
Abstract
Background
Individuals poststroke experience gait asymmetries that result in decreased community ambulation and a lower quality of life. A variety of studies have utilized split-belt treadmill training to investigate its effect on gait asymmetry, but many employ various methodologies that report differing results.
Objective
The purpose of this meta-analysis was to determine the effects of split-belt treadmill walking on step length symmetry in individuals poststroke both during and following training.
Methods
A comprehensive search of PubMed/MEDLINE, CINAHL, Web of Science, and Scopus was conducted to find peer-reviewed journal articles that included individuals poststroke that participated in a split-belt treadmill walking intervention. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) was used to assess risk of bias. Pooled Hedge’s g with random effects models were used to estimate the effect of split-belt training on step length symmetry.
Results
Twenty-one studies were assessed and included in the systematic review with 11 of them included in the meta-analysis. Included studies had an average STROBE score of 16.2 ± 2.5. The pooled effects for step length asymmetry from baseline to late adaptation were not significant (g = 0.060, P = .701). Large, significant effects were found at posttraining after a single session (g = 1.04, P < .01), posttraining after multiple sessions (g = −0.70, P = .01), and follow-up (g = −0.718, P = .023).
Conclusion
Results indicate split-belt treadmill training with the shorter step length on the fast belt has the potential to improve step length symmetry in individuals poststroke when long-term training is implemented, but randomized controlled trials are needed to confirm the efficacy of split-belt treadmill training.
Introduction
Stroke is a leading cause of serious long-term disability in the United States 1 with more than 40% of stroke survivors struggling with moderate to severe functional impairments. 2 Moderate impairments manifest as decreased gait speed, poor endurance, and asymmetric gait patterns that result in decreased community ambulation and a lower quality of life.3-5 One current focus of rehabilitation for stroke survivors is to improve their walking function by addressing these impairments, specifically that of gait asymmetry. 6 The improvement of rehabilitation strategies remains at the forefront of clinical research, and for stroke survivors, split-belt treadmill training has the potential to strengthen rehabilitation practices.
A split-belt treadmill has 2, independently controlled belts with each belt oriented for a single leg. During split-belt training, the belts will either move at the same speed (tied-belt) or at different speeds (split-belt) to perturb the walking pattern of the person on the treadmill. Most split-belt training paradigms start with a tied-belt condition, followed by split-belt training, and finish with a final tied-belt condition. The final tied-belt condition is conducted to test how gait asymmetry was affected by the split-belt training. While the overall structure of these training paradigms across studies is similar, how the split-belt training is performed often depends on the objective and focus of the study. The speed of each belt, which limb is placed on each belt, training duration, and other methodological factors lead to variable outcomes across studies investigating split-belt training.7-11
A common objective of split-belt training paradigms for individuals poststroke is to reduce step length asymmetry through the adaptation of gait characteristics to the perturbing locomotor environment.12-14 This is typically done by placing the limb with the shorter step length on the fast belt.11,15,16 This limb placement strategy augments the asymmetry already present in the participant’s gait. Since the person’s natural asymmetry is augmented by the different belt speeds, the participant starts to adapt their gait pattern to try and reduce the asymmetry caused by the treadmill. Adaptation to the split-belt is often a result of the participant increasing their step length on the fast belt in an attempt to arrive back at an asymmetrical pattern similar to baseline walking. 11 This locomotor adaptation to split-belt training has been shown to produce after-effects that result in reduced step length asymmetry following training.12,13 Depending on the study objective, the effects of the training could be acute and diminish quickly after training, 14 or it could potentially lead to a longer lasting effect. 11
While the majority of split-belt training paradigms aim to reduce asymmetry, there are other reasons to implement split-belt training and these reasons can lead to different benefits. For example, some studies place the paretic limb on the slow belt regardless of step length.8,17,18 Other studies focus on comparing participants’ biomechanical characteristics, such as baseline asymmetry or muscle strength, to how an individual is able to adapt to the protocol.8,17 Because not all studies utilizing a split-belt training paradigm aim to reduce gait asymmetry posttraining, it is important to consider study objectives when evaluating results and determining which protocol is best for improving step length symmetry.
As demonstrated above, there are large differences in training methodologies and reported outcome measures that make it difficult to identify the most beneficial protocol for rehabilitation. Therefore, the purpose of this systematic review with meta-analysis was to perform an evaluation of methods and results of existing studies that investigated the effects of split-belt treadmill training on step length asymmetry in individuals poststroke. Assessment of step length asymmetry was chosen due to reports of step length being more responsive to split-belt training than other spatiotemporal measures. 11 Specifically, we asked if individuals poststroke demonstrate improvements in step length symmetry following split-belt treadmill training regardless of the split-belt paradigm and study methodology.
Methods
This systematic review was unregistered but was carried out following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 19
Data Acquisition
An electronic database search was conducted by 4 of the coauthors (EAH, LER, TJL, and ACD) on the National Library of Medicine Catalog (MEDLINE/PubMed), the Cumulative Index for Nursing and Allied Health Literature (CINAHL), Web of Science, and Scopus from inception to June 12, 2020. Each coauthor searched one database. The initial key terms search consisted of “stroke” OR “hemipar*” OR “cerebrovascular” OR “hemipleg*” OR “cva” OR “brain attack” OR “pare*” AND “split belt” OR “splitbelt” OR “split-belt” OR “dualbelt” OR “dual-belt” OR “dual belt” AND “symmetr*” OR “asymmetr*” OR “adapt*” OR “learn*”. Additional key terms for English language and publication type were added for the Scopus database search. These key terms provided relevant literature to the research question and were agreed upon by the coauthors prior to completing the search.
Inclusion and Exclusion Criteria
All articles included in the systematic review and meta-analysis met the following inclusion criteria: (1) written in the English language; (2) research participants were adults (≥18 years old) suffering from chronic stroke (≥6 months following) 20 ; (3) inclusion of split-belt treadmill walking intervention; (4) measured step length symmetry at multiple time points; (5) step length symmetry as an outcome measure; (6) were published in a peer-reviewed journal. Research articles were excluded if the article did not report participants’ time since stroke.
Study Selection
Duplicates across databases were removed after the initial search was performed (Figure 1). After duplicates were removed, 2 of the coauthors (LER and ACD) independently inspected article titles and abstracts for inclusion and exclusion criteria. After relevant articles were identified, 2 of the other coauthors (EAH and TJL) reevaluated the full text of articles for inclusion and exclusion criteria. Full text was also screened by these coauthors to identify articles with duplicate data. A consensus of the final articles to be included was met by all coauthors.
