
Abstract
Background. Previous data suggest that the amount and aerobic intensity of stepping training may improve walking poststroke. Recent animal and human studies suggest that training in challenging and variable contexts can also improve locomotor function. Such practice may elicit substantial stepping errors, although alterations in locomotor strategies to correct these errors could lead to improved walking ability. Objective. This unblinded pilot study was designed to evaluate the feasibility and preliminary efficacy of providing stepping practice in variable, challenging contexts (tasks and environments) at high aerobic intensities in participants >6 months and 1-6 months post-stroke. Methods. A total of 25 participants (gait speeds <0.9 m/s with no more than moderate assistance) participated in ≤40 training sessions (duration of 1 hour) within 10 weeks. Stepping training in variable, challenging contexts was performed at 70% to 80% heart rate reserve, with feasibility measures of total steps/session, ability to achieve targeted intensities, patient tolerance, dropouts, and adverse events. Gait speed, symmetry, and 6-minute walk were measured every 4 to 5 weeks or 20 sessions, with a 3-month follow-up (F/U). Results. In all, 22 participants completed ≥4 training weeks, averaging 2887 ± 780 steps/session over 36 ± 5.8 sessions. Self-selected (0.38 ± 0.27 to 0.66 ± 0.35 m/s) and fastest speed (0.51 ± 0.40 to 0.99 ± 0.58 m/s), paretic single-limb stance (20% ± 5.9% to 25% ± 6.4%), and 6-minute walk (141 ± 99 to 260 ± 146 m) improved significantly at posttraining. Conclusions. This preliminary study suggests that stepping training at high aerobic intensities in variable contexts was tolerated by participants poststroke, with significant locomotor improvements. Future studies should delineate the relative contributions of amount, intensity, and variability of stepping training to maximize outcomes.
Introduction
Many studies have evaluated the efficacy of specific interventions to improve walking ability in individuals with gait impairments poststroke, although the critical training parameters that maximize recovery are not clear. Studies from animal models1,2 and humans with neurological injury 3 suggest that the amount of task-specific stepping practice may be an important parameter. Early studies utilizing treadmill training with therapist assistance to approximate speeds and/or kinematics observed in intact individuals4-7 demonstrated significant walking improvements, which may be related to the amount of stepping practice. Other studies suggest that the aerobic intensity of stepping training, estimated primarily using heart rate (HR), 8 may be another important training parameter to improve walking outcomes.9,10 Surprisingly, however, in some of these3,10 and other studies11-13 providing large amounts of stepping practice at low or high aerobic intensities, gait speed improvements are often not different compared with changes observed following interventions providing limited walking.
One training parameter that has received less attention is the variability of gait kinematics or tasks. Rather, many training protocols focus on consistent, symmetrical, kinematically correct stepping patterns during training4-7,11,14 and minimize kinematic variability and errors. However, animal 15 and human studies16,17 have shown that kinematically constrained treadmill stepping can limit improvements in gait symmetry or joint kinematics, particularly as compared with strategies that allow kinematic variability. Task variability is also limited in many studies, with many protocols providing only forward stepping on a treadmill, with limited practice overground.3,10,12,13 Conversely, recent data in animal models of spinal cord injury suggest that stepping training with variable “challenges” (ie, multiple directions 18 or overground with obstacles or stairs 19 ) improves locomotor performance greater than forward treadmill training. Such variable training protocols required investigators to reduce stepping speeds to ensure task completion, suggesting a tradeoff between amount and variability of stepping practice within scheduled training sessions.
Few studies have evaluated the feasibility and efficacy of stepping training in variable contexts (tasks or environments) in patients with neurological injury, particularly at high aerobic intensities. Such training may provide less stepping practice as compared with forward treadmill stepping, which may limit walking improvements. Nonetheless, stepping practice in variable contexts may simulate many of the barriers encountered in the community (ie, stairs/curbs, uneven terrains, and altered directions) 20 and be more specific to daily stepping activities.
Training that challenges a variety of locomotor tasks at high intensities may, however, elicit substantial errors in task performance, 21 which is often discouraged by traditional physical therapy paradigms. 22 However, if patients can adjust their locomotor strategies to correct these errors, allowing, inducing, or even augmenting errors during training may improve locomotor performance. The short-term effects of error-augmenting perturbations targeting specific gait deficits (eg, limb swing 23 and step-length asymmetry 24 ) have been tested, with recent studies suggesting long-term improvements with sustained training. 25 Patients poststroke, unfortunately, present with many gait impairments, and practice of multiple, challenging stepping tasks targeting these deficits may further improve locomotor function.
The purpose of this study was to evaluate the feasibility and preliminary efficacy of stepping training provided to individuals poststroke in variable contexts with applied perturbations and at high aerobic intensities. Feasibility was determined by the amount of stepping practice provided and the extent to which high aerobic intensities could be achieved, with estimates of patient tolerance and adverse events. Preliminary efficacy was evaluated in participants with chronic stroke (>6 months) using repeated baseline (BSL) assessments to estimate potential effect sizes, with similar assessments performed in participants with subacute stroke (1-6 months) to evaluate feasibility and efficacy early following injury. We hypothesized that such training would be tolerated by most individuals with few adverse events, although the efficacy of such training was uncertain.
