
Abstract
Objective. To develop consensus recommendations for the use of repetitive transcranial magnetic stimulation (rTMS) as an adjunct intervention for upper extremity motor recovery in stroke rehabilitation clinical trials. Participants. The Canadian Platform for Trials in Non-Invasive Brain Stimulation (CanStim) convened a multidisciplinary team of clinicians and researchers from institutions across Canada to form the CanStim Consensus Expert Working Group. Consensus Process. Four consensus themes were identified: (1) patient population, (2) rehabilitation interventions, (3) outcome measures, and (4) stimulation parameters. Theme leaders conducted comprehensive evidence reviews for each theme, and during a 2-day Consensus Meeting, the Expert Working Group used a weighted dot-voting consensus procedure to achieve consensus on recommendations for the use of rTMS as an adjunct intervention in motor stroke recovery rehabilitation clinical trials. Results. Based on best available evidence, consensus was achieved for recommendations identifying the target poststroke population, rehabilitation intervention, objective and subjective outcomes, and specific rTMS parameters for rehabilitation trials evaluating the efficacy of rTMS as an adjunct therapy for upper extremity motor stroke recovery. Conclusions. The establishment of the CanStim platform and development of these consensus recommendations is a first step toward the translation of noninvasive brain stimulation technologies from the laboratory to clinic to enhance stroke recovery.
Keywords
Introduction
Rehabilitation is critical for reducing stroke-related disability. 1 There is a growing recognition that cortical neuroplasticity supporting adaptive recovery may extend for years after stroke.2,3 Although intensive task-specific therapy promotes neuroplasticity and improves function poststroke,4,5 the frequency and intensity of task-specific therapy in a standard clinical rehabilitation session is insufficient to invoke these changes.6-8
Transcranial magnetic stimulation (TMS) is a safe, noninvasive method of stimulating the cerebral cortex. 9 Repetitive TMS (rTMS), when used either at low or high frequencies, may have the potential to enhance the brain’s ability to relearn task-specific functions and reduce the amount of standard therapy required to achieve functional gains.10,11 rTMS can modify cortical excitability both in local intracortical networks and in regions distal to the site of stimulation.12,13 Specifically, while stimulation of ipsilesional primary motor cortex (M1) at low frequencies (≤1 Hz) may reduce the amplitude of motor evoked potentials (MEP) as a measure of cortical excitability, M1 stimulation at high frequencies (≥5 Hz) can enhance it.14,15 Similarly, when applied to homologous regions in the contralesional hemisphere, inhibitory (low frequency) 1-Hz rTMS can modulate mechanisms of transcallosal inhibition, promoting functional reorganization in affected regions in the ipsilesional hemisphere. 16
While 2 recent multicenter studies have shown benefit for applying rTMS during stroke rehabilitation,17,18 a recent randomized-sham controlled trial of navigated rTMS in 167 (primarily) chronic stroke patients showed no difference between 1 Hz active and sham stimulation on measures of upper extremity motor function at 6 months. 19 The use of rTMS interventions in stroke rehabilitation trials has been limited by a lack of consensus regarding optimal parameters for the clinical application of TMS in stroke populations. Recent clinical guideline recommendations for the therapeutic use of rTMS indicate Level A evidence support for the efficacy of low-frequency rTMS to contralesional M1 in hand motor recovery at the post-acute stage. 20 However, it is important to note that, in light of the negative results from the NICHE trial, 19 evidence for the efficacy of low-frequency rTMS to contralesional M1 for motor recovery at the chronic stage was downgraded to possible efficacy (Level C). 20 Despite the fact that the beneficial effects of rTMS across these studies were primarily observed when rTMS was used before 30 to 60 minutes of physical therapy to prime recovery, these recommendations offer no consensus on the type of physical therapy to be combined with rTMS, the frequency and duration of rTMS sessions, patient characteristics, or specific outcome measures, representing a critical knowledge gap for the translation of rTMS to clinical practice.
The purpose of the present consensus process was to develop recommendations for a comprehensive clinical trials protocol for the investigation of the efficacy of rTMS as adjunct to physiotherapy in stroke rehabilitation clinical trials, with a specific emphasis on (1) patient population, (2) rehabilitation intervention, (3) outcome measures, and (4) stimulation parameters. Although several rTMS methods are available (ie, standard, accelerated, theta burst), the present recommendations focus exclusively on the standard use of rTMS for the recovery of upper extremity motor function poststroke, as the majority of available experimental and clinical data pertained to this area of research.
Methods
Participants and Consensus Process
The Canadian Platform for Trials in Non-Invasive Brain Stimulation (CanStim) is a national platform that aims to facilitate multicenter clinical trials for noninvasive brain stimulation interventions to augment recovery from stroke. As a first step, CanStim investigators convened a multidisciplinary team of experts in rTMS from institutions across Canada to form the CanStim Consensus Working Group and develop consensus recommendations for the delivery of rTMS as an adjunct to standard therapy in stroke rehabilitation clinical trials.
Prior to the consensus conference, we surveyed participants and stakeholders to identify 4 key themes specific to the use of rTMS and assigned experts from the Consensus Working Group as theme leaders: (1) patient population, (2) rehabilitation intervention, (3) outcome measures, and (4) stimulation parameters. Theme leaders conducted comprehensive literature reviews for each theme, according to accepted norms for Levels of Evidence (Supplemental Figure 1) and compiled available evidence for review by the CanStim Consensus Working Group members.