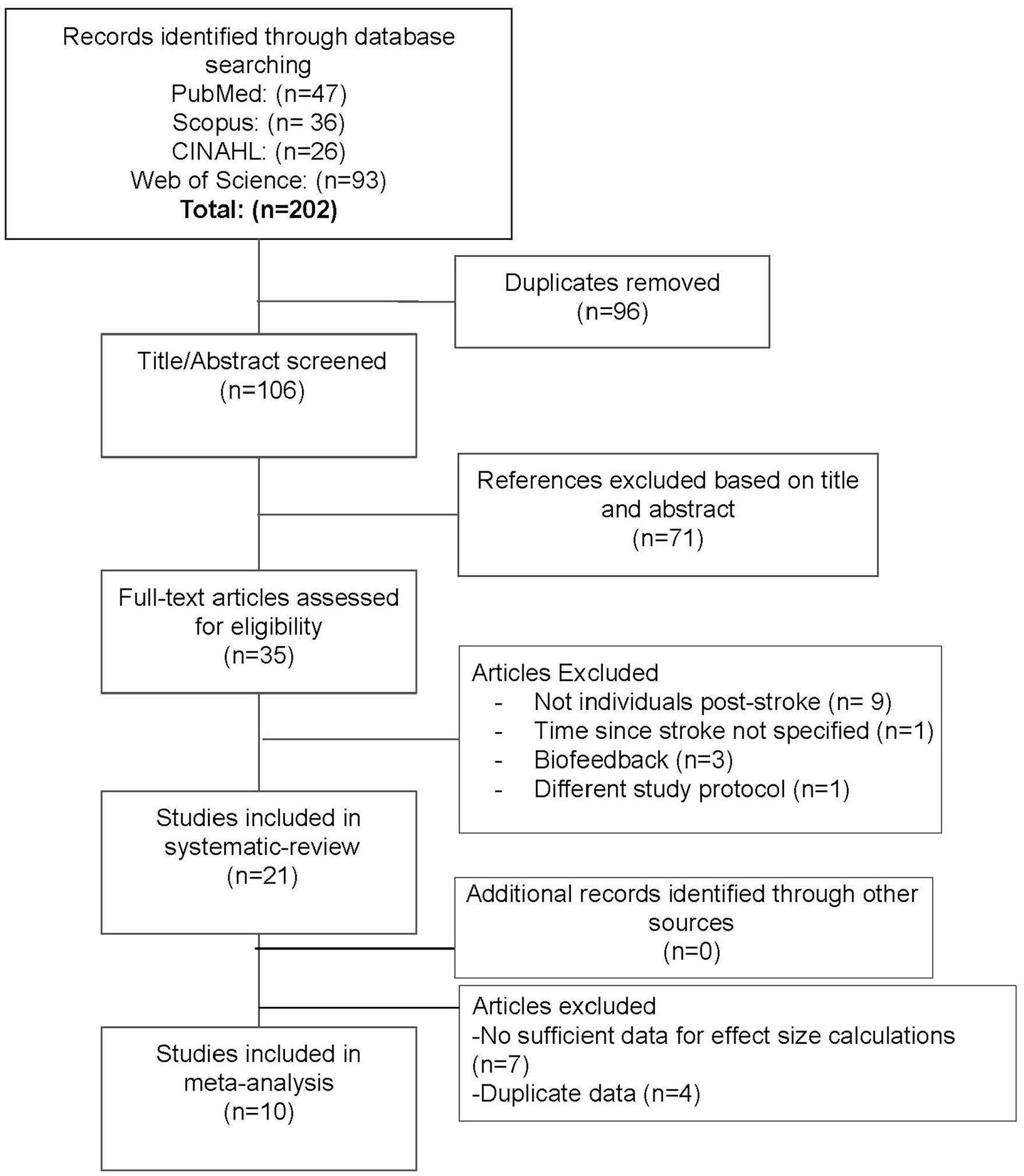
Search flow diagram. Flow chart of articles included in the systematic review and meta-analysis.
Assessment of Study Quality
All final articles were assessed using the checklist put forth by the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 21 Each article was independently assessed by 2 reviewers against the 22 criteria put forth in the STROBE statement to evaluate the reporting quality of each study (Supplementary Table 1). Studies were organized by alphabetical order according to the first author’s last name and date of publication. Two reviewers (TJL, EAH) assessed the first half of the studies, and 2 reviewers (LER, ACD) assessed the second half. Disagreements in STROBE scores were discussed and resolved between the 2 reviewers.
Data Extraction and Analysis
Information regarding the number of participants, intervention summary, and outcome measures were extracted as available from the studies evaluated for risk of bias (Table 1). Further information regarding the participant population including the age of participants, time since stroke, each participant’s paretic side, as well as additional information regarding the split-belt treadmill intervention were extracted (Supplementary Tables 2 and 3).
Summary of Extracted Data From Each Study a .
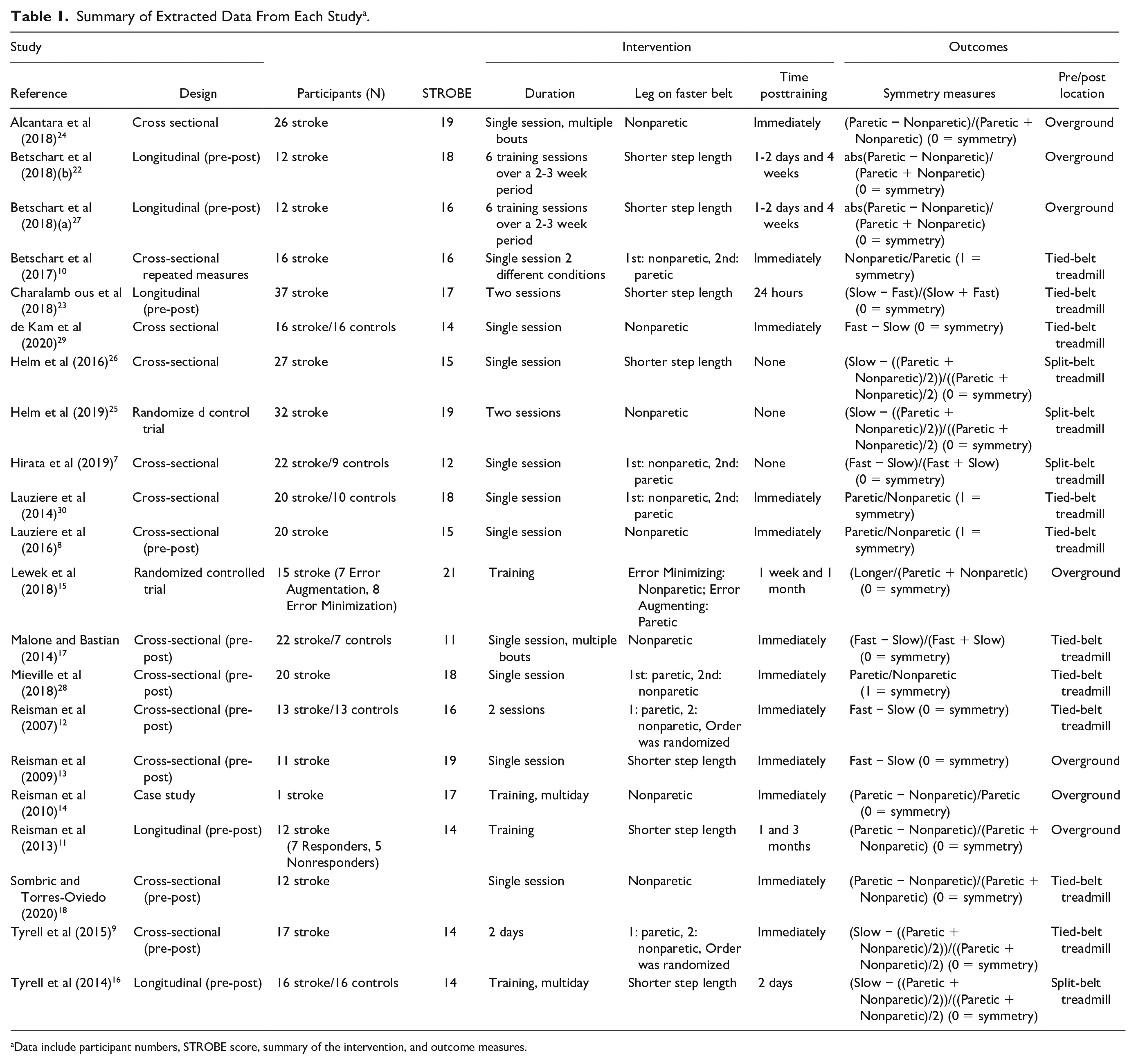
Data include participant numbers, STROBE score, summary of the intervention, and outcome measures.