Methods
Participants
Individuals with subacute and chronic hemiparesis following unilateral supratentorial stroke were recruited. Eligible participants presented with gait deficits that ranged from requiring moderate assistance to ambulate 10 m overground (ie, participant can perform 50%-74% of the walking task 26 ) up to walking without assistance but at self-selected speeds (SSSs) <0.9 m/s with devices and an ankle foot orthosis if needed. Additional inclusion criteria consisted of the following: 18 to 75 years old; ability to sit unsupported for 30 s; Mini-Mental Status Exam score ≥23/30; Patient Health Questionnaire <10; lower-extremity passive range of motion of 0° to 30° ankle plantarflexion, 0° to 60° knee flexion, and 0° to 30° hip flexion; and medical clearance to participate. Exclusion criteria were the following: osteoporosis, cardiovascular instability, inability to ambulate >150 feet prior to stroke, previous central nervous system injury, and inability to adhere to study requirements, including use of pedometers (please see below). Patients could not be concurrently enrolled in physical therapy. The project was approved by the local ethics committee; all participants provided written informed consent.
Experimental Protocol
Participants received ≤40 sessions, lasting 1 hour each, within 10 weeks, with a goal of 5 d/wk. Preliminary BSL assessments (PRE-BSL) were collected on chronic patients 4 to 5 weeks prior to BSL testing to evaluate the stability of outcome measures; stability was not expected nor tested in subacute participants. Midtesting (MID) and posttesting (POST) were repeated following up to 20 sessions or 5 weeks, with a 3-month follow-up (F/U).
Training sessions were structured and monitored by 1 of 5 therapists with assistance from a research aide if needed. All therapists followed the training protocol for either subacute or chronic participants as described below, with flexibility to address specific gait deficits using strategies outlined. Therapists regularly discussed strategies used with specific participants to ensure protocol adherence. Within the protocol, the primary goals of training were as follows:
Maximizing repetitions of stepping practice. Training consisted of reciprocal stepping in a specific direction (ie, forward, backward, or sideways) for ≤40 minutes, with rest breaks as needed. Successful stepping was defined as generating positive step lengths (swing limb extending beyond stance limb) without foot drag and absence of limb collapse while maintaining sagittal/frontal plane stability. Verbal feedback was provided to ensure stepping at targeted intensities (eg, cues for stepping further, higher, or quicker). Ankle foot orthoses and posterior knee braces were allowed to minimize orthopedic concerns.
Targeting high aerobic intensities. Training was performed with a goal to maintain HR within 70% to 80% HR reserve, 27 where Maximum Predicted HR = 208 − (0.7 × age) 28 and 70% to 80% HR reserve = Rest HR + [(Maximum HR − Rest HR) × (70%-80%)]. 8 The HR reserve was reduced by 10 to 15 beats/min according to age 29 if participants were prescribed medications to reduce HR. Scores of 15 to 17 (hard to very hard) on the Rating of Perceived Exertion were used for 2 participants unable to achieve 70% HR reserve.
Increasing task demands. Specific perturbations were applied to assist or challenge biomechanical subcomponents of upright walking, 30 including limb swing, weight bearing during stance, forward propulsion, and sagittal-frontal stability. If participants could not demonstrate successful independent stepping as defined above, assistance was provided as needed. With successful stepping, perturbations were applied to increase task difficulty (ie, error augmentation 31 ), with the types and magnitudes of perturbations varied according to an individual’s gait impairments. If participants could not perform successful stepping after 3 to 5 consecutive attempts, task difficulty was reduced to allow continuous stepping. A list of perturbation strategies are provided in the online Appendix and described below:
Limb swing. Participants unable to generate positive step lengths without foot drag were provided manual 16 or elastic 32 assistance only as needed, with progression to unassisted practice. With independent limb swing, task difficulty was increased using posterior-directed elastic resistance, leg weights, 23 or stepping over obstacles. 33
Weight bearing during stance. Participants unable to ambulate without limb collapse were provided weight support with a counterweight harness system only as needed, with support minimized as tolerated. 6 Task difficulty was increased using a weighted vest 34 , reduced upper limb use on handrails 6 , or assistive devices.
Propulsion. Participants with reduced propulsion (ie, slow gait speeds) were provided manual or elastic assistance at the pelvis 34 to maintain desired walking speeds. Perturbations included reduced upper-extremity use, faster stepping speeds, 5 inclined surfaces, 35 or elastic resistance at the pelvis. 34
Sagittal/frontal plane stability. Participants with reduced frontal/sagittal stability were stabilized at the pelvis with manual or elastic assistance 36 or allowed use of handrails 6 or assistive devices. Task difficulty was increased by reducing assistance, handrail use, or assistive devices, progressing to backward or sidestepping 33 ; stepping over or around obstacles 33 ; stepping over uneven, compliant, or narrow surfaces 37 ; and practicing dual physical tasks (eg, catching or dribbling a ball during walking).
