developed to evaluate the quality of unilateral upper limb motor function in children with CP aged 2.5 to 15 years. 28 Each child was asked to perform 14 functional tasks, which were video recorded for subsequent scoring of 4 subscales. The 4 subscales included (1) amount of active range of movement at each upper limb joint; (2) accuracy of reach for or in place of a task; (3) dexterity of finger movements when grasping, releasing, and manipulating objects; and (4) fluency or smoothness of movement. The BBT assesses manual dexterity by counting the number of blocks that are transferred with a single hand from 1 compartment to another within 60 seconds. 29 In this study, the transferred blocks of the more-affected hand were counted. In addition, the PMAL-R, a parent-reported assessment, was used to capture the spontaneous use of the more-affected upper limb in 22 daily activities. 30 Each activity was rated by parents/caregivers on 6-point ordinal scales (0-5) with 0.5-point increments possible and on 2 subtests: how often (HO), for the amount of use of the more-affected hand, and how well (HW), for quality of use of the more-affected hand.
Secondary Outcomes
The secondary outcomes were focused on the child’s bilateral motor performance. The Bruininks–Oseretsky Test of Motor Proficiency, Second Edition (BOT-2) and the ABILHAND-Kids were used to present the improvements on the activity domain of the ICF-CY. The subtest 3 of the BOT-2, manual dexterity, was used to assess the children’s bimanual upper limb dexterity. 31 This subtest consists of 5 goal-directed activities that involve reaching, grasping, and bimanual coordination with objects. The ABILHAND-Kids questionnaire is a Rasch-based assessment that measures children’s difficulty in performing ADLs that require the use of the bilateral upper limbs from the caregiver’s perspective. 32 It contains 21 items measuring manual ability and is rated on a 3-point response scale (0-2). The score, given in logits, is the conversion of the ordinal score into a linear measure of ability located on a unidimensional scale. In addition, the Parenting Stress Index-Short Form (PSI-SF) was used to evaluate the stress level of the participant’s parents. 33 It includes 36 items rated from 1 (strongly disagree) to 5 (strongly agree). High scores on the PSI-SF indicated lower stress in the parent.
Time Points of Measurement
All participants were assessed before and after completing the intervention. For distributed CIMT, evaluations were administered at the beginning of treatment (week 0) and the end of treatment (week 8). For intensive CIMT, evaluations were administered at the beginning of treatment (week 0), at the end of treatment (week 1), and 8 weeks after the beginning of treatment (week 8). Specifically, to examine the immediate treatment effects of the same dose, the outcomes from week 1 of intensive CIMT and those from week 8 of distributed CIMT were compared (W1int vs W8dis). Furthermore, to examine the treatment effects while controlling for the children’s developmental periods, an additional comparison between the 2 groups at week 8 was implemented (W8int vs W8dis). The outcomes measured at identical time points (ie, 8 weeks after the treatment beginning) were compared to eliminate the influence of motor development caused by the difference in the lengths of the intensive and distributed programs.
Statistical Analysis
Analysis of covariance (ANCOVA) was used to examine the pre- to post-test changes in the outcome measures between the 2 groups while controlling for the baseline values. The paired t-test with Cohen’s d effect size (dav) was used to estimate the within-group differences.
34
To examine the immediate treatment effects under the same amount of training, the outcomes from week 1 of intensive CIMT (W1int) and that from week 8 of distributed CIMT (W8dis) were compared. To examine the post-treatment effects while controlling for the children’s development over the same amount of training, the outcomes from week 8 of intensive CIMT (W8int) and that from week 8 of distributed CIMT (W8dis) were compared. An effect size of partial
Results
Fifty children with unilateral CP were included (Figure 1). Half were assigned to the intensive CIMT group and the other half to the distributed CIMT group. Demographics and baseline clinical characteristics are summarized in Table 3. The manual ability and the upper limb muscle tone of unilateral CP were assessed with the Manual Ability Classification System 39 and the Modified Ashworth Scale, 40 respectively.