In November 2017, CanStim hosted a 2-day Consensus Conference with members of the Consensus Working Group. Theme leaders presented literature reviews for each theme. Members were then divided into teams and break-out sessions were conducted for each consensus theme to identify up to a maximum of 5 decision items for consideration by the entire Consensus Working Group.
Several items were identified as standard requirements for the use of rTMS in stroke rehabilitation clinical trials which did not require consensus (Table 1). There was also unanimous consensus to adopt the recommendations of the Stroke Recovery and Rehabilitation Roundtable (SRRR) for demographic and stroke information data collection. 21
Standard Recommendations Adopted by the Canadian Platform for Non-Invasive Brain Stimulation (CanStim) Expert Working Group for the Use of rTMS as an Intervention in Motor Stroke Recovery Rehabilitation Trials.
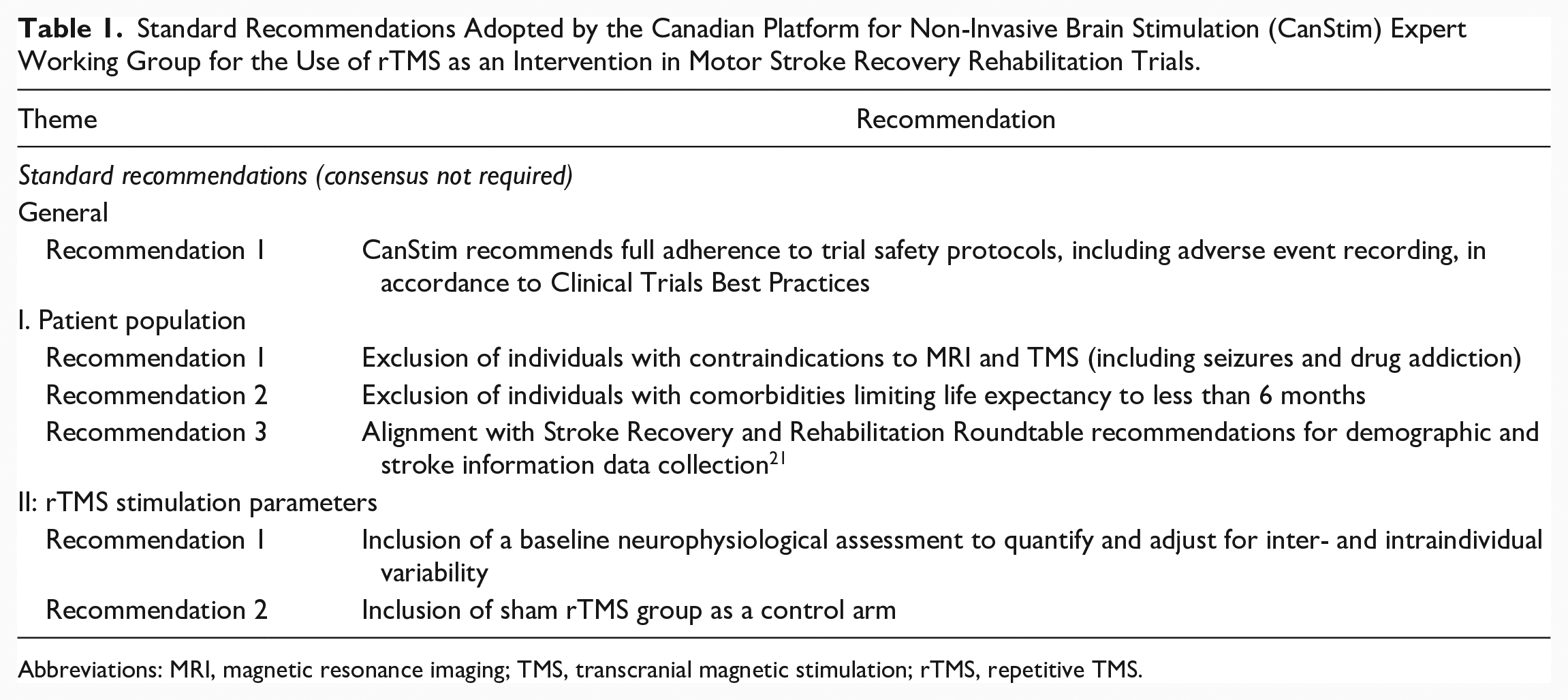
Abbreviations: MRI, magnetic resonance imaging; TMS, transcranial magnetic stimulation; rTMS, repetitive TMS.
For each decision item, alternatives were provided and consensus was reached via a weighted dot-voting procedure. Working Group members were each given 12 voting dots and were required to vote for the items within each theme they considered to be both essential and feasible for the use of interventional rTMS for upper extremity motor stroke recovery in the clinical trial setting. Weighted voting was permitted for items considered of greater versus lesser importance. Results of the voting procedure were tallied. Cutoffs of <40% and >60% were defined as majority and minority cutoffs for low versus high voter agreement and the middle range (between 40% and 60%) was defined as inconclusive and meriting further discussion by the entire Consensus Working Group. A moderated plenary discussion was conducted to review each item with moderate agreement and final consensus was reached via a majority vote.
Results
Descriptions and evidence ratings for the final consensus recommendations are provided in Table 2.
