
Abstract
Background. The vestibular system is vital for gaze stability via the vestibulo-ocular reflex, which generates compensatory eye motion in the direction opposite to head motion. Consequently, individuals with peripheral vestibular loss demonstrate impaired gaze stability that reduces functional capacity and quality of life. To facilitate patients’ compensatory strategies, two classes of gaze stabilization exercises are often prescribed: (i) transient (eg, ballistic) and (ii) continuous. However, the relative benefits of these two classes of exercises are not well understood. Objective. To quantify head motion kinematics in patients with vestibular loss while they performed both classes of exercises. Methods. Using inertial measurement units, head movements of 18 vestibular schwannoma patients were measured before and after surgical deafferentation and compared with age-matched controls. Results. We found that the head movement during both classes of exercises paralleled those of natural head movement recorded during daily activities. However, head movement patterns were more informative for continuous than transient exercises in distinguishing patients from healthy controls. Specifically, we observed coupling between kinematic measures in control subjects that was absent in patients for continuous but not transient head motion exercises. In addition, kinematic measures (eg, cycle duration) were predictive of standard clinical measures for continuous but not transient head motion exercises. Conclusions. Our data suggest that performing continuous head motion is a greater motor control challenge than transient head motion in patients with less reliable vestibular feedback during the sub-acute stage of recovery, which may also prove to be a reliable measure of progression in vestibular rehabilitation protocols.
Introduction
Gaze stability is the ability of the eyes to fixate at a stable point when the head is moving in space, which allows us to maintain a clear vision during daily activities such as walking, running, and driving. This function is supported by the vestibular system in the inner ear, where the time varying dynamics of head motion are encoded by the vestibular organs and sent through the vestibular nerve to its respective brain nuclei. These events trigger the vestibulo-ocular-reflex (VOR), which is required to generate compensatory eye movements that effectively maintain gaze direction in space. 1 Notably, head motion has significant power up to 20 Hz and routinely reaches peak rotational velocities of 100–250 deg/s during daily activities such as walking on a busy city sidewalk or riding on a bus.2,3 The VOR is thus required to make compensation possible over the frequency range of natural head movements, whereas the dynamics of the visually driven pursuit and optokinetic systems are too slow (see 4 ). Accordingly, in individuals with a compromised vestibular system, the VOR is impaired, resulting in blurred vision, motion sensitivity, increased fall risk, and low health-related quality of life.5,6
Gaze stabilization exercises improve gaze stability after vestibular loss.7-10 These exercises facilitate compensation of vestibular loss by helping patients to practice stabilizing their gaze direction during head motion. This is done both via central compensation mechanisms within the vestibular pathways, as well as changes in the coupling of corrective saccades and head motion.11,12 While healthy subjects maintain gaze by generating smooth compensatory slow phase eye movements opposing the head movement, patients with vestibular loss generate a saccade near the onset of the head movement 13 or during the head movement.14-18 There is conflicting evidence that the magnitude of the slow phase is enhanced by such exercises in patients with vestibular loss.12,19,20 Occasionally, the slow phase of the VOR recovers to rapid head rotation, albeit incompletely.21-23
While oculomotor behavior (saccadic and VOR) has been investigated as compensatory strategies in patients with vestibular hypofunction, less is known about the head movement strategies used during gaze stabilization exercises. Since gaze stabilization exercises involve both head movement and eye movement, we hypothesized that patients also change their head movement pattern to compensate for the vestibular loss. It has been reported that patients move their heads slower during daily life, 23 putatively to facilitate the anticipation of gaze instability with head rotation, or adopt different, less efficient, movement strategies to perform everyday tasks. 24 Thus, we believe that the information drawn from the quantification of head motion trajectories can add to a more comprehensive understanding of compensatory strategies in vestibular dysfunction.
Typical gaze stabilization exercises require patients to fixate on a target while moving their head horizontally or vertically. Prescription of gaze stabilization exercises varies in the distance between the target and the patient, head velocity, and the pattern and direction of head motion. These exercises are broadly categorized into two classes of head motion: continuous (ie, side to side) and transient (ie, with pause in between). Although continuous head motion is less common than transient head motion in relation to daily activities, each offers a unique opportunity to examine strategies of compensation related to head movement dynamics. Further, both continuous and transient head movements are essential to functional mobility, yet our knowledge on the extent to which they are affected by vestibular schwannoma, or by its resection, remains limited. Accordingly, the investigation of both types of exercises is important as they may hold unique properties related to sensorimotor compensation from a vestibular deficit.
In this study, we investigate compensatory strategies of head motion in patients with unilateral vestibular loss. We have analyzed patients’ head movement patterns in both continuous and transient gaze stabilization exercises, before and after resection of vestibular schwannoma. Notably, the dynamics of the head movements generated in both types of exercises (peak head velocities ∼100–300 deg/s, frequency range extending to ∼20 Hz) paralleled those of natural head movement recorded during daily activities.2,3,25,26 We then compared the head movement patterns of patients to those of healthy controls to reveal patients’ compensatory strategies.
Methods
Subjects
Eighteen patients (12 males and 6 females, mean age = 53.8 ± 13.0 years old, range = 24–73 years old) who were diagnosed with unilateral schwannoma and had scheduled a resection surgery were recruited. Nine of those patients (9 males, mean age = 56.1 ± 15.7 years old, range = 24–73 years old) completed the study both before and 6 weeks after the surgery. Subjectively, of the 9 patients, three patients reported imbalance, three reported dizziness, and six reported hearing loss. None of these nine subjects were actively followed by vestibular rehabilitation on a regular basis. Nine patients were lost to follow-up because they could not complete the study due to surgical complexity, or they resided out of state. Nine age-matched healthy participants (mean age = 49.3 ± 15.0 years old, range = 24–72 years old) who did not have any history of otologic or neurologic disease served as controls. This study was approved by the Johns Hopkins University Institutional Review Board, and written informed consent was obtained from each participant prior to data collection.
Overview
The pre-surgery measures were collected in an outpatient setting before the vestibular schwannoma tumor resection surgery. The post-surgery measures were collected at the sixth week (36–42 days) after the surgery. Traditional clinical measures and kinematic measures were collected concurrently and at both clinical visits, including abnormal audiogram and the six canal video head impulse test (Supplemental Table 1).
Kinematic Measurements
A list of the 12-gaze stabilization exercises used in the current study. The exercises vary in movement pattern, target type, and direction of head movement (represented in the table as “Dir.”. Transient exercises require subjects to make a head movement and pause before the next movement is made in the opposite direction. Continuous exercises require subjects to move their head repeatedly as fast as possible. “Hand” refers to the target being held by their dominant hand.
