
Abstract
Background. Upper limb function plays a significant role in enhancing independence for individuals with tetraplegia. However, there is limited knowledge about the specific input of sensorimotor deficits on upper limb function. Thus the theoretical framework designed to develop the Graded Redefined Assessment of Strength Sensibility and Prehension (GRASSP) was used as a hypothetical model to analyze the impact of impairment on function. Objective. To define the association of impairment (sensation, strength, and prehension measured by the GRASSP) to upper limb function as defined by functional measures (Capabilities of Upper Extremity Questionnaire, Spinal Cord Independence Measure). Methods. A hypothetical model representing relationships by applying structural equation modeling was used to estimate the effect of the impairment domains in GRASSP on upper limb function. Data collected on 72 chronic individuals with tetraplegia was used to test the hypothetical model. Results. Structural equation modeling confirmed strong associations between sensation, strength, and prehension with upper limb function, and determined 72% of the variance in “sensorimotor upper limb function” was explained by the model. Statistics of fit showed the data did fit the hypothesized model. Sensation and strength influence upper limb function directly and indirectly with prehension as the mediator. Conclusions. The GRASSP is a sensitive diagnostic tool in distinguishing the relative contribution of strength, sensation and prehension to function. Thus, the impact of interventions on specific domains of impairment and related contribution on clinical recovery of the upper limb can be detailed to optimize rehabilitation programs.
Introduction
Upper limb function is integral to independence for individuals with traumatic tetraplegia; therefore, restoration of upper limb function is of great significance to this population. 1 The extent of recovery has a direct bearing on the functional independence of an individual.2-7
However, the relationship between impairment and functional status is not well established8,9 and a greater understanding of impairment and its role in upper limb function could provide valuable information to support clinical decision making, 10 such as treatment selection, prescription, and understanding the specific effects of interventions.
Development of the Graded Redefined Assessment of Strength Sensibility and Prehension (GRASSP) incorporated the specific impairment domains: sensation, strength, and prehension,11,12 which we hypothesized to contribute to upper limb function. It was conceptualized in the theoretical framework designed prior to the development of the GRASSP 11 (Figure 1) that all 3 domains play a role in upper limb function. However, the contribution of each component was unknown and where the intermediate relationships (integration) existed among impairment domains was not fully understood. Motor strength and its relationship to function is often documented, 13 but the distinct effects of sensation on function and upper limb recovery specific to tetraplegia remain underreported. The GRASSP falls into the International Classification of Functioning, Disability, and Health category of body structures and function. Although, prehension would typically fall into the activity category; the tasks are measured by “how” they are performed rather than “if” the tasks are performed and defines innervation to a greater extent. Thus, the developers consider the GRASSP to be an impairment measure. Sensorimotor upper limb function was defined as the construct for the GRASSP, and a theoretical framework (Figure 1A) was designed to guide development of the measure. The framework incorporated the concepts of motor control and motor learning theory, 14 which involve the interactions of the function (task), the individual, and the environment. 15 Task performance, which depends on integrated systems of sensation, motor, and cognition, was also incorporated. An integrated (prehension) component was added to assess how sensory and motor impairments contribute to an integrated function; this issue becomes increasingly important during the recovery process. When scoring is directed toward the quality and performance of movement (noting how the grasp is produced) more so than the ability alone (task performed or not), the results indicate which neurological elements are intact and or recovering. 11 The combination of the 3 domains is one of the novel qualities of the GRASSP and has not yet been presented in any previous upper limb measures. 16 The domains of GRASSP characterize the upper limb specifically, which allows clinicians and researchers to elucidate some of the endogenous recovery mechanisms related to hand function and to determine specifically the effects of interventions. Thus, GRASSP will be invaluable in establishing efficacy in new trials and translating emerging mechanisms of hand function from bench to bedside.
