
Abstract
Background
Exercise positively affects multiple sclerosis (MS) symptoms, physiological systems, and potentially cognition. However, an uninvestigated “window of opportunity” exists for exercise therapy early in the disease.
Objective
This study presents secondary analyses from the Early Multiple Sclerosis Exercise Study, and aims to investigate the efficacy of exercise on physical function, cognition, and patient-reported measures of disease and fatigue impact early in the disease course of MS.
Methods
This randomized controlled trial (n = 84, time since diagnosis <2 years) included 48 weeks of aerobic exercise or an active control condition (health education) and between-group changes are based on repeated measurement mixed regression models. Physical function tests included measures of aerobic fitness, walking (6-minute walk, Timed 25-foot walk, Six-spot step test), and upper-limb dexterity. Tests of processing speed and memory evaluated cognition. The questionnaires Multiple Sclerosis Impact Scale and Modified Fatigue Impact Scale assessed perception of disease and fatigue impact.
Results
Following early exercise aerobic fitness showed superior between-group physiological adaptations (4.0 [1.7; 6.3] ml O2/min/kg; large effect size [ES = 0.90]). No other outcomes showed significant between-group differences, yet all measures of walking and upper-limb function showed small-to-medium effect sizes in favor of exercise (ES = 0.19−0.58). Overall disability status as well as cognition were unaffected by exercise, whereas perception of disease and fatigue impact were reduced in both groups.
Conclusion
In early MS, 48 weeks of supervised aerobic exercise seem to positively modify physical function, but not cognitive function. Perception of disease and fatigue impact may be modifiable by exercise in early MS.
Trial registration:
Clinicaltrials.gov (identifier: NCT03322761).
Introduction
In multiple sclerosis (MS) early diagnosis along with early initiation of disease-modifying drug treatments are considered crucial for the long-term impact of the disease. This notion is aligned with an emerging perception stating that all persons have inherent and somehow interdependent neurological (defined by brain volume and cognitive function) and physical functional (defined by the capacity of several physiological systems) reserve capacities, and that the neurodegenerative nature of MS gradually depletes these.1,2 When exhaustion of neurological and physical functional reserve capacities exceeds the neuroplastic compensatory mechanisms of the CNS clinical symptoms will manifest. The primary aim when treating MS therefore is to preserve nervous tissue (brain tissue in particular) by reducing disease activity, and to preserve physical as well as cognitive function (ie, preserve neurological and physical functional reserve). 3 Disease-modifying drug treatments have proven effective in reducing the disease activity and MRI burden—particularly when initiated early in the disease course, rather than later.4,5 Early initiation of disease-modifying drug treatment may also slow disability progression, 6 but disabilities still accumulate over time in terms of physical functional and cognitive impairments—suggesting limited direct effects of disease-modifying drug treatments on specific motor-related tracts and nuclei in the central nervous system. The physical functional and cognitive impairments manifest already from an early timepoint of the disease course, as do patient-reported measures such as fatigue.7,8 Considering the limited evidence for direct effects of disease-modifying drug treatment on measures of physical function, cognition, and MS symptoms such as fatigue, treatment strategies that from an early time point of the disease can aid in limiting these impairments, are warranted.
Exercise may be a promising candidate to aid in reducing the impact of MS, physical and cognitive function, as well as reducing fatigue. 9 However, a recent topical review performed by our group revealed that an overlooked “window of opportunity” exists in MS exercise research, as interventions are generally initiated rather late in the disease course. 10 This observation is likely explained by the fact that exercise therapy is commonly seen and applied as a symptomatic treatment aiming at improving (or reducing the impact of) symptoms when they have manifested, rather than as a potential preventive intervention. Consequently, it is still unresolved whether exercise therapy also holds the potential to preserve (or even improve) physical function and cognition when initiated early in the disease course of MS, ultimately postponing manifestation of clinical symptoms. Primary analyses from this study—the Early Multiple Sclerosis Exercise Study (EMSES)—found a positive effect of supervised aerobic exercise early in the disease course of MS on the microstructural integrity of a priori defined motor-related tracts and nuclei, indicating that early exercise may have beneficial effects on physical function. 11
With these secondary analyses from the EMSES study we now aim to further investigate the efficacy of 48 weeks of supervised aerobic exercise on measures of disability progression (Multiple Sclerosis Functional Composite [MSFC]), physical function (walking capacity, hand dexterity, and aerobic fitness level), cognitive function (processing speed, attention, and memory), and patient reported outcome measures of disease and fatigue impact. We hypothesized that the general progression of disabilities would be lower, and specifically that measures of walking capacity and aerobic fitness level would increase in the group of patients receiving supervised aerobic exercise when compared to the control condition. Measures of hand dexterity and cognition were not expected to differ between groups. Finally, we expected to find a positive effect on patients’ perception of MS symptoms and disease impact.
Methods
This paper presents analyses of secondary data from the EMSES study. Data on disease-modifying and neuroprotective parameters (primary outcomes) has been published elsewhere. 11 A separate study protocol including full details on study design, recruitment and eligibility of patients, methodologies of applied outcomes, and statistical analysis has also been published elsewhere. 12 The study is approved by The Central Denmark Region Committees on Health Research Ethics (1-10-72-388-17) and registered at the Danish Data Protection Agency (2016-051-000001 (706)).
Study Design and Participants
This was a national multicenter single-blinded parallel-group randomized controlled trial comparing an intervention group receiving usual care plus supervised exercise therapy and a control condition with usual care plus health education over a period of 48 weeks.
Recruitment was done in collaboration with six Danish regional MS clinics and the Danish MS Society according to the following inclusion criteria: (1) 18 to 60 years of age, (2) ≤2 years since clinical diagnosis with relapsing remitting MS, and (3) no relapses or changes in medication status 8 weeks prior to inclusion.