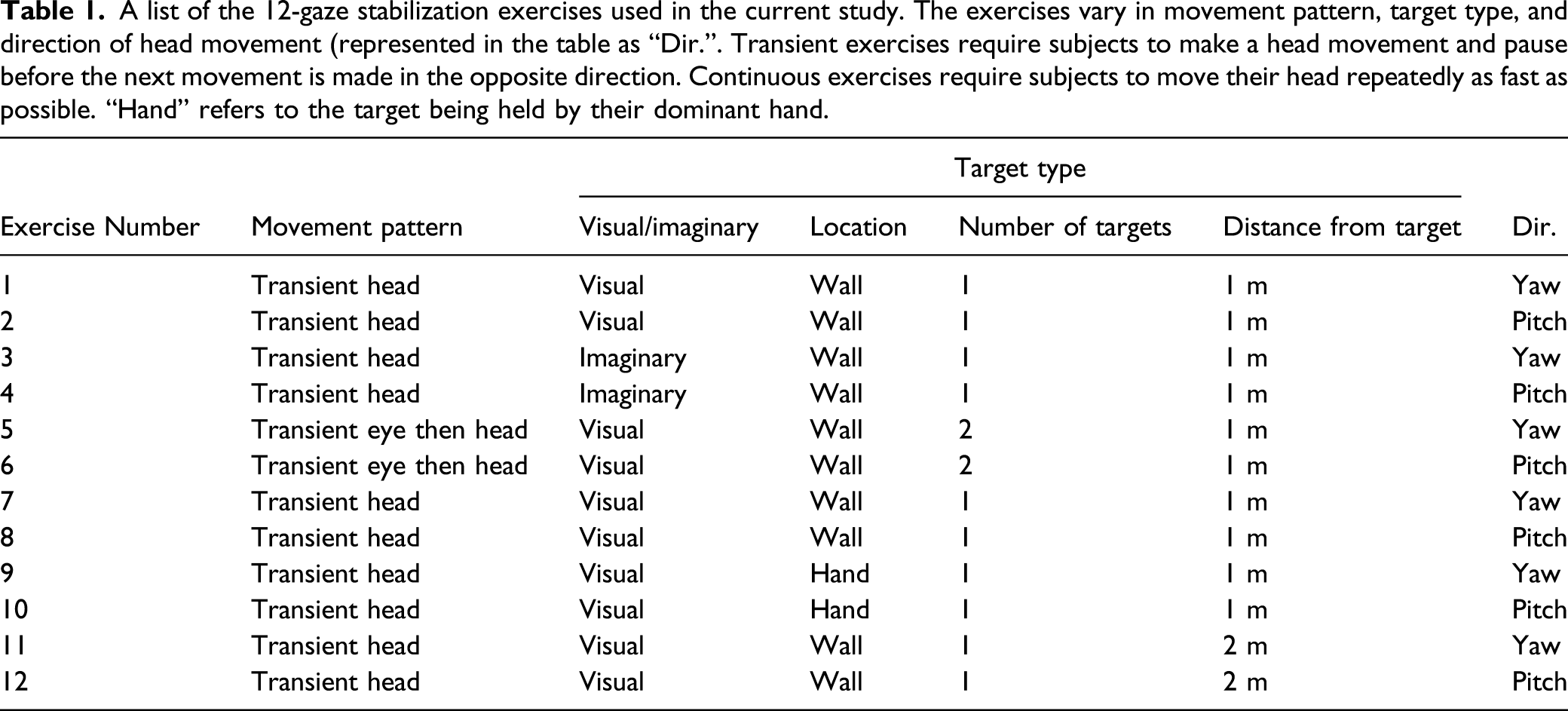
The six transient exercises included (Table 1, exercises 1–6) active (participant generated) head impulses while viewing a stable target (Table 1, exercises 1 and 2), active head impulses with an imaginary target (ie, eyes closed; Table 1, exercises 3 and 4), and eye-head gaze shifts, each performed, from a 1 m distance, in two movement directions (yaw and pitch; Table 1, exercises 5 and 6). Specifically, the active head impulse exercises required subjects to make a transient head movement to one side, return their head direction to the center, make a transient head movement to the other side, return their head direction to the center, and repeat (Table 1, exercises 1 and 2). The active head impulse imaginary target exercises were similar to the active head impulse, except that with imaginary target subjects were required to keep their eyes closed while making the transient head movement still attempting to keep their gaze focused on the target, even though they could no longer see (Table 1, exercises 3 and 4). Finally, for the eye-head gaze shift exercises, subjects alternated their gaze between two targets fixed on the wall 60 cm apart. Specifically, subjects stood in front of the middle of two targets with their head and gaze direction fixated at one of the targets. They were instructed to shift their gaze to the other target without moving their head and then turn their head toward that same target, realigning head and gaze direction (Table 1, exercises 5 and 6).
The six continuous exercises were also performed during yaw and pitch head motion. The exercises varied in target fixation (on the wall or held by the patient) and distance between target and patient (1 or 2 m, Table 1, exercises 7–12, see also 27 ). During the continuous exercises, subjects stood in front of a visual target (an X marked on paper) and made head movements continuously in one dimension for 30 seconds (ie, pitch), while keeping the target in focus. All subjects were instructed to move their head as fast as possible ensuring the target remained in focus.
The sensor was attached to the back of the subjects’ head using an elastic head band. The sensor module was 51 mm × 34 mm × 14 mm and extremely light, thus can be comfortably attached to the subjects’ head with little interference on their head movement. The plane spanned by the fore-aft, and the inter-aural axis of the sensor was set parallel to the subjects’ Frankfurt plane (ie, the plane passing through the inferior margin of the orbit to the external auditory meatus). The sensor collected head movement at six dimensions (angular velocity at three gyroscopic dimensions: roll, pitch, and yaw; and linear acceleration at three dimensions: fore-aft, inter-aural, and vertical). The data were sampled at 500 Hz and recorded on a built-in microSD card. Only the gyroscopic dimension aligned with the head moving direction of the gaze stabilization exercises was analyzed (eg, yaw in horizontal exercises and pitch in vertical exercises).