Final Consensus Decision Recommendations From the Canadian Platform for Non-Invasive Brain Stimulation (CanStim) Expert Working Group for the Use of rTMS as an Intervention in Motor Stroke Recovery Rehabilitation Trials.
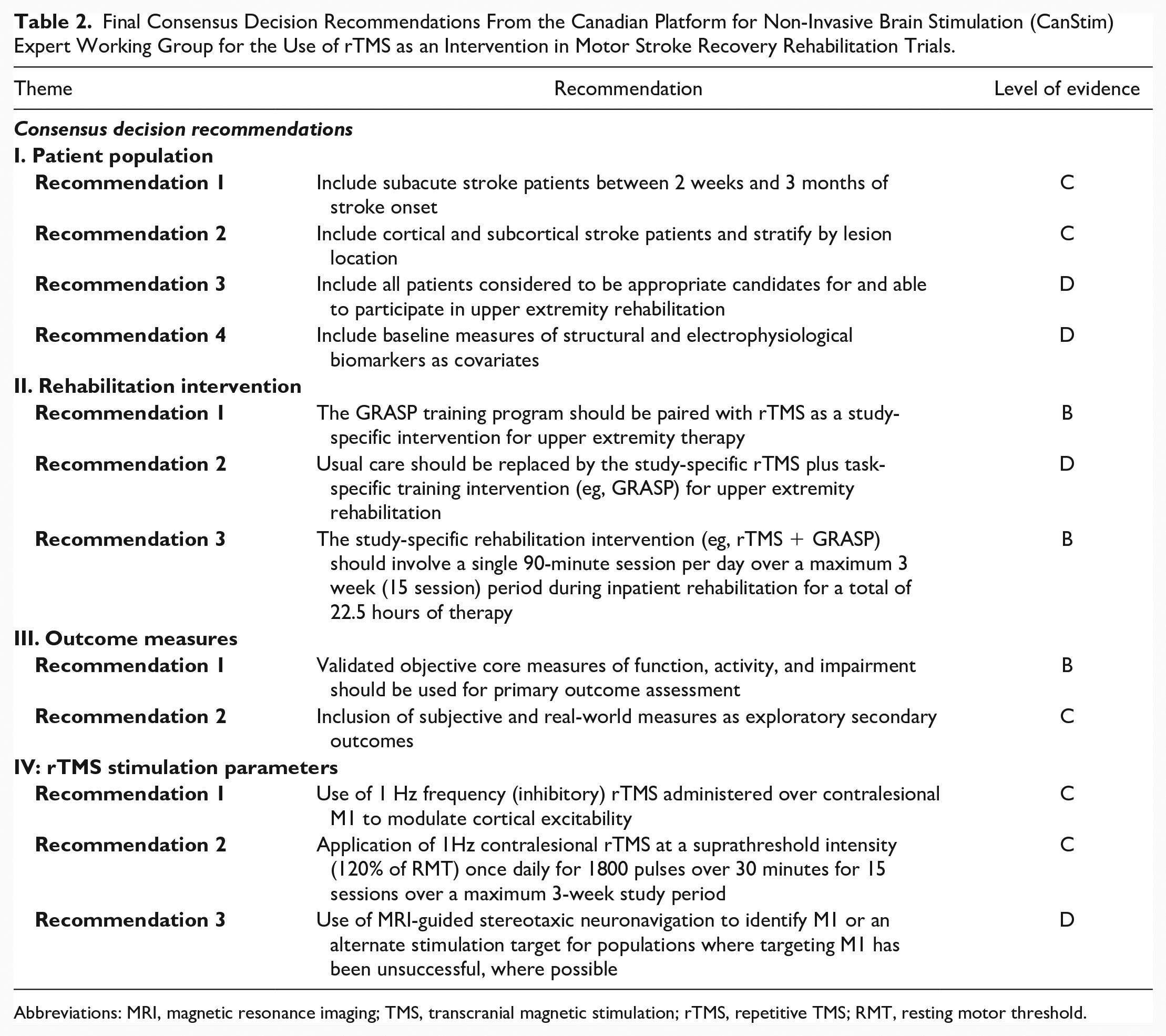
Abbreviations: MRI, magnetic resonance imaging; TMS, transcranial magnetic stimulation; rTMS, repetitive TMS; RMT, resting motor threshold.
Theme 1: Patient Population
Recommendations for patient selection criteria were based on evidence from 5 systematic reviews,22-26 1 meta-analysis, 27 2 consecutive prospective trials,28,29 and recommendations for patient biomarkers were based on 2 systematic reviews30,31 and 1 consensus paper 32 (Supplemental Table 1).