Study Groups
Group allocation was concealed by the sealed envelope principle, and participants were randomized in a 1:1 ratio stratified by line of treatment.
Supervised Exercise Therapy
The intervention group received an exercise program planned on the basis of four principles (adapted from Stathopoulos and Felson Duchan 13 ): (1) individual tailoring, (2) application of exercise types matching the goal of the intervention, (3) progressive overload, and (4) sufficient intensity to induce the desired effects of the intervention. The exercise intervention was therefore planned as high-intense aerobic exercise, monitored relative to the patients’ individual maximal heart rate (HRmax), and progressed within and between 4 meso cycles of 12 weeks. The exercise program included 2 weekly sessions, including a mixture of continuous sessions (lasting 30-60 minutes with an intensity of 60%-80% HRmax) and interval training sessions (lasting 30-60 minutes with an interval duration of 1-10 minutes and intensities varying from 65% to 95% HRmax) using patient-preferred (alternating) training modalities. All sessions were supervised by trained personnel, and a summary of the intervention is provided in Table 1. This summary, as well as full details on the exercise intervention have been published elsewhere.11,12
Summary of the Supervised Exercise Therapy Intervention.
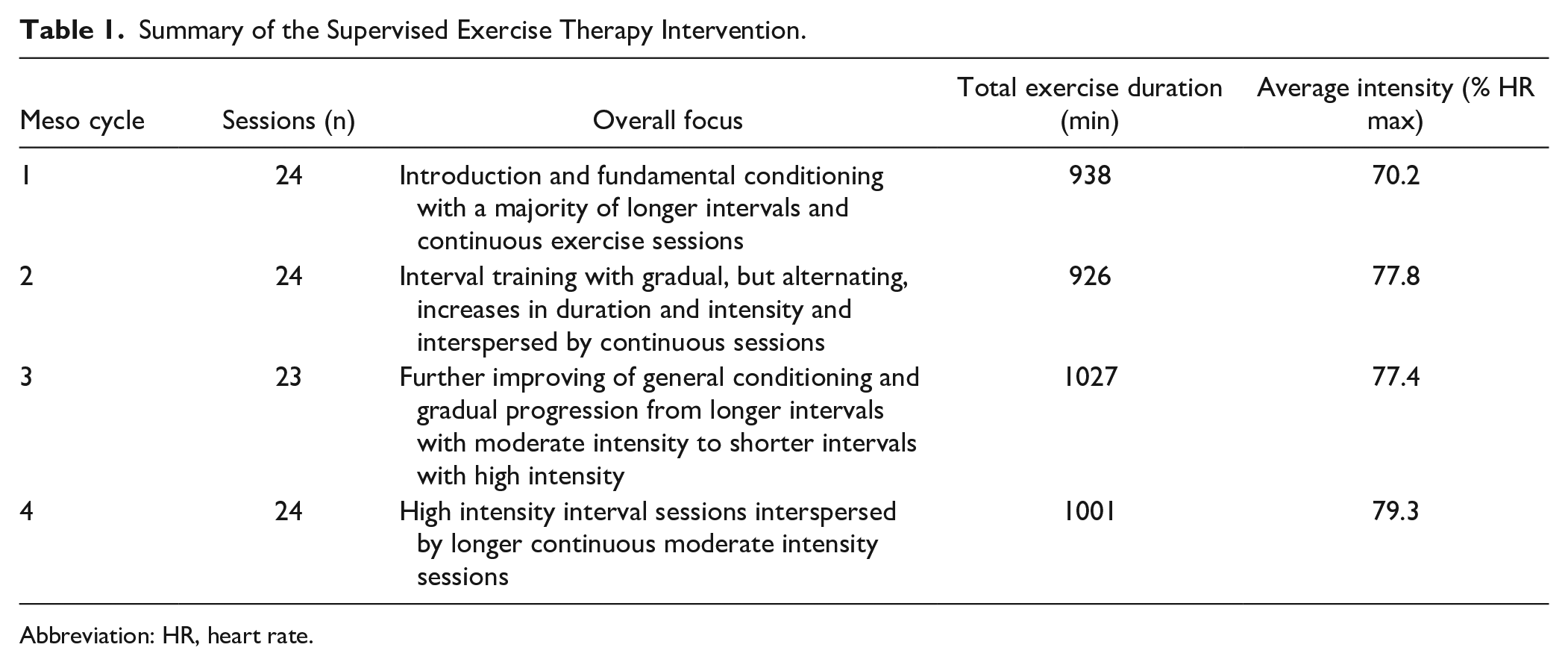
Abbreviation: HR, heart rate.
Health Education Control
The control group of the present study was offered four 1.5-hour health education—1 session every 12 weeks throughout the full study period of 48 weeks. The overall themes of the sessions were: session 1 “Physical activity,” session 2 “aerobic training,” session 3 “resistance training,” and session 4 “Alternative training.” Otherwise, the patients received usual care and were left to self-administered behavior. As a previous study showed no effect of an education program on MS impact or symptoms in mildly disabled patients with MS, 14 the only reason for offering these sessions were to facilitate adherence to this long-term control condition.
Outcomes
This paper present analysis of secondary data from The EMSES. Data on disease-modifying and neuroprotective parameters (primary outcomes) has been published elsewhere. 11
Outcomes were assessed at baseline (T0), after 24 weeks (T24), and after 48 weeks (T48).
