
Abstract
Background. Cognitive impairment is a highly prevalent, poorly managed, and disabling consequence of multiple sclerosis (MS). Exercise training that improves physical fitness represents a promising approach for managing cognitive impairment in persons with MS. There is limited evidence that physical fitness is associated with multiple domains of cognitive dysfunction across levels of MS disability. Objective. This cross-sectional study examined the associations among aerobic capacity, lower limb muscle strength, and cognitive functions in persons with mild, moderate, and severe MS disability. Methods. The sample included 62 persons with mild (n = 20), moderate (n = 21), and severe (n = 21) MS disability. The participants underwent neuropsychological assessments of cognitive processing speed (CPS; Symbol Digit Modalities Test [SDMT]), verbal memory (California Verbal Learning Test-2 [CVLT-2]), and visual memory (Brief Visuospatial Memory Test–Revised [BVMT-R]). All participants further underwent testing for measuring aerobic capacity (ie, peak oxygen consumption) and muscular strength (ie, peak torque of knee flexors and extensors). Results. Aerobic capacity and muscular strength outcomes were associated with SDMT (r = .35-.41), but not CVLT-2 or BVMT-R (r < .19) scores in the overall sample. Aerobic capacity (r = .42) and knee flexor peak torque (r = .39) were associated with SDMT scores in persons with mild disability, but not in those with moderate (r < .06) and severe (r < .14) disability. Conclusions. These results support examining aerobic and resistance exercise training programs for improving CPS, particularly among persons with mild MS disability.
Introduction
Cognitive impairment is highly prevalent and disabling in persons with multiple sclerosis (MS). Upwards of 50% of patients experience cognitive dysfunction, which primarily manifests as slowed cognitive processing speed and impaired learning and memory. 1 Cognitive impairment has been associated with unemployment, social isolation, loss of driving ability, and compromised quality of life in persons with MS. 2 Importantly, there are no Food and Drug Administration–approved pharmacological treatments for cognitive impairment in MS, and there is conflicting evidence regarding the efficacy of cognitive rehabilitation interventions in this population. 3 This highlights the importance of considering alternative approaches for managing cognitive impairment in persons with MS. One such approach involves exercise training. 4
Currently, there is equivocal evidence supporting exercise training and fitness for mitigating cognitive dysfunction in MS. There are 3 published randomized controlled trials (RCTs) examining the effects of exercise on cognitive function5-7 and 2 published cross-sectional studies8,9 examining the association between physical fitness (ie, a presumed surrogate for exercise training) and cognition in this population. The first 2 RCTs involved largely unsupervised aerobic and yoga exercise (mean Expanded Disability Status Scale [EDSS] = 2.9) 5 or combined aerobic and resistance exercise (median EDSS = 2.0), 6 respectively, and reported no significant intervention effects on cognitive function or physical fitness in persons with mild disability. The other RCT examined the effects of a supervised, aerobic exercise training intervention on fitness and cognitive function in persons with progressive MS who had moderate disability (mean EDSS = 4.95). 7 Persons undergoing cycle ergometer training demonstrated significant gains in cardiorespiratory fitness and improvements in verbal memory and alertness, but not in cognitive processing speed, compared with a wait-list control group. 7 The lack of an improvement in cognitive processing speed from the later RCT is not consistent with results from a previous cross-sectional study that reported a moderate correlation between cardiorespiratory fitness and cognitive processing speed (pr = .46) in persons with mild MS (mean EDSS = 2.2). 8 There further were no significant associations between cardiorespiratory fitness and measures of learning and memory in that study. 8 Another recent cross-sectional study reported significant associations between measures of cardiorespiratory fitness and cognitive processing speed (r = .44) as well as muscular strength and cognitive processing speed (|r| = .39) in persons with mild MS (median Patient-Determined Disease Steps [PDDS] score = 2). 9 Collectively, this pattern of results suggests that exercise training and fitness might have differential associations with cognitive domains that further depend on disability status. Indeed, 2 recent studies have described significant associations between measures of physical activity (ie, contraction of skeletal muscles resulting in increased energy expenditure) and cognitive processing speed in persons with mild, but not moderate, MS disability.10,11
To date, there are no published studies comparing the associations between domains of physical fitness and cognitive function across levels of disability status in MS. Such a comprehensive examination would better inform exercise training interventions for improving specific cognitive functions in persons with MS, depending on disability status. To that end, the current cross-sectional study examined multiple domains of physical fitness (ie, aerobic capacity and muscular strength) along with neuropsychological measures of cognitive processing speed and learning and memory in a sample of persons with mild, moderate, and severe MS disability. The primary hypothesis was that multiple domains of physical fitness would be associated with cognitive processing speed and learning and memory, such that better fitness would be associated with better cognitive performance. We further hypothesized that disability status would moderate those associations, such that fitness would be associated with cognitive function in persons with mild, but not moderate or severe, MS disability.
Methods
Participants
Prospective participants were contacted using a flyer that was distributed among patients in the North American Research Committee on Multiple Sclerosis (NARCOMS) registry and a preexisting database from previous studies conducted in our laboratory over the past 5 years. During the initial contact, the project coordinator explained the basic protocol of the study to prospective participants via telephone or e-mail. If the contacted individual was interested in the study, the project coordinator undertook screening for inclusion criteria. The inclusion criteria involved (a) definite diagnosis of MS based on physician verification; (b) relapse-free for the past 30 days; (c) ability to walk with or without an assistive device; (d) age between 18 and 64 years; (e) willingness and ability to complete in-person fitness and cognitive assessments; (f) low risk for contraindications of maximal exercise testing indicated by no more than a single “yes” response on the Physical Activity Readiness Questionnaire (PAR-Q 12 ); and (g) physician’s approval for participation. Prospective participants further underwent a self-reported EDSS 13 over the telephone (as we were interested in forming groups of mild, moderate, and severe disability). The resultant score was not used in data analyses, but was used as a preliminary indicator of disability status for the purpose of recruiting disability subgroups of relatively equal size. Participant recruitment and enrollment are presented in Figure 1. Briefly, we initially contacted 129 persons with MS, and 85 expressed interest in the study and underwent screening for inclusion; 4 persons did not meet inclusion criteria. We scheduled the remaining 81 persons for testing, and 18 individuals cancelled the appointment (for reasons unrelated to testing). This resulted in a final sample of 63 persons with MS.
