
Abstract
Background
A comprehensive scale assessing motor coordination of multiple body segments was developed using a 3-phase content validation process. The Comprehensive Coordination Scale (CCS) evaluates motor coordination defined as the ability to produce context-dependent movements of multiple effectors in both spatial and temporal domains. The scale assesses motor coordination in individuals with neurological injuries at 2 levels of movement description: the motor performance level describes end point movements (ie, hand, foot), and the movement quality level describes limb joints/trunk movements contributing to end point movement.
Objective
To determine measurement properties of the scale in people with chronic stroke.
Methods
Standardized approaches determined the internal consistency (factor loadings), intrarater and interrater reliability (interclass correlation coefficient), measurement error (SEM; minimal detectable change [MDC]), construct validity, and interpretability (ie, ceiling and floor effects) of the CCS.
Results
Data from 30 patients with chronic stroke were used for the analysis. The internal consistency of the scale was high (0.94), and the scale consisted of separate factors characterizing end point motor performance and movement quality. Intrarater (intraclass correlation coefficient [ICC] = 0.97-0.97) and interrater (ICC=0.76-0.98) reliability of the whole scale and subscales were good to excellent. The CCS had an SEM of 1.80 points (total score = 69 points) and an MDC95 of 4.98 points. The CCS total score was related to Fugl-Meyer Assessment total and motor scores and had no ceiling or floor effects.
Conclusions
The CCS scale has strong measurement properties and may be a useful measure of spatial and temporal coordination deficits in chronic stroke survivors.
Introduction
Stroke is a leading cause of disability worldwide. 1 Motor impairments are common following stroke 2 and may cause limitations in the performance of activities of daily living, reduced participation, and decreased quality of life.3,4 One important component of normal movement affected by stroke is the ability to perform coordinated movements. 5 However, the construct of coordination is poorly defined and poorly measured in clinical assessments.
Motor coordination is a process of organizing movements of different joints, body segments, or limbs in both spatial and temporal domains. 6 Coordination is a multidimensional construct 7 that can be assessed kinematically at 2 levels of movement description: the motor performance level and the movement quality level. 8 The motor performance level describes the characteristics of the end point movement such as velocity, smoothness, and accuracy. The movement quality level describes joint/segment rotations and displacements and can be used to quantify motor compensations.
Current clinical assessments of coordination primarily assess end point performance, often only by evaluating the time of execution. Assessment of variables describing temporal and spatial aspects of coordination is not routinely done. Instead, the ability to complete different tasks is assessed with the implicit assumption that some type of interjoint or intersegment coordination is needed to accomplish the task. Most scales also pay little or no attention to movement quality or the extent to which the task performance deviates from typical movement patterns observed in healthy individuals. 9 The description of end point variables is important to characterize task completion but is not sufficient to distinguish motor recovery from compensations. More detailed information about compensatory movements and atypical strategies used to perform a task is essential to guide clinicians in therapeutic goal setting for neurological patients. 10
We addressed this gap by developing a new, objective scale to quantify sensorimotor coordination of the limbs and trunk at the 2 levels of movement description described above. 11 The Comprehensive Coordination Scale (CCS; see the appendix in Alouche et al 11 ) consists of 6 tests used in either clinical practice or research to assess complementary aspects of motor coordination of the trunk, upper limb (UL), lower limb (LL), or combinations of them. These are as follows: Finger-To-Nose (FTN), 12 Arm-Trunk Coordination (ATC), 13 Finger Opposition (FOT), 14 Upper Limb Interlimb Coordination (ILC2), 15 Lower Extremity Motor Coordination (LEMOCOT), 16 and Four-limb Interlimb Coordination (ILC4). 17 The CCS score can be used in adults with neurological disorders to characterize multibody segment coordination or can be broken down into 4 subscales to assess UL, LL, or unilateral or bilateral coordination separately.
The new scale goes beyond current clinical coordination measures by assessing important aspects of movement performance and quality in addition to the traditional measures of time or ratings of task completion. In keeping with clinical constraints on instrumented kinematic analysis, movement performance and quality are assessed using observational kinematics. Observational kinematics, the process by which a therapist visually judges the quality of movement, has moderate to high accuracy for judgments of end point speed, smoothness, and straightness. 18
The CCS previously underwent a 3-phase content validation supporting its importance, level of comprehension and feasibility in identifying and quantifying coordination of movements made by individuals with neurological deficits in a clinical setting. 11 The next step in the validation process of the new scale is the determination of the internal consistency (factor loadings), intrarater and interrater reliability (interclass correlation coefficient), measurement error (SEM; minimal detectable change, [MDC]), construct validity, and interpretability (ie, ceiling and floor effects) in individuals with stroke. We hypothesized that the CCS would have good measurement properties. Because it was expected that clinicians may be interested in using the scale not only to characterize global coordination deficits, but also to identify localized deficits, we also investigated the psychometric properties of the 4 CCS subscales.
Methods
Participants
A total of 30 participants with chronic stroke were recruited from the Jewish Rehabilitation Hospital (JRH) in Laval, Canada, between April and December 2019. Participants were included if they were 18 years or older, in the chronic stage of stroke (>6 months poststroke), and were able to walk independently with or without mobility aids. Individuals with any type of stroke, level of sensorimotor severity, and chronicity were included. Potential participants were excluded if they had severe cognitive impairments, language impairments, or apraxia as measured by common clinical scales or other musculoskeletal or neurological injuries that may have interfered with task performance. The study was approved by the Research Ethics Board of the Centre for Interdisciplinary Research in Rehabilitation according to the Declaration of Helsinki, and all participants signed approved informed consent forms prior to participation.
Procedure
Each individual participated in 2 testing sessions (T1 and T2) held at least 2 days apart. The first session included clinical assessments and the CCS. Two assessors evaluated performance on the CCS. The primary assessor administered the test while the secondary assessor observed. Both assessors scored the test simultaneously and independently. The second session consisted of assessment and scoring of the CCS only by the primary assessor. The primary assessor was an occupational therapist with 30 years of clinical experience. The secondary assessors were physical and occupational therapists with 4 to 28 years of experience in stroke rehabilitation.