Training sessions were divided between treadmill, overground, and stair climbing activities, with continued focus on stepping amount and aerobic intensity during practice of multiple challenging tasks. In the initial 2 weeks (8-10 sessions), all training was performed on the treadmill at the highest speeds tolerated within the targeted intensities (ie, speed-dependent treadmill training). Weight support was applied as necessary, with treadmill speeds between 0.5 and 2.0 km/h, with minimal or no weight support (minimal tension on safety support system); speeds were increased to >2.0 km/h. Participants could hold onto the handrail but were encouraged to minimize weight bearing.
Training over the remaining sessions was divided into 10-minute increments between speed-dependent treadmill training, skill-dependent treadmill training, overground training, and stair climbing. Skill-dependent treadmill training was performed by applying perturbations as described above, including walking in multiple directions or over obstacles with limited handrail use. Perturbations were applied such that 2 to 5 different tasks were randomly alternated and repeated within 10 minutes to ensure substantial task repetition. Overground training focused on high speeds or applied perturbations described above, with 2 to 5 tasks alternated within the 10-minute period. Participants were guarded by therapists with the use of a gait belt or an overhead mobile or rail suspension system for safety, as available. Stair climbing was performed over static or rotating stairs (ie, similar to walking up a down-going escalator; Stairmaster, Vancouver, WA), using reciprocal gait patterns, leading with the paretic limb, with progression to higher speeds and reduced hand rail use.
Outcome Measures
Primary outcomes included changes in daily stepping (steps/d), SSS and fastest possible gait speed (FS) over short distances, and walking distance over 6 minutes (6-minute walk). Outcomes were studied by unblinded assessors. Daily stepping was recorded using Step Activity Monitors (Orthocare Innovations, Seattle, WA). Participants were requested to wear monitors for all waking hours throughout the study, with stepping activity recorded per minute. Changes in daily stepping without concurrent training were obtained at BSL, POST, and F/U by averaging data over 5 to 14 days as available (MID stepping activity was not available without training). Additional analyses included weekly averaged steps per day throughout training and averaged steps per session (1 week encompassed 4-5 sessions).
For overground SSS and FS, data were recorded using the Gait Mat II (Equitest Inc, Chalfont, PA), with assistive devices and braces. If participants required physical assistance, the amount of assistance and a SSS of 0 m/s were recorded. The 6-minute walk was recorded at SSS; the test was terminated after 6 minutes or when participants required assistance.
Secondary measures of spatiotemporal symmetry were utilized to estimate gait quality; such measures have been linked to impaired paretic limb power generation 38 and may reflect altered lower-limb impairments and gait function poststroke. Temporal symmetry was evaluated using paretic single-limb stance time (expressed as percentage gait cycle), with typical values of ~40%. Step length asymmetry was assessed using a ratio of step length that has been used previously 16 :
This calculation results in a maximum value of 100% irrespective of which limb demonstrates longer step lengths, with improvements observed as positive values.
Measures of feasibility included number of sessions attended, average steps per session, and the sessions reaching the targeted aerobic intensities. Additional measures included number of dropouts and adverse events, including orthopedic injuries, cardiovascular events (eg, incidence of hypertension or angina), and falls during and outside of training.
Data and Statistical Analysis
Outcome measures are presented as mean ± standard deviation in the text and tables, with mean ± standard errors in figures. Paired t tests revealed no differences between PRE-BSL and BSL assessments in chronic participants; further analyses utilized only BSL data. Repeated-measures ANOVAs were utilized, with subacute and chronic participants considered separately. Bonferroni corrections were applied for the 16 measures (α= .0031), and post hoc Tukey-Kramer tests were used to identify specific differences. Daily stepping (steps/d) without concurrent training was evaluated at BSL, POST, and F/U. Separate ANOVAs determined differences in weekly steps per day and steps per session during training. Associations between changes in primary outcomes and steps per session or steps per day throughout the study were determined using Pearson’s correlation analyses.
Results
Of 36 individuals consecutively referred to the study, 25 (13 chronic and 12 subacute) fulfilled the inclusion criteria and were enrolled. Data from 3 chronic participants were excluded secondary to inability to complete at least 4 weeks of training. One participant reported exercise intolerance, a second participant relocated to another city, and a third was dismissed secondary to an unstable vascular condition (pulsatile mass in the neck). Only the first participant was unable to sustain the targeted aerobic intensity prior to withdrawal. Demographic and clinical characteristics are presented in Table 1.
