
Abstract
In motor skill learning, larger doses of practice lead to greater efficacy of practice, lower efficiency of practice, and better long-term retention. Whether such learning principles apply to motor practice after stroke is unclear. Here, we developed novel mixed-effects models of the change in the perceived quality of arm movements during and following task practice. The models were fitted to data from a recent randomized controlled trial of the effect of dose of task practice in chronic stroke. Analysis of the models’ learning and retention rates demonstrated an increase in efficacy of practice with greater doses, a decrease in efficiency of practice with both additional dosages and additional bouts of training, and fast initial decay following practice. Two additional effects modulated retention: a positive “self-practice” effect, and a negative effect of dose. Our results further suggest that for patients with sufficient arm use post-practice, self-practice will further improve use.
Introduction
When individuals with or without a neurologic injury practice motor tasks, their ability to perform these tasks improves through skill acquisition.1,2 In individuals with chronic stroke, appropriate task practice can thus lead to improved arm and hand functions to perform daily activities. 3 However, the neural damage often sets a limit on how much motor impairments, such as weakness, can be reduced in the chronic phase. Therefore, functional improvements in the chronic phase is thought to be due to the learning of alternative strategies, often termed compensatory movements, in which the individual uses different joints and muscles from those originally used before the injury to achieve a movement goal.4,5
Extensive behavioral research in motor skill learning 6 has shown that (1) increasing the amount of training increases efficacy (“practice makes perfect”), (2) increasing the amount and duration of training decreases efficiency (“the diminishing returns of practice” 7 ), and (3) increasing the amount of training improves retention following practice.8,9 However, to what extent these principles translate to motor learning in individuals poststroke remains unclear for 3 reasons. First, the effect of increasing the amount of practice on clinical outcomes is controversial. While our recent Dose Optimization for Stroke Evaluation (DOSE) trial, 10 recent high dosage trials,11,12 and meta-analyses3,13 suggest that high doses lead to greater gains, a recent phase II clinical trial showed no effect of dose on arm function. 14 Second, although studies of task-specific practice after stroke show that most gains in movement performance are achieved in the initial sessions,15,16 the changes of efficiency of training with both additional dosages and additional bouts of training on clinical outcomes are unknown. Third, previous studies have shown that retention following task practice in stroke survivors is highly variable, but the reasons for such variability are unclear. Whereas some studies have shown decay of the gains postpractice, 17 as least for subgroups of patients, 18 others have shown that the gains can be maintained after practice,15,19 yet others have shown that the gains can even further increase following practice,12,20 possibly through “self-practice” if arm use is sufficient.18,21,22
Here, we analyzed the changes in the Quality of Movement subscale of the Motor Activity Log (henceforth the MAL) during the DOSE trial, in which participants with chronic stroke were randomized into 4 dose groups total doses (0, 15, 30, and 60 hours) that were equally distributed over the 3 practice bouts. The MAL, which measures the participant’s perception of their amount and quality of movements by asking them to recall and rate the quality of movement of the paretic arm for 28 activities of daily living, was collected in 14 longitudinal assessments before and after practice in each of the three 1-week training bouts and then monthly for 6 months following the last training bout.
Using linear models, we previously showed that the changes in MAL due to practice in DOSE was dose-dependent. 10 While such “fixed” regression models can predict response to either interventions or recovery,10,14,16 they cannot simultaneously account for both the changes in outcomes during task-specific practice (when an increase in performance is expected) and outside of training (when either a decrease in performance due to forgetting or an increase in performance due to self-practice are possible) for individual stroke survivors. We need methods that can model both increases and decreases in outcomes during and outside of supervised practice sessions. These models need to incorporate covariates of interest such as the dose and timing of practice sessions. Finally, because stroke is characterized by considerable between-subject variability in lesions, recovery, and responsiveness to therapy, 23 these models need to incorporate specific random effects to model individual differences in change of performance.24-26
We therefore developed novel mixed-effect dynamical models to model the changes in MAL in the DOSE trial. Development of these models was inspired by previous models in motor learning and adaptation,27,35 in which increases in motor memory are modulated by “learning rate” parameters, and decays in memory are modulated by “retention rate” parameters. 1* The models allow us to test statistically the efficacy, efficiency, and retention of task practice. Specifically, we modeled the learning and retention rates as linear models of both experimental variables, such as the dose of task practice, the bout of practice, and the time post-practice, as well as participant covariates, such as performance pre- and postpractice. Testing for significance of these model parameters allowed us to test the following hypotheses, derived from behavioral motor learning and stroke research, referenced above: (1) the efficacy of task practice will increase following larger doses of task practice; (2) the efficiency of task practice will decrease with larger doses of practice; (3) the efficiency of task practice will decrease with additional bouts of practice; (4) retention will improve with larger dosages; (5) retention will show an initial fast decay followed by a slower decay; and (6) the level of performance after supervised task practice will modulate retention through “self-practice.”