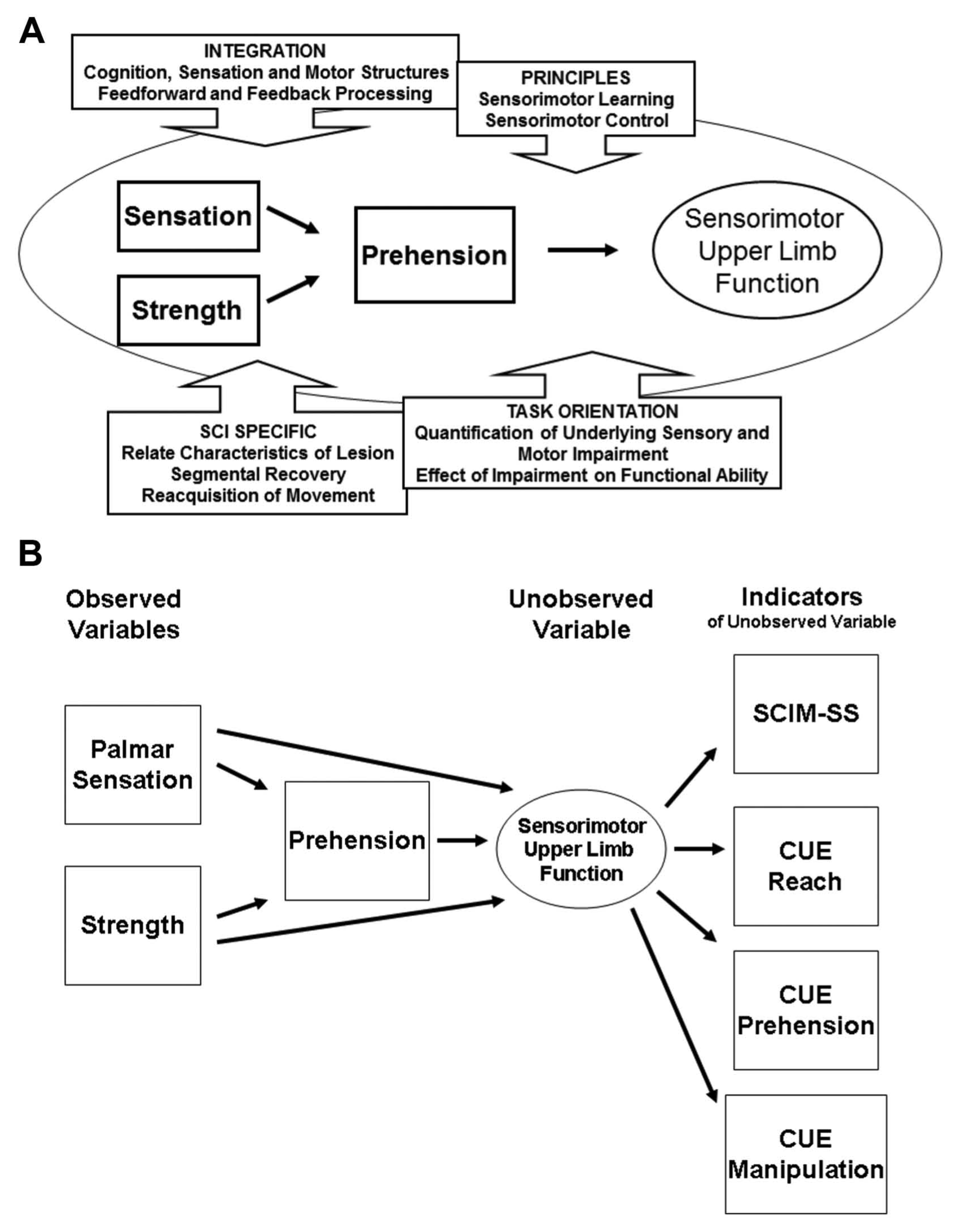
(A) Theoretical framework and (B) hypothetical model.
Two previous articles have reported on the development 11 and psychometric properties 12 of the GRASSP. The analysis in this article is conducted using the same data collected in the validation study. However, the aim here is to confirm the hypothesized relationships between the domains defined in the theoretical framework and measure with this cohort of data.
Specifically, the objective of this analysis was to determine the association between the impairment domains (sensation, motor, and prehension) and the construct of “sensorimotor upper limb function” 11 by testing the hypothetical model (based on the theoretical framework). The purpose of this analysis is to establish further insight into what GRASSP subtest scores define individually and collectively. For clinicians and researchers administering the GRASSP, these findings can define the change of impairment and how it affects function clinically. Furthermore, the elements of impairment that are influenced by mechanisms of recovery and interventions can also be identified using GRASSP.
Methods
Data were collected as part of the GRASSP validation study 12 where methods, data collection, and description of the sample are available. This article represents a second analysis performed with elements of the original data set collected for reliability and validity. Analysis was conducted with SPSS 17.0 and M-Plus 5.2.