Demographic Characteristics of Participants Who Completed the Study. a
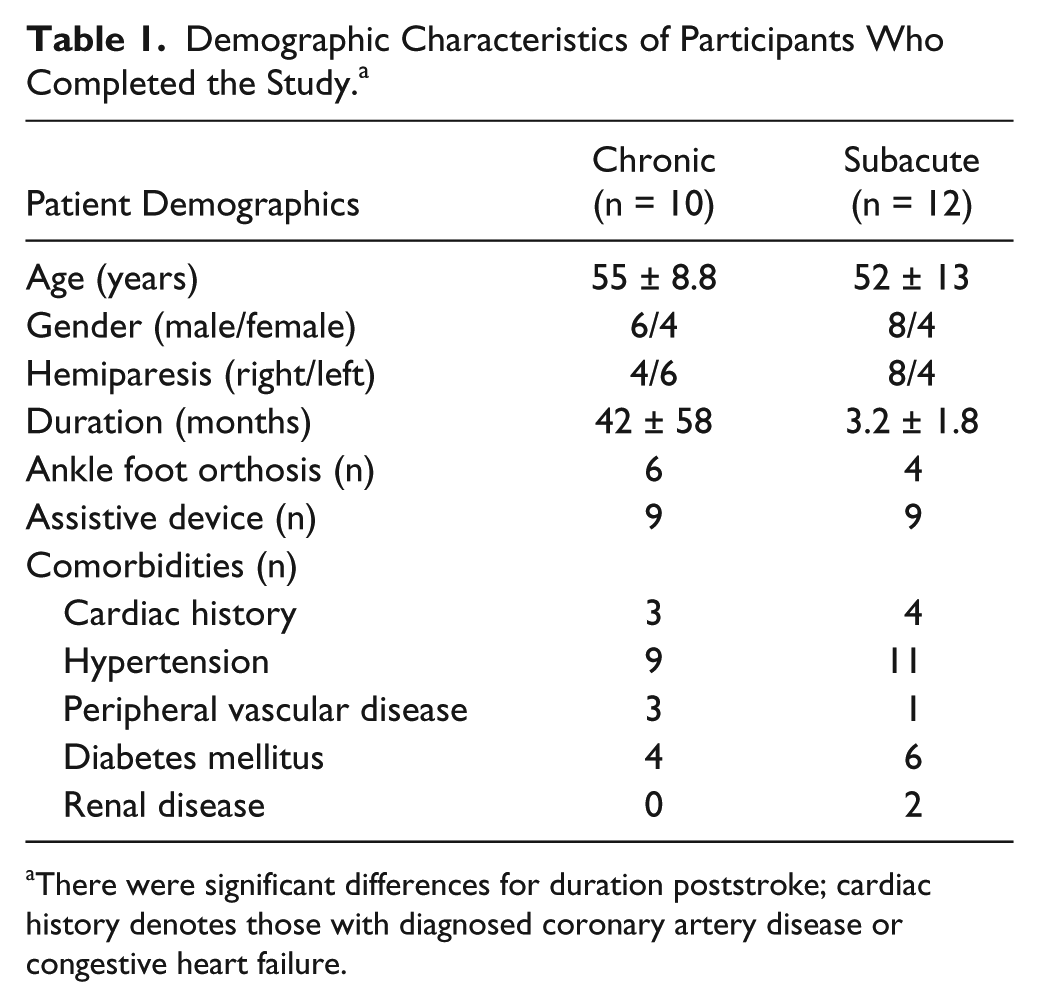
There were significant differences for duration poststroke; cardiac history denotes those with diagnosed coronary artery disease or congestive heart failure.
Of those who completed ≥4 weeks of training, 3 subacute participants required moderate assistance to ambulate at BSL, with all other participants’ SSSs <0.9 m/s (Table 2). Two participants completed only 4 to 5 weeks of training secondary to exercise intolerance (1 chronic) or family obligations (1 subacute), with MID training outcomes imputed to POST; 4 participants sustained a single fall outside of training (1 with humeral fracture), but all completed the study. One reported angina during training, which was controlled with prescribed medications. Incidence of hypertension limited training in 4 participants until consultation with their physician. Also, 5 participants reported transient lower-extremity discomfort during training, which did not interfere with study completion, with no additional orthopedic injuries.
Outcomes for Chronic and Subacute Participants.