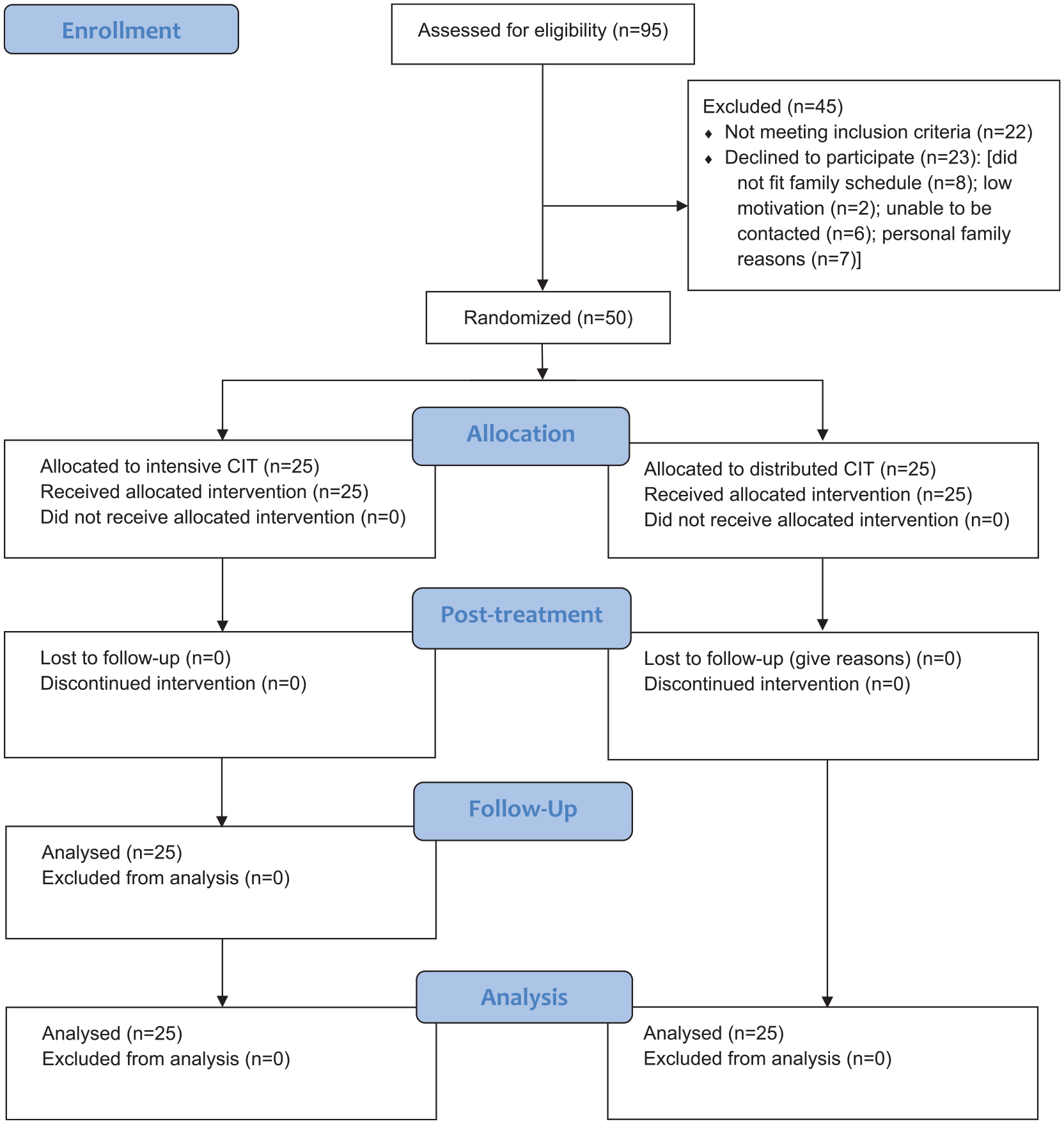
Description of Recruitment Following CONSORT Guidelines.
Demographics of the Study Participants.