Outcome Measures
The GRASSP is a multidomain impairment measure specific to the upper limb for individuals with tetraplegia. It consists of 5 subtests, palmar sensation and dorsal sensation measured by Semmes Weinstein Monofilaments, Strength of 10 arm and hand muscles measured by traditional motor grading, prehension activity, and performance measured by observation of grasping and task acquisition. Further details of the development, theoretical framework, and content are available in 3 published articles.11,12,16 The Spinal Cord Independence Measure (SCIM) 17 is a global measure of performance specific for individuals with spinal cord injury (SCI), used to define the function and independence of the sample in this study. Interrater reliability is greater than .8 when assessed by agreement statistics for most SCIM items, and intraclass correlation coefficient for the total score is .94. 18 Concurrent validity of the SCIM with the Functional Independence Measure (FIM) is .79. 18 Within the SCIM, there are 3 subscales (self-care, respiration and sphincter management, and mobility) and in this analysis the SCIM self-care subscale (SCIM-SS) was used as one of the representations of upper limb function. The SCIM-SS includes items solely related to the use of the upper limb; therefore, comparison between the GRASSP subtests are made with the SCIM-SS, rather than the total SCIM score. Subscales of the SCIM are reliable and useful quantitative representations of the specific constructs of independence in SCI.19-21
The Capabilities of Upper Extremity Questionnaire (CUE) is a subjective questionnaire that determines one’s perception of functional ability. The questions asked are related to one’s perception of how difficult a task may be. The CUE is embedded with questions that fall into the three components of upper limb function reaching tasks, prehension tasks, and manipulation tasks, scores for each task are added for a total CUE score. Psychometric properties of the CUE have been reported as .92 (Cronbach’s α) and .74 (Pearson correlation coefficient) for concurrent validity with the FIM. 22 GRASSP, SCIM, and CUE results collected during the same visit were extracted from the data set for the analysis of impairment and “upper limb function.”
Analytic Plan
During the development of the theoretical framework (hypothetical model, Figure 1A and B) we anticipated there would be a positive relationship between the impairment domains and upper limb function, specifically; strength would play a stronger role than sensation in upper limb function. Structural equation modeling (SEM) was selected as the method for analysis to test the hypothetical model, because it is a more robust method to analyze data. SEM has a specific sample size adequacy test based on the number of parameters being estimated in the model, thus we estimated only one parameter, the latent trait which could be managed with our data set (n = 72).
Structural equation modeling is a general approach to multivariate data analysis, used to study complex relationships among variables. It is used to describe directed dependencies among a set of variables and provides an opportunity to test models with multiple dependent variables and provides a value of both direct and indirect effects of all variables. SEM is a confirmatory technique that confirms a specified model23,24; our hypothetical model was based on the theoretical framework (Figure 1A). In SEM, a latent trait variable is defined and predicted by dependent variables 25 ; in the case of our model, “sensorimotor upper limb function” was the latent trait. The independent variables used were the palmar sensation subtest total score, the strength subtest total score, and prehension performance subtest total score, right side data only (see Table 1). Dorsal sensation and qualitative prehension are the remaining 2 subtests and were not used in the analysis as they are not as relevant to function as the selected 3 variables. 11 The SCIM-SS and CUE were the indicators of the latent trait. The data were then run through the model to determine how well the data fit the hypothesized model. The fit of the model is known as the “goodness of fit.”24,25 Statistics of fit determine how well the specified model (hypothesis) fits the actual data. A χ2 test is conducted to evaluate the overall model fit, which assesses the magnitude of discrepancy between the sample and fitted covariance matrices. A large χ2 with an insignificant value (where P < .05 is considered significant) indicates a good fit of the model. The χ2, although not the most rigorous index of fit, is used and often accompanied by other indices. The root mean square error of approximation (RMSEA) evaluates how well the model fits the population’s covariance and is sensitive to the number of estimated parameters in the model. A value less than .10 indicates a good fit. The RMSEA is used when the number of estimated parameters is low in the case of this model, only one parameter is estimated. The standardized root mean square residual (SRMR) is the square root of the difference between the residuals of the sample covariance matrix and the hypothesized covariance model. A value of less than .09 indicates a good fit. The SRMR is used when there are varying ranges of scales among indicators, which is the case in the model tested. The comparative fit index (CFI) accounts for the sample size, all latent variables are uncorrelated and compared to the sample covariance matrix with the null model. The Tucker–Lewis index (TLI) of fit is used when a small sample size is being analyzed and can point out a poor fit when other indices are pointing to a good fit. A value greater than .96 indicates a good fit for both of these indices. The CFI considers the small sample size and the TLI considers simple models. Thus, the selection of indices was specific to the model hypothesized.25,26 All hypotheses were examined simultaneously by specifying one structural equation model (Figure 1B). One latent variable of “sensorimotor upper limb function” was incorporated which brought several benefits to the measurement of variables in this model, hence the accuracy of its structural relations. 23
GRASSP Scoring Details Included in This Analysis (Subtest and Item Scores and Ranges).