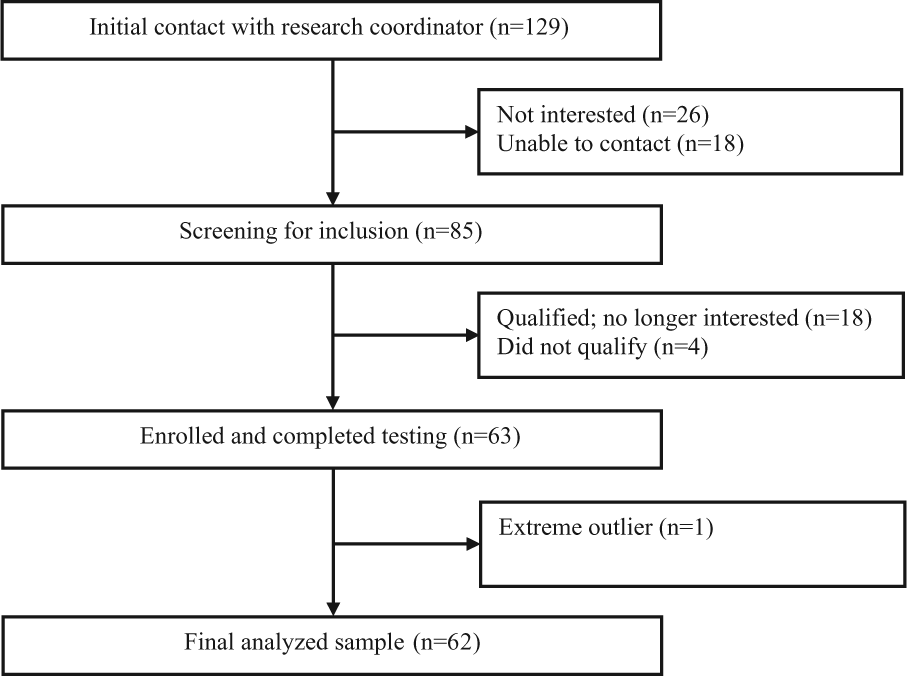
Flow diagram of participant recruitment and enrollment.
Primary Measures
Aerobic Capacity
Aerobic capacity was measured as peak oxygen consumption (VO2peak) using an incremental exercise test on a recumbent stepper (Nustep T5XR, Nustep Inc, Ann Arbor, MI) and an open-circuit spirometry system (TrueOne, Parvo Medics, Sandy, UT) for analyzing expired gases. Initially, participants were fitted to the stepper, and the testing procedures, along with instructions for reporting rating of perceived exertion (RPE), were provided by an investigator. After being fitted with a mouthpiece (Hans Rudolph, Kansas City, MO) for collecting expired gases, participants performed a 1-minute warm up at 15 watts. The initial work rate for the exercise test was 15 watts, and the work rate continuously increased at a rate of 5 to 10 watts/minute until the participant reached volitional fatigue. With the use of the open-circuit spirometry system, oxygen consumption (VO2), respiratory exchange ratio (RER), and work rate were measured continuously and expressed as 20-second averages. Heart rate (HR) was displayed using a Polar heart rate monitor (Polar Electro Oy, Finland), and HR and RPE were recorded each minute during the test. VO2peak was expressed in mL·kg-1·min-1 based on highest recorded 20-second VO2 value when 2 of 3 criteria were satisfied: (a) RER ≥ 1.10; (b) peak HR within 10 beats per minute of age-predicted maximum (ie, 220-age); or (c) peak RPE ≥ 17.
Muscular Strength
Bilateral isometric knee extensor (KE) and flexor (KF) peak torque was measured using an isokinetic dynamometer (Biodex System 3 Dynamometer, Shirley, NY). We focused on lower extremity muscle strength as it is more commonly impaired in persons with MS than upper extremity muscle strength and is an easily identifiable target for exercise training interventions. 14 Participants were seated in the dynamometer according to the manufacturer’s recommendations. Briefly, the axis of rotation of the machine aligned with the lateral epicondyle of the femur. The lower edge of the calf pad against which the participant exerted force was positioned at the midpoint of the lateral and medial malleoli of the fibula and was securely attached using straps. A belt was placed over the torso region to minimize movement during the test. Isometric torque was assessed at 3 joint angles: 45°, 60°, and 75°. At each joint angle, participants performed three, 5-second maximal knee extensions and one 5-second maximal knee flexion. There was a 5-second rest period between contractions within a set, and the rest period between sets was 1 minute. This testing protocol has been previously used within our laboratory to identify strength deficits in persons with MS. 9 The highest recorded peak torque for the stronger leg, regardless of joint angle, was used as a measure of KE and KF isometric strength (N m). We further expressed lower limb muscle strength as an asymmetry score for KE and KF (ie, relative difference in the strength of a particular muscle group between strong and weak limbs), based on previous work. 9 The score is interpreted such that a larger value indicates a greater side-to-side disparity in muscle strength.