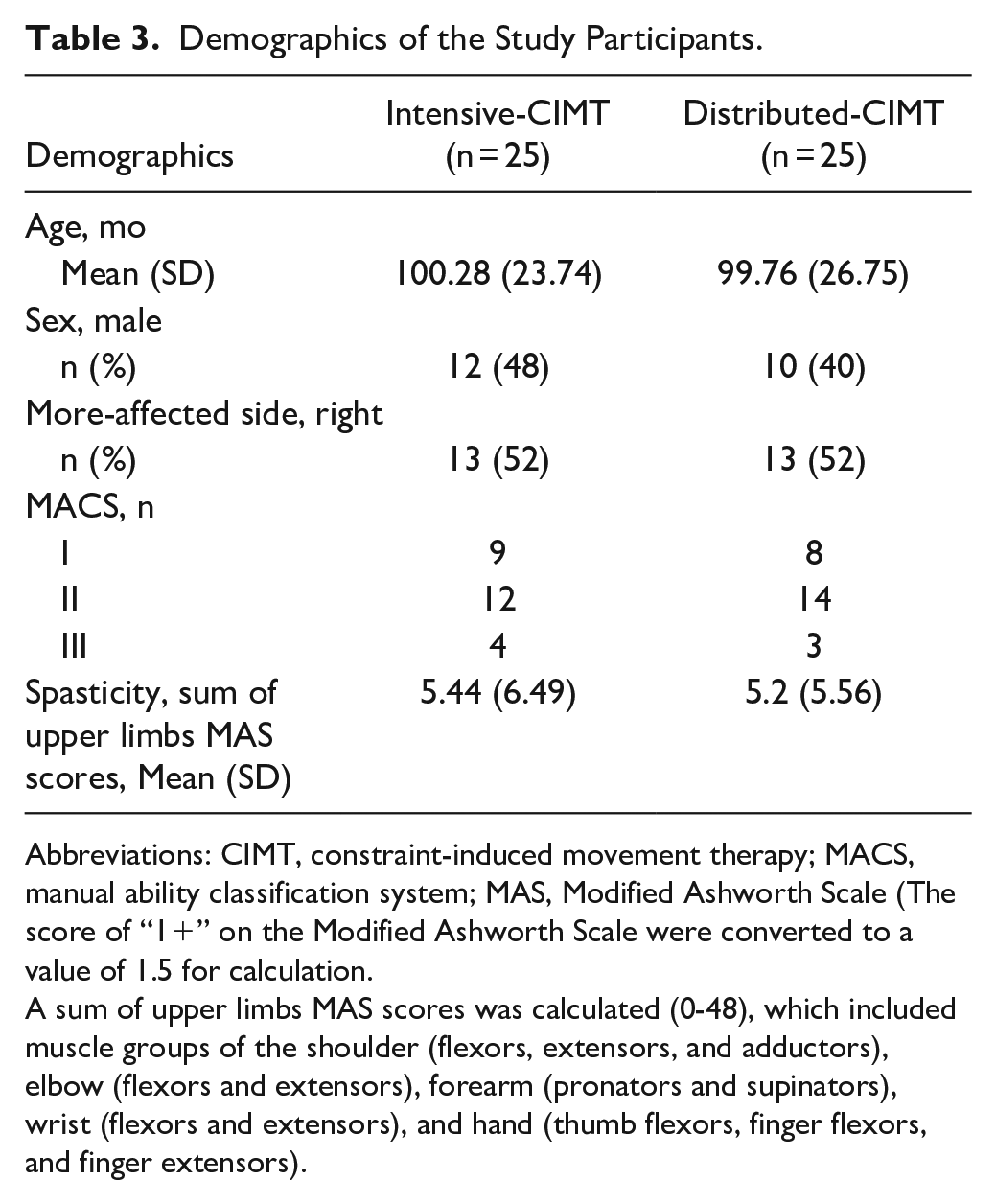
Abbreviations: CIMT, constraint-induced movement therapy; MACS, manual ability classification system; MAS, Modified Ashworth Scale (The score of “1+” on the Modified Ashworth Scale were converted to a value of 1.5 for calculation.
A sum of upper limbs MAS scores was calculated (0-48), which included muscle groups of the shoulder (flexors, extensors, and adductors), elbow (flexors and extensors), forearm (pronators and supinators), wrist (flexors and extensors), and hand (thumb flexors, finger flexors, and finger extensors).