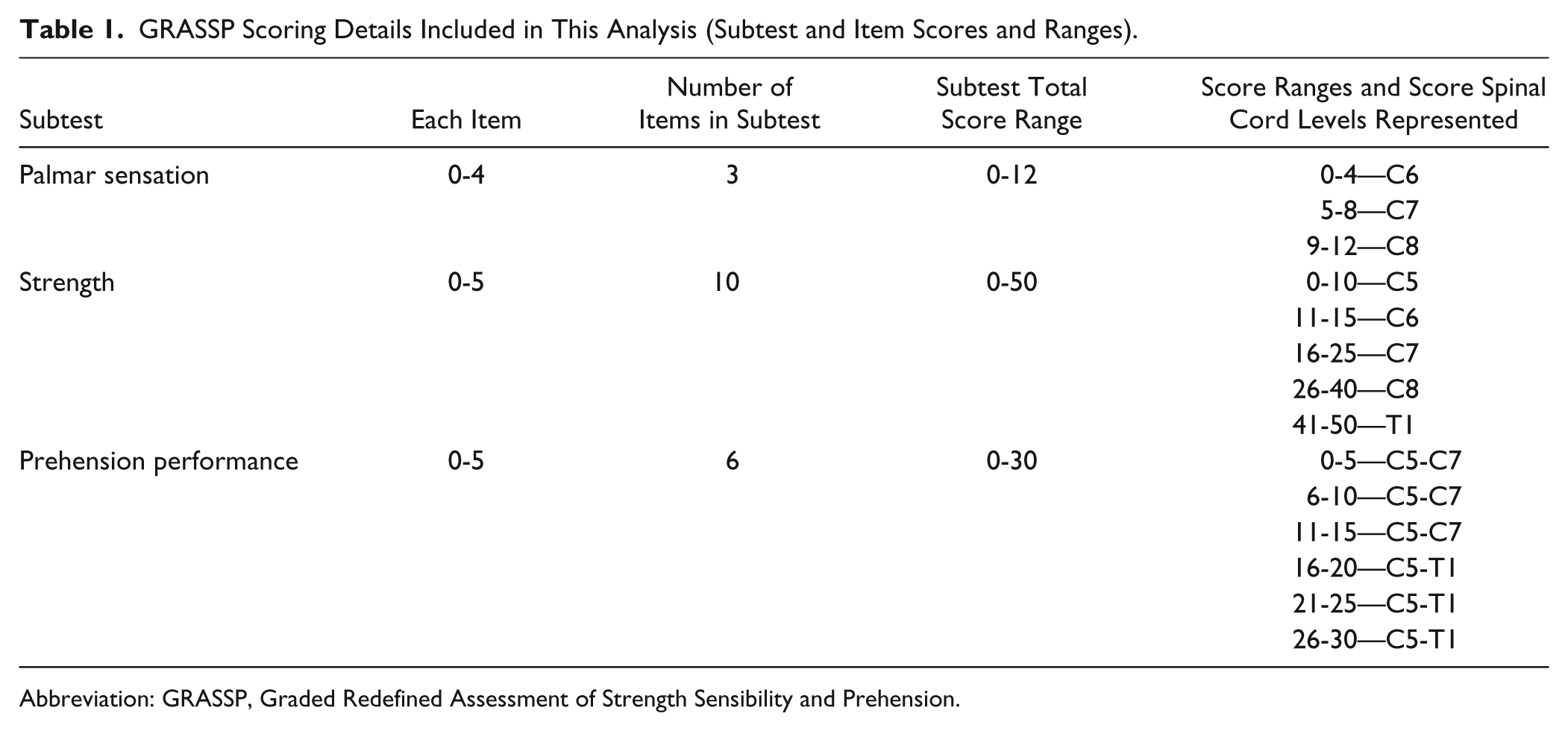
Abbreviation: GRASSP, Graded Redefined Assessment of Strength Sensibility and Prehension.