Clinical Assessments
A battery of standardized assessments was used to evaluate UL and LL motor impairments and activity limitations. UL motor impairment was assessed using the Fugl-Meyer Assessment of the Upper Extremity (FMA-UL), 19 prehension, and pinch strength. Unilateral gross manual dexterity (Activity domain of the International Classification of Functioning) was assessed with the Box and Blocks Test (BBT). 20 LL motor impairment was assessed with the FMA Lower Extremity (FMA-LL), and activity was assessed with the 10-m Walk Test (10mWT). 21
FMA is a stroke-specific, performance-based impairment index. It is composed of 5 domains: motor function, sensory function, balance, passive joint range of motion, and joint pain, scored on 3-point ordinal scales ranging from 0 to 2, for a maximal total score of 212 points for all 5 domains. The maximal score for motor functioning is 66 points for the FMA-UL and 34 points for the FMA-LL, with higher scores indicating better motor performance. The FMA (UL + LL) total motor score has excellent interrater reliability (intraclass correlation coefficient [ICC] = 0.97). 22 The motor score is also strongly correlated with the Action Research Arm Test (r = 0.93) and BBT (r = 0.92). 22
Prehension and pinch strength are commonly measured in clinical practice and research and have been related to UL function.23-25 Manual grip and palmar pinch force were measured using hand and pinch dynamometers and recorded in kilograms. The average of 3 trials was used. Both grip and pinch strength have excellent test-retest reliability in people with chronic stroke (ICC = 0.93-0.99). 26 Intrarater reliability for grip strength is excellent (ICC = 0.94-0.99) and good for pinch strength (ICC = 0.83-0.89). 27 Strong correlations were found between grip strength and FMA (r = 0.84), Test Évaluant la Performance des Membres supérieurs des Personnes âgées (r = 0.88), BBT (r = 0.87), and FTN (r = 0.79). 24 Values obtained were expressed as raw data and normalized to age and sex norms for dominant and nondominant arms.20,28
The BBT is used to measure unilateral manual dexterity. The task is to transfer wooden cubes from one side of a box to the other in 1 minute. A higher number of cubes transferred is attributed to better dexterity. In individuals with stroke, the BBT demonstrates excellent test-retest (ICC = 0.93-0.98) 26 and interrater (ICC = 0.99) reliability and is strongly correlated with the Action Research Arm Test (r = 0.95), FMA (r = 0.92), and Hemispheric Stroke Scale (r = −0.67). 22 Scores obtained were expressed as raw data and also normalized to age and sex norms for each side of the body. 20
For prehension, pinch, and BBT evaluations, values were obtained for each arm. The unilateral values are relevant to evaluate patients with one side of the body more affected than the other (ie, stroke), whereas the summed bilateral values are relevant to evaluate patients with both sides affected (ie, multiple sclerosis, traumatic brain injury, etc).
The 10mWT is a common clinical measure used to assess comfortable or maximal gait speed. Participants walked 10 m in a straight line at a comfortable speed, and the results were recorded in seconds. The 10mWT has good test-retest reliability (ICC = 0.87-0.88) and excellent intrarater reliability (ICC = 0.95-0.99) in individuals with chronic stroke. 29 Scores are strongly correlated with the Barthel Index (r = 0.78) 21 , the 6-Minute Walk Test (r = 0.94), 30 and the Timed Up and Go (r = −0.84) 31 in individuals with chronic stroke.
The CCS includes 13 items distributed across the 6 tests: FTN, ATC, FOT, ILC2, LEMOCOT, and ILC4. Each item is scored on a 4-point scale ranging from 0 (impaired coordination) to 3 (normal coordination). In all, 10 items are scored separately for each side of the body, and in 3 items, bilateral activity is scored, for a total of 69 points. Higher scores indicate better motor coordination. The scoring of the each CCS subscale is as follows: (1) The CCS-UL includes scores of FTN, ATC, FOT, and ILC2 for a total of 54 points; (2) The CCS-LL consists of the LEMOCOT score for a total of 12 points; (3) The CCS-Unilateral includes scores from FTN, ATC, FOT, and LEMOCOT for a total of 30 points and is assessed separately for the right and left limbs; and (4) The CCS-Bilateral comprises scores of ILC2 and ILC4 for a total of 9 points.
Statistical Analysis
Analyses were performed with SPSS version 27.0 (SPSS Inc, Chicago, IL) and R version 4.0.1. Data normality was determined using Shapiro-Wilk tests.
Internal Consistency
Because the CSS is composed of a compilation of heterogeneous but similar items, the number of factors measured by the 13 scale items was analyzed by principle component analysis. Factors with eigenvalues >1 were identified. Then, exploratory factor analysis was used to identify factor groupings without a priori expectations about the number of factors. This analysis explained the variance between a smaller set of latent variables using 2 factors as follows: Factor analysis (r = corMatrix; nfactors = 2; rotate = “varimax”; factoring method = “principle axis”). The composite reliability test was used to investigate the internal consistency by evaluating the individual item reliability of each latent variable. 32 Confirmatory factor analysis was used to generate the standardized factors.