Disability Progression
The MSFC was used to assess the general disability progression of patients as it is suggested to be more sensitive to changes than the Expanded Disability Status Scale (EDSS). 15 The components of the MSFC will be described in the following sections, and the MSFC scores have been calculated according to the MSFC administration and scoring manual with the mean baseline results as reference, when calculating follow-up (24 and 48 weeks) Z-scores to evaluate treatment effects. 16
Physical Function
Walking capacity has been rated as one of the most important bodily functions by MS patients.17,18 Therefore, 3 different measures of walking were included in the present study. The timed 25-foot walk test (T25FWT) was applied as a simple short walking test at maximal walking speed (part of the MSFC), whereas the six-spot step test (SSST) was applied as a more complex short walking test at maximal speed, specifically challenging balance and coordination. Also, the 6-minute walk test (6MWT) was applied to assess walking endurance. The 9-hole peg test was administered as a measure of manual dexterity and upper limb function (part of the MSFC). Finally, the aerobic fitness level was measured by direct assessment of the maximal rate of oxygen uptake during an incremental exercise test on a bicycle ergometer. As improvement in aerobic fitness is the primary physiological response to the exercise intervention and thus serves as an important compliance measure, the data on aerobic fitness change is presented both elsewhere, and in the present paper. 11
Cognition
Patients completed the selective reminding test (SRT) as a measure of verbal learning and memory. The test includes measures of long-term storage (SRT-LTS), consistent long-term retrieval (SRT-CLTR), and delayed recall (SRT-D). To assess processing speed and attention both the symbol-digit modality test (SDMT) and the paced auditory serial addition test (PASAT) were conducted, with the latter also contributing to the MSFC score.
Patient-Reported Outcome Measures
Patients completed the 29-item multiple sclerosis impact scale (MSIS) to report on their perception of general as well as physical and psychological disease impact. The 12-item multiple sclerosis walking scale (MSWS) was used to measure the impact of MS on walking ability, and the modified fatigue impact scale (MFIS) assessed the impact of fatigue. To evaluate physical behavioral changes and specifically participation in structured exercise, the sport index of the Baecke Physical Activity Questionnaire was completed in 1-year retrospect at T0 and T48.
Statistical Analysis
Sample size was calculated based on expected effects on the 2 primary outcomes, which were annual relapse rate and global brain atrophy rate. 12
All longitudinal data was analyzed using repeated measurements mixed effects regression models with participants as random effects and group, time, and the interaction between group and time (including baseline) as fixed effects. All presented between-group estimates rely on the regression model and represents the change from T0 to T48. Model validation included likelihood-ratio tests, and standardized residuals were visually inspected as Quantile-quantile plots and plots of standardized residuals against fitted values. In all cases, the analysis was performed as intention-to-treat and thereby include all patient data regardless of their compliance to the protocol.
For graphical presentation of results within-group changes (T0-T48) were expressed as mean percentage change (95% confidence interval) relative to T0. Furthermore, effect sizes were calculated to quantify the magnitude of treatment effects and were interpreted according to the recently published empirically based guidelines specific for rehabilitation studies with small, medium, and large effect sizes set at 0.14, 0.31, and 0.61, respectively. 19
Pairwise Pearson correlations were made on pooled data (total group of patients) to explore potential associations between change in exercise behavior (Baecke sport index), and all measures of physical function, cognition, and patient-reported outcomes.
Consistent with recent statistical guidelines, the interpretation of P-values is toned down to avoid a dichotomous interpretation of statistical significance.20,21
STATA 16.1 (StataCorp LP, Texas, USA) and GraphPad PRISM 7.0e (GraphPad Software, California, USA) was used to perform statistical analysis and graphical presentations, and the level of statistical significance was set at P ≤ .05.
Results
From a total of 164 eligible patients, 84 patients (63 females/21 males) with an average age of 37.4 (9.8) years, time since diagnosis of 10.6 (6.8) months and an EDSS score of 1.6 (1.0) were included (see Figure 1 for flow of patients through all study phases). Details on baseline characteristics is presented in Table 2. Data on baseline characteristics along with data on the representativeness of the study sample have also been presented elsewhere. 11 In brief, the present study sample was generally considered representative of the general early MS population (≤2 years since diagnosis) as a comparison to data from the full population of early MS patients from the Danish MS registry revealed only minor differences in time since diagnosis, gender distribution, and disease-modifying drug status.