Timing of Treatment Onset
Recovery of motor function after stroke is a dynamic, nonlinear process with the largest functional improvement occurring in the first months poststroke. It has previously been recommended that rehabilitation interventions consider this trajectory. 33 However, evidence for the optimal time interval to start standard rehabilitation22,24 and, specifically for the timing of the initiation of rTMS as an adjuvant therapy, is inconsistent. 26 While evidence for contralesional (low frequency) 1-Hz rTMS in chronic stroke was classified as level B and for subacute stroke as level C, 26 none of the reviewed studies were specifically designed to investigate the question of timing. While recent meta-analyses of randomized controlled trials (RCTs) showed greater effects of rTMS for upper limb motor recovery when administered in the acute and subacute versus chronic stages poststroke,34,35 another only showed significant benefits of rTMS for fine motor performance in mild-moderate chronic stroke patients. 36 Evidence from a matched case-control study 28 specifically investigating the effectiveness of early (<20 days) versus delayed (21-40 days and 41-60 days) onset of rehabilitation for global functional outcome favored early onset treatment within 20 days. 28 A similar time window can be derived from an observational cohort study of 1197 consecutive patients, showing that 95% of patients completed functional recovery between 8 and 17 weeks. 29 There thus may be moderate evidence favoring early treatment (during the first months after stroke) using rTMS as an adjunctive therapy34,35 and from data for other therapies, including assistive technologies for upper extremity (UE) rehabilitation22,37 and low-dose constraint-induced movement therapy (CIMT). 24
Based on the available data (Supplemental Table 1), only moderate consensus was reached for the proposed onset time windows (ie, 2 weeks to 3 months vs 3-6 months vs >6 months) in stroke rehabilitation clinical trials. In the subsequent plenary discussion, feasibility of patient recruitment, patient safety, and spontaneous recovery as a potential confounder were discussed. In a review of the literature on rTMS safety, we found 2 recent reports of delayed seizure onset after 1-Hz TMS in chronic stroke patients, one occurring at 24 hours poststimulation 38 and the other at 18 hours poststimulation 39 ; however, no reports of seizure associated with low-frequency stimulation to the contralesional hemisphere in the subacute phase poststroke. In addition, data supporting the safety and the feasibility of contralesional 1-Hz rTMS performed early after subcortical stroke are also available. 40 A recent editorial 41 of these findings suggests that low-frequency rTMS is not suspected to have seizure-eliciting properties as, unlike high-frequency rTMS, it does not involve fast rhythmic stimulation or enhance cortical excitability of the target area and emphasizes that prior evidence-based clinical guidelines have indicated that “a direct epileptogenic effect of rTMS on the target region is improbable, since low-frequency rTMS reduces cortical excitability” 42 and the target region is contralesional cortex not directly affected by ischemia.
The Working Group also considered logistic requirements within the specific context of standard stroke rehabilitation care in the Canadian public health system. Across Canada transfer from acute stroke units to rehabilitation settings typically takes place between 10 and 14 days and most patients will start rehabilitation therapy at around 2 weeks poststroke. 7 Length of treatment varies between 6 and 18 weeks and intense poststroke rehabilitation is rarely given after 4 to 6 months. 7 The subacute period thus represents the period of greatest standardization of treatment for stroke rehabilitation, but it is important to note that rTMS as an adjunct to rehabilitation training has potential to enhance motor function beyond this specific time window. In the absence of strong evidence favoring a specific timing of treatment onset, the consensus group felt it was critical to time-lock the delivery of the adjunct therapy with the period of the most intensive delivery of standard-of-care stroke rehabilitation in order to adequately test the efficacy of rTMS to augment recovery and thus recommended that rTMS stroke rehabilitation clinical trials include patients in the subacute phase, between 2 weeks and 3 months poststroke.
Infarct Location
As imaging was not a necessary inclusion requirement for most systematic reviews, evidence for a differential role of cortical versus subcortical infarct location in UE recovery is scant.22,24 One systematic review reported differential efficiency for 1-Hz rTMS over the affected hemisphere in subcortical but not cortical stroke 26 and one meta-analysis 27 conducted a planned subgroup analysis on lesion site and found a mean effect size of 0.73 (95% confidence interval [CI] = 0.44-1.02) for the subcortical group compared to 0.45 (95% confidence interval = 0.23-0.67) for the group with nonspecified lesions. In addition, one prior study reported motor improvement associated with high-frequency (10 Hz) TMS over ipsilesional M1 for patients with subcortical but not cortical stroke. 43 Available evidence was thus considered insufficient to exclude patients from trial participation based solely on infarct location and consensus was reached in favor of recommendations for rTMS rehabilitation clinical trials that include patients with both subcortical and cortical lesions; however, it was recommended that all trials perform stratification by lesion location to determine potential location-specific effects.
Stroke Severity
Lesion load to the cortical spinal tract (CST) and cortical motor regions correlates with motor impairment at baseline. 44 While impairment of UE function at baseline remains the best single predictor of recovery, 23 neglect, incontinence, impaired visual and sensory function, and higher global disability also predict poorer outcomes. 23 Nonmotor stroke deficits may also further limit a patient’s capacity for motor rehabilitation45-47 and initial deficit severity may impact the feasibility and effectiveness of a specific intervention. 24
Within stroke patient care trajectories in the Canadian public health system, standardized individual assessments of rehabilitation needs are routinely performed in the acute hospital setting and again upon admission to rehabilitation centers. Within this context, the ability of a patient to participate in a specific UE rehabilitation program constitutes an alternative criterion for patient eligibility. Based on evidence for the high number of potential confounders which may influence intervention efficacy beyond standardized measures, consensus was reached to recommend the inclusion of patients in rTMS stroke rehabilitation clinical trials based on rehabilitation needs and ability versus standardized measures of severity.