Reliability
Intrarater and interrater reliability 33 were evaluated with ICCs (2-way random effects, absolute agreement, and multiple raters), with 95% CIs. Values <0.5, between 0.5 and 0.75, between 0.76 and 0.89, and >0.9 indicate poor, moderate, good, and excellent reliability, respectively. 34
Measurement Error
SEM and MDC were determined for the CCS score and CCS subscale scores. SEM was calculated based on the SD of the sample and the reliability of measurement:
Construct Validity
To assess the construct validity, the scores of the CCS and the 4 CCS subscales (UL, LL, Unilateral, Bilateral) were correlated with clinical assessment scores using the Spearman ρ, where values <0.3, between 0.30 and 0.59, and ≥0.6 are considered as weak, moderate, and strong. 38
Interpretability
Interpretability was assessed by identifying ceiling and floor effects defined as the number of minimal or maximal values that exceeded 15% of the total number of values. 39
Results
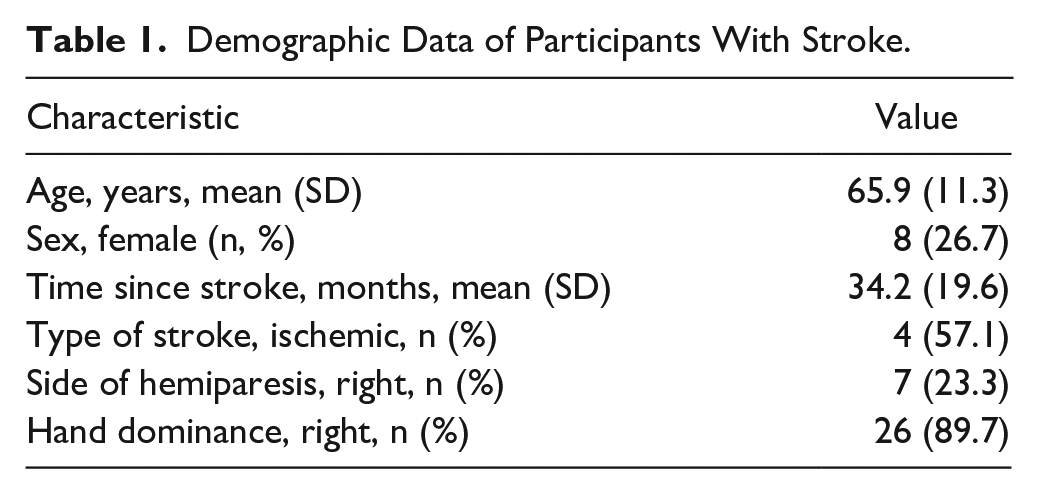
Participants ranged in age from 40 to 88 years old (mean ± SD: 65.9 ± 11.3 years) and were in the chronic phase of stroke (Table 1). They had severe to mild UL and LL impairment as reflected in impairment and activity clinical scores (Table 2). FMA motor scores (UL + LL; 100 points) ranged from 32 to 99 points. The time to complete the CCS was less than 15 minutes, regardless of the level of sensorimotor impairment of the patient.
Demographic Data of Participants With Stroke.
Scores, Mean (SD), of Clinical Tests and Normalized Scores Based on Norm-Referenced Values for Tests of Prehension and Pinch Force and for the BBT.
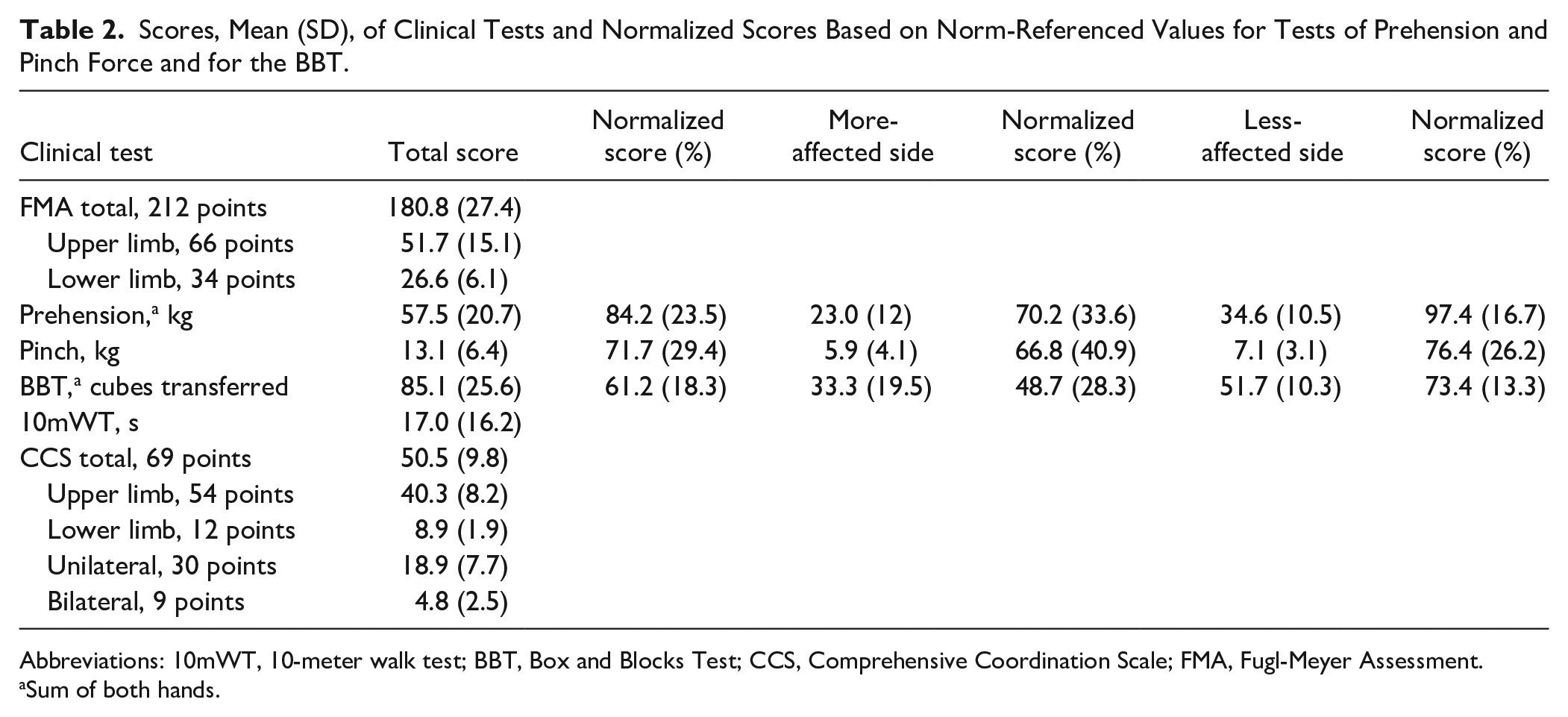
Abbreviations: 10mWT, 10-meter walk test; BBT, Box and Blocks Test; CCS, Comprehensive Coordination Scale; FMA, Fugl-Meyer Assessment.