Cognitive Function
Cognitive function was measured using the Brief International Cognitive Assessment for Multiple Sclerosis (BICAMS). The BICAMS consists of the oral version of the Symbol Digit Modalities Test (SDMT), 15 the first 5 recall trials of the California Verbal Learning Test-2 (CVLT-2), 16 and first 3 recall trials of the Brief Visuospatial Memory Test–Revised (BVMT-R) 17 as neuropsychological measures of cognitive processing speed, verbal learning and memory, and visual learning and memory, respectively. 18 Briefly, the SDMT involved pairing 9 abstract geometric symbols with single digit numbers in a key. The task was to voice correct numbers for unpaired symbols as rapidly as possible for 90 seconds. Responses were recorded by the examiner, and the primary outcome of the SDMT was the number of correct responses provided in 90 seconds (ie, raw score). 15 The CVLT-2 involved the examiner reading a list of 16 words, with 4 items belonging to 4 categories (eg, vegetables, animals, furniture, modes of transportation) that are randomly arranged. The list was read aloud 5 times in the same order, with each word voiced at a rate of approximately 1 word per second. Participants were instructed to recall as many items as possible, in any order, following each reading of the list. The primary outcome of the CVLT-2 was the total number of correct words identified over the 5 trials (ie, raw score), with a maximum score of 90. 16 The BVMT-R involved 3 trials of the examiner presenting a 2 × 3 array of abstract geometric figures approximately 15 inches in front of the participant for 10 seconds. Following this period, the array was removed and participants were required to draw the array as precisely as possible, with the figures in the correct location. Each drawing is scored on a 0 to 2 scale, based on accurately portraying each figure and its correct location. The primary outcome of the BVMT-R was the total raw score across the 3 trials (ie, maximum score = 36), with higher scores indicating better visuospatial memory. 17 We further computed z-scores for the SDMT, CVLT-2, and BVMT-R based on published norms, 19 but such scores were not included in the primary data analysis. The z-scores were for comparison regarding the extent of cognitive impairment in our sample.
Disability Status
All participants underwent a neurological exam by a Neurostatus-certified examiner who generated Expanded Disability Status Scale (EDSS) 20 scores for describing the sample and stratifying persons into 3 groups based on mild (EDSS of 0-3.5; n = 21), moderate (EDSS of 4.0-5.5; n = 21), and severe (EDSS of 6.0-6.5; n = 21) disability status; these groupings are consistent with research on ambulation in MS. 21
Disease Modifying Treatment Use
We included a self-report yes/no item regarding use of a disease modifying treatment (DMT) along with a space for providing the type of DMT (eg, interferon beta-1a, interferon beta-1b, glatiramer acetate, natalizumab) and dosage, as part of our laboratory’s standard demographics questionnaire. This was coded as 1 for persons indicating use of a DMT, and 0 for persons indicating that they were not currently using a DMT.
Protocol
All participants provided written informed consent approved by a university institutional review board. The study was completed over 2 testing sessions, separated by a 7-day period. The order of assessments and breaks between sessions were designed to minimize physical and cognitive fatigue. For the first session, participants arrived to the laboratory and underwent a neurological examination for generation of an EDSS score. The remaining assessments were broken down into 2 different orders that were counterbalanced across participants (ie, all participants underwent the EDSS on the first day, followed by either the Day A or Day B assessments, and completed the other day’s assessments on the second testing session, 7 days later). The Day A protocol involved initially completing a demographics questionnaire followed by muscle strength testing on the Biodex isokinetic dynamometer. The Day B protocol began with administration of the BICAMS neuropsychological battery; the order of cognitive tests was consistent across participants (ie, administration of the SDMT, CVLT-2, and BVMT-R). Participants underwent the incremental exercise test to exhaustion on the recumbent stepper following cognitive testing on Day B. Participants were remunerated $150 on completion of both sessions.
Data Analysis
All data were analyzed using SPSS version 21 (SPSS Inc, Chicago, IL). We first examined differences between disability groups in demographic and clinical characteristics (ie, age, sex, education, disease duration, and DMT use), physical fitness (ie, aerobic capacity, KE peak torque, KF peak torque, KE asymmetry score, KF asymmetry score), and cognitive (ie, SDMT, CVLT-2, BVMT-R) measures using χ2 difference tests and one-way ANOVA. We further used post hoc Bonferroni corrections to examine specific differences in those variables between groups based on EDSS scores, and computed z-scores for the SDMT, CVLT-2, and BVMT-R based on published norms. 19 The magnitude of group differences in physical fitness and cognitive variables (raw scores) were expressed using partial eta-squared (ηp2), with values of .01, .06, and .14 interpreted as small, moderate, and large, respectively. 22 We then examined age, sex, education, and DMT use as potential covariates by conducting preliminary bivariate correlations and independent samples t-tests in the overall sample, as demonstrated in previous research.10,23,24 We then performed additional bivariate Pearson product–moment correlations (r), using 1-tailed tests, for all physical fitness and cognitive variables in the overall sample. If fitness and cognitive variables were significantly associated in the overall sample, we then conducted similar bivariate correlations in the disability group subsamples. This afforded the opportunity to compare the associations among fitness and cognitive outcomes across disability status groups (ie, moderation). Values for correlation coefficients of .1, .3, and .5 were interpreted as small, moderate, and large, respectively. 22 Lastly, we performed exploratory bivariate correlations among groups based on clinical course of MS (ie, relapsing–remitting versus secondary/primary progressive MS).