Baseline Patient Structural and Electrophysiological Biomarkers
Measures of CST integrity include fractional anisotrophy (FA) derived from diffusion tensor imaging (DTI) as index of structural integrity, and the presence or absence of motor evoked potentials (MEPs), which indicate electrophysiological integrity.30,31,48 While the available evidence is insufficient at present to recommend one or both of these measures to individualize clinical treatment decisions, recent consensus recommendations suggest that measures of the CST should be used to stratify individuals in clinical stroke recovery trials. 32
Consensus was reached to recommend that stroke rehabilitation trials include both structural and electrophysiological measures of CST integrity, including DTI and binary MEP parameters (MEP+/MEP−) as covariates to retrospectively identify potential therapy responders from nonresponders. The working group agreed that further evidence is required prior to exclusion of patients from trial participation based on biomarker data or prior to initiation of trials with differential interventions based on these biomarkers.
Theme 2: Rehabilitation Interventions
Recommendations for the type, delivery, and dosing of rehabilitation interventions were based on the Canadian Best Practice Recommendations for Stroke Care, 49 the Evidence Based Review of Stroke Rehabilitation, 50 1 systematic review and meta-analysis, 51 and 1 Cochrane review of upper extremity interventions poststroke 22 (Supplemental Table 1).
Type of Rehabilitation Paired With rTMS
In stroke rehabilitation, direct task-specific training focuses on improved performance in functional tasks through goal-directed practice and repetition.5,52 Task-specific training not only improves functional outcomes53-55 but also induces neuroplastic changes that support continued recovery.10,56 Direct task-specific therapeutic interventions are thus the established standard of care for inpatient rehabilitation, with Canadian Best Practice Recommendations indicating that stroke patients should receive 3 hours per day, 5 days a week. 57
Based on these recommendations, the working group considered evidence for 2 interventions that align with the principles of task-specific therapy: CIMT 58 and the Graded Repetitive Arm Supplementary Program (GRASP). 59 Available evidence from across 41 RCTs including patients in all phases of rehabilitation shows Level 1 evidence for the efficacy of CIMT for improvement of UE function late (>6 months) in stroke rehabilitation.1,33,50,60 However, a similar level of evidence (A and 1b, respectively) indicates that CIMT is not effective early (<6 months) after stroke. Furthermore, despite evidence of efficacy, CIMT has not been widely implemented by therapists in the clinical setting.61-63 owing to a number of factors, including the large practice doses required (much greater than 3 h/day).
GRASP is a supplemental arm and hand training program, which is designed to increase the intensity of use of the affected arm. GRASP has been shown to increase active movement and functional use of the affected arm between therapy sessions 59 (Early- Evidence Level B; Late—Evidence Level C) and, unlike CIMT, is available to a greater number of patients, 59 is easier and cheaper to administer, and as a result has undergone a more rapid translation into clinical practice. 64
Consensus was not reached and further discussion of these therapies via a moderated plenary session was required. Given conflicting evidence for the effectiveness of CIMT in early stroke rehabilitation compared to Level of Evidence B for GRASP and evidence of better uptake for GRASP versus CIMT among practitioners, consensus was reached to recommend GRASP as an effective and feasible intervention for upper extremity training at the subacute stage.
Specific Therapy Versus Standard of Care
Best evidence for the effectiveness of rTMS for the rehabilitation of motor function after stroke supports the use of rTMS as an adjunct therapy in combination with a PT or OT intervention. 42 The majority of rTMS studies to date have administered therapy sessions following stimulation. 22 However, in many cases the UE intervention was left to the discretion of treating therapists and thus did not control for dose, or therapy content and intensity. 65 Indeed, in a recent meta-analysis of RCTs, when variable treatment protocols were used across studies, rTMS combined with upper-limb training conferred no additional benefit 66 and in the few instances where the UE intervention was controlled, 67 no control or sham group was included. Thus, as isolating the effect of rTMS as an adjunct to an UE intervention requires the standardization of treatments within and across sites, the Working Group recommended that stroke rehabilitation trials replace usual and customary care with a standardized study-specific rehabilitation intervention.
Dose and Duration of Intervention
While Canadian Best Practice Recommendations suggest 3 hours per day of direct task-specific therapy, 5 days a week, 57 numerous studies have demonstrated that the amount of therapy patients actually receive is considerably less.68-70 This discrepancy presents a challenge for determining an effective, yet feasible, dose of therapy. Repetitive task training seems to have a beneficial effect when given for more than 20 hours in total over the entire training period. 22 Recent studies confirm that an increase in therapy dose results in improved functional recovery,71,72 yet others have shown this dose-effect relationship does not seem to hold for all therapies and therapeutic windows. 73
Considering the evidence and the feasibility of integrating treatment into the patient’s individual therapy schedule, as well as the duration of the TMS after-effect (see Theme 4), consensus was reached to recommend 120 minutes of therapy per day (30 minutes of rTMS plus 90 minutes of GRASP), yielding a total of 22.5 hours of therapy over a maximum 3 week (15 sessions) study period during standard inpatient rehabilitation, with an allocation of 30 minutes of therapist-guided free therapy per session to be performed after the study-specific therapy.
Theme 3: Outcome Measures
Recommendations for core outcome measures were based on evidence from 2 systematic reviews74,75 and recent consensus recommendations from the SRRR group. 21 Recommendations for secondary subjective and real-world outcomes were based on evidence from 1 RCT, 76 1 systematic review, 77 and the SRRR recommendations 21 (Supplemental Table 1), with consideration of feasibility and implementation.