Sum of both hands.
Internal Consistency
Factor analysis of the whole scale revealed 2 factors with eigenvalues greater than 1 (factor 1 [PA1], eigenvalue = 8; factor 2 [PA2], eigenvalue = 5) that explained 99% of the variance. The factor loadings for all variables for each factor are shown in Table 3 and for those of PA1 and PA2 are shown in Figure 1. The composite reliability value was 0.938, which indicates excellent internal consistency.
Factor Loadings of Each of the Components (PA1 and PA2) of the CCS. a
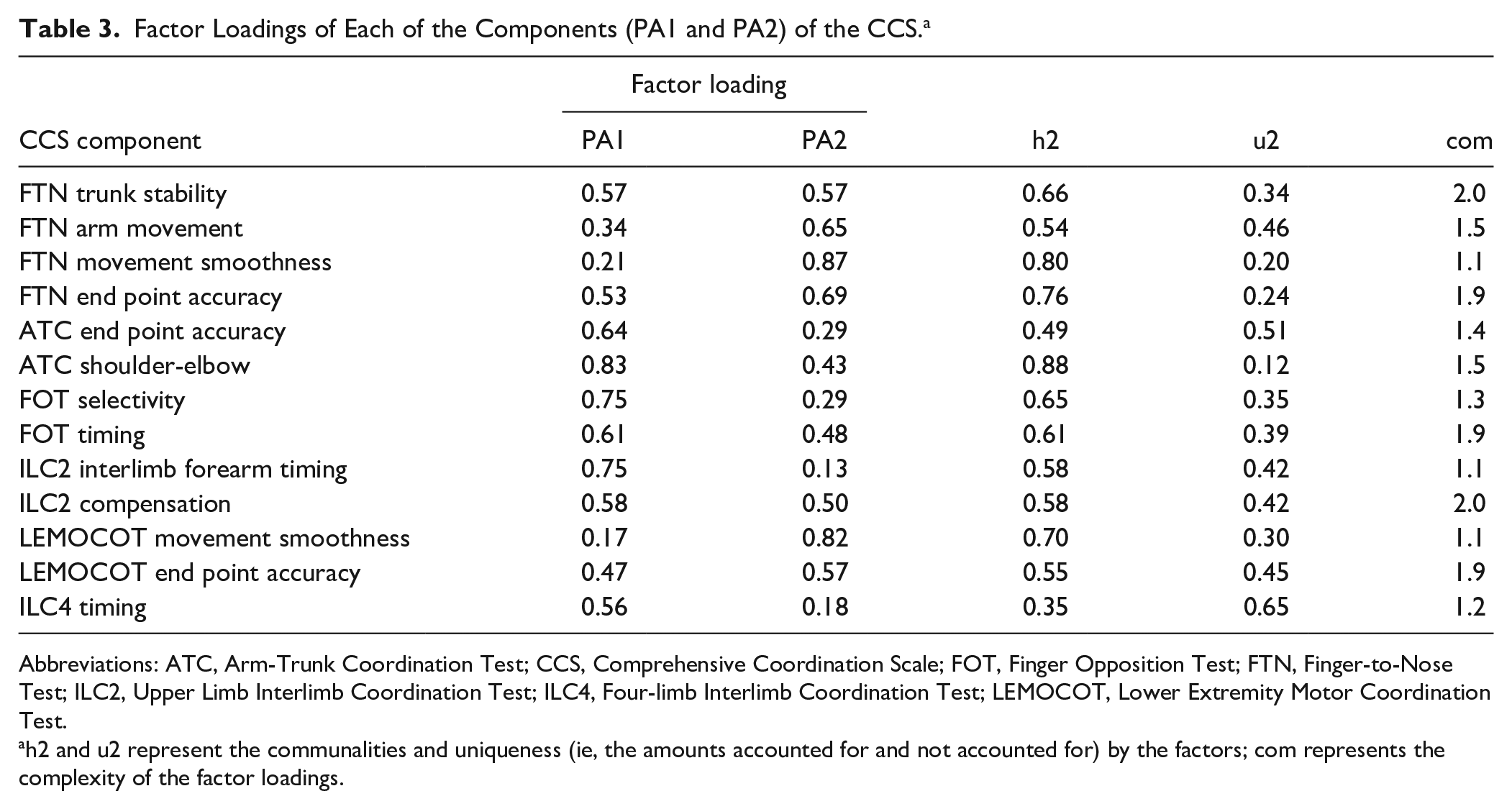
Abbreviations: ATC, Arm-Trunk Coordination Test; CCS, Comprehensive Coordination Scale; FOT, Finger Opposition Test; FTN, Finger-to-Nose Test; ILC2, Upper Limb Interlimb Coordination Test; ILC4, Four-limb Interlimb Coordination Test; LEMOCOT, Lower Extremity Motor Coordination Test.
h2 and u2 represent the communalities and uniqueness (ie, the amounts accounted for and not accounted for) by the factors; com represents the complexity of the factor loadings.