Means and standard deviations of step length symmetry indexes were extracted for effect size calculations. All symmetry ratios were converted to standardized mean differences (Hedge’s g). Data from 4 studies8,10,15,22 were obtained from the original research articles, whereas data from 6 studies7,9,11,16-18 were obtained from the authors through electronic correspondence. Data from 7 studies12-14,23-26 were not obtained after reaching out to the corresponding authors. Four articles presented duplicate datasets to other included articles and, therefore, were excluded from the meta-analysis.27-30 Individual and pooled Hedge’s g effect sizes were calculated using RStudio (Package: meta, RStudio Inc). A random effects model was chosen due to the distribution of the included studies’ methods. Four different time points during split-belt training were analyzed including late adaptation, posttraining after a single session, posttraining after multiple sessions, and follow-up. Therefore, 4 separate pooled effect sizes were calculated to evaluate the effects of split-belt training on step length symmetry. Leg placement strategies differed between posttraining after a single session and after multiple sessions. The effect size calculated from baseline to posttraining after a single session exclusively contained studies that placed the paretic leg on the slow belt. Conversely, the effect size calculated from baseline to posttraining after multiple sessions exclusively contained studies that placed the leg with the shorter step length on the fast belt. Effect sizes were interpreted as very small (0-0.19), small (0.20-0.49), medium (0.50-0.79), and large (>0.80). 31 Heterogeneity among individual effects was assessed using the I2 statistic and publication bias was assessed using the Fail-Safe N. Statistical significance was evaluated at α ≤ .05.
Results
Article Screening
Upon initial article screening, 202 articles were identified using initial search terms, with 106 remaining after duplicates were removed (Figure 1). Seventy-one articles were then removed based on title and abstract, leaving 35 full-text articles to be screened for eligibility. After the assessment of full text, 9 articles were removed for not including individuals poststroke,32-40 3 were removed for including biofeedback in their protocol,41-43 1 study did not investigate the effects of split-belt training on step length asymmetry as a postintervention, 44 and 1 study did not report how long it had been since their subjects had suffered a stroke. 45 The reference list of each journal article was reviewed in an attempt to find any additional studies not found in our initial search. No additional studies were identified. Finally, 21 articles are included in this systematic review, 5 are longitudinal studies,11,16,22,23,27 12 cross sectional,7-9,12,13,17,18,24,26,28-30 1 cross sectional with a crossover design, 10 2 randomized controlled trials,15,25 and 1 case study. 14 The average STROBE score was a 16.2 ± 2.5 out of a possible 22 (Supplementary Table 1). The objective of each study is listed in Supplementary Table 4.
Participants
Among the 21 studies that were reviewed, the number of participants in each study ranged from n = 1113 to n = 37, 23 in addition to one case study of n = 114 (Table 1). When combining all of the studies, 450 participants were recorded with 379 of them being stroke survivors and 71 being healthy participants.
Intervention
All of the studies had a split-belt training paradigm. Every training paradigm started with a tied-belt condition, followed by a split-belt training paradigm, and ended with either a tied-belt or overground walking session to evaluate after effects. The split-belt training paradigm varied across studies (Table 1, Supplementary Table 3). There were 11 studies that conducted a single split-belt session7,8,10,13,17,18,24,26,28-30 and 10 studies that performed a multiple training sessions,9,11,12,14,15,22,23,25,27 which ranged from 2 sessions9,12,23,25 to 18 sessions. 15 Each split-belt walking period ranged from 5 minutes11,14,17 to 20 minutes.15,22,27
Belt Speeds
Twenty of the studies used a 2:1 ratio for speed differences between the 2 belts during the split-belt paradigm. Out of these 20 studies, 9 calculated the fast belt speed as the fastest comfortable walking speed and the slow belt speed as half of that speed,7,9,11,13,16,23-26 6 calculated the slow belt speed as the participant’s self-selected speed and the fast belt as twice the self-selected speed,8,10,22,27,28,30 3 studies had the fast belt move at 1.0 m/s and the slow belt move at 0.5 m/s,12,14,17 and 2 studies calculated each participant’s self-selected speed and the fast belt was 133% of that speed and the slow belt was 66% of that speed.18,29 One study 25 had a group complete the training at 3 different speed ratios, 1.5:1, 2:1, and 2.5:1. Last, one study controlled the ratio of the belt speeds based on the degree of the patient’s asymmetry and it changed on a step-by-step basis. 15
Limb Placement Strategies
Seven of the studies placed the shorter step length on the fast belt regardless of which was the paretic side.11,13,16,22,23,26,27 Fourteen studies determined limb placement based on the participant’s paretic and nonparetic side. Seven of these studies had individuals walk only with their nonparetic side on the fast belt and their paretic side on the slow belt.8,14,17,24,25,29,38 The other 7 studies utilized a repeated measures design where participants walked in 2 conditions, one with their nonparetic side on the fast belt and another with their paretic side on the fast belt.7,9,10,12,15,28,30 Limb placement strategy can vary depending on the objective of the study. 12
Meta-Analysis Data
Seven of the 21 studies12-14,23-26 did not include sufficient data for effect size calculations. Four of the 21 studies27-30 had duplicate datasets and were excluded from the meta-analysis portion of the study. Individual effect sizes were calculated from 10 of the 21 studies. Six individual effect sizes from 5 studies7,9,10,16,18 were used to calculate the pooled effect of baseline to late adaptation, with four7,9,10,18 individual effect sizes being from studies that placed the paretic leg on the slow belt and two9,16 individual effect sizes being from studies that placed the shorter step length on the fast belt. These studies were combined into one analysis and the heterogeneity statistic (I2) for this analysis was very low, indicating minimal variation between study outcomes (I2 = 0%, P = .50, Figure 2). Four individual effect sizes8,10,17,18 were used to calculate the pooled effect of baseline to posttraining after a single session. Five individual effect sizes from 3 studies11,15,22 were used to calculate the pooled effect of baseline to posttraining after multiple training sessions, and 5 individual effect sizes from 3 studies11,15,22 were used to calculate the pooled effect of baseline to follow-up. All studies performing multiple training sessions placed the shorter step length on the faster belt. The pooled effects for step length asymmetry from baseline to late adaptation were not significant (g = 0.060, P = .701; Figure 2), while the pooled effects for step length asymmetry from baseline to posttraining after a single session (g = 1.04, P < .01), baseline to posttraining after multiple sessions (g = −0.70, P = .01), and baseline to follow-up (g = −0.718, P = .023) were significant (Figures 3-5). The Fail-Safe N values for the pooled effect of baseline to posttraining after a single session, posttraining after multiple sessions, and follow-up were 12.45, 12.50, and 10.64, respectively. Funnel plots for baseline to late adaptation, posttraining after a single session, posttraining after multiple sessions, and follow-up are located in Supplementary Figures 1 to 4.