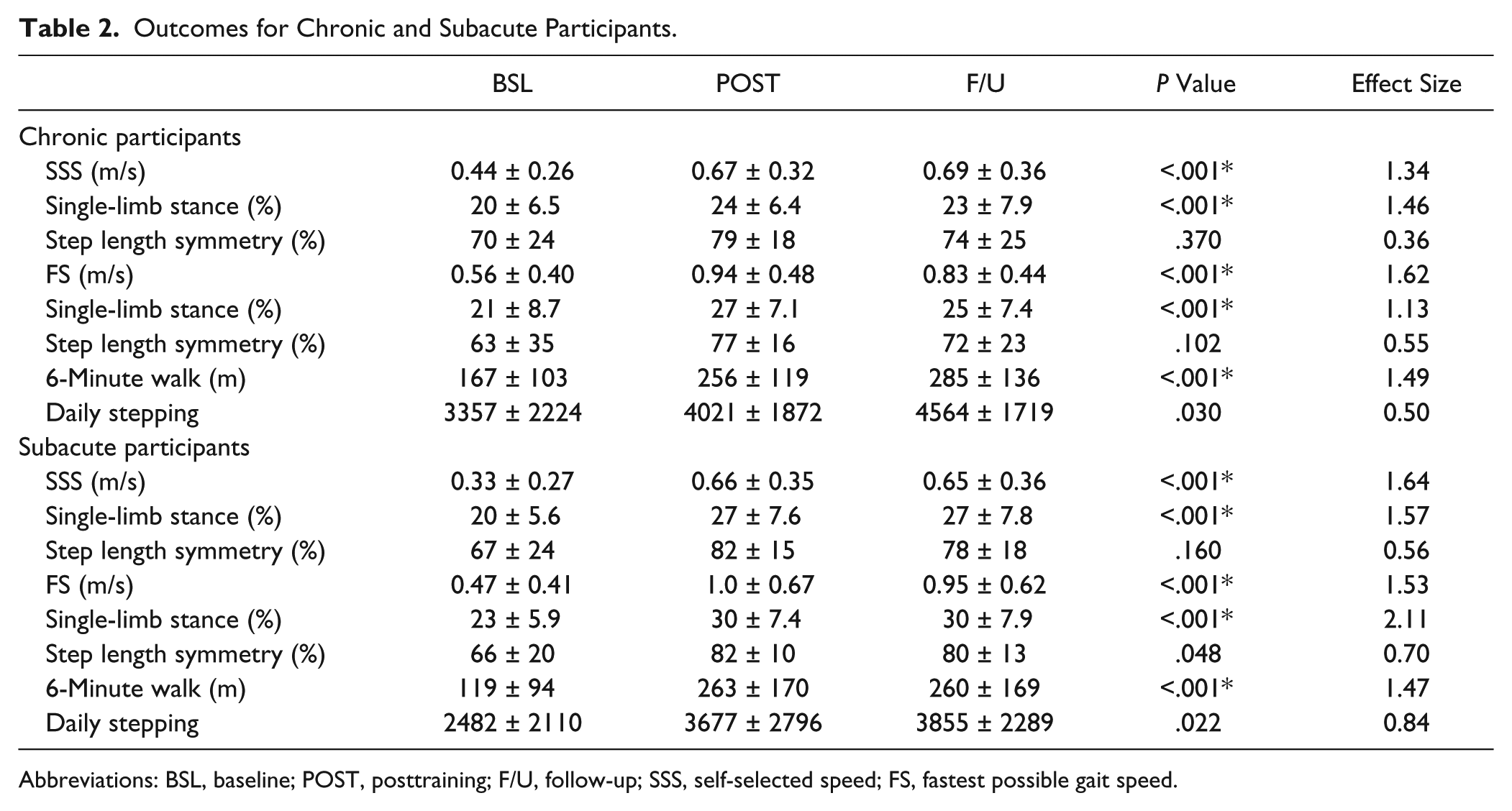
Abbreviations: BSL, baseline; POST, posttraining; F/U, follow-up; SSS, self-selected speed; FS, fastest possible gait speed.
Participants performed an average of 36 ± 5.8 training sessions (range = 17-40); 19 of 22 participants achieved either 70% HR reserve or rating of perceived exertion ≥15 at the first session; all others reached the targeted aerobic intensity by the sixth session and were able to reach this intensity at every session thereafter. Figure 1 depicts mean steps per day of all participants at BSL, POST, and F/U assessments, with weekly average steps per day during training and steps per session. An average of 2887 ± 780 steps/session (subacute, 2845 ± 869; chronic, 2967 ± 722) was performed with no differences across the weeks of training. An average of 5824 ± 2772 steps/d was achieved during the weeks of training (training sessions included). Nonsignificant improvements were observed from BSL to POST (subacute, 1216 ± 454 steps/d; chronic, 658 ± 1367 steps/d) or F/U (subacute, 1395 ± 1368 steps/d; chronic, 1206 ± 1294 steps/d; Table 2).
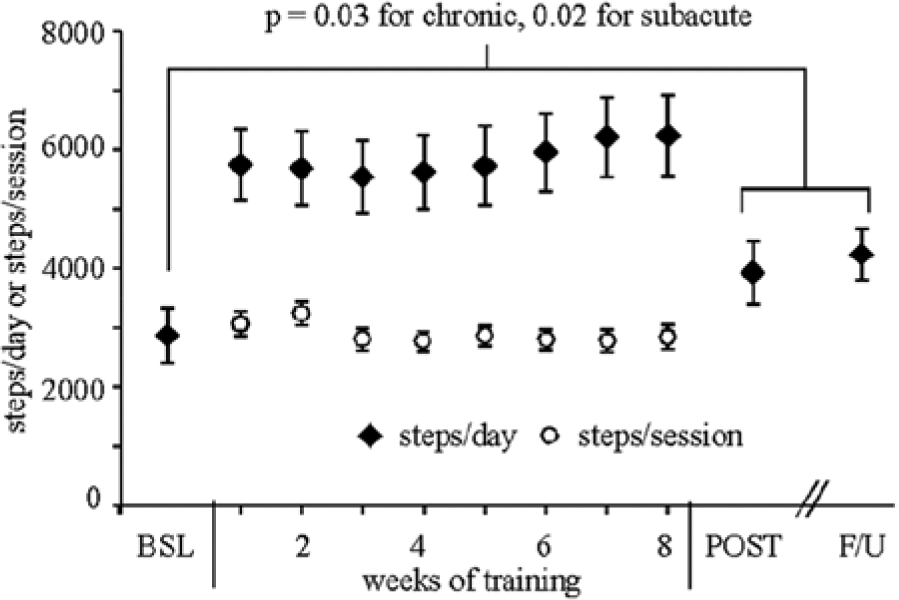
Average daily stepping across all participants at BSL (baseline), POST (posttraining), and F/U (follow-up) at 3 months, with differences not significantly different between BSL compared with POST and F/U. Weekly averages of steps per session and steps per day throughout training were not different throughout training.