Data Analysis
Kinematic measurements were calculated based on the head angular velocity recorded by the sensor. We divided the head motion into individual cycles. In continuous exercises, each cycle was defined as the head moving from one end (eg, left or up) to the other end (eg, right or down). In transient exercises, each cycle was defined as the head moving from the center to one end (eg, left, right, up, or down). Mean peak velocity is the average of the peak velocity in each cycle. Coefficient of variation (CV) of peak velocity is the standard deviation divided by the mean peak velocity. Cycle duration is the time spent to finish each cycle, and CV cycle duration is the standard deviation divided by the mean of cycle duration. By integrating the angular velocity, we calculated the amplitude of head rotation in each cycle. Mean move range is the average range of motion, and CV move range is the standard deviation divided by the mean of range of motion. Asymmetry measurements were calculated by dividing the ipsilesional or up measurements by the contralesional or down measurements, respectively. For example, asymmetries between kinematic measures of ipsilesional and contralesional head movements were computed by dividing the former by the latter. Correlations between measurements were calculated to reveal the patients’ head movement patterns. We also computed the power spectral densities of angular head velocity during each exercise using Welch’s averaged periodogram with a Bartlett window (2048 ms duration, 50% overlap) and 0.1 Hz frequency resolution (Pwelch function, MATLAB, MathWorks).
Results
Examples of the head movements generated by a typical healthy control vs a patient during pre-surgery and post-surgery testing are shown in Figure 1. Figure 1A shows the time course of the head velocities generated during a transient horizontal gaze stability exercise made while standing and viewing a target fixed on the wall 1 m away (see Methods). Figure 1B shows the time course of the head velocities during a continuous horizontal gaze stability exercise also made while standing and viewing a target fixed on the wall 2 m away (see Methods). These example data clearly demonstrate a difference in the head movement pattern of this patient and healthy control during a continuous exercise, but not during a transient exercise. In particular, the example patient and healthy control had comparable range of movement in the transient exercise (Figure 1A, bar plot), while the example patient had a larger range of head movement than the healthy control in the continuous exercise before and after the surgery (Figure 1B, bar plot). Example data from one healthy control and one patient in preoperative and postoperative testing during (A) a transient horizontal gaze stability exercise with the target fixed on the wall and 1m away and (B) a continuous horizontal gaze stability exercise with the target fixed on the wall and 2m away. Grey traces and shades show the mean and standard deviation of head velocity, respectively. Bar plots on the upper right corner compare the range of motion calculated from the example data. (C & D) comparing the mean range of motion from all the subjects during the example transient (C) and continuous (D) exercises. Insets: power spectrum of horizontal angular head velocity during the example transient (C) and continuous (D) exercises, where the superimposed blue trace corresponds to the power spectra of the horizontal angular head velocity measured during natural voluntary behaviours.
26
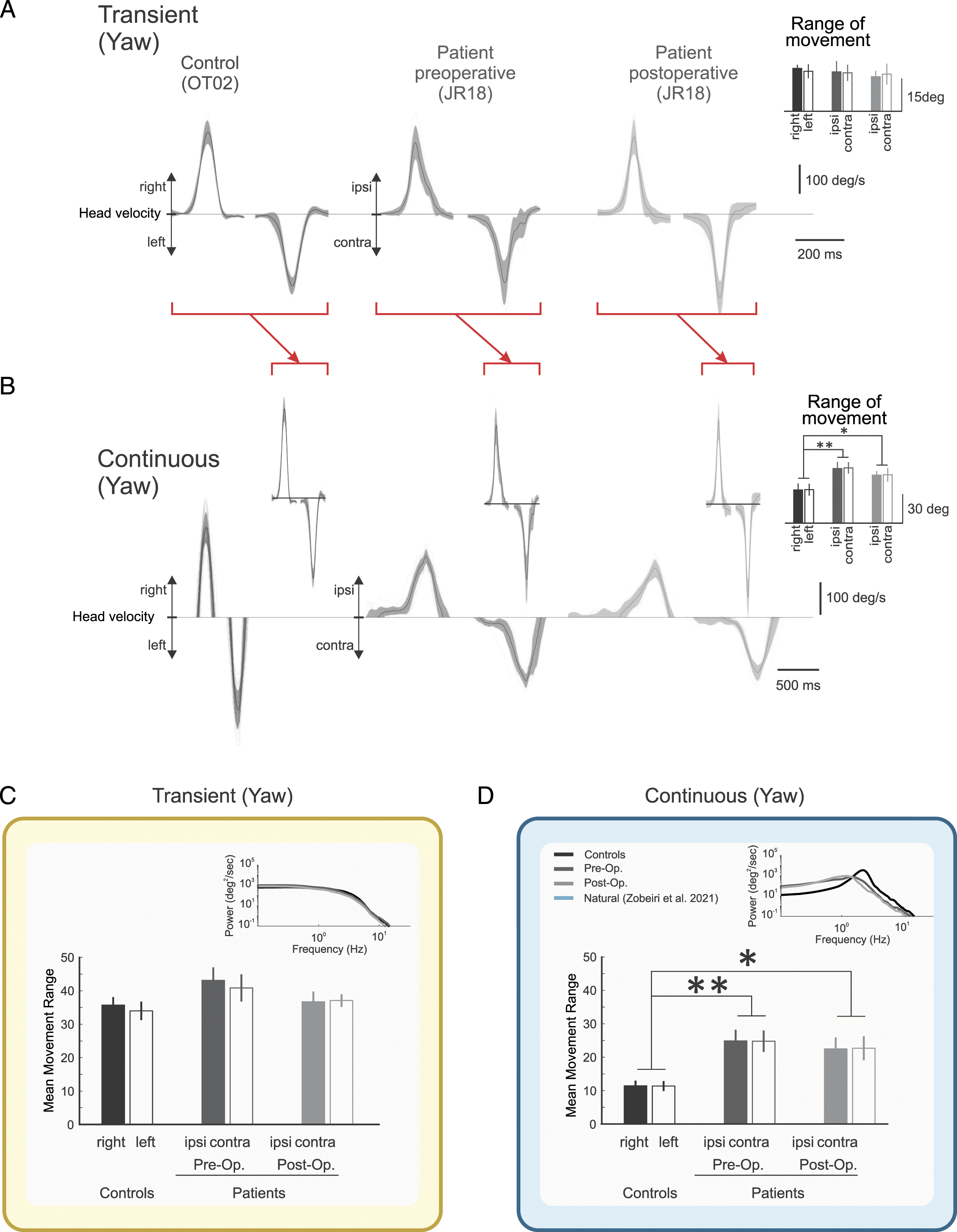
The above observations held true when we compared the range of head motion during the example continuous and transient exercises for all patients and control subjects (Figure 1C, D). Furthermore, the intra-subject range of movement variability was comparable in patients and controls for the example transient exercise (Figure 1C; compare standard deviation of the means). Conversely, the inter-subject range of movement variability was greater in patients than controls for the example continuous exercise (Figure 1D, p < .01). Correspondingly, an analysis of the frequency content of the head movements revealed that power spectra were comparable for patients’ and healthy controls during the transient exercise (Figure 1C, inset). During the continuous exercise, however, patients’ head motion showed reduced power and frequency (Figure 1D, inset, black vs grey traces, data plotted for comparison from Table 2 27 ). Interestingly, the spectral power of head motion generated during both types of exercises paralleled that observed for natural head movement in terms of amplitude and frequency range 26 (Figures 1C and 1D, insets, blue curves).