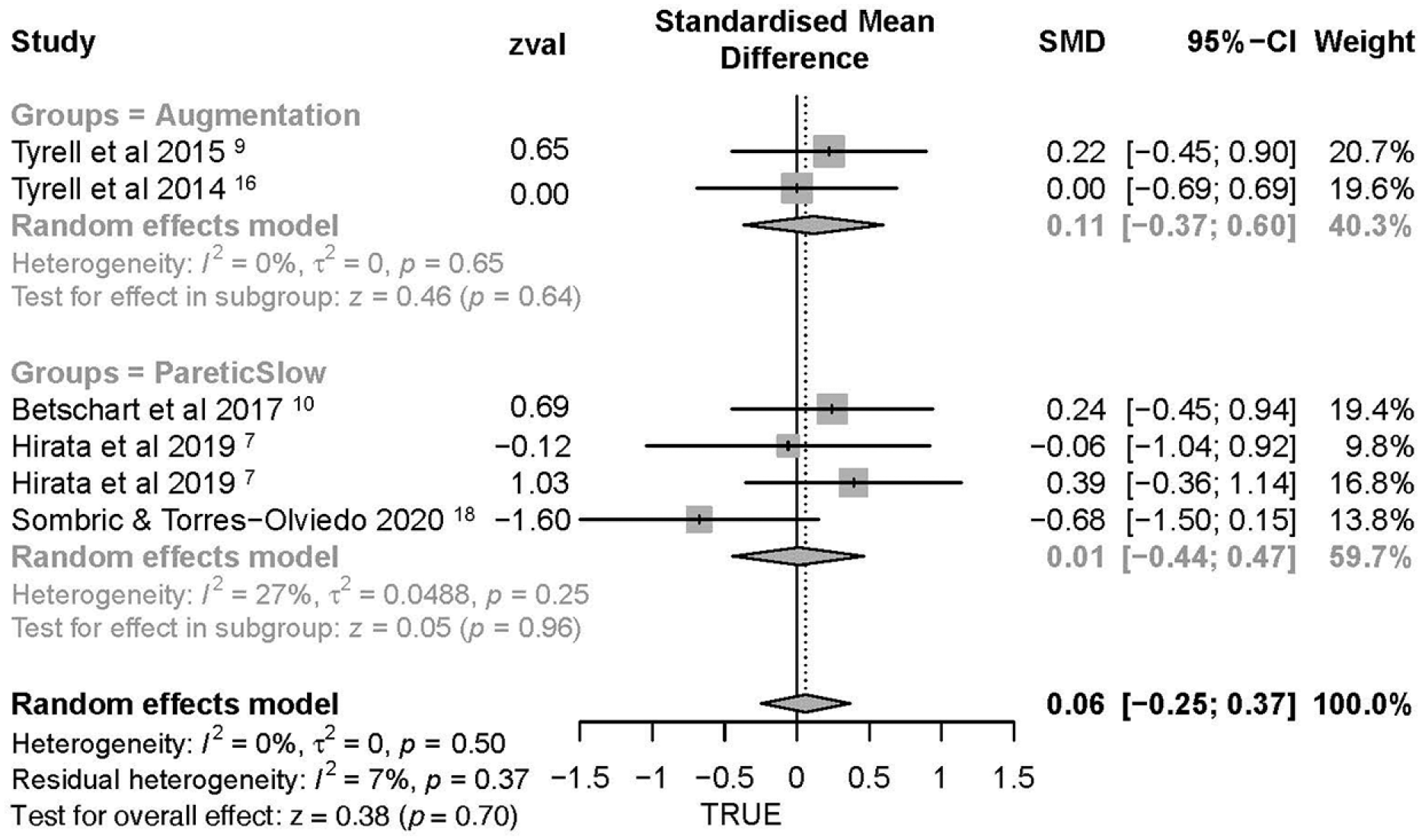
Symmetry during late adaptation. Forest plot of individual effect sizes (Hedge’s g) and their associated 95% confidence intervals for studies that assessed step length symmetry during the late adaptation phase of split-belt treadmill walking. Effect sizes to the left of zero indicate an increase in step length symmetry from baseline to late adaptation (square = individual effect size, diamond = pooled effect size). The augmentation grouping includes studies that utilized an error augmentation split-belt paradigm. The paretic slow grouping includes studies that placed the paretic limb on the slow belt.