Figure 1B defines the hypothetical model for which SEM was conducted to determine the relationship of impairment to upper limb function. In SEM, it is necessary to establish a latent trait variable otherwise known as an unobserved value, which is estimated by observed variables. In this model, the latent trait variable was “sensorimotor upper limb function,” which was indicated by the SCIM-SS and the CUE component (reach, prehension, manipulation) scores. In SEM it is more reliable to have at least 3 variables to estimate the latent trait 26 ; therefore, the CUE was split into the 3 components (reach, prehension, manipulation) that represent upper limb function.15,27
Results
Sample
The data used in this analysis included a multicenter/multinational cross-sectional sample. The total sample consisted of 72 individuals with chronic tetraplegia ranging from 6 months to 20 years postinjury. Distribution of the sample according to the International Standards of Neurological Classification in Spinal Cord Injury (ISNCSCI)28,29 is defined in Table 2. Approximately 52.5% of the individuals presented with the C6-C7 motor levels whereas approximately 66% presented with C4-C6 sensory levels. According to AIS (American Spinal Injury Association Impairment Scale) classification, 39% (n = 28) of the sample were deemed to be AIS A complete, and 61% (B 25%, n = 18; C 19%, n = 14; D 17%, n = 12) of the sample as AIS B, C, or D incomplete.28,29 Complete details of the sample are available in the article that reports validation of the GRASSP. 12
Demographics Based on ISNCSCI Single Neurological Level (n = 72).
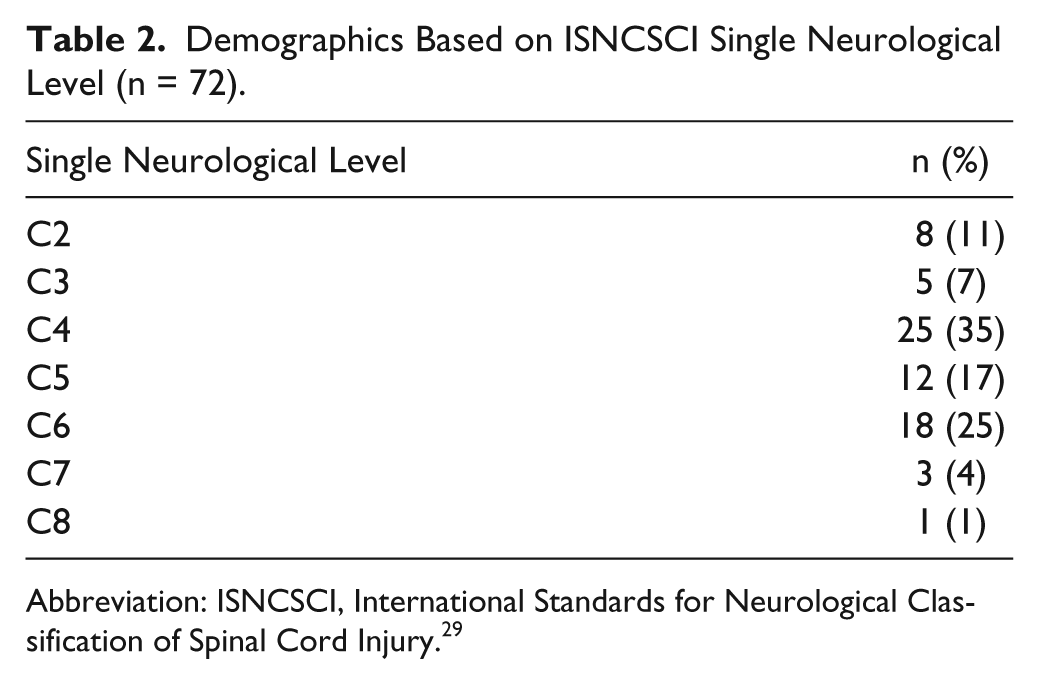
Abbreviation: ISNCSCI, International Standards for Neurological Classification of Spinal Cord Injury. 29
Structural equation modeling rendered the strength of association between impairment, function and the latent trait variable of sensorimotor upper limb function. Figure 2 shows the SEM results for the hypothetical model, which presents the effect of impairment on sensorimotor upper limb function. The SEM results show a very good fit of the model to the data; the model explained 72% of the variance in “sensorimotor upper limb function.” The very high value of R2 was substantiated by the goodness-of-fit indices. The goodness-of-fit indices were greater than the accepted thresholds (χ2 = 14.3, P = .11; CFI = .99, TLI = .97, and RMSEA = .09, SRMR = .02), which implies that the R2 value is reliable and the relationship among variables are also reliable. Prehension has a significant positive effect on upper limb function and strength and palmar sensation both have a direct and indirect effect through prehension on upper limb function.