We next investigated how the head movement kinematics generated by patients pre- and post-surgery differed from those generated by controls during transient exercises (Figure 2). First, our comparison of ipsilesional and contralesional movement did not reveal any significant differences. Even once ipsilesional and contralesional data were combined to increase the data set for each comparison, we found few differences across groups for the transient exercises (yellow shaded area). This contrasts with the striking differences observed in the head movement kinematics generated by patients pre- and post-surgery vs controls during continuous exercises (blue shaded area, data replotted from
27
). Notably, pre-operative patients had a longer cycle duration for all continuous exercises and a wider range of motion in three of the six continuous exercises compared to healthy controls (Figure 2A). Similarly, while post-operative patients also had a longer cycle duration and a wider range of motion in all continuous exercises compared to healthy controls (Figure 2B, blue shaded area, data replotted from
27
), no such pattern was found in the transient exercises (Figure 2B, yellow shaded area). In addition, post-operative patients showed decreased coefficient of variation (CV) of range of motion compared to healthy controls in all continuous exercises, which was not the case for transient exercises. Comparison of kinematic measurements between (A) preoperative patients and healthy controls, (B) postoperative patients and healthy controls. Columns correspond to different kinematic measurements, while rows correspond to the 6 transient gaze stability exercises (yellow shaded areas) and 6 continuous gaze stability exercises (blue shaded areas), where the latter are replotted from
27
to facilitate comparison. In addition, the small yellow and blue rectangles within each shaded area correspond to the bar plots illustrated in figures 1C and 1D, respectively. Asterisks indicate differences at three significance levels (∗: 0.05, ∗∗: 0.01. ∗∗∗: 0.001). Black asterisks indicate that the first group, as indicated in the title, had a larger value than the second group and grey asterisks indicate that the first group had a smaller value than the second group.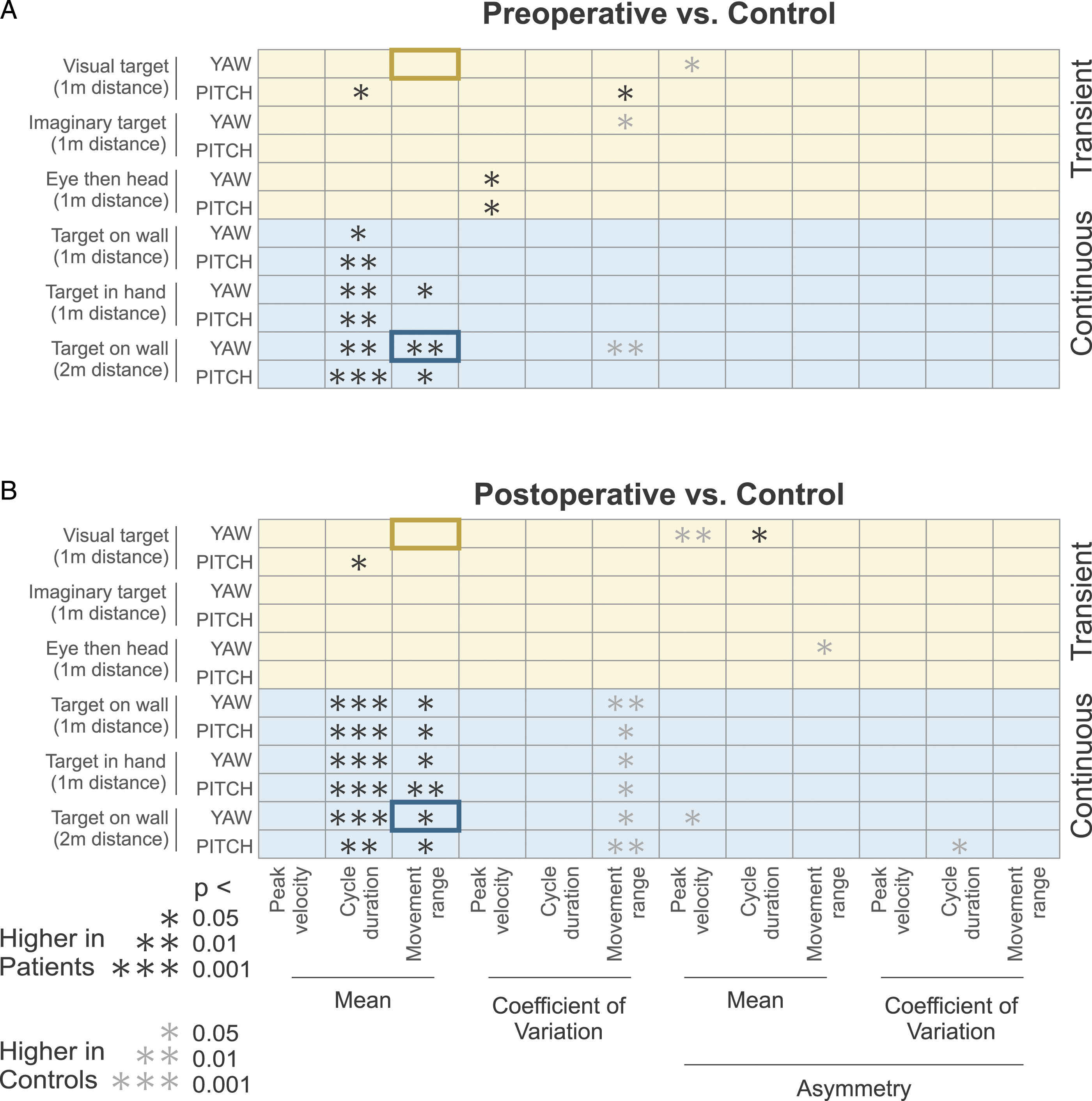
To investigate potential differences in the movement strategies used by patients vs controls during both types of exercises, we analyzed the relationship between different kinematic measures. Figure 3A shows an example of this analysis for the relationship between mean peak velocity and mean range of head motion in healthy controls (circles), pre-operative patients (squares), and post-operative patients (crosses) for two transient (yellow box) and one continuous exercises (blue box). In transient exercises with a visual target and horizontal head rotations, significant correlations were only found between these measures in pre-operative patients but not in healthy controls and post-operative patients. In transient exercises with an imaginary target and horizontal head rotations, movement range and peak velocity were significantly correlated in both pre- and post-operative patients, as well as in healthy controls. In continuous exercises with a visual target and horizontal head rotations, significant correlation between mean peak velocity and range of motion was found only in