Primary Outcome Measures
The within-group analyses demonstrated significant differences on all primary outcomes. As for the between-group analyses, there were no significant differences in the primary outcomes at the post-treatment comparison (W1int vs W8dis, P = .07-.89, Table 4). In addition, in the 8-week comparison of the intensive group and distributed group (W8int vs W8dis, Table 5), only the HW subtest of the PMAL-R showed a statistically significant difference between groups (P = .02, Table 4). No statistically significant differences were observed in the 4 subtests of the MA2, the BBT, or the HO subtest of the PMAL-R.
Primary Outcome Measures at Pre-treatment, Post-Treatment, and the 8-Week After Treatment Beginning.
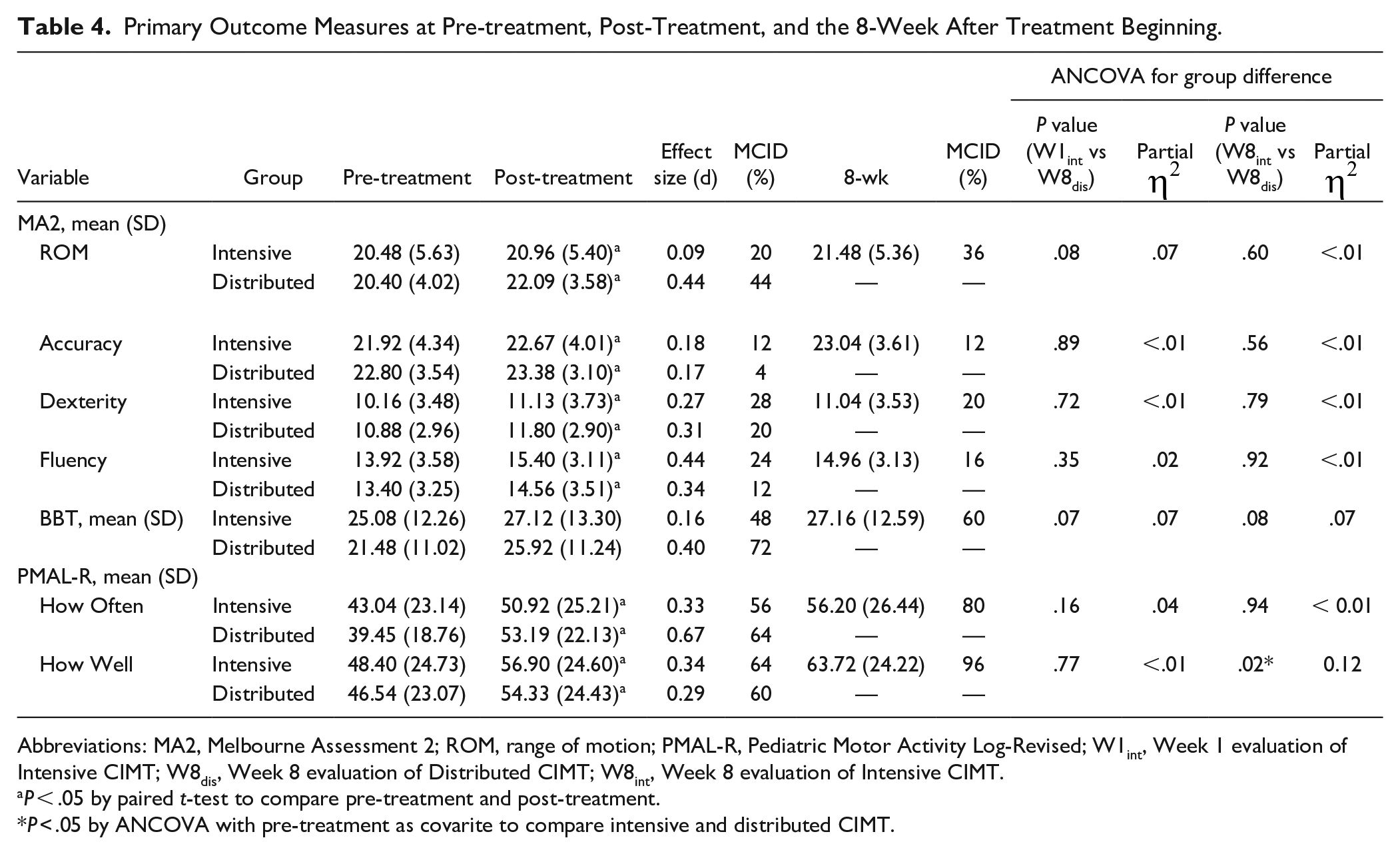
Abbreviations: MA2, Melbourne Assessment 2; ROM, range of motion; PMAL-R, Pediatric Motor Activity Log-Revised; W1int, Week 1 evaluation of Intensive CIMT; W8dis, Week 8 evaluation of Distributed CIMT; W8int, Week 8 evaluation of Intensive CIMT.