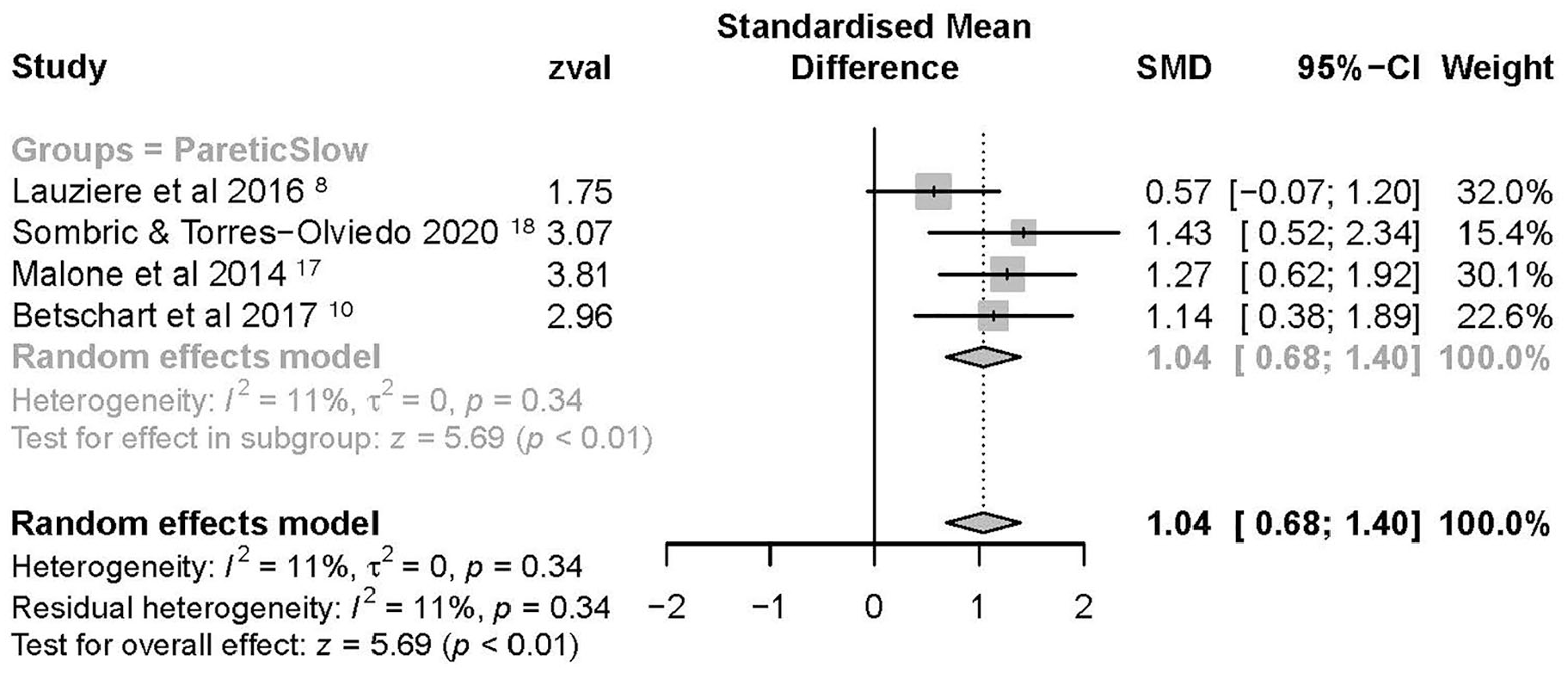
Symmetry during posttraining after a single session. Forest plot of individual effect sizes (Hedge’s g) and their associated 95% confidence intervals for studies that assessed step length symmetry during the posttraining assessment after a single training session. Effect sizes to the left of zero indicate an increase in step length symmetry from baseline to posttraining after a single session (square = individual effect size, diamond = pooled effect size). The paretic slow grouping includes studies that placed the paretic limb on the slow belt.
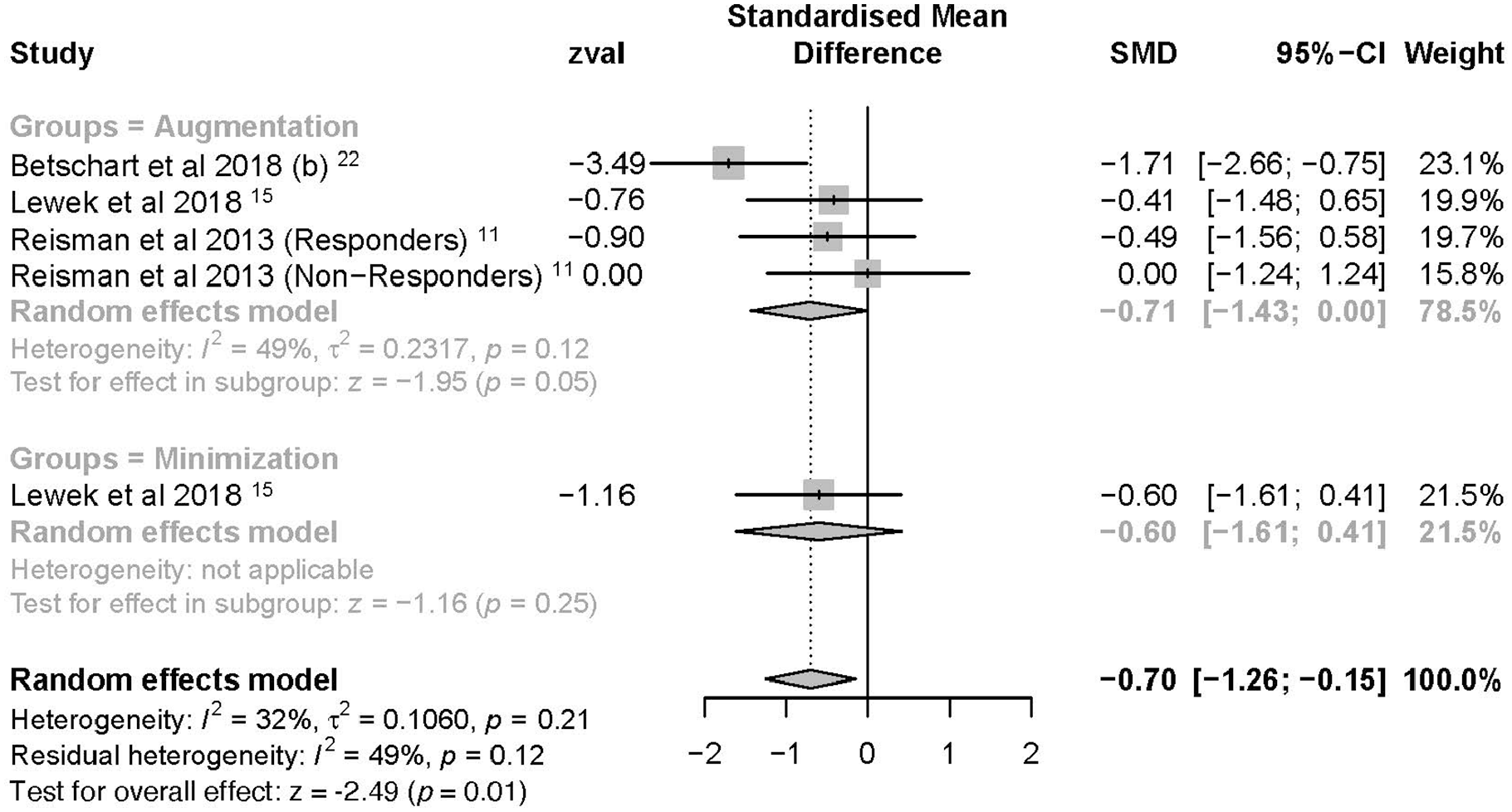
Symmetry during posttraining after multiple training sessions. Forest plot of individual effect sizes (Hedge’s g) and their associated 95% confidence intervals for studies that assessed step length symmetry during the posttraining assessment after multiple training sessions on the split-belt treadmill. Effect sizes to the left of zero indicate an increase in step length symmetry from baseline to posttraining after multiple sessions (square = individual effect size, diamond= pooled effect size). The augmentation grouping includes studies that utilized error augmentation split-belt paradigm. The minimization grouping includes studies that utilized an error minimization split-belt paradigm.