Primary Outcomes: Validated Objective Core Measures
The World Health Organization (WHO) International Classification of Functioning Disability and Health (ICF) distinguishes between the domains of (1) body structure and function, (2) ability, and (3) participation. 78 Due to the vast array of available outcome measures, 74 consensus was reached to adopt a suite of validated objective primary outcomes composed of measures of functional impairment (ICF domain 1) and activity (ICF domain 2), in accordance with SRRR recommendations for the subacute phase of recovery, who previously published ratings of available measures. 21
To measure body function and impairment, the working group recommended the motor portion of the Fugl-Meyer Assessment (FMA) of the upper limb, which has been shown to be a reliable measure of motor impairment following stroke 74 and is recommended for interventional trials targeting motor function 79 with favorable psychometric properties, including moderate interrater and test-retest reliability and interpretability.21,75 For assessment of motor activity and limitations of the upper-limb, the Action Research Arm Test (ARAT) is recommended due to its psychometric properties and its sensitivity to measure change in motor function21,75 and has been shown to have high intra- and interrater reliability. 80 Finally, the Modified Rankin Scale (mRS), 81 a clinician-reported measure of global disability is recommended to index global impairment, as it is one of the most widely used scales for the evaluation of stroke outcomes and a frequent end point in randomized clinical trials. 82 However, it is important to note that some have shown significant interobserver variability with the use of the ARAT and mRS and in recovery clinical trials.83,84 Given prior recommendations,21,79 evidence for the clinical utility of these measures, 85 and comparability to previous studies, the consensus of the working group was to include the FMA, the ARAT, and the mRS as the core set of primary outcome measures, but to also include multiple secondary and exploratory measures to provide a comprehensive set of outcome assessments.
Exploratory Secondary Outcomes: Patient-Centered and Real-World Measures
Given that only patient-centered outcomes can assess the efficacy of a specific therapy to improve functional independence and social participation, these measures were included as a decision item for this theme. Two such individualized patient-centered goal directed tools are the Canadian Occupational Performance Measure (COPM) 86 and the Stroke Impact Scale (SIS), a patient-centered measure of difficulty of hand use. 87 A previous RCT using transcranial direct current stimulation in perinatal stroke showed significant increases in COPM scores with stimulation, despite a lack of change in motor function on objective measures. 88 In adult stroke, the COPM has also been shown to have satisfactory reliability and validity. 89 The SIS correlates strongly with scores on standard scales, 90 but has also been shown to be sensitive to the presence of arm motor deficits in patients classified as having minimal or no disability. 91
In addition to patient-centered outcomes, SRRR recommendations identified the need for recovery trials to evaluate kinematic measurements alongside clinical assessments. 21 The working group identified real world actigraphy measures as a means to quantify continuous UE use. Lightweight wrist accelerometers can constantly measure and store subtle movements and also track movements in disabled persons. A recent study using pedometers to monitor walking performance in chronic stroke patients demonstrated feasibility for this approach 92 and it has also recently been incorporated in an active clinical trial protocol. 93 Thus, despite insufficient evidence to recommend the inclusion of these measures as primary outcomes, consensus was reached to recommend the COPM, SIS, and wrist actigraphy as exploratory secondary outcomes.
Theme 4: Stimulation Parameters
Recommendations for the optimal parameters for use of rTMS were based on evidence-based guidelines for the therapeutic use of rTMS, 42 3 systematic reviews,26,65,94 and the 2015 update of the International Federation of Clinical Neurophysiology report 95 (Supplemental Table 1).
Stimulation Frequency and Location
Increasing evidence indicates that the use of both 1 Hz and 5 Hz rTMS to modulate M1 excitability have beneficial effects for motor recovery poststroke.26,96,97 Based on this work, there is evidence that “conventional” rTMS protocols consist of either the upregulation of excitability in the ipsilesional motor cortex via high-frequency (>5 Hz) stimulation or downregulation of excitability in contralesional cortex via the use of low-frequency (>1 Hz) stimulation. 42 Evidence for the therapeutic value of these protocols in individuals with stroke depends on multiple parameters including lesion size, location, and time since stroke onset.98-100 With respect to stimulation intensity and location, the working group considered the available evidence for both low-frequency (1-Hz rTMS) applied to contralesional M1 and high-frequency (5-Hz rTMS) applied over the ipsilesional cortex.