P < .05 by paired t-test to compare pre-treatment and post-treatment.
P < .05 by ANCOVA with pre-treatment as covarite to compare intensive and distributed CIMT.
Secondary Outcome Measures at Pre-treatment, Post-Treatment, and the 8-wk After Treatment Beginning.
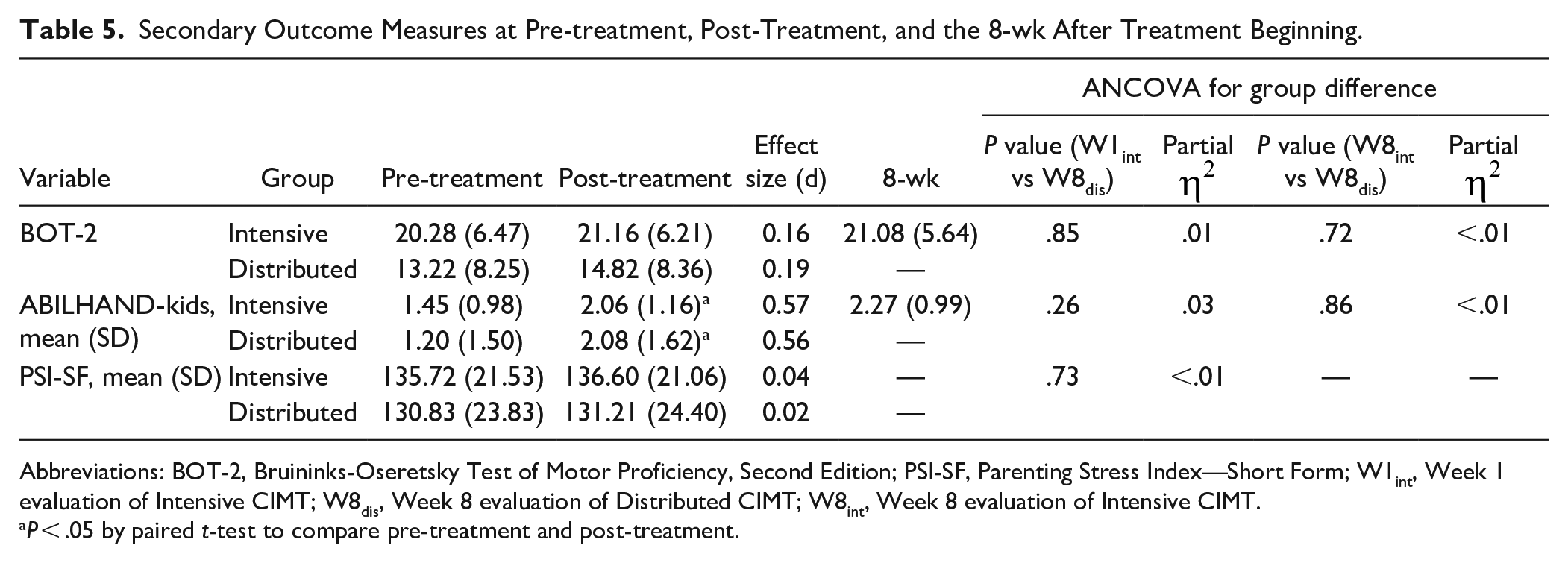
Abbreviations: BOT-2, Bruininks-Oseretsky Test of Motor Proficiency, Second Edition; PSI-SF, Parenting Stress Index—Short Form; W1int, Week 1 evaluation of Intensive CIMT; W8dis, Week 8 evaluation of Distributed CIMT; W8int, Week 8 evaluation of Intensive CIMT.