Results
Participant Characteristics
Demographic and clinical characteristics of the overall sample and disability subsamples are presented in Table 1. We removed 1 participant from the data analyses based on being nearly 4 standard deviations younger than the mean age, and scoring nearly 5 standard deviations above the overall mean on the SDMT (ie, raw score of 102; extreme outlier); this resulted in a final analyzed sample of 62 persons with MS. There were no statistically significant differences in age, F(2, 59) = 0.87, P = .42, sex, χ2(df = 2) = 1.33, P = .51, DMT use, χ2(df = 2) = 2.29, P = .32, or disease duration, F(2, 59) = 2.25, P = .12, between disability groups. However, there were significant disability group differences in education, χ2(df = 4) = 10.54, P = .03.
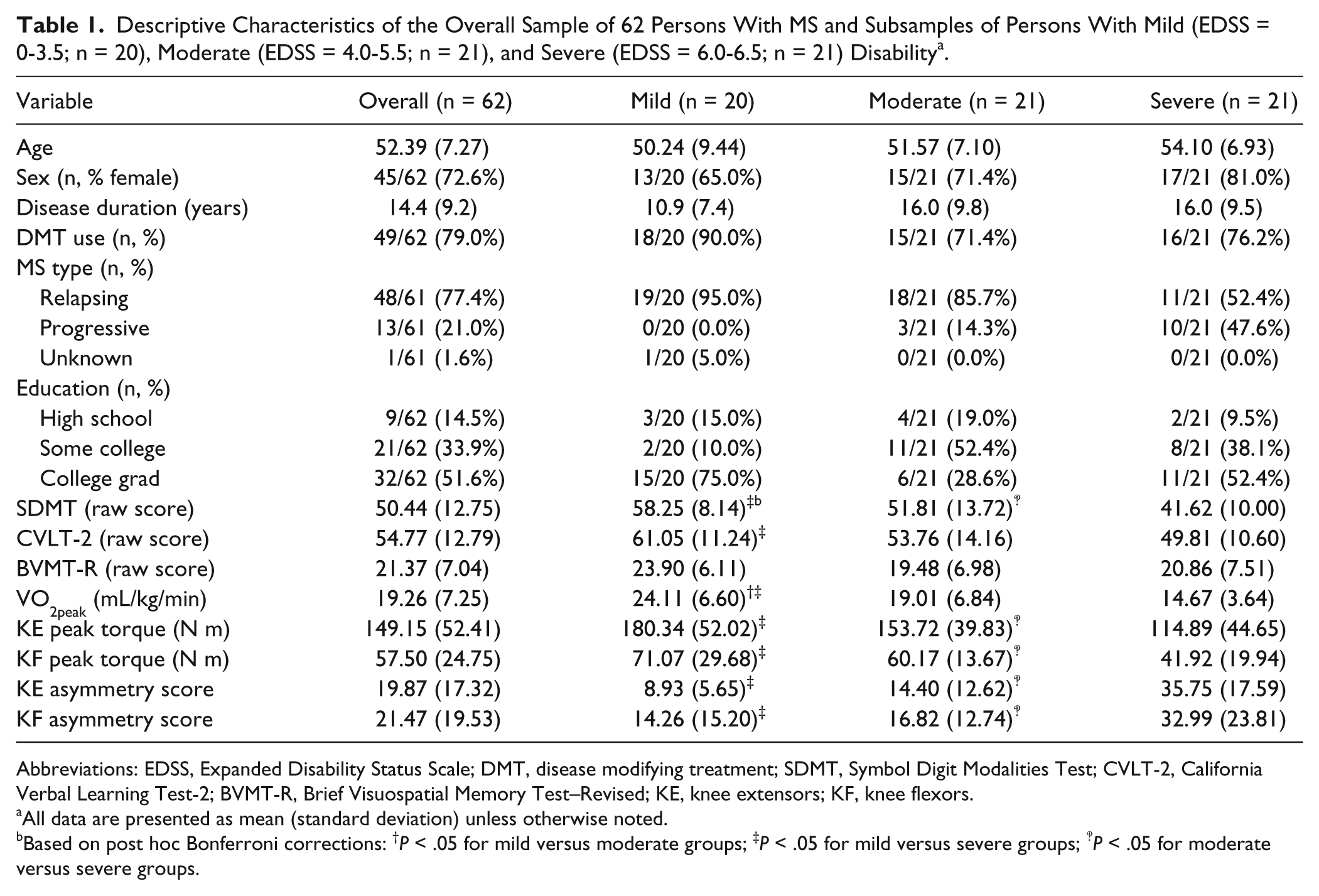
Descriptive Characteristics of the Overall Sample of 62 Persons With MS and Subsamples of Persons With Mild (EDSS = 0-3.5; n = 20), Moderate (EDSS = 4.0-5.5; n = 21), and Severe (EDSS = 6.0-6.5; n = 21) Disability a .
Abbreviations: EDSS, Expanded Disability Status Scale; DMT, disease modifying treatment; SDMT, Symbol Digit Modalities Test; CVLT-2, California Verbal Learning Test-2; BVMT-R, Brief Visuospatial Memory Test–Revised; KE, knee extensors; KF, knee flexors.
All data are presented as mean (standard deviation) unless otherwise noted.
Based on post hoc Bonferroni corrections: †P < .05 for mild versus moderate groups; ‡P < .05 for mild versus severe groups; ‽P < .05 for moderate versus severe groups.