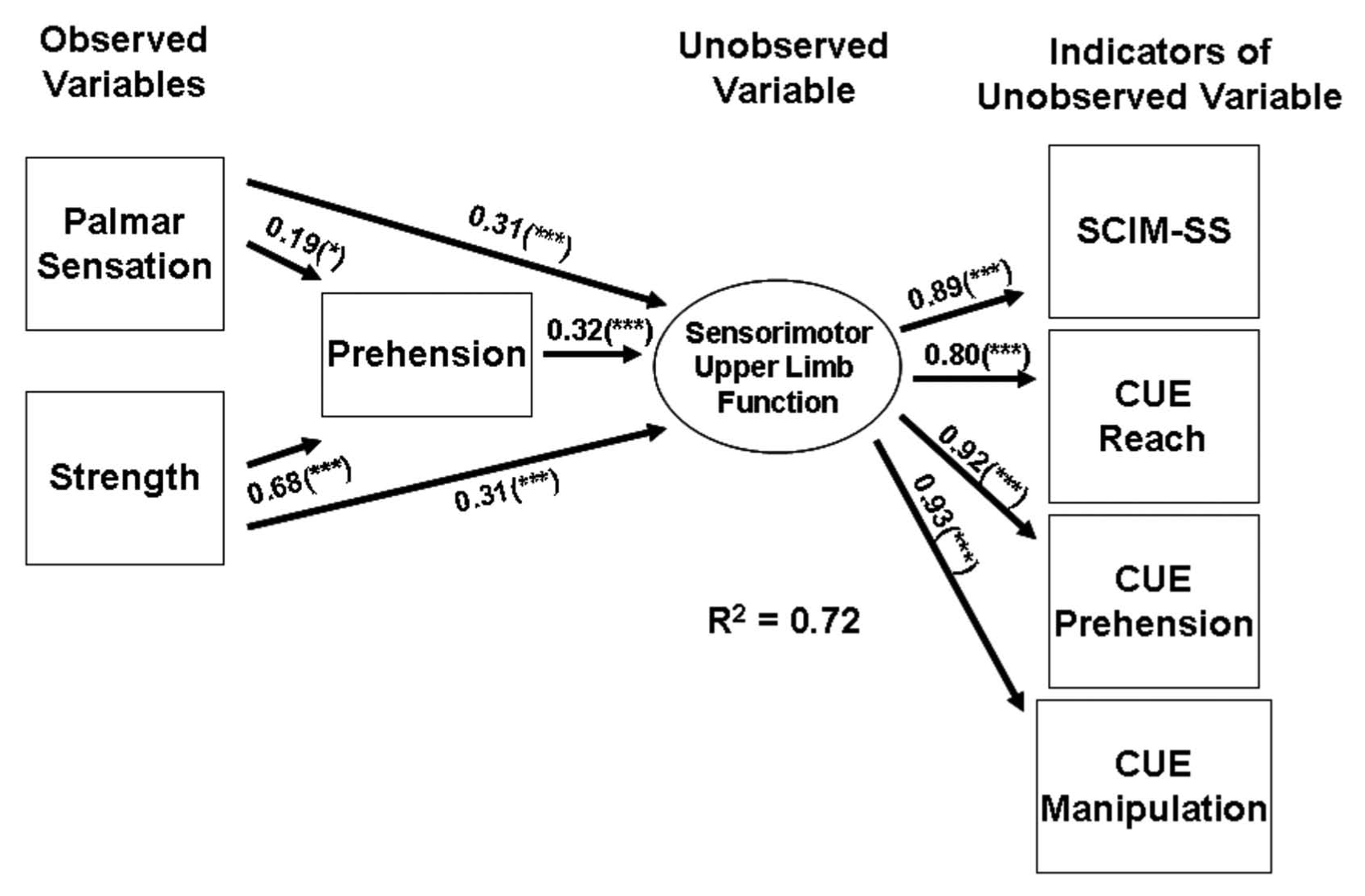
Structural equation modeling results for the hypothetical model.