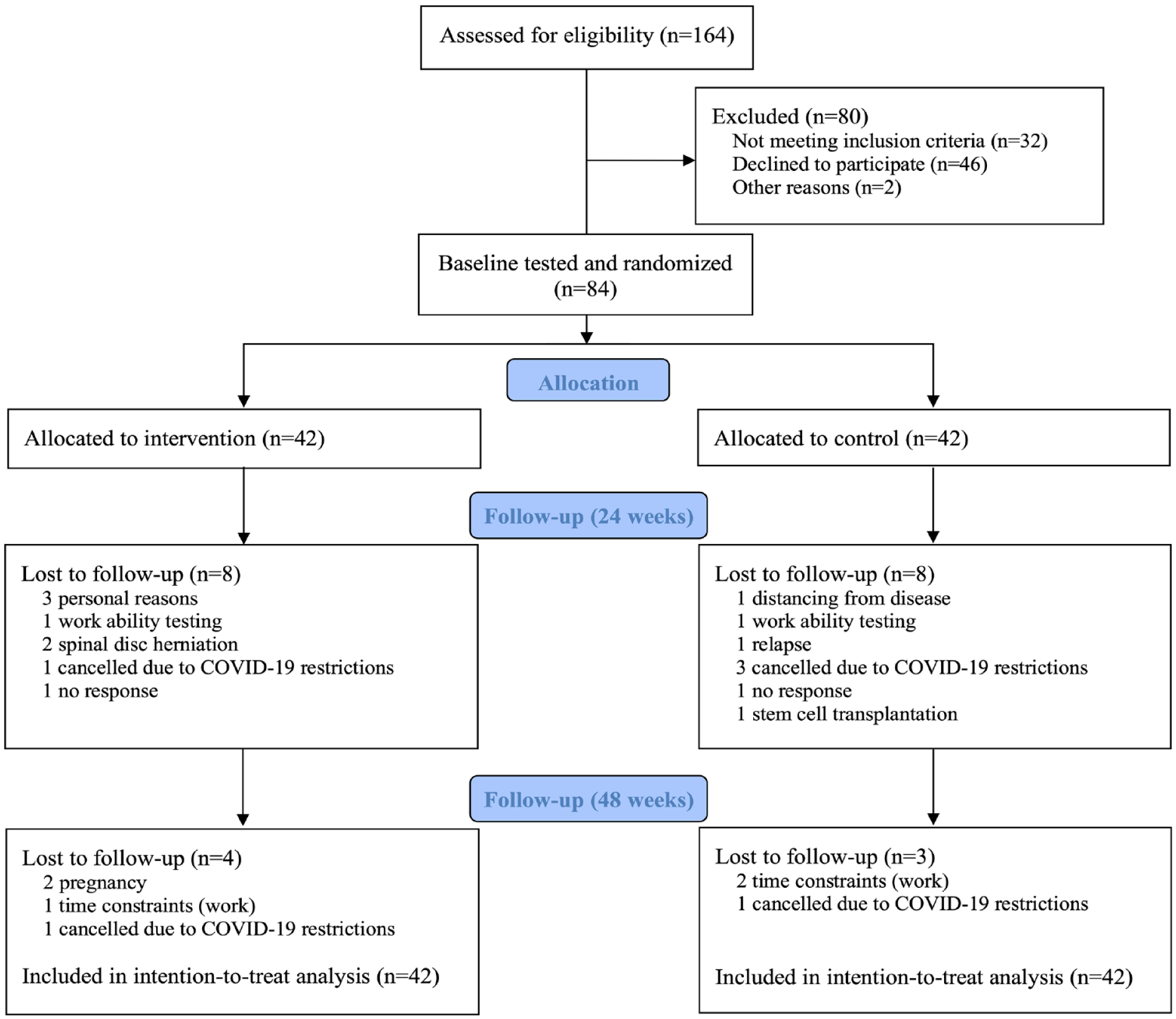
Flow diagram of study phases. None of the dropouts were, to the knowledge of the authors, related to the exercise intervention.
Baseline Characteristics of Included Patients.
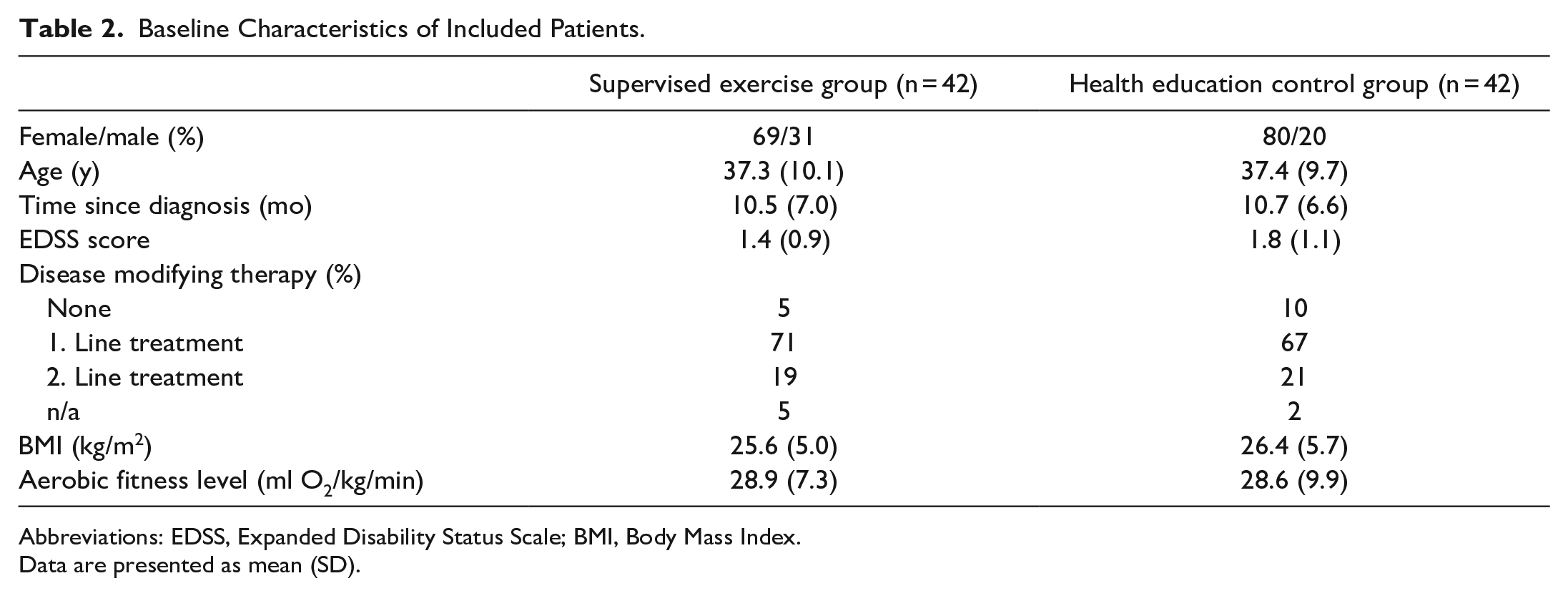
Abbreviations: EDSS, Expanded Disability Status Scale; BMI, Body Mass Index.