Fitness and cognitive outcomes in the overall sample and by disability group are presented in Table 1. Briefly, the overall sample demonstrated aerobic capacity and muscular strength levels that were consistent with those from other samples of persons with MS.25-27 Overall, 61.3% of participants met at least 2 of the 3 criteria for determining VO2peak; this proportion is larger than that (ie, 43%) from a recent validation study of maximal exercise testing in persons with MS. 28 Importantly, the proportion of participants meeting those criteria in the current study did not significantly differ between disability groups, χ2(df = 2) = 4.76, P = .09. The current sample had similar scores on tests from the BICAMS neuropsychological battery to other samples of persons with MS. 19 The overall sample, on average, demonstrated slowed cognitive processing speed (SDMT z-score = −1.18) and impaired visuospatial (BVMT-R z-score = −0.96), but not verbal (CVLT-2 z-score = −0.11), memory compared with published norms. 19 There were large, statistically significant differences among disability groups in aerobic capacity, F(2, 58) = 12.58, P < .01, partial-η2 = .31, KE peak torque, F(2, 59) = 10.68, P < .01, partial-η2 = .27, KF peak torque, F(2, 59) = 9.26, P < .01, partial-η2 = .24, KE asymmetry scores, F(2, 59) = 24.59, P < .01, partial-η2 = .46, KF asymmetry scores, F(2, 59) = 6.66, P < .01, partial-η2 = .18, SDMT scores, F(2, 59) = 12.15, P < .01, partial-η2 = .29), and CVLT-2 scores, F(2, 59) = 4.52, P = .02, partial-η2 = .13. However, there were not significant disability group differences in BVMT-R scores, F(2, 59) = 2.19, P = .12, partial-η2 = .07. Post hoc Bonferroni corrections indicated that overall, persons with severe disability had reduced aerobic capacity, weaker knee extensors, weaker knee flexors, greater asymmetries in knee extensor and flexor strength, slower cognitive processing speed, and worse verbal memory than persons with mild/moderate disability (Table 1).
Covariate Analyses
We considered age, sex, education, and DMT use as potential covariates—if those variables were jointly associated with fitness and cognitive outcomes in the overall sample. Age was associated with aerobic capacity, KE peak torque, KF peak torque, and KE asymmetry score (P < .02), but was not associated with KE asymmetry score and scores on the SDMT, CVLT, or BVMT (P > .06). There were substantial sex differences in aerobic capacity, knee extensor and knee flexor peak torque (P < .01), but there were no differences in KE asymmetry, KF asymmetry, SDMT, CVLT, or BVMT scores (P > .05). Education was not associated with any fitness or cognitive outcome (P > .24). There were small, but statistically significant differences based on DMT use in SDMT scores (P < .05), but not in any other fitness or cognitive outcome (P > .08). Accordingly, we did not include age, sex, education, or DMT use as covariates in subsequent analyses, given the lack of bivariate correlations with both fitness and cognitive variables.
Correlations Among Fitness and Cognitive Variables
Correlations among fitness and cognitive variables in the overall sample are presented in Table 2. Aerobic capacity (r = .41, P < .01), KE peak torque (r = .35, P < .01), KF peak torque (r = .39, P < .01), and KE asymmetry scores (r = −.36, P < .01) were moderately and significantly associated with SDMT scores, respectively. KF asymmetry scores were not significantly associated with SDMT scores (r = −.06, P = .32). Aerobic capacity was not significantly associated with CVLT-2 (r = .19, P = .07) or BVMT-R (r = .18, P = .08) scores, respectively. KE peak torque and KF peak torque, respectively, were not significantly associated with CVLT-2 (r = .07, P = .30; r = .13, P = .14, respectively) or BVMT-R (r = .09, P = .24; r = .08, P = .28, respectively) scores. Similarly, KE asymmetry scores and KF asymmetry scores, respectively, were not significantly associated with CVLT-2 (r = −.19, P = .07; r = −.09, P = .24, respectively) or BVMT-R (r = −.14, P = .14; r = −.04, P = .39, respectively) scores. This indicates that measures of aerobic and muscular fitness were associated with cognitive processing speed, but not verbal or visuospatial learning and memory.
Correlations Among Physical Fitness and Cognitive Variables in 62 Persons With Multiple Sclerosis.