P < .05 by paired t-test to compare pre-treatment and post-treatment.
Secondary Outcome Measures
The within-group analyses demonstrated significant differences in bilateral motor performance as measured by the BOT-2 and the ABILHAND-Kids. In the between-group analyses, no statistically significant differences in the secondary motor outcomes were observed in any time point comparisons (Ps > .05, Table 5), indicating that the improvements on these motor outcomes were similar. In addition, the parents of the children in both groups were assessed with the PSI-SF at pre- and post-treatment to monitor the parents’ stress during our interventions. The results showed no significant increases in stress for either intervention (P = .73, Table 5).
Discussion
This study investigated the effectiveness of different dosing schedules for delivering CIMT, that is, intensive or distributed, in children with unilateral CP. To decrease potential bias in comparisons of the 2 dosing schedules, all intervention activities were provided by certified therapists with a therapist–child ratio of 1:1 and a dose of 36 training hours. Generally, there were no differences between the 2 programs immediately following intervention or at the 8-week follow-up period. However, the intensive CIMT demonstrated an additional benefit on parent-rated quality of use of the more-affected hand in daily activities, as measured by the PMAL-R at the 8-week comparison time point.
The intensive and distributed programs both led to significant improvements in motor outcomes, including motor capacity (as measured by the MA, BBT, and BOT-2) and daily use of the more-affected hand in unilateral and bilateral functional activities (as measured by the PMAL-R and ABILHAND-kids). In other words, both programs led to improvements in body function and activity domains of the ICF-CY after 36 hours of training. These findings were generally consistent with those of previous studies that confirmed the benefits of CIMT on motor performance. 9 It is noteworthy that the CIMT programs in this study offered a relatively lower treatment dose of 36 hours. The positive results not only provide cumulative evidence to support a minimum recommended dose of CIMT of greater than 30 hours 23 but also imply an increase in the clinical feasibility for school-aged children. Due to the busy schedules of school-aged children in Asian countries, conventional CIMT programs delivered with high frequencies over long program periods have frequently been targets of complaint. 41 This study arranged intervention schedules of twice a week for the distributed program and 1 week for the intensive CIMT program to fit the ecological features of local families’ routines. 14 The results indicated that all participants in this study completed 100% of the intervention hours and that parental stress levels remained stable. These findings are encouraging and even better than those of previous studies, which have reported increases in parental stress from CIMT programs.11,19,41 The favorable results may be explained by the strategy of providing a suitably arranged intervention schedule. Together with the comparable motor benefits, the tight adherence to the intervention protocol further supported the clinical friendliness and feasibly of the proposed CIMT programs.
In addition to the similar within-group improvements, there were no significant between-group differences in motor capacity or daily function immediately after the intervention. These findings indicate that the children in both groups demonstrated equal gains on multiple motor outcomes immediately after the 36-hour intervention. Specifically, for the same number of training hours, implementing CIMT in a distributed way (eg, 36 hours over 8 weeks) is as effective as implementing CIMT in an intensive way (eg, 36 hours within 1 week). This study provides preliminary evidence that the motor improvements were similar under the design of these 2 specific dosing schedules (1 week vs 8 weeks to deliver 36 hours training). The results have important implications for clinicians and clients; under these 2 schedules, they might have more flexibility in decision-making with regard to the delivery method to fit their preferences for family routines.