Methods
Participants
Data from 41 participants, mild-to-moderately impaired chronically after stroke (onset at least 5 months prior to inclusion; upper extremity Fugl-Meyer motor [UEFM] score in the 19-60 range out of 66), who completed the DOSE trial were analyzed. Detailed participant characteristics as well as inclusion and exclusion criteria are described in Winstein et al. 10 Ten participants were assigned to the 0-, 15-, and 30-hour dosages, and 11 participants to the 60-hour dose. Participants signed an informed consent, and the study was approved by the Institutional Review Board of the University of Southern California.
The DOSE Clinical Trial Design Overview
Each of the 4 dosages were distributed over 3 week-long practice bouts each separated by 1 month, in a “train-wait-train” paradigm (Figure 1A). The intervention was based on the Accelerated Skill Acquisition Program (ASAP),19,36 which notably includes elements of purposeful and skilled movement execution, including challenging and progressive task practice. The participants underwent 14 clinical assessments, each including the MAL, the Wolf Motor Function Test (WMFT), and an arm reach performance and choice test, the Bilateral Arm Reaching test (BART). 37 The assessments were given (1) twice in the month before each practice bout with a 2-week interval to assess baseline values; (2) for each of the three 1-week practice bouts, in the morning of the first day of practice and within 3 days following that practice bout; and (3) monthly for 6 months following the last practice bout (see Figure 1A). 10
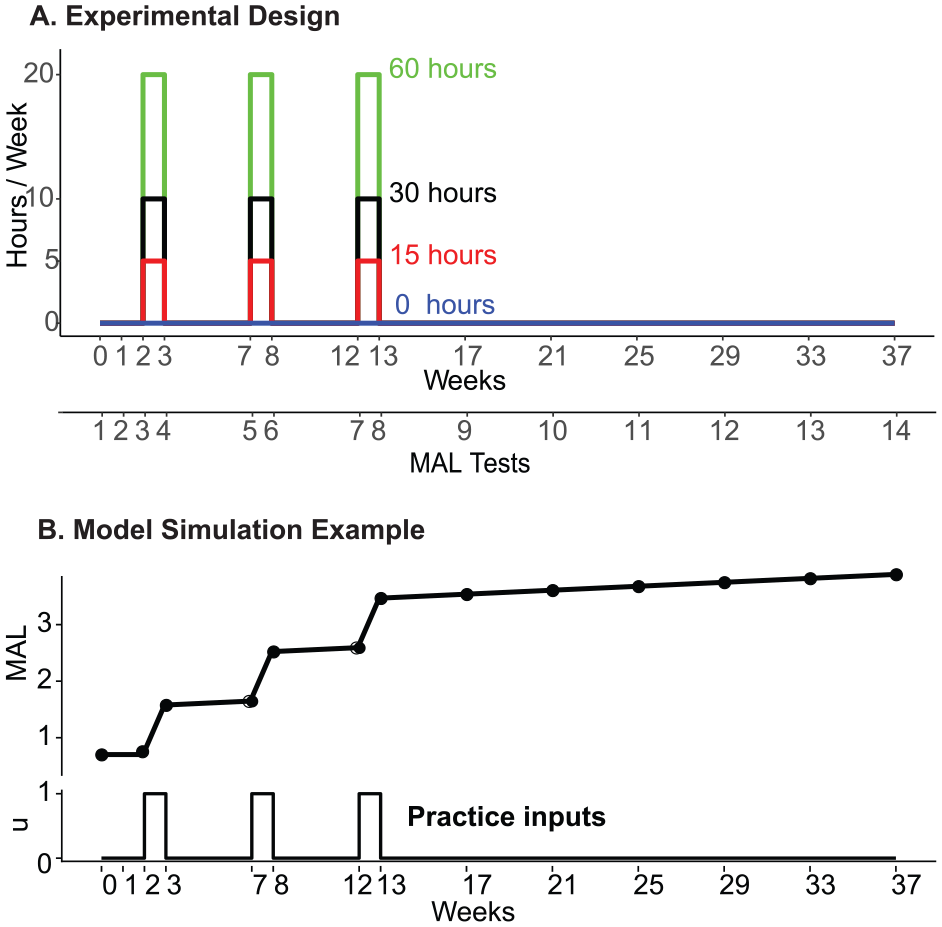
Schematics of the schedules of task practice and MAL assessments in DOSE. (A) Timing of motor practice based on the train-wait-train paradigm, in which three 1-week bouts of practice are separated by 1-month “wait” periods. (B) Example of a simulation showing the changes in perceived quality of arm movements in the train-wait-train paradigm modeled with a piece-wise linear model with a positive retention parameter (see Equation 1). The black dots show the timing of each assessment over the 37 weeks of the DOSE trial.