Data are presented as mean (SD).
Exercise Adherence and Behavior
As also reported elsewhere, 11 patients in the supervised exercise group completed 90.0 (8.6)% of the planned sessions at an average intensity of 84.4 (3.0)% HRmax. The Baecke sport index showed an increased structured exercise participation in both groups (exercise: 0.57 [0.33; 0.81], and control: 0.32 [0.08; 0.55]) with a trend toward a greater increase in the supervised exercise therapy group (Table 3), that was supported by a between-group medium effect size (ES = 0.20).
Disability Progression Measured by MSFC, As Well As Physical Function, Cognitive, and Patient-Reported Outcomes.
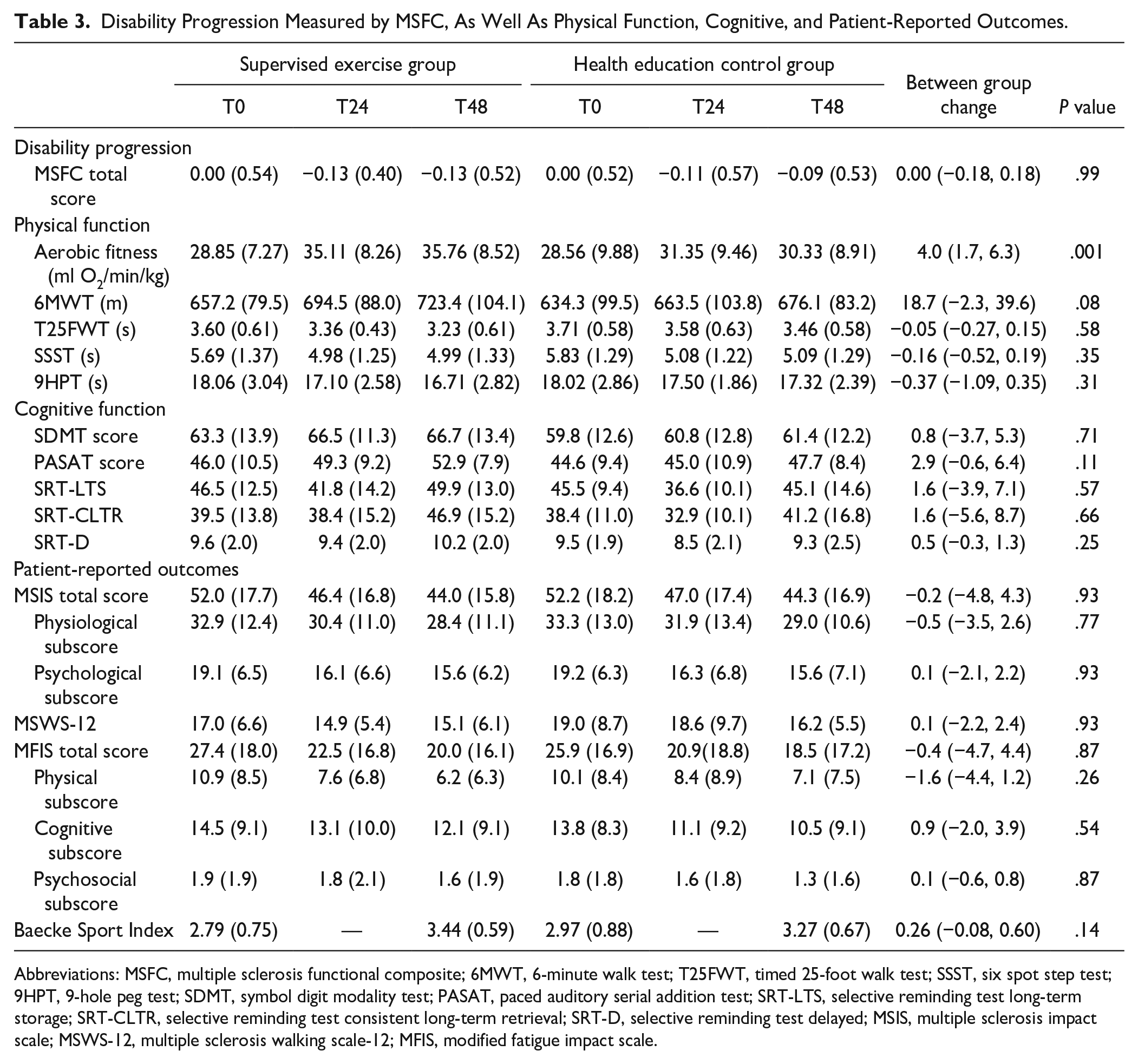
Abbreviations: MSFC, multiple sclerosis functional composite; 6MWT, 6-minute walk test; T25FWT, timed 25-foot walk test; SSST, six spot step test; 9HPT, 9-hole peg test; SDMT, symbol digit modality test; PASAT, paced auditory serial addition test; SRT-LTS, selective reminding test long-term storage; SRT-CLTR, selective reminding test consistent long-term retrieval; SRT-D, selective reminding test delayed; MSIS, multiple sclerosis impact scale; MSWS-12, multiple sclerosis walking scale-12; MFIS, modified fatigue impact scale.
Disability Progression
The overall disability status did not progress differently between study groups, when measured by the MSFC (Table 3).
Physical Function
Both study groups showed within-group improvements in all measures of physical function, except for aerobic fitness level in the health education control group (0.82 [−0.82; 2.46], P = .33). Between groups, the aerobic fitness level increased more in the supervised exercise group than in the health education control group (4.0 [1.7; 6.3] ml O2/min/kg, P = .001; large effect size), as also presented elsewhere. 11 No further between-groups differences were observed (Table 3). However, medium effect sizes for the 6MWT and the SSST and small effect sizes for the T25FWT and 9HPT were observed—all in favor of the supervised exercise group (Figure 2).