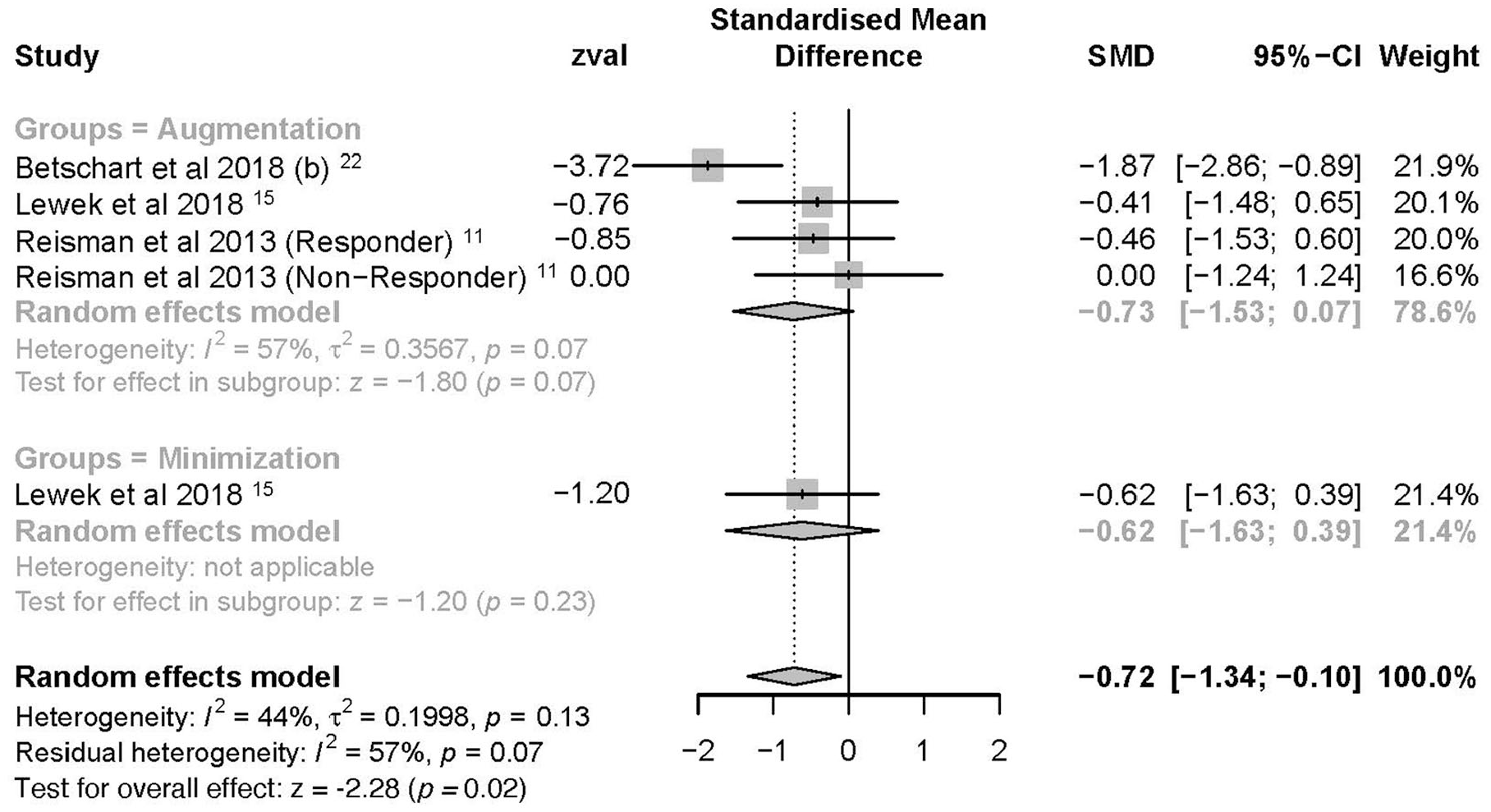
Symmetry during follow-up. Forest plot of individual effect sizes (Hedge’s g) and their associated 95% confidence intervals for studies that assessed step length symmetry during the follow-up assessment multiple weeks after the last training session. Effect sizes to the left of zero indicate an increase in step length symmetry from baseline to follow-up (square = individual effect size, diamond = pooled effect size). The augmentation grouping includes studies that utilized error augmentation split-belt paradigm. The minimization grouping includes studies that utilized an error minimization split-belt paradigm.
Discussion
The purpose of this systematic review with meta-analysis was to investigate the effects of split-belt treadmill training on step length asymmetry in individuals poststroke. Our results demonstrate that individuals poststroke experienced a significant improvement in step length symmetry after partaking in a split-belt training paradigm. However, no significant effects of split-belt training were found from baseline to late adaptation.
Late Adaptation
The lack of significant differences between baseline and late adaptation indicate that individuals poststroke overcame the error induced by the treadmill and returned to their baseline walking pattern while walking on the treadmill.7,9,10,16,18 Several studies suggest that the treadmill protocol has little impact on the participants’ ability to adapt back to baseline walking during treadmill training.10,17,30 Contradictory to these claims, Tyrell and colleagues reported that participants returned to baseline asymmetry during an error augmentation protocol but failed to do so when the split-belt minimized the error in the participants’ gait. 16 During the error minimization protocol, the participants did not adapt back to baseline but maintained an improved step length symmetry on the split-belt.
Hirata et al (2019) suggested that some participants may be more likely to return to their baseline gait asymmetry during late adaptation compared to others. To identify participants that were more likely to adapt to training, Hirata et al (2019) analyzed an angle between the center of mass and the center of pressure. Their results indicated that the participants whose center-of-mass to center-of-pressure angle were more symmetric were also better able to adapt to the split-belt treadmill and return to their baseline asymmetry. 7 However, a more symmetric center-of-mass to center-of-pressure angle may also be indicative of greater walking ability, and therefore, these results should be interpreted cautiously.
Posttraining
Step length symmetry was altered between posttraining and baseline walking in both cross sectional and longitudinal study designs. In cross-sectional studies, individuals reported significantly greater asymmetry posttraining whereas the longitudinal studies reported significant improvements in gait symmetry.