Modeling the Dynamics of Recovery During and After Rehabilitation
We developed models to account for the time course of the changes in MAL in response to discrete practice bouts with different dosages. The models are based on first-order linear differential equations with a time step of 1 week, which corresponds to the duration of each practice bout. In the text below we outline the methods for 2 models; we refer the reader to Supplementary material for a complete description of our modeling methods.
Let MAL(t) be the MAL at time t, with t in increments of days, with practice input u(t). To isolate the effect of task practice, we assumed that forgetting was smaller than learning during practice. Thus, the simplest first order dynamical model of changes in MAL for a single subject i at time
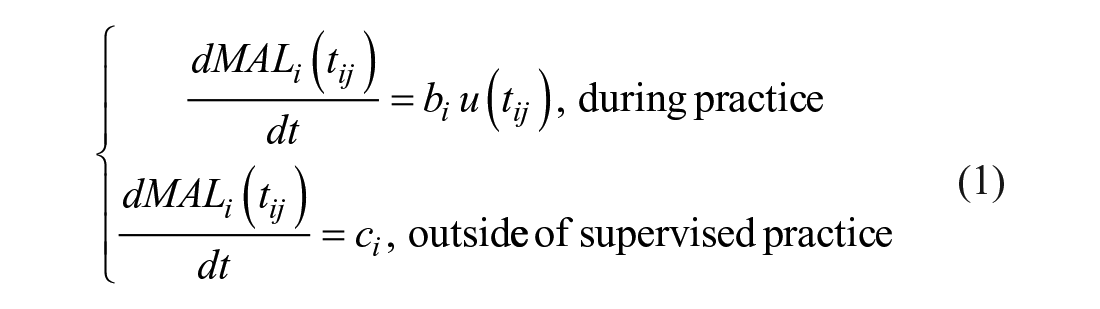
where
We built several models, each to test a specific hypothesis. For this, the learning and retention rates were modeled as linear functions of experimental variables and/or between-subject covariates, and included a random effect term to model individual differences.24-26 For most models, we developed both a continuous version, in which the parameters (learning and retention rates) depended linearly on a variable of interest (dose, time of practice, time post-practice, baseline MAL, and average MAL post-practice; see above), and a corresponding categorical version (see Table 1). Comparison of the parameters of the categorical models to the linear models helped visualize deviations from linearity.
Models Selected for All Hypotheses Tested. a
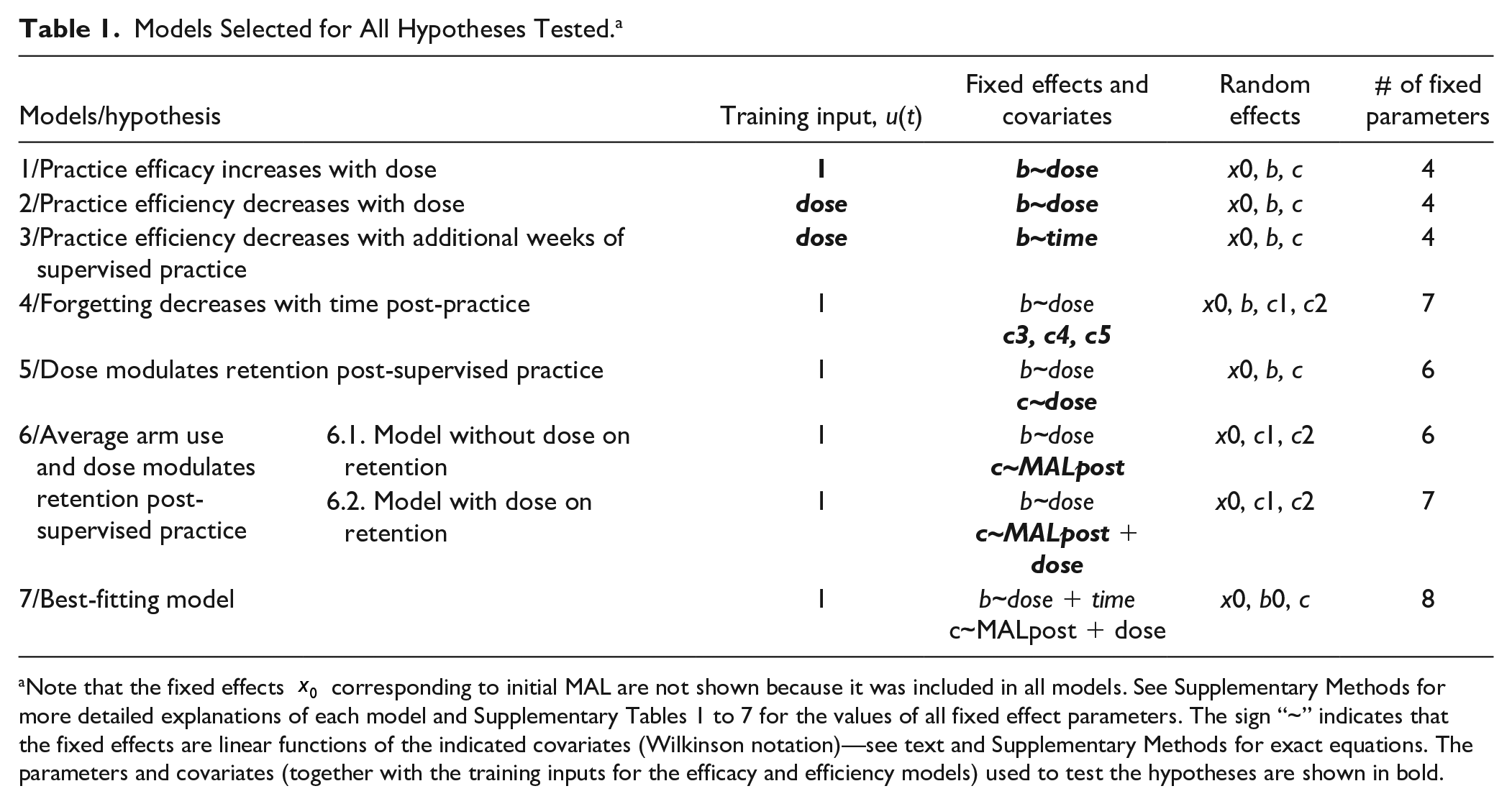
Note that the fixed effects
For instance, in Model 1, we assessed the efficacy of task practice with increasing dose. u(t) represents the timing of practice, and u(t) = 1 during task practice (as in the simulation of Figure 1B). In the continuous Model 1.1, the learning rate was modeled as a linear function of dose, given by

where
In Model 2, we assessed the efficiency of task practice with increasing dosage. In Model 2.1, the learning rates were also a linear function of dose, but the inputs were modeled as step inputs of magnitudes equal to the weekly dose u(t) =

with the learning rate modeled as a linear function of dose, given by