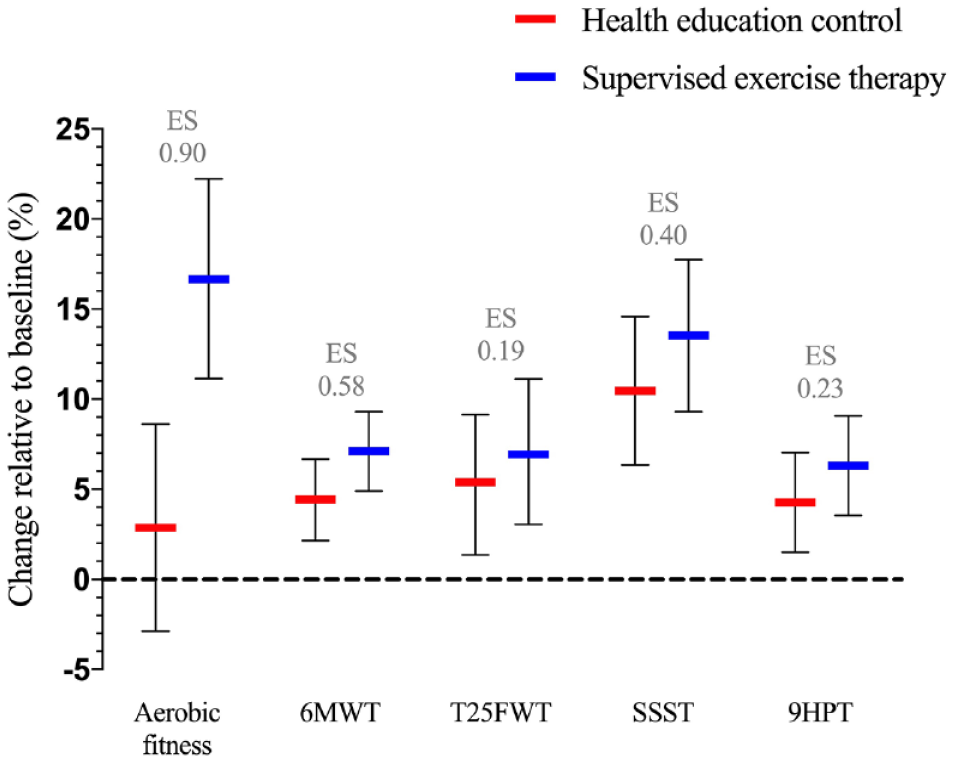
Percentage within-group changes in physical functional outcome measures relative to baseline and between-group effect sizes of treatment effects.
Cognition
Performance on the PASAT was improved in both study groups (exercise: 5.9 [3.5; 8.4], p<0.001, control: 3.1 [0.7; 5.5], P = .01), and the CLTR in the SRT was improved in the supervised exercise therapy group only (5.2 [0.2; 10.1], P = .04). While no between-group differences were observed, a medium effect size in favor of the supervised exercise group was observed for the SRT-D along with small effect sizes for the PASAT and the SRT-LTS (Figure 3).
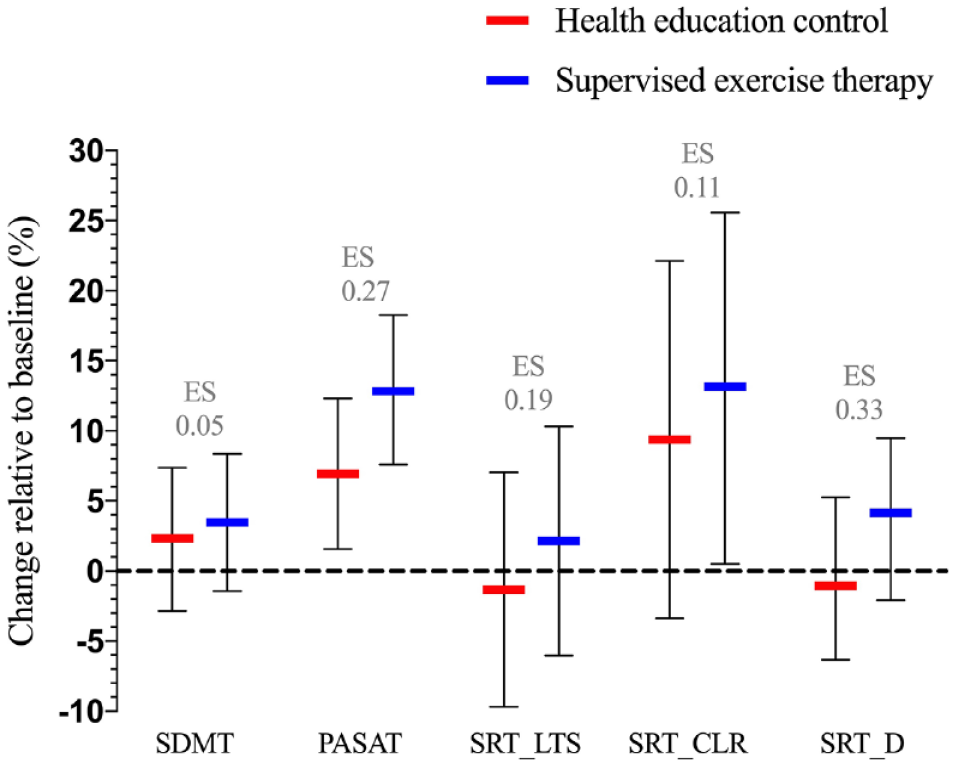
Percentage within-group changes in cognitive outcome measures relative to baseline and between-group effect sizes of treatment effects.