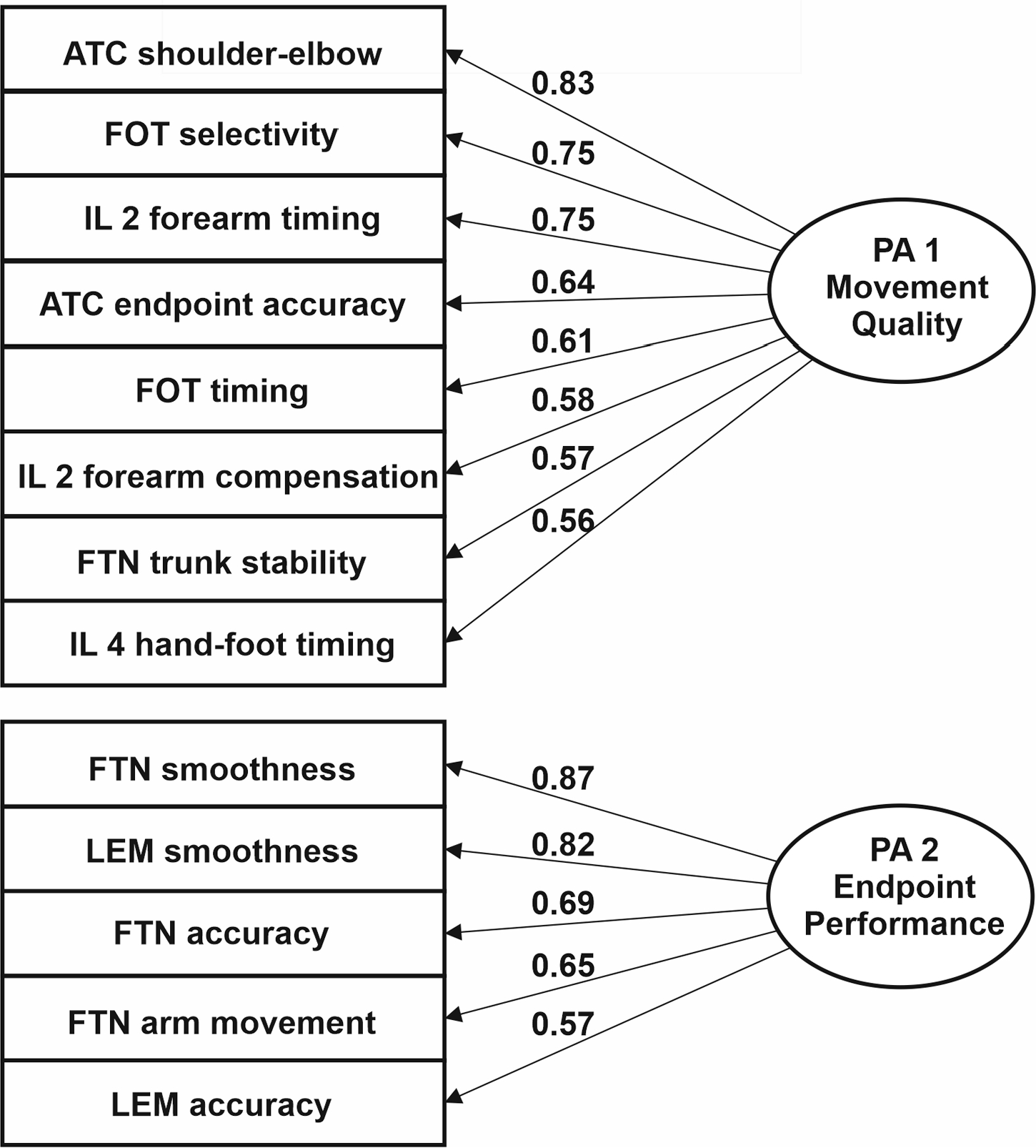
Comprehensive Coordination Scale (CCS) factor analysis.
Confirmatory factor analysis indicated that PA1 included mainly movement quality variables, such as shoulder and elbow movement, FOT, trunk movement, and timing. PA2 included predominantly measures of end point motor performance (ie, smoothness and accuracy).
Reliability
CCS scores ranged from 25 to 68 points (Table 2). It had excellent intrarater (ICC = 0.97; 95% CI: 0.93-0.98) and interrater reliability (ICC = 0.98, 95% CI: 0.95-0.99; Figure 2).
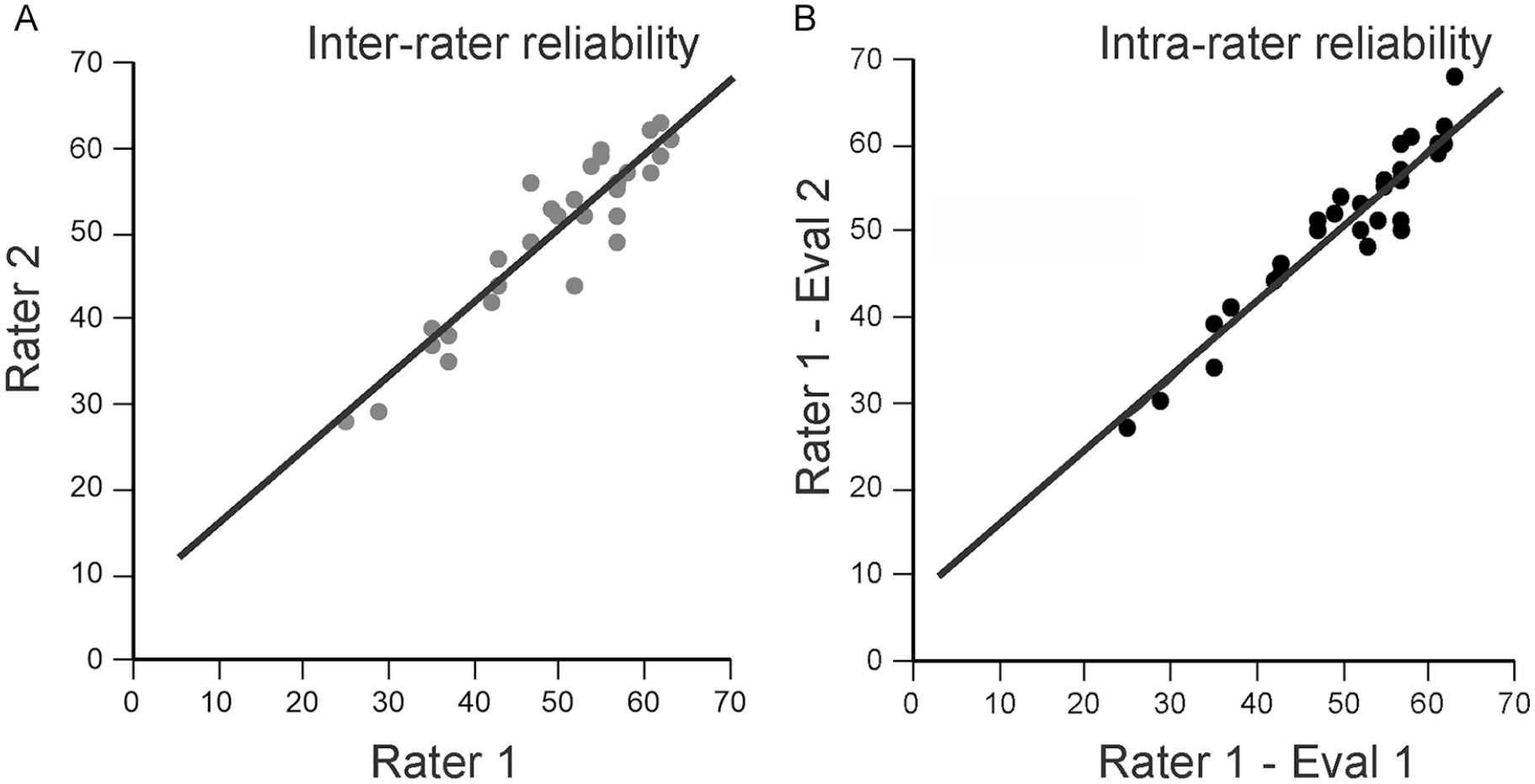
Interrater (A) and intrarater (B) reliability of the Comprehensive Coordination Scale.
Scores on the CCS-UL subscale ranged from 18 to 54 points. The CCS-UL subscale had excellent intrarater (ICC = 0.96; 95% CI: 0.92-0.98) and interrater reliability (ICC = 0.96; 95% CI: 0.91-0.98). For the CCS-LL subscale, scores ranged from 4 to 12 points. The subscale had good intrarater (ICC = 0.79; 95% CI: 0.36-0.92) and interrater (ICC = 0.76; 95% CI: 0.25-0.9) reliability. CCS-Unilateral scores