where
Similarly, we assessed the efficiency of practice with increasing practice bouts, by modeling the learning rate as a function of increasing weeklong bouts of practice (Models 3). We assessed the dynamics of retention, by modeling the retention rates as a function of time after practice (in 2-month increments; Models 4), dose of practice (Models 5), and average amount of arm and hand use after practice (averaged MAL over 6 months; Models 6).
Except for the best fitting model (Model 7), significance of the fixed slopes for the learning or retention linear models was used to test our hypotheses (see Table 1). We refer the reader to Supplementary Material and Table 1 for descriptions of all models and for fitting procedures.
Note that the nominal dosages for each of the 3 weeks of task practice are 0, 5, 10, and 20 hours. Because the WMFT and BART pre- and post-practice tests contained multiple movements and lasted approximately 1 hour, were added 2 hours to the actual dose per weeklong practice bout in the models. In addition, to account for the large variability in initial arm and hand use, we modeled MAL as a function of initial MALinit at baseline (median of MAL at 0, 1, and 2 weeks), which was significant for all models (P < .01).
Results
Qualitative Predictions From the Best Fitting Model
Figure 2A shows both actual MAL data and the fits of the best fitting model (Model 7, Table 1). The model well accounts for changes in MAL during both practice and following formal practice for 40 subjects (one subject exhibited poor fit due to highly variable measured MAL; see 3rd row, 2nd column). Figure 2B shows the model fits rearranged by dosage. Visual inspections of the plots inform the following general observations: (1) larger initial increases in MAL for larger doses (increased efficacy); (2) diminishing returns for larger doses (decreased dose efficiency); (3) diminishing returns for more practice bouts (decreased time efficiency); (4) decay of MAL post-practice for larger doses; (5) further increase in MAL in the months following practice for participants with higher MAL post-practice; and (6) in 0 dose group, increase in MAL during and following testing sessions. We confirm these observations in the analyses below using the models of Table 1.