Patient-Reported Outcome Measures
Patients’ perception of MS impact, as measured by the MSIS, were reduced at the end of the study period (exercise: −5.3 [−8.5; −2.2], control: −5.1 [−8.2; −2.0]) but with no between-groups difference (Table 3) and no effect size suggestive of a treatment effect (ES = 0.06). The same pattern was observed for the MFIS and the MSWS (exercise: −4.9 [−8.6; −1.2], and −1.5 [−3.1; 0.1], respectively and control: −4.4 [−8.1; −0.8], and −1.6 [−3.2; 0.0], respectively), but again between-groups differences and treatment effects (ES = 0.10 and 0.07, respectively) were not observed.
Across data from both groups, explorative analyses further revealed that the change in Baecke sport index was associated with changes in 6MWT, MSIS, MFIS, and trending to be associated with change in SSST and PASAT, but not T25FWT, 9HPT, MSWS, or any of the other cognitive outcomes (Table 4).
Pairwise Correlations Between Change in Baecke Sport Index and Respective Changes in Physical Functional, Cognitive, and Patient-Reported Outcomes.
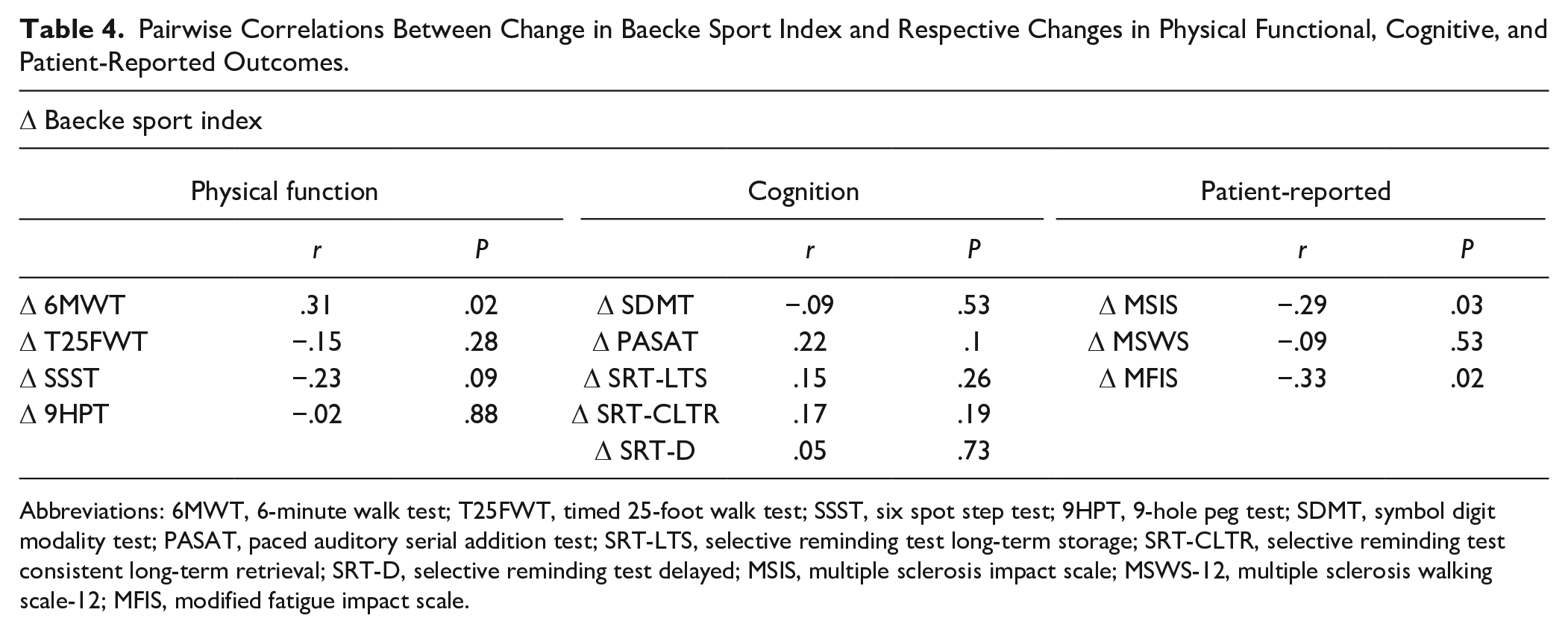
Abbreviations: 6MWT, 6-minute walk test; T25FWT, timed 25-foot walk test; SSST, six spot step test; 9HPT, 9-hole peg test; SDMT, symbol digit modality test; PASAT, paced auditory serial addition test; SRT-LTS, selective reminding test long-term storage; SRT-CLTR, selective reminding test consistent long-term retrieval; SRT-D, selective reminding test delayed; MSIS, multiple sclerosis impact scale; MSWS-12, multiple sclerosis walking scale-12; MFIS, modified fatigue impact scale.
Discussion and Perspectives
This is the first study to investigate whether exercise holds the potential to reduce disability progression, preserve or even improve physical function and cognition, and reduce patients perception of disease-impact and symptom burden in the overlooked “window of opportunity” early in the disease course of MS. 10
In summary, no reduction in disability progression (MSFC) was observed. Only, aerobic fitness improved significantly between-groups. However, the supervised exercise intervention showed superior treatment effect sizes in all measures of physical function when compared to the health education control condition, particularly in aerobic fitness and walking endurance (6MWT). The cognitive function was mainly unaffected over the course of the 48-weeks study period. Both study groups reduced their perception of disease and fatigue impact during the study period, and a trend toward a reduction of impact of the disease on perceived walking abilities was also observed. However, no between-group differences were found for these patient-reported outcomes either. The fact that all physical functional outcomes showed superior mean treatment effect sizes along with substantial improvements in aerobic fitness and walking endurance in favor of the supervised exercise intervention suggest that the physical functional reserve capacity benefits from early exercise intervention. The lack of significant between-group differences for other outcomes than aerobic fitness may be attributed to ceiling effects of some outcomes in this early and mildly disabled group of patients, behavior changes in the control group, learning effects, and/or lack of statistical power.