ranged from 0 to 30 points. The subscale had excellent intrarater (ICC = 0.98; 95% CI: 0.96-0.99) and interrater (ICC = 0.99; 95% CI: 0.97-0.99) reliability. The CCS-Bilateral scores ranged from 0 to 8 points. The subscale had excellent intrarater (ICC = 0.95; 95% CI: 0.89-0.97) and interrater (ICC = 0.95; 95% CI: 0.89-0.98) reliability.
Measurement Error
The CCS SEM was 1.80 points, and the MDC95 was 4.98 points (Table 4). The SEM and MDC95 values for the CCS, the CCS-UL, CCS-Unilateral, and CCS-Bilateral were less than 17%. Only the CCS-LL had an MDC95 greater than 17%. For the CCS and all subscales, the SEM was smaller than the MDC95.
SEM and MDC95 Scores for the CCS-Total and the CCS-UL, CCS-LL, CCS-Unilateral, and CCS-Bilateral Subscales. a
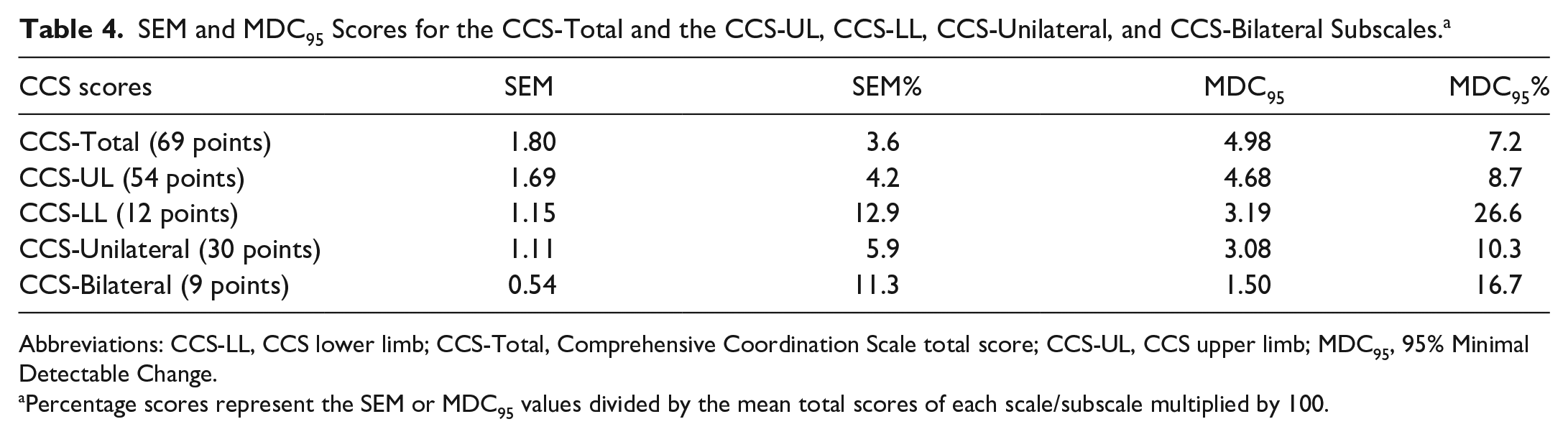
Abbreviations: CCS-LL, CCS lower limb; CCS-Total, Comprehensive Coordination Scale total score; CCS-UL, CCS upper limb; MDC95, 95% Minimal Detectable Change.
Percentage scores represent the SEM or MDC95 values divided by the mean total scores of each scale/subscale multiplied by 100.