Figure 2 and Table 2 depict changes in SSS, FS, and 6-minute walk. For chronic participants, there were no differences from pre-BSL to BSL assessments (Figure 2). Post hoc analyses revealed improvements from BSL to MID, and MID to POST and F/U, with no differences between POST and F/U. Specific differences from BSL to POST included improvements in SSS (subacute, 0.33 ± 0.20; chronic, 0.23 ± 0.17 m/s), FS (subacute, 0.54 ± 0.35 m/s; chronic, 0.39 ± 0.23 m/s), and 6-minute walk (subacute, 144 ± 98 m; chronic, 89 ± 60 m).
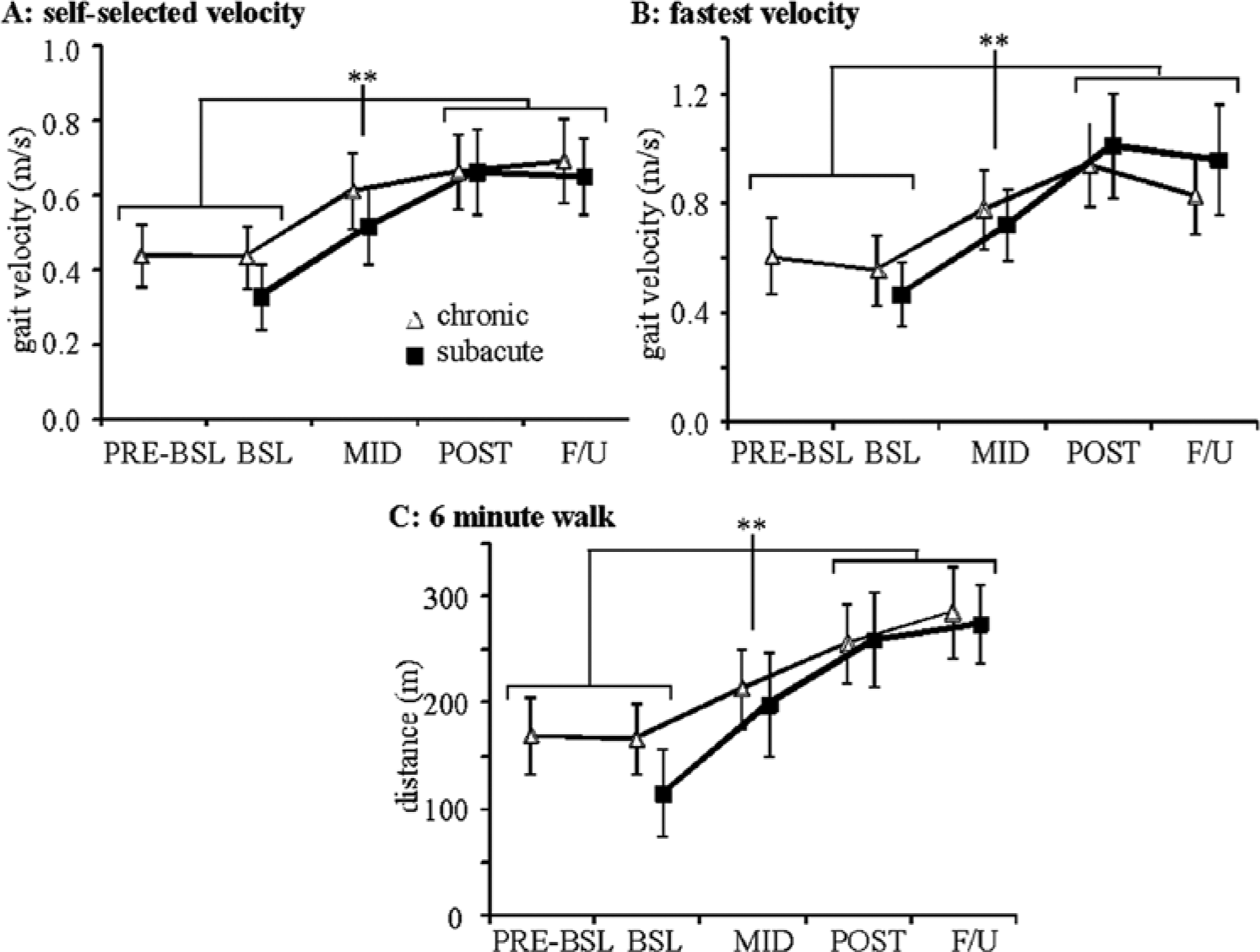
Average changes in (A) SSS, (B) FS, and (C) 6-minute walk at PRE-BSL (chronic only), BSL, MID, POST, and F/U (asterisks indicate Tukey-Kramer differences from BSL to MID to POST and F/U, with no differences at F/U).