The worsening of step length symmetry at posttraining immediately following the split-belt paradigm was most likely due to differences in the methodology and/or research objectives of the studies that were analyzed with a cross-sectional design8,17,18 compared to the studies with a longitudinal design.11,15,22 The cross-sectional studies had objectives that were not necessarily aimed at improving step length symmetry following split-belt treadmill walking and utilized training methodologies that were not intended to reduce asymmetry. The protocols used in the 4 studies with a cross-sectional design only consisted of one study visit whereas the protocols of Betschart et al (2018), Lewek et al (2018), and Reisman et al (2013) all consisted of at least 6 split-belt training sessions over multiple weeks before the posttraining assessment.11,15,22 Additionally, Betschart et al (2018), Lewek et al (2018), and Reisman et al (2013) required subjects to have an asymmetric gait pattern at baseline as inclusion criteria whereas the studies with a cross sectional design did not. Due to this discrepancy in inclusion criteria, Malone et al (2014) 17 and Sombric and Torres Oviedo (2020) 18 reported the 2 smallest baseline asymmetry measures, and Lauziere et al (2016) reported that 8 of 20 participants had minimal baseline asymmetry. Step length symmetry that became worse after split-belt training has also been observed in studies with healthy controls who do not have a step length asymmetry during baseline walking. 46 Moreover, when Lauziere et al (2016) analyzed the 12 individuals that presented step length asymmetries at baseline, they found a significant reduction in step length asymmetry from baseline to posttraining.
Another factor that may have contributed to the worsening of gait symmetry following training in Lauziere et al (2016), 8 Malone et al (2014), 17 and Sombric and Torres Oviedo (2020) 18 is the method for evaluating posttraining symmetry. All 3 of these studies performed posttraining assessments during tied-belt treadmill walking8,17,18 in contrast to the other studies which performed posttraining assessments during overground walking.11,15,22 Previous work has shown that individuals poststroke demonstrate a shorter step length on their paretic side during treadmill walking compared to walking overground. 47 This offers further explanation for the asymmetry present in the subjects of Lauziere et al (2016), 8 Malone et al (2014), 17 and Sombric and Torres Oviedo (2020) 18 during the post-training assessment. It should be noted that one other study within this review not included in the meta-analysis also assessed posttraining step length symmetry during tied-belt treadmill walking and reported improvements in step length symmetry. 12 However, this improvement was only observed when the studies employed an error augmentation protocol.
Another methodological discrepancy between Lauziere et al (2016), 8 Malone et al (2014), 17 and Sombric and Torres Oviedo (2020) 18 and the other studies in the posttraining analysis is how limb placement was determined on the split-belt treadmill. Lauziere et al (2016), 8 Malone et al (2014), 17 and Sombric and Torres Oviedo (2020) 18 chose to place the paretic limb on the slow belt regardless of which side had the shorter step length. The other 3 studies chose to have at least one of their study groups perform an error augmentation protocol by placing the limb with the shortest step length on the fast belt.11,15,22 The studies included in our systematic review support the notion that error augmentation strategies, rather than error minimization strategies, may be best for reducing asymmetry following split-belt treadmill training.11,13-15,27 As further support, 3 studies that utilized an error minimization strategy demonstrated the intervention had a detrimental effect on the participant’s step length symmetry posttraining.8,12,17 On the other hand, Lewek et al (2018) reported no differences between the error augmentation and error minimization groups for improvements in step length symmetry posttraining. However, this result is likely due to verbal feedback regarding the subject’s walking symmetry that was provided from a therapist during the walking trials. This study reported improvements in step length symmetry for all groups including a control group of individuals poststroke that did not participate in the split-belt paradigm. Previous studies investigating effects of treadmill training on gait poststroke and did not see improvements in step length symmetry in subjects who only received low-intensity treadmill exercise.48,49 Results from those studies indicate that it is likely the verbal feedback received by subjects in Lewek et al (2018) that contributed to the improvements seen in step length symmetry across all intervention groups and results from this study should be interpreted with caution. Several other studies in this meta-analysis utilized an experimental protocol where either the paretic or nonparetic limb was placed on the fast belt of the split-belt treadmill, regardless of which limb had the shorter step length.8,24,28-30 Therefore, we were unable to classify these methodologies as error augmentation or error minimization protocols.
Follow-up
The significant improvement in step length symmetry during the follow-up visit demonstrates that split-belt training can elicit long-term improvements in step length symmetry for individuals poststroke. All studies included in the follow-up analysis had participants perform a longitudinal split-belt training protocol of at least 6 sessions and utilized an error augmentation strategy.11,15,22 Furthermore, Reisman et al (2013) demonstrated a trend in step length symmetry improvements up to 3 months following the completion of the training sessions. 11 One other study not included in the effect size calculations, also reported retained improvement to step length asymmetry 1 month following a split-belt training protocol. 14 These results demonstrate that when an error augmentation protocol is combined with multiple split-belt training sessions, significant improvements in step length symmetry can be achieved and persist after the cessation of training.
Limitations
A number of limitations need to be acknowledged in this systematic review with meta-analysis. Most notably, the number of studies analyzed in this systematic review with meta-analysis was small, and of the included studies, the sample sizes were relatively low. Additionally, publication bias may have been present as the Fail-Safe N was relatively low. The average STROBE score among studies was a 16.2 ± 2.50. The STROBE has a maximum score of 22, which puts our systematic review’s average STROBE percentage score at 74 ± 11%. Common pitfalls among studies’ STROBE were failing to report how the sample size was arrived at and how the authors addressed potential sources of bias. Other pitfalls were failing to clarify study design in the title or abstract and failing to report limitations.
Another limitation with the studies’ STROBE scoring was that studies were divided among authors. Two authors performed a risk of bias assessment for the first half of studies where the other 2 authors evaluated the second half. Although each author received the same training in how to perform risk of bias assessments, there is a possibility that the 2 groups of authors had different perspectives on study quality and STROBE scoring criteria that could have skewed results. Additionally, due to the small number of studies, investigating the effects of methodology such as time from training to posttraining assessment, speed of the belts during training, and total training time was not considered to be statistically appropriate and thus, was not investigated in the current study.
Future Studies Recommendations
Based on the results of this systematic review with meta-analysis, randomized controlled trials are needed to determine the true efficacy of split-belt treadmill training on gait symmetry in individuals poststroke. If randomized controlled trials find split-belt treadmill training improves step length symmetry in this population as alluded to in this meta-analysis, future research should then focus on establishing minimal detectable change and clinically important difference values for the symmetry metrics utilized by these studies. Additionally, further studies comparing the different split-belt treadmill paradigms to normal tied-belt treadmill paradigms could further demonstrate the benefit of split-belt treadmill trainings. Further investigation into the effect of verbal feedback during walking should also be explored as demonstrated by the results of Lewek et al (2018). 15
Conclusion
The results of this meta-analysis demonstrate that a longitudinal error augmentation split-belt training paradigm, compared to other methodologies including error minimization, has the potential to be an effective clinical intervention for improving step length symmetry in individuals poststroke, but randomized controlled trials are needed to confirm the efficacy of this training paradigm. Additionally, given the limited number of studies available for analysis, these results should be interpreted with caution. Last, because of the variability in the amount of training between longitudinal studies, future experiments should focus on identifying an optimal amount of time necessary for clinically meaningful adaptations to occur.