healthy controls, but not in pre- or post-operative patients. Specifically, this relationship for healthy controls can be well fit by a straight line (R = .95, Figure 3A, right panel), that provides a baseline for assessing impairment in patients performing continuous gaze stabilization exercises. The relationship between the specific kinematic measurements during gaze stability exercises. (A) Scatter plots showing the correlation between mean movement range and mean peak velocity. Lines correspond to the best linear fit showing significantly correlated relationships. (B) Illustration of the number of transient exercises during which the kinematic measurements were significantly correlated for healthy controls (left), preoperative patients (middle) and postoperative patients (right). (C) Illustration of the number of continuous exercises during which the kinematic measurements were significantly correlated for healthy controls (left), preoperative patients (middle) and postoperative patients (right). Green and red squares indicate positive negative correlations, respectively. Brightness and number in the square indicate the number of exercises (0-6) showing a significant correlation (p < .05).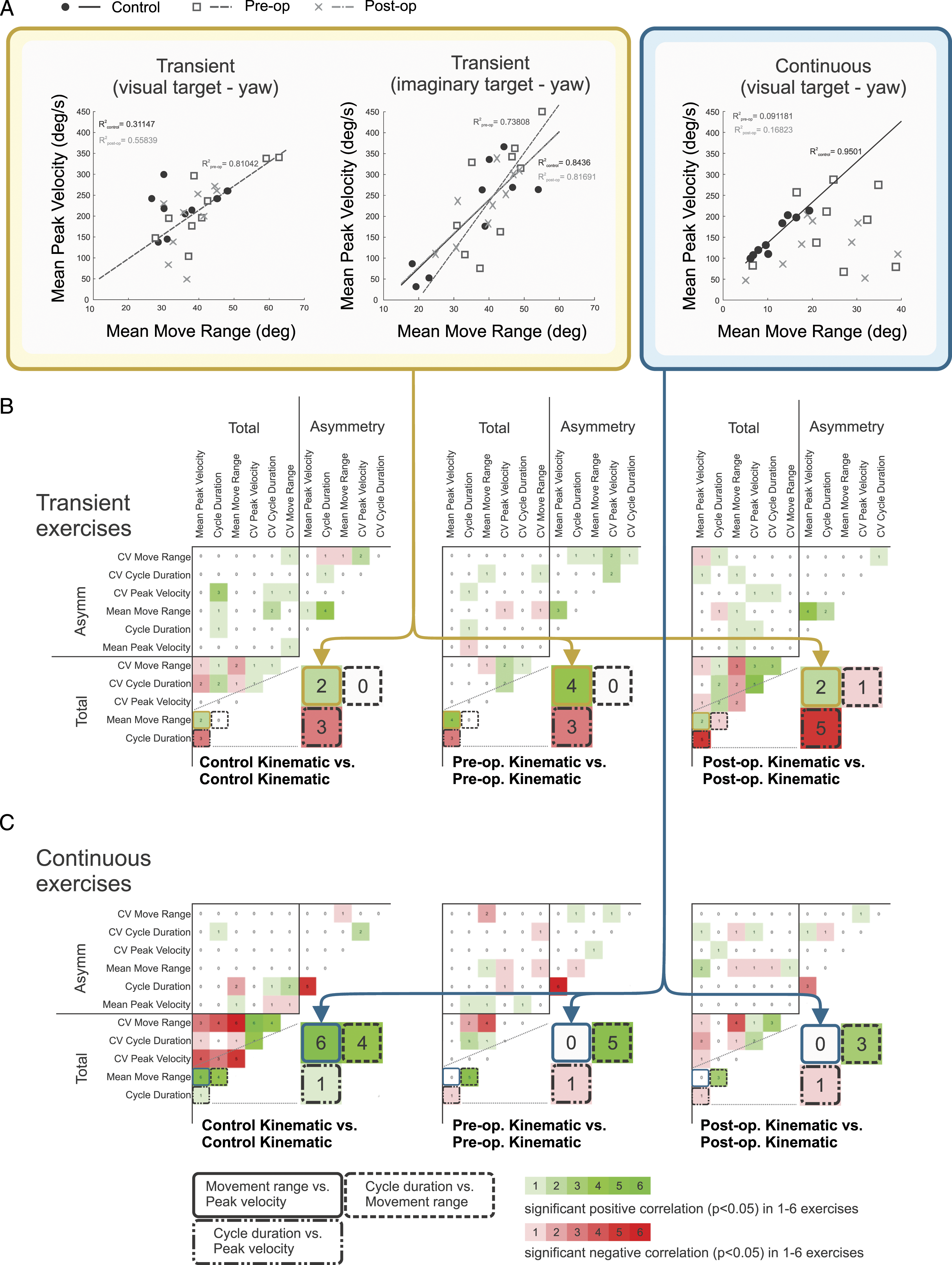
Figures 3B and 3C plot the summary of our correlation analyses between kinematic measures for healthy controls (left panels), pre-operative patients (middle panels), and post-operative patients (right panels) during all transient and continuous exercises, respectively. As shown in Figure 3B, our analysis of head kinematics in the transient exercises did not reveal distinctive correlation patterns that were consistent across patients and control subjects. First, even in healthy controls, we did not find significantly consistent correlations between kinematic measures across the transient exercises, with the exceptions that asymmetry of mean move range was positively correlated with asymmetry of cycle duration in four of the six transient exercises, and cycle duration was negatively correlated with mean peak velocity in three of the six transient exercises. Significant correlations were different (and again sparse) in pre-operative patients: mean peak velocity was positively correlated with mean move range in four of the six transient exercises and was negatively correlated with cycle duration in three of the six exercises; asymmetry of mean move range was positively correlated with asymmetry of mean peak velocity in three of the six transient exercises. Finally, correlations between kinematic measures were most prevalent in our analysis of post-operative patients. We found that their mean peak velocity was negatively correlated with cycle duration in five of the six exercises, CV move range was negatively correlated with mean move range and was positively correlated with CV peak velocity and CV cycle duration in three of the six transient exercises, CV cycle duration was positively correlated with CV peak velocity in five of the six transient exercises, and asymmetry of mean move range was positively correlated with asymmetry of mean peak velocity in four of the six transient exercises. Altogether, post-operative patients showed more correlation between head motion kinematic measures than healthy controls and pre-operative patients during transient exercises, but these correlations were not consistent across exercises.