Construct Validity
The CCS score was moderately to strongly correlated with measures of impairment (Table 5). In particular, it was strongly related to the FMA total score and the FMA total motor scores (Figure 3). For the subscales, CCS-UL and CCS-Unilateral scores were moderately to strongly correlated with all measures of UL and LL impairment and activity limitations. The CCS-LL subscale was moderately correlated with measures of LL impairment and UL activity limitations. The CCS-Bilateral subscale was moderately correlated with UL activity limitation measures (Table 5).
Spearman ρ Correlations and Associated Significance Values (P) Between CCS-Total and CCS Subscale Scores a and Clinical Assessments.
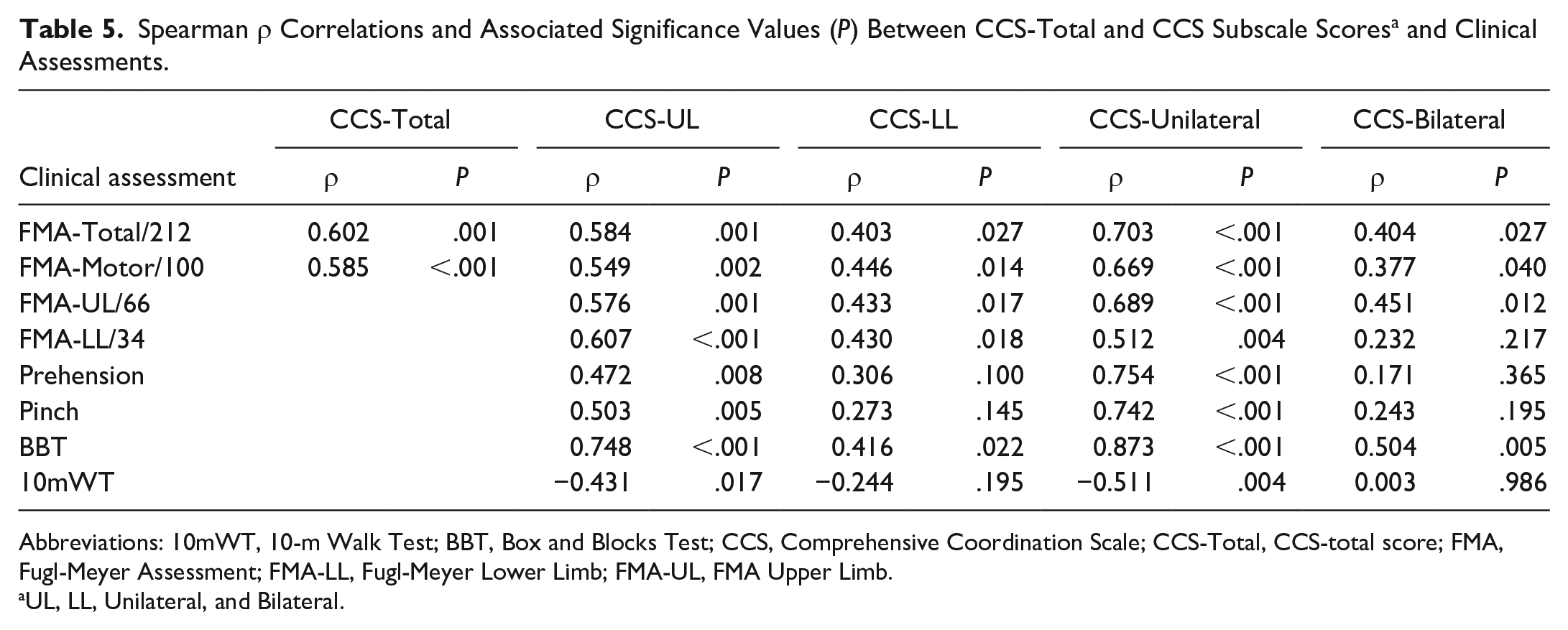
Abbreviations: 10mWT, 10-m Walk Test; BBT, Box and Blocks Test; CCS, Comprehensive Coordination Scale; CCS-Total, CCS-total score; FMA, Fugl-Meyer Assessment; FMA-LL, Fugl-Meyer Lower Limb; FMA-UL, FMA Upper Limb.
UL, LL, Unilateral, and Bilateral.
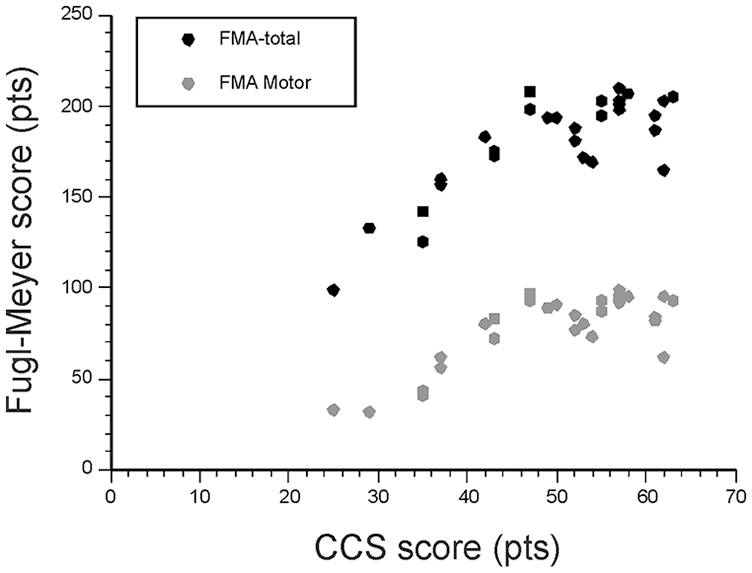
Correlations between the score of the Comprehensive Coordination Scale (CCS) and the total Fugl-Meyer Assessment (FMA) scores of the upper and lower limbs (FMA-total) and the FMA motor scores of the upper and lower limbs (FMA-motor).