To provide compelling evidence on the differences between the 2 dosing schedules, this study also investigated the between-group differences at 8 weeks after the initiation of treatment. A difference in post-treatment effects with development controlled for was only found on the HW of the PMAL-R, demonstrating that the intensive CIMT program had additional benefits on parent reported quality of use of the more-affected hand in daily activities. These findings were in line with the clinical relevance point that improvements surpassing the MCID were achieved by 96% of the participants in the intensive CIMT and by 60% of the participants in the distributed CIMT. Combined with the finding of immediate post-treatment effects, this result might indicate that the children in the intensive CIMT group had immediate parent reported motor quality improvement within a short time (1 week) and that the improvement continued for 8 weeks. It is interesting that the HO of the PMAL-R, representing the frequency of use the more-affected hand in daily activities, did not demonstrate a similar result. These findings might support the above point that the habit of using the more-affected hand in children with unilateral CP can be improved obviously as soon as the training program is completed. Specifically, once the habit was established during the intensive training, the children kept practicing on daily activities by themselves and thereby had more potential to gain improvement on quality of use in activity domain. However, investigations of additional 8-week follow-up in the distributed program for integrating improvements into daily activities (ie, week 8 in intensive CIMT vs week 16 in distributed CIMT) are warranted in future studies.
Apart from the dosing schedule, the intervention environment could also contribute to the treatment effectiveness. A previous study that compared the impact of receiving CIMT in home and clinical settings found that outcomes favored the home program. 42 In the present study, the distributed CIMT (in a natural environment) and the intensive CIMT (in a day camp setting) demonstrated comparable immediate treatment effectiveness. This similarity might suggest that the impact of the environment difference on the implementation of the CIMT programs might be trivial. In addition, to reduce the influence of environment and focus on the dosing schedule, a therapist-to-child ratio of 1:1 was provided for both groups to ensure the quality of the programs. Further studies should be conducted to confirm the influence of environment on treatment effectiveness.
This study investigated the outcomes of upper limb motor rehabilitation under 2 different treatment dosing schedules: 36 hours over 1 week or 2 months. In the previous pilot studies, a study of HABIT by Brandão et al 22 demonstrated no difference between a 90-hour program and a 45-by-2-hour program, while another CIMT study by Wu et al 21 demonstrated a difference in effectiveness between 2 distributed programs (40 hours over 4 or 2 weeks). Although these 2 studies addressed the effects of dosing schedule, the preliminary findings still need to be validated with larger sample sizes, especially for CIMT. Thus, the present study implemented a quasi-randomized trial design with a relatively large sample size to strengthen and extend the current evidence on the comparison of different treatment dosing schedules.
Several limitations of this study need to be considered. First, it should be noted that the beneficial findings were achieved under strict conditions. All intervention activities were provided by therapists with a therapist-to-child ratio of 1:1. This design might challenge the cost-effectiveness of the intervention. Second, the Assisting Hand Assessment (AHA) is considered as a gold standard for estimating how effectively the more-affected hand is spontaneously used during bimanual tasks, but a certified training course is required for accessibility. Instead, we used both performance-based and questionnaire-based measures to estimate the unilateral and bilateral improvements of the more-affected hand. Comparisons of study outcomes with the AHA are suggested as future work. Third, conducting multiple comparisons might have led to potential biases, such as the increased type I error. Thus, the discussion was mainly focused on relatively robust patterns and results to avoid overinterpretation of the negligible findings. Fourth, this study did not investigate motor control strategies of kinematics, which are reported to be reliable and sensitive. 43 Future studies may consider the inclusion of kinematic analyses to broaden the understanding of motor outcomes. In this study, the quasi-randomized controlled trial, which allocated participants based on the order in which they were recruited, might have incurred bias due to time-dependency. A strictly randomized controlled trial design is suggested for future studies to validate our study findings.
Conclusions
Previous studies have compared the treatment effectiveness by different ages, different restraint methods, different total doses or different dosing schedules.11,17 This study provided further evidence to investigate the effectiveness of the CIMT under 2 dosing schedules, that is, intensive and distributed CIMT, with a larger sample size of children with unilateral CP. Both CIMT programs were under a total of 36 training hours with equal therapist-to-child ratios. The results of this quasi-randomized controlled trial demonstrated similarly positive findings for both dosing schedules, while the intensive CIMT yielded better quality of daily use of the more-affected hand at the 8-week evaluation time point. This finding indicated that the habit of using the more-affected hand in children with unilateral CP, once established, may lead to further gains on quality of use of the more-affected hand in daily activities.
Footnotes
Acknowledgements
The authors thank the children and their families for participating in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Science and Technology, Taiwan [grant number 107-2628-E-002 -004 -MY3 and 107-2314-B-002-049-MY3].