Based on the SEM, palmar sensation showed a direct and indirect relationship to upper limb function. (Note: Each arrow represents the strength of the association that it illustrates, in the case of this model arrow values can be added if consecutive on the left of the latent trait.) The relationship mediated through prehension is larger (0.19 + 0.32) than the direct relationship (0.31); but both direct and indirect relationships are statistically significant. Strength also showed a direct and indirect relationship to upper limb function. The relationship mediated through prehension is larger (0.68 + 0.31) than the direct relationship to upper limb function, but both direct and indirect relationships are statistically significant. Therefore, sensorimotor upper limb function can be predicted by palmar sensation and strength through prehension. The values on the right of the latent trait 0.89, 0.80, 0.92, 0.93) simply confirm that sensorimotor upper limb function is adequately estimated by the variables used. The values are very high and significant, which would be expected as the SCIM and CUE are functionally relevant tests and the construct of “sensorimotor upper limb function” is well defined by impairments that are functionally relevant. Essentially, changes in strength and sensation are most likely to have an effect on upper limb function when associated with improvement in prehension.
Discussion
This is the first assessment tool to reveal the importance of separate domains in integrated functions and will assist in understanding the impact of emerging mechanisms of recovery for hand function and specific rehabilitation interventions. In summary, this analysis has contributed to the body of knowledge that provides information to confirm that the GRASSP version 1.0 is useful and relevant in a clinical and research setting.
Significance of Findings
The development process of GRASSP version 1.0 has consisted of many stages, one of which was the design of the theoretical framework (Figure 1A). The framework guided the process of item generation. This analysis confirms that the design of the measure and the elements incorporated in GRASSP do capture what they were intended to—core and integrated elements of impairment to define with greater sensitivity upper limb function. Thus, this analysis confirms the adequacy of the framework and design of the assessment tool.
Significance of Sensory Testing of the Hand in Tetraplegia
Second, this analysis establishes the importance of sensory testing in the hand for individuals with tetraplegia to establish status at baseline, over the course of recovery and to define the relationship of impairment to function. Sensation is reported to have a significant impact on prehension and manipulation.15,30,31 The recovery of sensation after peripheral hand injury is considered to be fundamental for the return of function.31,32
Preliminary evidence has shown improvements in sensation when measured by Semmes Weinstein Monofilaments after a 3-week intensive massed practice and somatosensory stimulation protocol for individuals with tetraplegia. Overall hand function was most improved for individuals receiving massed practice and somatosensory stimulation, versus just massed practice or somatosensory stimulation, or conservative management alone.33-35 Apart from this work there is very little reference to the significance of measuring hand sensation in tetraplegia in the field of SCI. Some developers of tests have commented on the additional benefit sensory testing would provide in elucidating functional ability31,36; however, they have not incorporated sensation or been able to show its significance. Thus, this work has shown within the confines of what GRASSP measures that the role of sensation is significant for the assessment of individuals with tetraplegia as it plays a role in defining not only impairment but also function.
Core and Integrated Impairment
Third, this work confirms that sensation, strength, and prehension play a distinct role in upper limb function as hypothesized by the theoretical framework. At the outset, we assumed it was important to measure all 3 domains of impairment to reflect function accurately. However, the magnitude of the relationships was unknown. We anticipated that there was an intermediate relationship where strength and sensation would influence prehension, and prehension would then have an association with upper limb function. So far there is little evidence available to define the relationship between sensation and strength on upper limb function in tetraplegia. Furthermore, changes in impairment do not have a uniform impact on clinical recovery between individuals, thus the assessment of the strength and sensation should be accompanied by the assessment of prehension to understand recovery on an individual basis.