Significant changes in gait symmetry were limited to paretic single-limb stance time at SSS and FS in both participant populations, with ~6-7% improvements at POST training (normal ~40%; Table 2). Step-length symmetry demonstrated positive but nonsignificant changes.
Correlation analyses revealed a moderate association between mean steps per session across all training and changes in 6-minute walk from BSL to POST (Figure 3A; r = 0.50; P = .02). However, nonsignificant correlations were observed with changes in other primary outcomes (SSS: r = 0.00, P = .99; FS: r = 0.41, P = .06; daily stepping: r = 0.23, P = .34). Changes in primary outcomes were not correlated to mean steps per day during training (all r < 0.32). Furthermore, changes in outcome measures were not associated with initial walking impairments, as demonstrated for initial versus change in 6-minute walk distance (Figure 3B; r = 0.02, P = .92), with nonsignificant correlations for all other initial versus change scores (all r < 0.10).
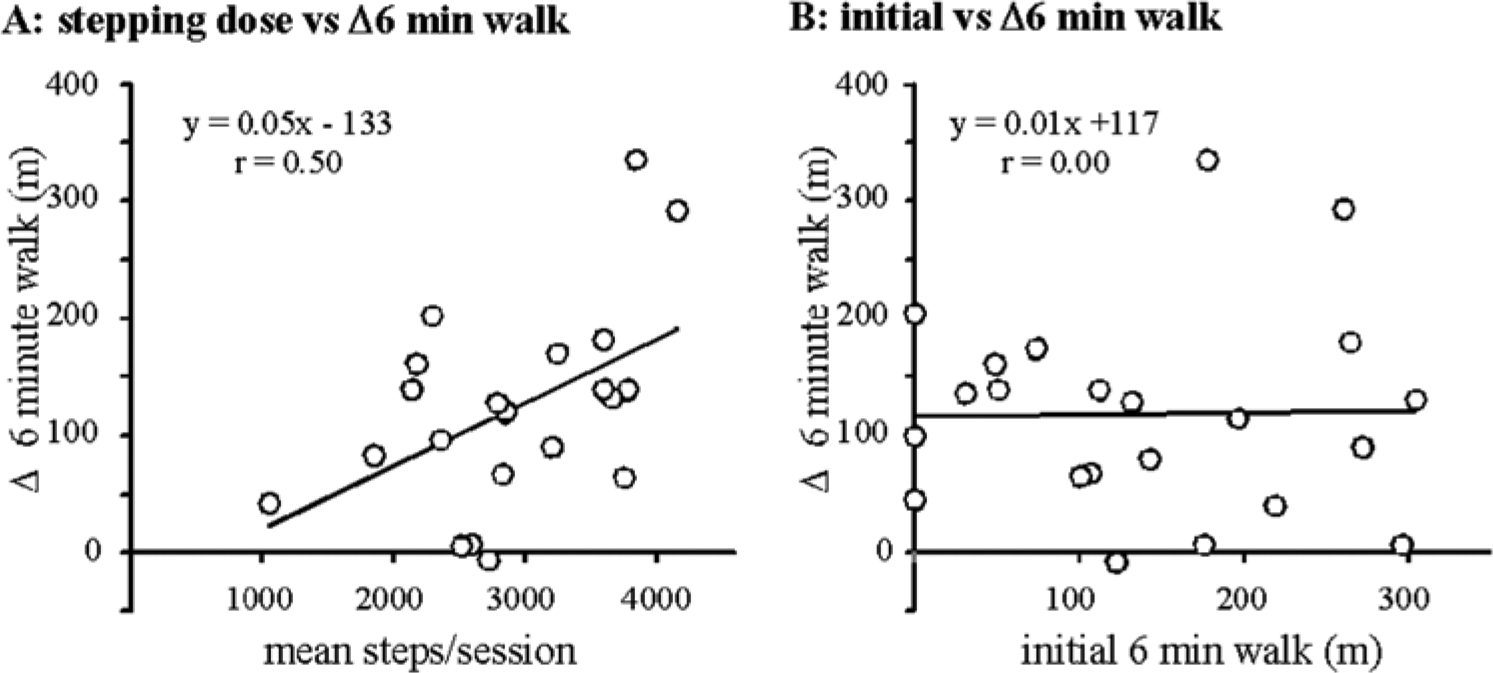
Correlations between (A) average stepping per session throughout session and changes in 6-minute walk and (B) initial values and changes in 6-minute walk.