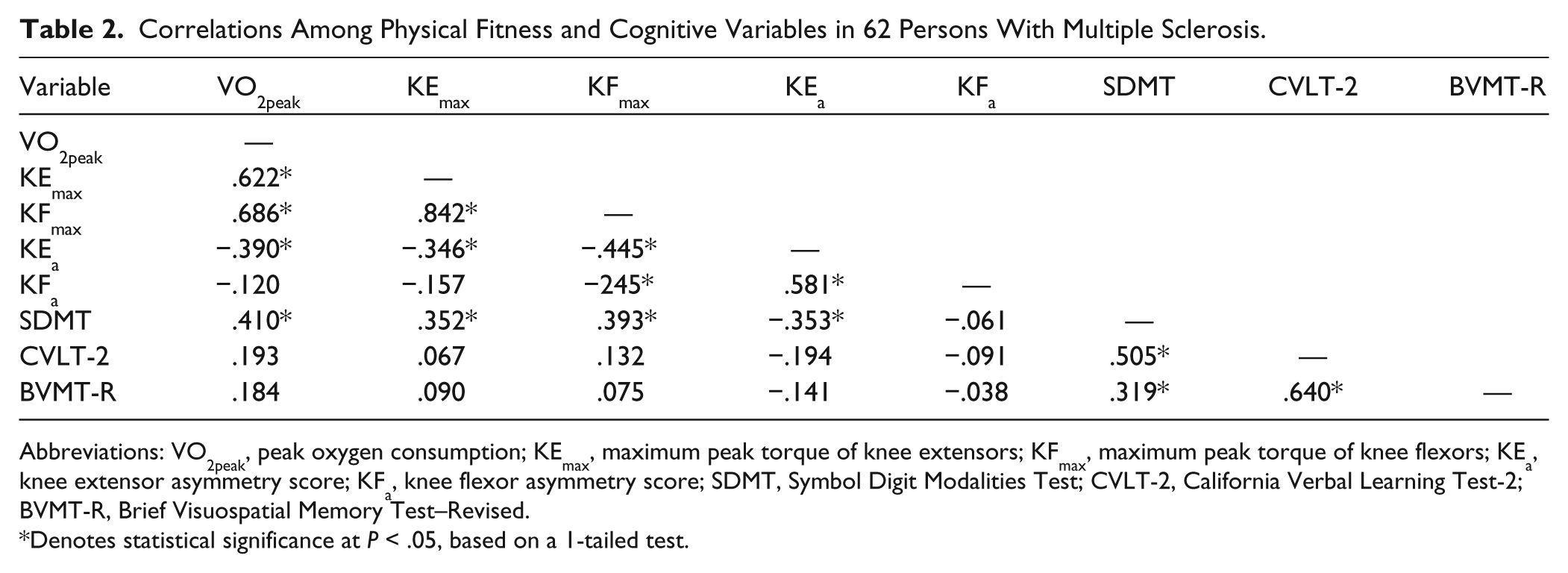
Abbreviations: VO2peak, peak oxygen consumption; KEmax, maximum peak torque of knee extensors; KFmax, maximum peak torque of knee flexors; KEa, knee extensor asymmetry score; KFa, knee flexor asymmetry score; SDMT, Symbol Digit Modalities Test; CVLT-2, California Verbal Learning Test-2; BVMT-R, Brief Visuospatial Memory Test–Revised.
Denotes statistical significance at P < .05, based on a 1-tailed test.
We next conducted bivariate correlations among aerobic capacity, KE peak torque, KF peak torque, KE asymmetry scores, and SDMT scores within the disability group subsamples (Table 3). Aerobic capacity (r = .42, P = .03), KF peak torque (r = .39, P = .04), and KE asymmetry scores (r = −.53, P = .01), but not KE peak torque (r = .20, P = .20), were significantly associated with SDMT scores in persons with mild disability. Aerobic capacity and muscular strength variables were not significantly associated with SDMT scores in persons with moderate (P > .05) and severe (P > .05) disability.
Correlations Among Physical Fitness and Cognitive Variables by Disability Status Subgroup.
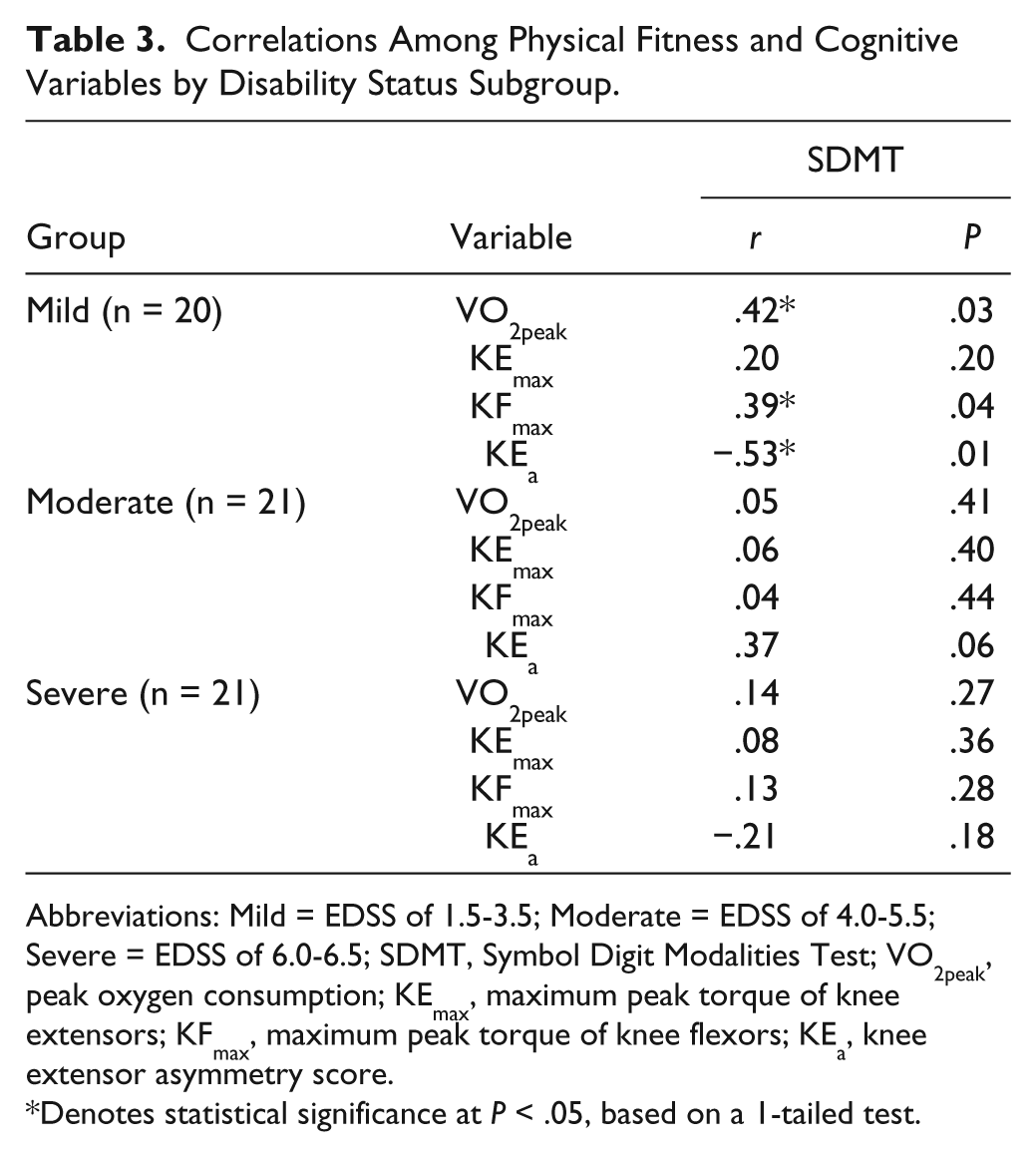
Abbreviations: Mild = EDSS of 1.5-3.5; Moderate = EDSS of 4.0-5.5; Severe = EDSS of 6.0-6.5; SDMT, Symbol Digit Modalities Test; VO2peak, peak oxygen consumption; KEmax, maximum peak torque of knee extensors; KFmax, maximum peak torque of knee flexors; KEa, knee extensor asymmetry score.