This analysis defines for the field how the GRASSP allows us to distinguish the contribution of strength, sensation, and prehension to upper limb function. Understanding the contribution of strength and sensation is important in clinical studies to distinguish and better understand the effect of interventions, which is now possible with GRASSP. The GRASSP has the potential not only to inform as to whether the prehension is changing but also what elements contribute to the change, thus allowing the developers of new hand function therapies to establish efficacy and also understand the integration of the core elements of impairment. The GRASSP will enable us to see what impairment (sensation or strength) is most affected by a therapy further informing us of the benefits of new treatments. Furthermore, it can inform the administrator whether change in sensation has an effect on hand and arm function.
Evidence for Therapeutic Interventions
Some of the most basic and important functions for humans occur by way of prehensile ability. 30 With restoration of hand function as the focus in certain labs,33-35,37,38 the significance of components of prehension and the best possible ways to enhance prehension are paramount. This analysis provides us with some insights into this. SEM substantiates that sensation and strength are relatively equal in their effect on upper limb function. The relationships of sensation and strength mediated through prehension show that strength is a stronger factor. These relationships of upper limb function mediated through prehension support the concept of rehabilitation processes incorporating the use of functional tasks, specifically prehension retraining protocols. Therefore, it is of importance that recovery of sensation on the palmar surface of the hand be enhanced after SCI. Targeted sensory retraining of the hand within a functional paradigm (task-specific prehension) may be necessary to refine functional ability during the rehabilitation phase. In this analysis, it is noted that having good sensation indirectly impacts upper limb and hand function. Therapies need to be applied so that the palmar surface of the hand is stimulated, to promote activity optimizing sensory activity leading to recovery. Furthermore, interventions targeted toward recovering motor function must be applied within a functional context, with varying degrees of force generation and sequencing of muscle activation.
Limitations
This particular analysis was conducted with a cross section of data collected on individuals with chronic tetraplegia. Thus, the findings established with this set of data are likely not to be recreated with a more acute sample of data. In fact, the authors are interested to see the differences between the 2 groups, which is a proposed future analysis. Sample size was not a shortcoming of this work; however, to repeat the analysis on a second cohort would be optimal to confirm the defined relationships. Furthermore, the opportunity to conduct SEM with additional independent variables would allow the authors to define additional associations and relationships, which could help develop a greater understanding of the interrelationships of impairment, function, and quality of life.
Conclusion
In conclusion, the GRASSP assesses impairment in 3 domains. During the development of the GRASSP, the theoretical framework guided item generation to be anatomically, neurophysiologically, and functionally relevant. 11 The GRASSP was intended to distinguish the contributions of sensation and strength to function and does so effectively. This analysis confirms that all 3 domains are relevant in the assessment of impairment of the upper limb post–cervical SCI. Such measures are needed to better understand what and where treatments achieve improvements. The SEM confirms the concepts and components of the construct particularly the domains and their individual and integrative importance.
Quantifying impairment more precisely has enabled the investigators to establish the magnitude of the relationships and integration of palmar sensation, upper limb strength, and prehension to upper limb function. In the future, using the SEM approach across the recovery period could assist in determining the magnitude of impairment change that will lead to different levels of functional change. The next steps will be to test the degree of these relationships and integration during the course of recovery.
Footnotes
Acknowledgements
The International GRASSP Research & Design Team would like to acknowledge the GRASSP Cross Sectional Study Group for their commitment to the study and for providing assistance in operating the study at their specific centers.
Authors’ Note
GRASSP Cross Sectional Study Group: Kimberley Eberhardt and Rebecca Ozelie at Rehabilitation Institute of Chicago; Megan Watts and Rob Corcoran at Vancouver Coastal Health; Marlene Adams, Sylvia Coates, and Abigail Dry at Toronto Rehabilitation Institute; Gina Cooke at Magee Rehabilitation–Regional Spinal Cord Injury Center of the Delaware Valley; Christina Robert at University Hospital Balgrist; Martha Horn and Simone Hirsch at Traumacenter, Murnau; Kristin Lorenz and Petra Schatz at Hohe Warte, Bayreuth.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
Financial support was provided by The Christopher and Dana Reeve Foundation, The Rick Hansen Foundation, The Ontario Neurotrauma Foundation and Toronto Rehabilitation Institute Student Scholarship Fund. Dr Beaton was supported by a CIHR New Investigator’s award during the conduct of this study. The European study was supported by the EMSCI network.