Interestingly, our analysis of head kinematics in continuous exercises revealed strikingly different results, with distinctive patterns of correlation that were consistent across control subjects and patients before and after the surgery (Figure 3C). In healthy controls, most measurements, except the asymmetry measurements, were significantly correlated in more than half of the continuous exercises. Specifically, CV move range, CV peak velocity, and CV cycle duration are positively correlated with each other. CV move range and CV peak velocity are negatively correlated with mean peak velocity and mean move range. Mean move range is positively correlated with mean peak velocity and cycle duration. However, in pre- and post-operative patients, most of the correlations found in healthy controls were absent. The only significant correlations consistently observed in patients are that mean move range is positively correlated with cycle duration and negatively correlated with CV move range.
Next, we directly assessed the relationship between changes in specific kinematic measures observed before vs after surgery. To measure the change, we computed the difference between each kinematic measure in the post-operative and pre-operative states. Specifically, for a given exercise, we calculated the change (delta) of each measurement for each patient, by subtracting the pre-surgery values from the post-surgery values. Figure 4A shows the correlations between computed deltas (Δ) for each head kinematic measure. For the transient exercises, changes in peak head velocity were consistently positively correlated with changes in movement range. In contrast, we did not see this relationship during continuous exercises (Figure 4B, left). Instead, for these exercises, changes in mean move range were positively correlated with the delta of cycle duration, and changes in the asymmetry of cycle duration were negatively correlated with changes in the asymmetry of mean peak velocity (Figure 4B, right). These results again suggest that patients deploy different compensatory strategies when performing gaze stability exercises involving continuous and transient head motion. In the first, patients significantly reduced their head velocities, thereby increasing movement cycle duration using a strategy that likely enabled better gaze fixation. In the latter, however, faster velocities were associated with larger ranges of motion during head movement of a transient nature–a behavior comparable to that of healthy controls. The relationship between changes in specific kinematic measures observed in preoperative versus postoperative. (A) Correlations between changes (Δ: post-surgery – pre-surgery) in kinematic measurements during transient (left) and continuous (right) exercises. Green and red squares indicate positive and negative correlations, respectively. Brightness and number in the square indicate the number of exercises (1-6) showing a significant correlation (p < .05). (B) Left: Scatter plots showing the correlation between changes in mean movement range and those in mean peak velocity during yaw head movements (top) and pitch head movements (bottom). Right: Scatter plots showing the correlation between changes in cycle duration asymmetry and those in peak velocity asymmetry during yaw head movements (top) and pitch head movements (bottom).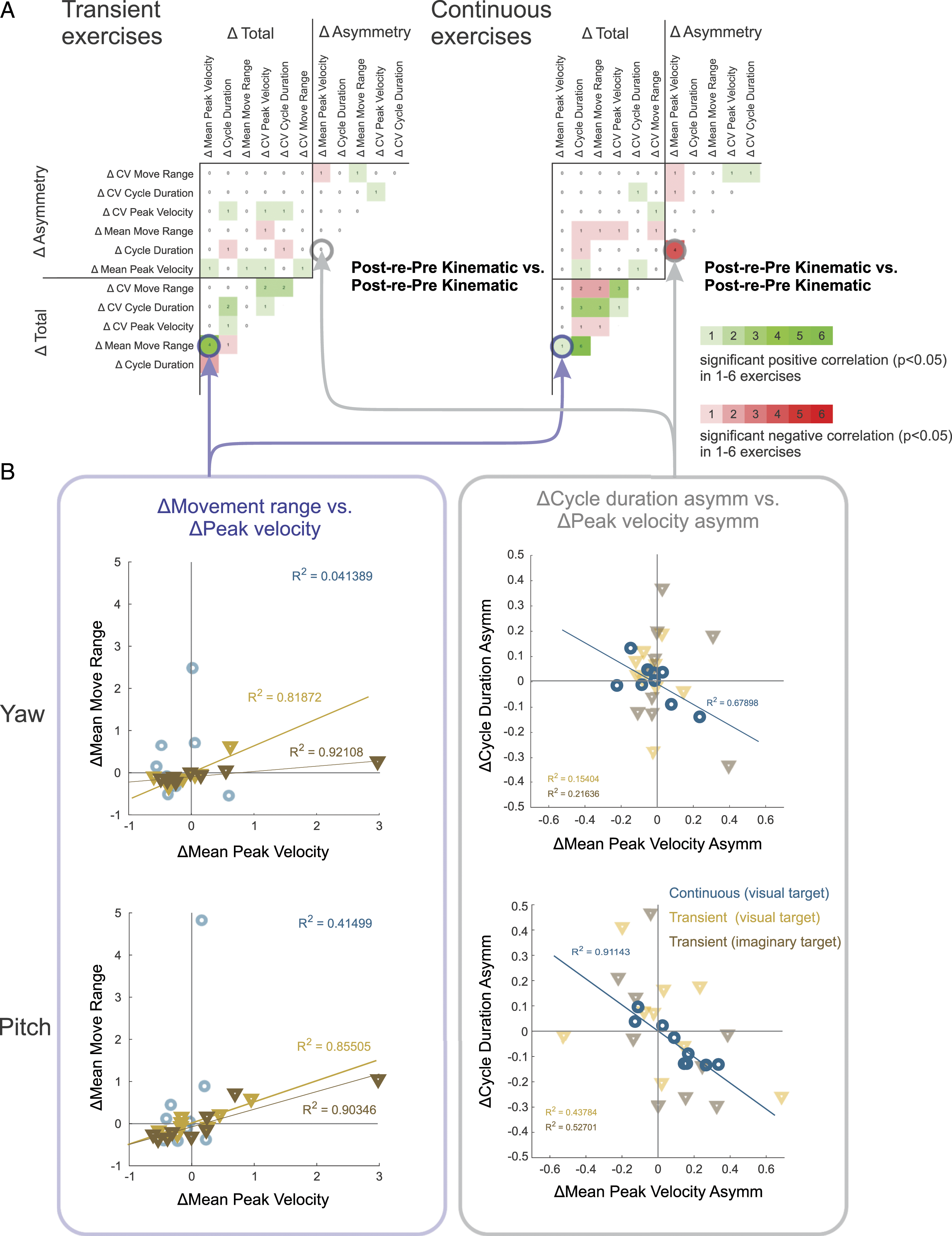
Finally, we assessed the relationship between kinematic measures and clinical measures. As shown in Figure 5A, there were not many significant correlations between pre-operative clinical measurements and pre-operative kinematic measurements. The significant correlations observed were not consistent across different exercises. Figure 5B shows a closer look at the correlations between kinematic measurements and the functional clinical measurements such as the Dynamic Visual Acuity (DVA), Timed Up and Go (TUG), and gait speed and Functional Gait Assessment (FGA) scores, before and after surgery. Again, we found that transient exercises (Figure 5B, top: yellow shaded areas) were less informative than continuous exercises (Figure 5B, bottom: blue shaded areas, data replotted from
27
for comparison). Specifically, there were more significant correlations between kinematic measures and clinical measures for continuous exercises than in transient exercises at all stages of assessment. Notably, of the kinematic measurements, cycle duration correlated most consistently with clinical measurements. Thus, preoperatively, a patient who had a longer cycle duration would be expected to have worse DVA scores, take a longer time to complete the TUG task, and walk slower. To investigate whether a patient’s subjective scoring of their symptoms correlated with their motor performance, we then completed a parallel analysis examining the relationship between kinematic measures and subjective clinical measures (Supplemental Figure 1). In contrast to our analysis of functional measures above, we did not find consistent correlations between kinematic measures and subjective clinical measures for either transient or continuous head motion. The relationship between specific clinical and kinematic measurements during gaze stability exercises. (A) Illustration of the number of transient exercises during which the preoperative kinematic measurements were significantly correlated with preoperative clinical measurements. (B) Number of transient (top; yellow shaded areas) and continuous (bottom; blue shaded areas, replotted from