Denotes statistical significance at P < .05, based on a 1-tailed test.
We then performed additional, exploratory bivariate correlations among aerobic capacity, KE peak torque, KF peak torque, KE asymmetry scores, and SDMT scores in groups of persons with relapsing–remitting (n = 48) and progressive (n = 13) MS, separately. Briefly, aerobic capacity (r = .39, P < .01), KF peak torque (r = .27, P = .03), and KE asymmetry scores (r = −.29, P = .02) were associated with SDMT scores in persons with relapsing–remitting MS, although the magnitude of those associations was slightly weaker than in persons with mild MS disability. Aerobic capacity and KE asymmetry scores were not associated with SDMT scores in persons with progressive MS (P > .05), although KF peak torque was significantly associated with SDMT scores (r = .48, P = .05) in this group. This suggests that both disability status and clinical disease course similarly moderated the associations among fitness and cognition in MS.
Post hoc Regression Analysis
We conducted post hoc regression analysis with stepwise entry to determine whether aerobic capacity, KF peak torque, or KE asymmetry scores independently predicted SDMT scores in the overall sample, based on the statistically significant associations among aerobic capacity, KF peak torque, and KE asymmetry scores (Table 2). We did not perform this analysis in the mild MS disability subgroup based on the small sample size. Briefly, aerobic capacity entered into the equation alone (B = .75, SE B = .22, β = .41) and explained significant variance (R2 = .17) in SDMT scores. This indicates that aerobic capacity emerged as an independent predictor of cognitive processing speed.
Discussion
The current study is the first to directly examine the associations among multiple domains of physical fitness and cognitive function in 62 persons with different levels of MS disability in order to better inform exercise training interventions for improving specific cognitive functions in MS, possibly depending on disability status. Aerobic capacity and measures of muscular strength were associated with cognitive processing speed, but not learning and memory, in the overall sample. Disability was a moderator of those associations such that aerobic capacity, KF peak torque, and KE asymmetry score were associated with cognitive processing speed only in those with mild MS disability, perhaps due to those fitness outcomes being limited by lower limb/ambulatory disability. 28 Furthermore, in the overall sample, aerobic capacity independently explained approximately 17% of variance in cognitive processing speed. Collectively, this suggests that there is a selective association of physical fitness and cognitive function domains in persons with MS, such that aerobic fitness, and to a lesser extent lower limb muscle strength, is associated with the specific domain of cognitive processing speed among persons with MS, particularly those with mild disability. This seemingly supports the design and implementation of an aerobic exercise training intervention for improving cognitive processing speed in persons with mild MS disability. Conversely, the current results lead to the hypothesis that such an intervention might not benefit cognitive processing speed as much in persons with moderate or severe disability, consistent with a recent RCT. 7
One novel aspect of the current study is that we directly examined the differential associations of fitness and cognition based on disability status to explain a pattern of results from previous reports. To that end, the current results were not unexpected. We have previously observed significant associations between physical activity behavior and cognitive processing speed among persons with mild, but not moderate, MS disability in a different sample of persons with MS, using a prospective 10 and a RCT design. 11 Similarly, in the current study, clinical disease course moderated the associations among fitness and cognitive outcomes, such that aerobic capacity and muscle strength were associated with cognitive processing speed in persons with relapsing–remitting MS, but not in persons with progressive MS. The extension of this pattern of results from physical activity to physical fitness might further explain null results for cognitive processing speed from a recent aerobic exercise training intervention involving persons with progressive MS and moderate disability (mean EDSS = 4.95). 7 An EDSS score of 4.0 is indicative of irreversible disability that often presents as limitations in ambulation, 29 and frequently represents the onset of a secondary (oftentimes progressive) neurodegenerative disease process whereby disease modifying therapies have equivocal effects on reducing brain atrophy. 30 Perhaps the cardiorespiratory fitness–cognitive processing speed association is only applicable in persons with MS who have relatively high levels of physical function. Another potential explanation is that perhaps at this point of irreversible disability (ie, EDSS of 4.0), the secondary stage of the MS disease process overwhelms the capacity for aerobic exercise and physical activity to affect certain brain regions that are important for cognitive processing speed. Prior to reaching this critical point (ie, when MS is characterized by primarily inflammatory processes), it is plausible that the selective association of aerobic capacity and cognitive processing speed in mild MS, and perhaps relapsing–remitting MS, actually reflects the association between aerobic capacity and executive control that has been widely reported in the general population.31,32 Although the SDMT is primarily considered a neuropsychological measure of cognitive processing speed, it does require some degree of executive function (eg, working memory) to complete. To that end, a recent study reported that improvements in physical fitness were associated with improvements in executive function, but not information processing speed, in 88 persons with MS (disability status not reported 33 ). Future studies should examine the potentially differential effects of aerobic exercise on cognitive processing speed and underlying executive control processes more thoroughly in persons with mild MS to better inform an exercise training intervention for optimally improving cognitive function.