Supplemental Material
sj-docx-1-nnr-10.1177_15459683211011226 – Supplemental material for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis
Supplemental material, sj-docx-1-nnr-10.1177_15459683211011226 for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis by Alex C. Dzewaltowski, Erica A. Hedrick, Todd J. Leutzinger, Lindsey E. Remski and Adam B. Rosen in Neurorehabilitation and Neural Repair
Supplemental Material
sj-jpg-1-nnr-10.1177_15459683211011226 – Supplemental material for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis
Supplemental material, sj-jpg-1-nnr-10.1177_15459683211011226 for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis by Alex C. Dzewaltowski, Erica A. Hedrick, Todd J. Leutzinger, Lindsey E. Remski and Adam B. Rosen in Neurorehabilitation and Neural Repair
Supplemental Material
sj-jpg-10-nnr-10.1177_15459683211011226 – Supplemental material for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis
Supplemental material, sj-jpg-10-nnr-10.1177_15459683211011226 for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis by Alex C. Dzewaltowski, Erica A. Hedrick, Todd J. Leutzinger, Lindsey E. Remski and Adam B. Rosen in Neurorehabilitation and Neural Repair
Supplemental Material
sj-jpg-11-nnr-10.1177_15459683211011226 – Supplemental material for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis
Supplemental material, sj-jpg-11-nnr-10.1177_15459683211011226 for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis by Alex C. Dzewaltowski, Erica A. Hedrick, Todd J. Leutzinger, Lindsey E. Remski and Adam B. Rosen in Neurorehabilitation and Neural Repair
Supplemental Material
sj-jpg-12-nnr-10.1177_15459683211011226 – Supplemental material for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis
Supplemental material, sj-jpg-12-nnr-10.1177_15459683211011226 for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis by Alex C. Dzewaltowski, Erica A. Hedrick, Todd J. Leutzinger, Lindsey E. Remski and Adam B. Rosen in Neurorehabilitation and Neural Repair
Supplemental Material
sj-jpg-13-nnr-10.1177_15459683211011226 – Supplemental material for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis
Supplemental material, sj-jpg-13-nnr-10.1177_15459683211011226 for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis by Alex C. Dzewaltowski, Erica A. Hedrick, Todd J. Leutzinger, Lindsey E. Remski and Adam B. Rosen in Neurorehabilitation and Neural Repair
Supplemental Material
sj-jpg-14-nnr-10.1177_15459683211011226 – Supplemental material for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis
Supplemental material, sj-jpg-14-nnr-10.1177_15459683211011226 for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis by Alex C. Dzewaltowski, Erica A. Hedrick, Todd J. Leutzinger, Lindsey E. Remski and Adam B. Rosen in Neurorehabilitation and Neural Repair
Supplemental Material
sj-jpg-15-nnr-10.1177_15459683211011226 – Supplemental material for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis
Supplemental material, sj-jpg-15-nnr-10.1177_15459683211011226 for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis by Alex C. Dzewaltowski, Erica A. Hedrick, Todd J. Leutzinger, Lindsey E. Remski and Adam B. Rosen in Neurorehabilitation and Neural Repair
Supplemental Material
sj-jpg-2-nnr-10.1177_15459683211011226 – Supplemental material for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis
Supplemental material, sj-jpg-2-nnr-10.1177_15459683211011226 for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis by Alex C. Dzewaltowski, Erica A. Hedrick, Todd J. Leutzinger, Lindsey E. Remski and Adam B. Rosen in Neurorehabilitation and Neural Repair
Supplemental Material
sj-jpg-3-nnr-10.1177_15459683211011226 – Supplemental material for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis
Supplemental material, sj-jpg-3-nnr-10.1177_15459683211011226 for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis by Alex C. Dzewaltowski, Erica A. Hedrick, Todd J. Leutzinger, Lindsey E. Remski and Adam B. Rosen in Neurorehabilitation and Neural Repair
Supplemental Material
sj-jpg-4-nnr-10.1177_15459683211011226 – Supplemental material for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis
Supplemental material, sj-jpg-4-nnr-10.1177_15459683211011226 for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis by Alex C. Dzewaltowski, Erica A. Hedrick, Todd J. Leutzinger, Lindsey E. Remski and Adam B. Rosen in Neurorehabilitation and Neural Repair
Supplemental Material
sj-jpg-5-nnr-10.1177_15459683211011226 – Supplemental material for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis
Supplemental material, sj-jpg-5-nnr-10.1177_15459683211011226 for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis by Alex C. Dzewaltowski, Erica A. Hedrick, Todd J. Leutzinger, Lindsey E. Remski and Adam B. Rosen in Neurorehabilitation and Neural Repair
Supplemental Material
sj-jpg-6-nnr-10.1177_15459683211011226 – Supplemental material for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis
Supplemental material, sj-jpg-6-nnr-10.1177_15459683211011226 for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis by Alex C. Dzewaltowski, Erica A. Hedrick, Todd J. Leutzinger, Lindsey E. Remski and Adam B. Rosen in Neurorehabilitation and Neural Repair
Supplemental Material
sj-jpg-7-nnr-10.1177_15459683211011226 – Supplemental material for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis
Supplemental material, sj-jpg-7-nnr-10.1177_15459683211011226 for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis by Alex C. Dzewaltowski, Erica A. Hedrick, Todd J. Leutzinger, Lindsey E. Remski and Adam B. Rosen in Neurorehabilitation and Neural Repair
Supplemental Material
sj-jpg-8-nnr-10.1177_15459683211011226 – Supplemental material for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis
Supplemental material, sj-jpg-8-nnr-10.1177_15459683211011226 for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis by Alex C. Dzewaltowski, Erica A. Hedrick, Todd J. Leutzinger, Lindsey E. Remski and Adam B. Rosen in Neurorehabilitation and Neural Repair
Supplemental Material
sj-jpg-9-nnr-10.1177_15459683211011226 – Supplemental material for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis
Supplemental material, sj-jpg-9-nnr-10.1177_15459683211011226 for The Effect of Split-Belt Treadmill Interventions on Step Length Asymmetry in Individuals Poststroke: A Systematic Review With Meta-Analysis by Alex C. Dzewaltowski, Erica A. Hedrick, Todd J. Leutzinger, Lindsey E. Remski and Adam B. Rosen in Neurorehabilitation and Neural Repair
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.