Interpretability
There were no floor or ceiling effects for the CCS and CCS-Bilateral subscale. For the CCS-UL and CCS-LL subscales, 3.3% and 6.7% of participants reached the maximal score, respectively. In all, 10% of participants scored 0 or 30 on the CCS-Unilateral subscale.
Discussion
The CCS was developed to quantify sensorimotor coordination at 2 levels of movement description in a clinical setting: the motor performance level and the movement quality level. Following a 3-phase content validation, this study aimed to assess the measurement properties of the new scale in people who have had a stroke. The results provide evidence that the CCS is a reliable and valid measure of sensorimotor coordination in people with chronic stroke.
CCS had excellent internal consistency. The results (99% of the variance) show that all the items (13) of the scale measure the global construct of coordination. The factor analysis was used to assess the content validity and showed that coordination can be defined by 2 measurable components. The first component included 8 scale items related to movement quality variables such as shoulder, elbow, and trunk displacements as well as timing or synchronicity of movements. The second component was related to motor performance variables of the end point such as smoothness and accuracy. Thus, CCS goes beyond current clinical scales of coordination by providing a more complete characterization of the spatial and temporal domains underlying problems at both motor performance and movement quality levels in the production of coordinated movement. It provides new information that can be used by therapists to design treatments targeting the remediation of underlying coordination deficits.
The CCS score as well as scores of 3 of the subscales (CCS-UL, CCS-Unilateral, CCS-Bilateral) showed excellent intrarater and interrater reliability, with high ICC values (>0.96). However, the ICC values for the CCS-LL were relatively lower (0.79 and 0.76) but still within an acceptable range. The poorer values for the CCS-LL subscale may be related to the smaller sample size used in this study because the reliability of the original version of LEMOCOT was 0.83 to 0.88 using a sample of 144 individuals with stroke. 16 Nevertheless, our results suggest that scores on the CCS and subscales obtained from multiple raters and sessions can be considered representative of the actual motor behavior related to coordination of different body segments.
The SEM is relevant when monitoring the health status of patients and when deciding whether changes exceed the measurement error. SEM is a distribution-based measure that provides a value in the same units as the scale. A small error level is needed to distinguish clinical change from measurement error. 39 The SEM% is independent of the scale units and, therefore, easier to interpret. 37 The SEM% values were small, implying that the CCS and subscales are sensitive and have low measurement errors. Based on SEM values, the MDC values were computed. The MDC is defined as the smallest change in score that can be detected by the instrument that is not a result of the measurement error. 35 Differences in scores that are larger than the MDC95 value can be attributed to real change in an individual’s performance at a 95% confidence level. 40
Construct validity assesses the extent to which scores on a particular instrument relate to other measures. 39 Good construct validity of the CCS was demonstrated by high values for most of the tested correlations between CCS total score and scores of CCS subscales with clinical assessments of motor impairments and UL activity limitations. However, no correlation was found between CCS-LL and the 10mWT. The 10mWT assesses gait speed at the activity level of the International Classification of Functioning. 1 Although coordination is required for locomotion, different body functions like joint mobility, muscle tone, and balance may also affect gait speed. The relationship between CCS-LL and gait speed could be evaluated in a larger cohort of patients in a future study.
The CCS-Bilateral subscale was moderately associated with the BBT but not with prehension or pinch strength. A possible explanation may be that the CCS-Bilateral score consists of 2 interlimb coordination tests. These tests require the performance of coordinated limb movements in a synchronous manner in both space and time but are not related to strength. It is likely that higher correlations between the CCS-Bilateral subscale and clinical measures may be found in individuals with bilateral impairment caused by other neurological conditions such as Parkinson disease and multiple sclerosis.
Finally, in terms of interpretability, we found that despite the wide range of sensorimotor impairment in the subject cohort measured by FMA motor scores (UL + LL), no floor or ceiling effects were found for the CCS and subscales. This suggests that the CCS and its subscales can be used to detect changes in individuals with mild to severe stroke symptoms.
Limitations
Although our sample size was smaller than that generally recommended for reliability studies, 41 we obtained a high power for the different tests with 30 individuals. This suggests that increasing the size of the sample would not have led to substantially stronger results. 42
Our study evaluated the validity and reliability of the CCS only for stroke survivors who were in the chronic stage. However, impairments in coordination may be different for individuals with more acute stroke or for individuals with ataxia or other neurological conditions and age ranges. It is also unknown whether or not the CCS may be able to distinguish between different neurological impairments. Participants with severe cognitive impairments, severe aphasia, or apraxia were excluded from the study, limiting the generalizability of the results to the entire adult stroke population. Whereas the CCS can be administered in less than 15 minutes and requires minimal material, the feasibility of administering the CCS in a busy clinical environment has not been evaluated. Finally, this study did not establish the responsiveness of the CCS or the minimal clinically important difference.
Clinical Implications
The CCS is a valid and reliable clinical tool that provides clinicians with the capacity to measure motor coordination of multiple body segments. It is the only clinical measure that provides a comprehensive assessment of both temporal and spatial aspects of coordination. It also distinguishes between coordination deficits at the end point (ie, hand, foot) level to quantify motor performance as well as at the arm/trunk/leg joints underlying the end point movement in order to quantify the quality of movement and movement compensations. The use of visual observation instead of complex and costly motion analysis equipment to analyze movement makes this scale clinically accessible and easy to use. Future studies may reevaluate the psychometric properties of the CCS-LL subscale in individuals with different neurological impairments, in acute and subacute stroke survivors, or in a larger sample size of chronic stroke survivors. An assessment of the responsiveness of the CCS and the 4 subscales is also needed to determine whether changes over time can be detected.
Footnotes
Acknowledgements
The authors wish to thank all the participants who volunteered for this study and Rejean Prevost for his assistance with clinical assessment and statistical analysis and for his feedback on the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by funding from Canada Research Chairs (MFL). MD was supported by the Fonds de la Recherche du Québec en Santé. SRA was funded by Grant #2018/04544-9, Sao Paulo Research Foundation (FAPESP), Brazil.