One important aspect of the current study involved the examination of aerobic capacity and learning and memory in MS. Aerobic capacity was not associated with verbal or visuospatial learning and memory in the overall sample. This is consistent with previous cross-sectional studies that did not report significant associations between aerobic capacity and verbal learning in persons with mild-to-moderate MS disability, without memory impairment.8,34 However, the lack of association between aerobic capacity and learning and memory in the current study was not entirely expected based on widely reported improvements in learning and memory following aerobic exercise training in older adults, 35 and a recent RCT that reported increases in verbal learning following aerobic exercise in persons with moderate MS disability. 7 In addition, a case study reported significant improvements in memory and concomitant increases in hippocampal volume following aerobic exercise training in 2 memory-impaired persons with MS. 36 Perhaps the association between aerobic fitness and memory might be contingent on the level of memory impairment in persons with MS, as the current sample did not demonstrate highly impaired memory based on normative CVLT-2 (z = −0.11) and BVMT-R (z = −0.96) scores. 19
Importantly, results from the current cross-sectional analysis indicated that muscular strength was associated with cognitive processing speed in the overall sample, and when analyzed within disability groups, this association was statistically significant only in those with mild MS disability. However, post hoc regression analysis in the overall sample indicated that aerobic capacity, but not muscular strength, was a significant predictor of cognitive processing speed (ie, aerobic capacity independently explained approximately 17% variance in cognitive processing speed), perhaps because of a large correlation between aerobic capacity and KF peak torque. This proportion of variance is consistent with results from a recently successful exercise training intervention in persons with MS, such that changes in aerobic capacity following cycle ergometry training explained approximately 16% of variance in changes in verbal learning. 7 Such results from the current study seemingly support combined aerobic and resistance exercise training for improving cognitive processing speed, with an emphasis on aerobic exercise, in persons with MS. Muscular strength was not associated with learning and memory in the current sample. There is mixed evidence supporting resistance exercise for improving memory based on animal work and studies involving older adults, perhaps based on an indirect pathway involving IGF-1, BDNF, and the hippocampus. 37 Future work is clearly necessary, as we are unaware of any other published studies examining the associations among muscular strength variables and memory in MS.
There are many strengths of the current study that include the use of objective assessments of physical fitness and use of validated neuropsychological tests of cognitive processing speed and learning and memory in persons with MS. There are important limitations. The primary limitation is the cross-sectional nature of the study as it does not indicate causation between improvements in physical fitness and cognitive processing speed. Indeed, physical fitness might influence cognitive function as much as cognitive function influences the capacity to exert maximal aerobic capacity and muscle strength during fitness tests; thus, the results should be interpreted with caution. We do note that this cross-sectional study was necessary prior to investing considerable time, effort, and resources into a longitudinal exercise training intervention. Furthermore, the range of disability within the mild MS disability group, based on EDSS scores, was greater than the range of disability within the moderate and severe MS disability groups, respectively. This might have influenced the strength of the correlations between fitness and cognitive processing speed within each disability group, though these EDSS groupings are consistent with research on ambulation in MS. 21 Another limitation involves the difficulty in measuring aerobic capacity in persons with substantial MS disability. In persons with severely limited lower and upper extremity motor function, oftentimes it is difficult to reach maximal aerobic capacity (ie, VO2max)28,38 during an incremental exercise test, which might bias the association between aerobic capacity and cognitive processing speed. We conducted the incremental exercise test to exhaustion on a recumbent stepper in order to minimize this issue, and the proportion of participants meeting the criteria for VO2peak in the current study did not differ between disability groups, χ2 (df = 2) = 4.76, P = .09. The large overall sample size was a strength of the current study; however, the smaller sample sizes in each disability group were a limitation in that we were unable to perform post hoc regression analyses on aerobic capacity, KF peak torque, and KE asymmetry as predictors of cognitive processing speed in persons with mild MS disability only. There was a high proportion of persons with relapsing–remitting MS in the severe MS disability group, despite the stratification of participants into EDSS groups of mild, moderate, and severe disability. However, as expected, the number of relapsing–remitting cases within the severe disability group was significantly lower than in the mild and moderate disability groups. To account for this potential limitation, we performed an additional, exploratory analysis by recategorizing the data based on clinical disease course. Importantly, both disability status and clinical disease course similarly moderated the associations among fitness and cognition in MS. One final limitation involves the lack of a comparison group of healthy controls matched by age, sex, height, and weight. This would be useful for comparing the specificity of the associations among fitness and cognitive outcomes in persons with mild MS disability with healthy controls.
Conclusions
The primary novel findings from the current cross-sectional study of 62 persons with mild, moderate, and severe MS were that (a) in the overall sample, measures of physical fitness were associated with cognitive processing speed, but not learning and memory, and (b) physical fitness was associated with cognitive processing speed in persons with mild, but not moderate or severe, MS disability. Collectively, this suggests that disability is indeed a moderator of the association among fitness outcomes and cognitive processing speed and supports the advent of aerobic exercise training interventions, in particular, for improving cognitive processing speed in persons with mild MS. This is important in that aerobic exercise represents a promising symptom management tool for potentially mitigating slowed cognitive processing speed, particularly among persons with mild MS disability.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a grant from the National Multiple Sclerosis Society, Grant Number IL0003.