27
to facilitate comparison) gaze stability exercises during which the functional clinical measurements were significantly correlated with kinematic measurements in comparisons for all stages of assessment, that is (i) preoperative clinical measurements with preoperative kinematic measurements, (ii) postoperative clinical measurements with postoperative kinematic measurements, and/or (iii) preoperative clinical measurements with postoperative kinematic measurements. Green squares and red indicate positive and negative correlations, respectively. Brightness and number in the square indicate the number of exercises (1-6) showing a significant correlation (p < .05).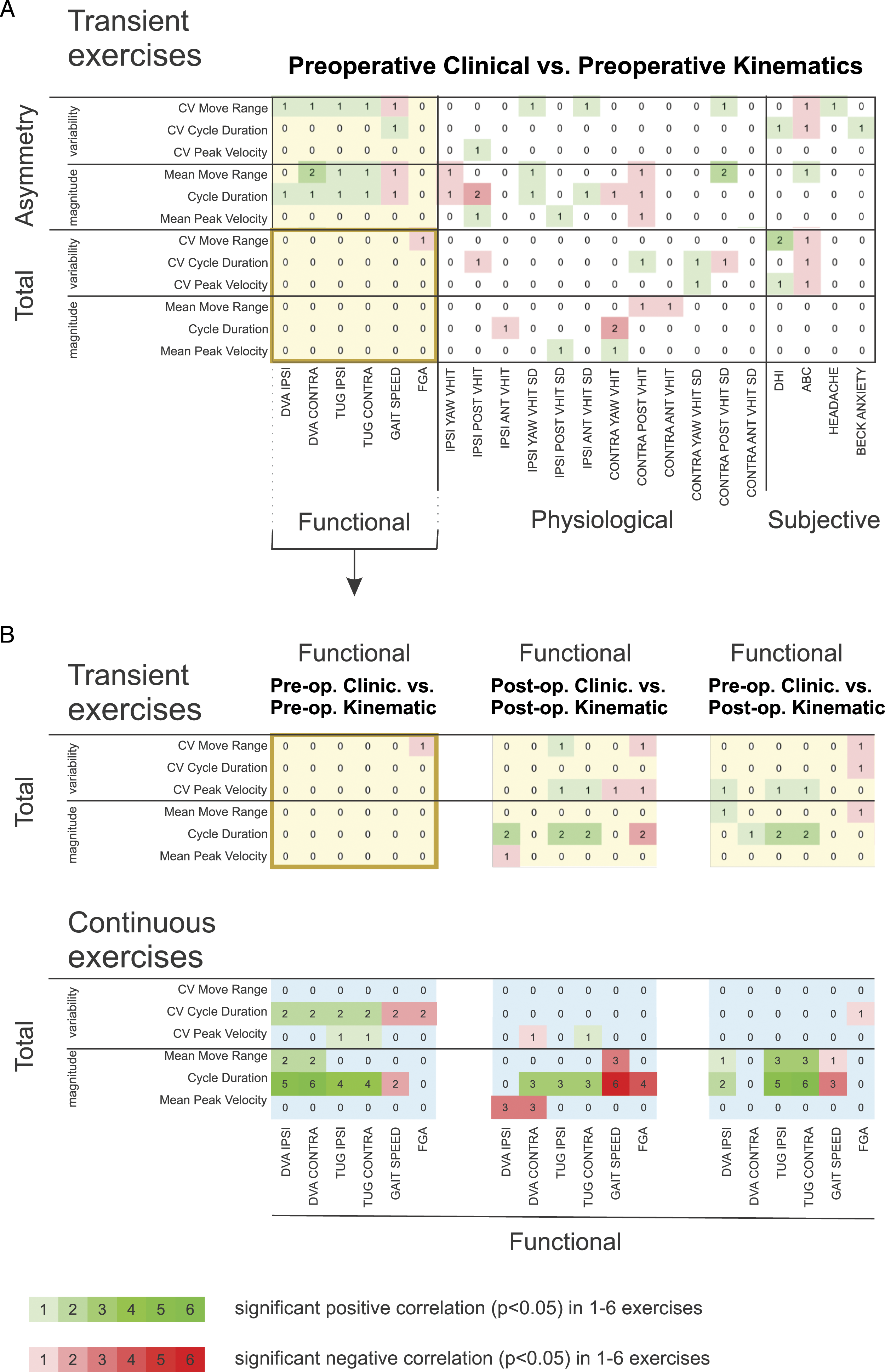
Discussion
This study examined head motion kinematics during two types of standard active gaze stabilization exercises in patients pre- and post-vestibular deafferentation surgery at the sub-acute stage of recovery. We found that continuous exercises are more informative than transient exercises in distinguishing patients’ head movement pattern from healthy controls in three primary ways. That is, for continuous exercises only, (1) kinematic characteristics (cycle duration and range of motion) are different between patients and healthy controls (Figures 1 and 2), (2) the normal coupling between kinematic characteristics (head velocity vs range of motion) observed in control subjects is absent in patients (Figure 3), and (3) kinematic measures, most notably cycle duration, are predictive of clinical measures (Figure 5). Importantly, the head velocities and frequencies achieved by patients and controls during both transient and continuous exercises were consistent with head velocities experienced in natural environments.2,24,26
Our analysis of continuous gaze stability exercises found that cycle duration and mean magnitude of movement range of the patients’ heads were the kinematic standout variables that differed from healthy controls both before and after the surgery. In contrast, the same kinematic patterns were not distinguishable between patients and healthy controls during transient gaze stability exercises. One possible explanation for this discrepancy might be the difference in our familiarity with these two general classes of head motion. In daily life, transient head movements are commonly made–consider responding to someone calling your name while navigating a busy city sidewalk–and in particular are more frequent than continuous head movements (eg, 2 ). Such motor familiarity is coupled to the construction of well-established internal models that are strengthened by the correspondence between sensory feedback and the specific kinematics of voluntary head movements.28,29
In conditions where compensation or learning is required, as was the case for our patients, the reweighting/realignment of extra-vestibular sensory input (eg, proprioception vs vestibular signals) is driven by a mismatch between estimates of motor state across sensory modalities to recalibrate sensory predictions of movement (reviewed in Refs. 28-31). Single unit recording studies in monkeys have revealed the neural correlate for this strengthening of input of such extra-vestibular contributions.32,33 Specifically, when vestibular information becomes less reliable following peripheral vestibular loss, more reliable proprioception and motor efference copy signals are rapidly up-weighting at the level of the single neurons that constitute the first central stage of vestibular processing (reviewed in Ref. 34). Notably, the up-weighting of motor efference signals has been shown to afford an improvement in vestibular function for actively generated vs passively applied head rotations following vestibular loss.12,15,35
In the present study, we suggest that transient head motion can be considered as a more feedforward ballistic/automated head rotation, as compared to continuous head motion, which requires the ongoing monitoring of head motion feedback in order to ensure accuracy. 36 Transient head motion therefore seems to offer less of a motor control challenge for attempting to stabilize gaze than a continuous head motion in patients where vestibular feedback is less reliable. Indeed, a recent experiment has shown that, following peripheral vestibular loss, changes in the reliability of the sensory input to central pathways impact the statistical structure of head motion of patients during voluntary “everyday” behaviors as compared to control subjects. 26 Specifically, patients demonstrated an increase in head-torso movement variability during tasks that required rapid online vestibular feedback. Here, this finding suggests that impaired vestibular feedback during continuous gaze stabilization exercises was not completely compensated by up-weighting of proprioception and motor efference copy signals in our patients.