Numerous controlled trials have reported evidence supporting the use of low-frequency rTMS to improve motor function in acute/subacute40,101-103 and chronic stages of recovery.104-107 These findings have prompted a recent update of recommendations to Level A evidence (definite efficacy) for low-frequency rTMS over contralesional M1 for hand motor recovery at the postacute stage after stroke and a Level C rating (possible efficacy) at the chronic stage. 20 There is further evidence27,101,108 indicating that 1-Hz rTMS over the contralesional cortex produces greater improvement in motor function than ipsilesional 5-Hz rTMS; however, recent RCT data from the NICHE trial reported no additional improvement in function on the ARAT and Fugl-Meyer with low-frequency rTMS over contralesional M1 versus sham stimulation. 19 While it is important to note that this trial involved primarily chronic stroke patients and did not target the rTMS intervention to the recovery period with the most intensive dose of task-oriented rehabilitation, this negative evidence has impacted recommendations for the efficacy of low-frequency rTMS to contralesional M1 in chronic stroke. 20 Data supporting the safety and the feasibility of contralesional 1-Hz rTMS performed early after subcortical stroke are available 40 and, further, the effectiveness of this type of stimulation as an adjunct to outpatient rehabilitation in patients with mild-to-severe hand paresis has been established, with effects persisting at 1-month follow-up. 109
Although fewer studies have tested 5-Hz rTMS applied over ipsilesional M1, available data suggest that ipsilesional 5-Hz rTMS also can improve motor performance in the acute/subacute stage.101,102 However, only 3 controlled studies with more than 10 chronic patients have been conducted, with 2 reporting motor improvement107,110 and another showing no benefit. 111 As a result, there is presently Level B evidence (probably efficacy) for the use of high-frequency rTMS over ipsilesional M1 for hand motor recovery in the postacute stage, 20 while the evidence for 5-Hz rTMS applied over ipsilesional M1 for individuals in the chronic stages after stroke remains at Level C (possible efficacy). 42
Based on this evidence and considering our recommendation to target subacute patients with both subcortical and cortical stroke, in combination with evidence that all high-frequency rTMS (faciliatory) over the ipsilesional hemisphere has been associated with an increased risk of seizures poststroke, 112 the working group reached a consensus in favor of the use of 1-Hz rTMS (inhibitory) over contralesional M1.
Stimulation Intensity and Duration
Evidence for the optimal intensity and duration of rTMS in stroke patients is limited. Prior work suggests that reliable effects on cortical excitability are induced with higher intensities of stimulation, where stimulation trains are repeated. 42 Early studies reported that repeated consecutive rTMS sessions over 5 days in chronic patients were associated with beneficial effects on motor outcomes lasting up to 2 weeks. 106 More recently, 2 systematic reviews explicitly tested session-number dependent effects of rTMS on recovery of dexterity poststroke and showed a maximal therapeutic effect for 5 sessions, with increases beyond 5 sessions showing no incremental benefits. 94
Although numerous studies have evaluated the effects of the intensity and duration of 1-Hz rTMS on cortical motor excitability, results have been highly variable.113-116 One study systematically varied 1-Hz rTMS stimulus intensities and duration to compare dose responses within subjects and showed that, while suprathreshold rTMS at 1 Hz applied for at least 10 minutes or 20 minutes reduced resting MEP amplitude in healthy young adults, subthreshold rTMS at 1 Hz only significantly downregulated motor cortical excitability when applied for longer but not shorter durations. 117
The working group thus voted on parameters for stimulus intensity and duration for the 1-Hz rTMS protocol. Given the available data, consensus was reached in favor of a suprathreshold stimulus intensity of 120% resting motor threshold (RMT) during a once daily 30 minutes session for a total of 15 sessions over a maximum 3-week study period, to align with Canadian Best Practice recommendations for the number of therapy hours which are deemed to be minimally necessary to achieve an improvement with therapy alone. 57 However, it is important to note when generalizing across diverse practice settings that, as described, prior work suggests efficacy with a minimal therapy length of 5 sessions. 94 It is also important to note that any protocol using these rTMS parameters should include a blinded sham-controlled study arm, where patients would be randomized to receive either sham or rTMS treatment. While not part of the present consensus process, the working group agreed that for sham-stimulation the coil should be placed over the interhemispheric fissure at the vertex and stimulation performed at low intensity (10% RMT) to cause similar skin sensations as real stimulation but not induce currents in motor relevant areas.
Identification of M1
The working group considered 2 alternative methodologies for the identification of M1, specifically identifying the stimulation site by varying coil placement to determine the optimal MEP response in the paretic ECR 118 or identification of M1 via MRI-guided stereotaxic neuronavigation. Although many early TMS studies used MEP responses to identify the motor “hotspot,”118-120 recent work has demonstrated that the motor hot spot does not always correspond to the hand knob and M1 location in both healthy and patient populations. 121 In addition, the working group acknowledged the ongoing debate about whether M1 is necessarily always the most appropriate mechanism to target or whether facilitation of alternate regions may be indicated based in part on factors including severity of impairment. 122 The use of frameless stereotaxic neuronavigation systems, combined with individual MRI data, offer several advantages for improved targeting and stabilization of stimulus delivery.123,124 As a result, the stereotaxic identification of anatomical landmarks provides greater accuracy for the precise identification of small (mm scale) cortical targets than non-navigated techniques. 125 In addition, the optical-tracking system enables simultaneous tracking of both coil and participant head movement, greatly reducing trial-to-trial 126 and intersession variability.
Despite the clear advantages associated with the use of MRI-guided neuronavigation, particularly for multisite acquisition, the working group had significant concerns about the feasibility of recommending neuronavigation as a trial standard, particularly for sites in smaller centers with fewer resources. As a result, a moderated discussion was required to establish consensus. It was determined that trial protocols should make efforts to utilize MRI-guided neuronavigation to target M1 or an alternate stimulation target for populations where targeting M1 has been unsuccessful, to achieve reductions in intersubject variability between sessions and across sites. However, in the absence of stereotactic neuronavigation, use of single-pulse TMS-based hotspot localization using cranial 10 to 20 EEG landmarks may be useful to localize the most appropriate stimulation target.