Discussion
The present study assessed the feasibility and preliminary efficacy of providing stepping practice in variable challenging contexts at high aerobic intensities. Of those enrolled, 12% (3 chronic participants) dropped out or were dismissed prior to completing 4 weeks of training, similar to other stepping training protocols.11,14 Two additional participants did not complete 8 weeks with data imputed to POST training. Adverse events regarding fall incidence and cardiovascular events were noted, with only 1 event requiring study dismissal. Significant changes were observed for SSS, FS, and 6-minute walk at MID training, with continued improvements at POST training. There was no significant improvement observed for daily stepping. Despite the primary focus on task completion (ie, successful stepping as described), significant changes in paretic single limb stance but not step length symmetry were observed.
The average steps/session provided in the present study was nearly 3 to 10 times greater than previously observed in clinical physical therapy sessions of individuals poststroke (average range of 200-900 steps/session).3,39 However, stepping activity in this study was approximately ~1000 steps/session less than forward treadmill training at high aerobic intensities 3 in individuals with similar diagnoses and locomotor function (average SSS = 0.51 ± 0.21 m/s). The moderate, significant correlation with only the 6-minute walk suggests that amount of stepping practice may contribute to walking outcomes, although this relationship is uncertain.
The aerobic intensity of training may have also contributed to improved walking function. Training protocols that provide treadmill stepping at high aerobic intensities nearly always elicit improvements in cardiovascular function, but demonstrate variable changes in locomotor outcomes (6-minute walk10,12 vs daily stepping 3 ). However, improvements in standard measures such as SSS are often not significantly different from control interventions.3,10,12
Practice of multiple, variable tasks is not a novel rehabilitation strategy for individuals poststroke. Multicenter evaluation of clinical physical therapy sessions with patients poststroke in different settings indicate that practice of many tasks occurs within single sessions (eg, transfers, strengthening, balance, and gait). 39 However, sufficient practice of any 1 task may be limited with this approach. Conversely, training of variable tasks while focusing entirely on stepping activities at high intensities has received very limited investigation in individuals poststroke. In a higher-functioning population (initial SSS = 0.62 ± 0.24 m/s), Ada et al 33 used a treadmill and overground walking program in multiple environments and directions with additional cognitive tasks but did not focus on application of perturbations to elicit errors, nor on training intensity (see also Musselman et al 40 for similar protocols in spinal cord injury). Studies focusing on inducing or augmenting gait errors have revealed transient changes in specific biomechanical walking tasks (limb swing 23 and step symmetry 24 ) following short-term training perturbations, with recent promising data detailing long-term improvements with sustained training. 25 However, focus on single gait deficits may not address the multiple impairments that contribute to locomotor dysfunction poststroke.
An additional rationale for providing stepping training in variable challenging contexts was to simulate tasks and environments encountered in the community to improve daily stepping. The changes in daily stepping observed here were similar to those observed in other studies in patients poststroke (subacute 11 and chronic 3 ), although were not statistically significant. Lack of significant improvements may be partly because of the strict α level utilized with multiple comparisons but also because of the inherent variability of daily stepping observed in patients poststroke (see Table 2). Nonetheless, the observed changes were not sufficient to increase average daily stepping above the threshold of sedentary activity (ie, 5000 steps/d). 41 Greater focus toward developing training paradigms or community programs directed toward enhancing daily stepping may be warranted.
Improvements in other primary outcomes were significant, with average changes well above minimally clinically important differences (MCID) in gait speed (0.10 m/s) or 6-minute walk (50 m). 42 Improvements in paretic single-limb stance time at SSS and FS were also observed, although changes may partly reflect increases in walking speed. In general, the kinematic patterns approached normal gait symmetry without substantial focus on gait patterns during training other than task completion.
The primary limitations of this preliminary study included a lack of a control group and unblinded assessors; such limitations cannot exclude the possibility of history, testing, or selection effects or potential bias by the assessors evaluating the reported outcomes. Furthermore, the small sample size may limit generalizability of the findings. The present data and derived effect sizes now permit sample size calculations for future randomized trials in similar patient populations. Given the variability of daily stepping, SSS, FS, and 6-minute walk would be likely choices for primary outcomes, all of which demonstrated very large effect sizes. Defining comparative training strategies remains a primary question, however, because stepping amount, intensity, and variability/challenge may all represent important independent training parameters. For example, high-intensity treadmill training provides substantial amounts of stepping practice but limited variability, with improvements in chronic stroke ranging from 0.05 to 0.13 m/s for SSS3,5,10,43 and 27 to 58 m for the 6-minute walk.3,10,12 For subacute stroke, changes in SSS range from 0.23 to 0.26 m/s,4,11 with 6-minute walk improvements from 60 to 82 m. Such changes are also substantial and above specific MCIDs, and evaluation of the present versus previous protocols requires further investigation.
In summary, substantial amounts of walking practice provided during high-intensity stepping training in variable contexts was tolerated by nearly all participants throughout 4 to 8 weeks and elicited significant improvements in selected outcome measures. Future investigations should focus on identifying the contribution of each training variable to locomotor outcomes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by NIDRR Grant #H133B031127.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.