A systematic review and meta-analysis did not find any effect of exercise interventions on disability progression when measured by the EDSS score and compared to untreated control groups. 22 The present study is therefore in line with previous findings, even when measured by the supposedly more sensitive MSFC. However, the present study is likely limited by a ceiling effect as the study sample is very early in the disease course and has a low disability status at enrollment. As such, this may call for new outcomes that are particularly sensitive at early disease stages when performing future studies in persons with early MS.
Despite the generally low disability status of patients, the aerobic fitness level improved by more than 17% in the supervised exercise group, ensuring a real change, and providing evidence that the exercise intervention induced the expected physiological response. 23 Moreover, this finding is particularly interesting as the aerobic fitness level has been shown to be associated with all levels of the International Classification of Functioning, Disability and Health model and with the risk of cardiovascular comorbidities known to exacerbate the disease burden of MS.24,25 Furthermore, the improvement observed in both study groups for walking distance on the 6MWT is well beyond the clinically relevant change of 22 m. as reported by Baert et al 26 and the trend toward a between-group difference in favor of the supervised exercise group is in close proximity to this cut-off value. These findings suggest that early supervised exercise can increase the physical functional reserve capacity early in the disease course of MS. The small-to-medium effect sizes observed in favor of the supervised exercise group for the T25FWT, SSST, and 9HPT are not approaching the clinically relevant changes for the respective outcomes. 26 However, the existing cut-off values are likely less applicable to this early and low disabled group of patients due to ceiling effects or only a very little room for improvements. An interesting finding was that both the supervised exercise group and the health education control group experienced within-group improvements in almost all physical functional outcomes, suggesting that patients early in their disease course are susceptible to lifestyle modifications, when presented for such options. This finding furthermore highlights the relevance of increasing the focus on early exercise efforts in clinical practice.
There is conflicting evidence related to the effects of exercise on cognition in MS. In particular, patients that are not cognitively impaired may have a diminished response due to the very little room for improvement.27,28 The present data are therefore in line with the literature. However, as the present study is one of the longest MS exercise studies conducted and small-to-medium mean effect sizes were observed in favor of exercise, it may suggest that exercise aid in preserving cognitive reserve capacity. Although speculative, this notion may serve as a rationale for future long-term and large-numbered studies setting out to elucidate the potential of exercise to affect (preserve) cognition throughout the disease course.
Exercise has previously shown the potential to reduce perception of both disease-impact and fatigue, and the MSWS is the most sensitive tool to assess walking ability at low disability levels along with being modifiable by exercise.29 -31 Interestingly, the increase in the self-reported participation in structured exercise as measured by the Baecke sport index, was positively associated with the changes in both MSIS and MFIS. This may possibly explain the observation that both study groups improve to a comparable extent in all three patient-reported outcomes, and adds further support to the previous notion that patients early in the disease course of MS are susceptible to lifestyle modifications. The reduction in perceived fatigue impact is considered clinically meaningful in both groups, but the reductions in disease impact and walking impairments are not.
The present study present with some limitations that must be kept in mind when interpreting the results. First of all, and as already stated, the analyses presented here are secondary and is therefore considered exploratory. Secondly, only relapsing-remitting MS patients were enrolled (as relapse rate was a primary outcome), limiting generalizability to other MS types. Third and finally, the change in exercise behavior (as evidenced by the change in Baecke Sport Index) must be kept in mind when interpreting the results as it may diminish intervention-effects.
In conclusion, 48 weeks of supervised aerobic exercise did not affect overall disability progression, as measured by the MSFC. Following the early exercise intervention aerobic fitness showed significant and superior between-group physiological adaptations. Despite no further significant between-group differences evaluation of treatment effect sizes suggest that the early exercise intervention was superior in improving all measures of physical function, but not cognitive function. Finally, exercise may reduce patient’s perception of disease and fatigue impact in the early stages of the disease course.
Footnotes
Acknowledgements
The authors thank the study participants, as well as the collaborators in this national multicenter trial: MS clinics (Aarhus University Hospital, Odense University Hospital, Clinics of Southern Denmark [Sønderborg, Esbjerg, Kolding] and Hospital Unit of Western Denmark), Physiotherapy Schools (VIA University College [Holstebro, Haderslev, Esbjerg], University of Southern Denmark).
Author Contributions
Conception and design of the work: All. Data collection: MR. Data analysis: MR, LGH. Interpretation of data: All. Drafting the manuscript, revising, and/or final approval of the version to be published: All.
Declaration of Conflicting Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MR, and UD reports grants for the present manuscript from Tryg Foundation, The Danish MS Society, and from Augustinus Foundation. UD reports grants from Canadian MS Society, Aarhus University, Sanofi Genzyme, and Fabrikant Vilhelm Peternsens Legat, outside the submitted work. LGH serve as an unpaid board member in the board of Rehabilitation in Multiple Sclerosis (RIMS). TP and ES has nothing to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is financed by Aarhus University, Faculty of Health (Vennelyst Boulevard 4, 8000 Aarhus C, DK,
Data Sharing
The data underlying the results presented in this article will be made available in a period from 6 months after publication of the present article to 5 years after. A review committee of the study authors will grant access to the data upon reasonable request. Once access is granted, data will be available through The Danish National Archives at sa.dk/en/ (please contact the corresponding author at