Conclusion
The purpose of this consensus process was to develop recommendations for the delivery of rTMS as adjunct therapy in stroke rehabilitation clinical trials. These recommendations (Table 2) propose that clinical trials should recruit cortical and subcortical stroke patients between 2 weeks and 3 months after stroke who are appropriate candidates for upper extremity rehabilitation; that patients should be randomized to receive 1800 pulses of 1-Hz rTMS over contralesional M1 at 120% of RMT or sham stimulation, immediately followed by 60 minutes of GRASP therapy, for a total of 15 sessions over 3 weeks; that core primary outcomes are measures of impairment, function, and ability comprising the FMA, ARAT, and mRS and that subjective patient-centered (COPM, SIS) as well as real-world actigraphy as secondary outcomes and acquisition of CST biomarkers, including DTI and binary MEP parameters (MEP+/MEP−), should be included as part of any stroke rehabilitation trial protocol.
While these recommendations were based on best available evidence and existing consensus recommendations and examined in the context of the Canadian stroke rehabilitation care pathway, the protocol comprises 2 novel recommendations concerning the physiotherapy intervention that might be applied to all rehabilitation clinical trials. First, the dose of upper extremity rehabilitation follows best-practice recommendations of therapy hours which are deemed to be minimally necessary to achieve an improvement with therapy alone. Second, this is the first protocol to propose a controlled treatment with known effects (ie, GRASP) instead of usual and customary care which can vary between centers and therapists. Controlling dose and therapeutic intervention were deemed crucial for isolating the potential additive effects of rTMS.
These recommendations may impose challenges for implementation in practice (therapist commitment, patient retention). However, involving stakeholders in the consensus process was seen as strategy to mitigate these risks. Other aspects of this protocol selected to increase acceptance and facilitate implementation were the use of GRASP as the rehabilitation therapy, which has shown high levels of uptake among practitioners 64 and consideration of existing care pathways, accounting for typical transfer times from acute to rehabilitation hospitals, as well as average length of stay in in-patient rehabilitation.
Once efficacy of rTMS as an adjunctive therapy has been established in standardized clinical trials, future iterations will be poised to consider the role of therapy individualization. While it is unlikely that all patients will equally respond to the rTMS treatment recommended here, the available evidence for selecting patients based on individual factors such as lesion location or biomarkers is still very preliminary. Biomarkers were thus recommended as baseline measures in all patients to generate evidence from larger patient cohorts required to distinguish potential responders from nonresponders and develop personalized stimulation protocols.
Moving from proof-of-principle to large-scale clinical trials is a necessary next step toward recognition of rTMS as a standard therapeutic option for stroke rehabilitation. Building trial capacity in this field nationally and internationally will enable the translation of noninvasive brain stimulation technologies, from the laboratory to clinical practice for stroke rehabilitation.
Supplemental Material
sj-docx-1-nnr-10.1177_1545968320981960 – Supplemental material for Canadian Platform for Trials in Noninvasive Brain Stimulation (CanStim) Consensus Recommendations for Repetitive Transcranial Magnetic Stimulation in Upper Extremity Motor Stroke Rehabilitation Trials
Supplemental material, sj-docx-1-nnr-10.1177_1545968320981960 for Canadian Platform for Trials in Noninvasive Brain Stimulation (CanStim) Consensus Recommendations for Repetitive Transcranial Magnetic Stimulation in Upper Extremity Motor Stroke Rehabilitation Trials by Jodi D. Edwards, Sandra E. Black, Shaun Boe, Lara Boyd, Arthur Chaves, Robert Chen, Sean Dukelow, Joyce Fung, Adam Kirton, Jed Meltzer, Zahra Moussavi, Jason Neva, Caroline Paquette, Michelle Ploughman, Sepideh Pooyania, Tarek K. Rajji, Marc Roig, Francois Tremblay and Alexander Thiel in Neurorehabilitation and Neural Repair
Supplemental Material
sj-docx-2-nnr-10.1177_1545968320981960 – Supplemental material for Canadian Platform for Trials in Noninvasive Brain Stimulation (CanStim) Consensus Recommendations for Repetitive Transcranial Magnetic Stimulation in Upper Extremity Motor Stroke Rehabilitation Trials
Supplemental material, sj-docx-2-nnr-10.1177_1545968320981960 for Canadian Platform for Trials in Noninvasive Brain Stimulation (CanStim) Consensus Recommendations for Repetitive Transcranial Magnetic Stimulation in Upper Extremity Motor Stroke Rehabilitation Trials by Jodi D. Edwards, Sandra E. Black, Shaun Boe, Lara Boyd, Arthur Chaves, Robert Chen, Sean Dukelow, Joyce Fung, Adam Kirton, Jed Meltzer, Zahra Moussavi, Jason Neva, Caroline Paquette, Michelle Ploughman, Sepideh Pooyania, Tarek K. Rajji, Marc Roig, Francois Tremblay and Alexander Thiel in Neurorehabilitation and Neural Repair
Footnotes
Authors’ Note
Jason Neva is now affiliated with School of Kinesiology and Physical Activity Sciences, Université de Montréal. Arthur Chaves is now affiliated with Department of Cellular and Molecular Medicine, University of Ottawa.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The CanStim Consensus Conference was funded by a Collaborative Grant from the Canadian Stroke Trials for Optimized Results (CaSTOR) to CanStim co–principal investigators Dr Jodi Edwards and Dr Alexander Thiel.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.