Furthermore, it is noteworthy that humans implement different motor strategies when performing transient (ballistic, impulsive) vs continuous motor actions.36,37 As noted above, in the first case, we suggest that movements are driven by pre-programmed strategies, while in the second case, movements are believed to be heavily influenced by feedback modulation. Indeed, there is evidence that the neural control of tasks requiring continuous feedback differs from that required for ballistic tasks. For example, performance of a repetitive ballistic finger task is disrupted by rTMS applied to the finger region of motor cortex. 38 Nevertheless, this same study demonstrated that the performance of a finger task that required feedback to learn an external force field was unaffected by the same stimulation, suggesting that the focus of the motor memory is more distributed—potentially over several cerebral areas. We speculate that the neural control of continuous head movements generated by subjects during the gaze stabilization exercises in this study was likewise more broadly distributed over different cerebral areas as compared to that of head movements made in transient exercises.
Finally, it is notable that the amplitude of head movements generated by patients and controls in our study covered a large portion of the distribution of natural head motion experienced in daily activities along all three canal orientations.2,3,26 An exception was that during the most dynamic of the activities described by Carriot et al (eg, playing soccer and running in the woods), normal subjects generated even higher significant power over this same frequency range. Furthermore, we found that subjects generated lower amplitude head movements during continuous compared to transient exercises. We suggest that this result is again consistent with the proposal that the neural control of the ballistic transient exercises was more automated (less distributed) than that of the continuous task, which in the latter provided a greater control challenge to motor pathways. In the context of motor control, pausing to realign with the visual target after a transient head motion enables a calibration time to refine the next transient movement.39,40 In contrast, continuous exercises being “nonstop” impose the constraint of an ongoing calibration of successive cycles of head movement, 41 likely translating to a more demanding challenge. In this scenario, reducing head movement velocity and hence increasing cycle duration seem to be the strategy chosen putatively to maintain stable gaze during continuous head motion. Thus, given that subjects likely used different motor strategies to perform continuous and transient gaze stabilization exercises, we argue that it ultimately remains worthwhile to have patients perform both types of movement in an exercise-based vestibular rehabilitation program. Our prior work specified that post-operative VOR gain was not correlated with head motion kinematics in vestibular deafferentation 27 ; an interesting finding given the notable reduction in VOR gains, pre- vs post-surgery, across all 3 ipsilesional semicircular canals (SCCs) (yaw = 55%, posterior = 55%, anterior = 46%) (Supplemental Table 1). It remains possible, however, that the kinematics of head motion described in patients with vestibular deafferentation may not be representative of the head kinematics from other patients that are also prescribed gaze stability exercises as part of a vestibular rehabilitation program (ie, dizziness from non-peripheral vestibular pathology). Further research is warranted to examine the role of symptom intensity and varied pathology on head kinematics during vestibular rehabilitation.
Conclusions
The current study suggests that kinematic measurements can distinguish abnormal head movement patterns during continuous gaze stabilization exercises, which emphasizes the clinical value of tracking and assessing head movement in individuals undergoing vestibular rehabilitation. Furthermore, our results indicate that motor performance in continuous gaze stabilization exercises may have relevance beyond their role in patient training, potentially serving as a unique measure of progress that may guide clinicians to refine and provide a more personalized rehabilitation protocol.
Supplemental Material
sj-pdf-1-nnr-10.1177_15459683211034758 – Supplemental Material for Continuous Head Motion is a Greater Motor Control Challenge than Transient Head Motion in Patients with Loss of Vestibular Function
Supplemental Material, sj-pdf-1-nnr-10.1177_15459683211034758 for Continuous Head Motion is a Greater Motor Control Challenge than Transient Head Motion in Patients with Loss of Vestibular Function by Lin Wang, Omid A. Zobeiri, Jennifer L. Millar, Wagner Souza Silva, Michael C. Schubert and Kathleen E. Cullen in Neurorehabilitation and Neural Repair
Supplemental Material
sj-pdf-2-nnr-10.1177_15459683211034758 – Supplemental Material for Continuous Head Motion is a Greater Motor Control Challenge than Transient Head Motion in Patients with Loss of Vestibular Function
Supplemental Material, sj-pdf-2-nnr-10.1177_15459683211034758 for Continuous Head Motion is a Greater Motor Control Challenge than Transient Head Motion in Patients with Loss of Vestibular Function by Lin Wang, Omid A. Zobeiri, Jennifer L. Millar, Wagner Souza Silva, Michael C. Schubert and Kathleen E. Cullen in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgments
We thank the Rubenstein Foundation for their financial support and John Carey, MD for helpful discussions in the early phases of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by a Rubenstein Foundation grant (MCS and KEC), R01-DC002390, R01-DC018061, and 1UF1NS111695-01 from the National Institutes of Health (KEC) and W81XWH-15-1-0442 and W8lXWH-l7-CTRR-CTA from the Department of Defense (MCS).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.