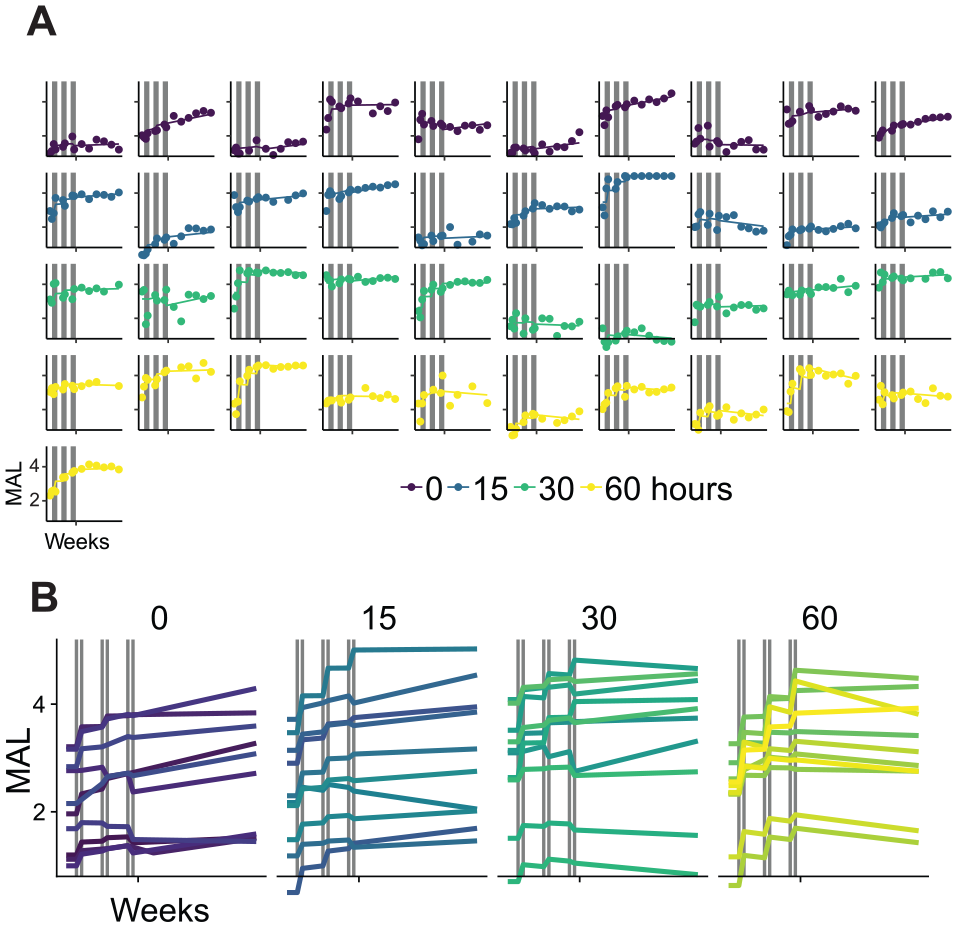
Quality of movement as measured by the MAL over the 37 weeks of the DOSE trial, assessed before, during, between, and following the 3 practice bouts, and an example of model fit to the data, using the best fitting model (Model 7, Table 1). (A) Data (dots) and model fit (lines) for all 41 participants. Gray vertical lines show the 3 week-long practice bouts. Note the overall excellent fit of the model to all participants (except for second participant in 30-hour dose, who exhibited large MAL variability). (B) Individual models rearranged by nominal dosages. Note the following: (1) larger increase in MAL during practice for larger dosages (increased dose efficacy); (2) diminishing returns for larger dosages (decreased dose efficiency); (3) diminishing returns for more practice weeks (decreased practice bout efficiency); (4) decrease in MAL post-practice for larger dosages; (5) further increase in MAL for high average post-practice MAL; and (6) in 0 dosage group, increase in MAL. These observations were all confirmed statistically—see text.
Increasing the Dosage Increases the Efficacy of Task Practice
Increasing the dose of task practice increases the efficacy of practice, as shown by the positive slope between dose and learning rate in Model 1.1 (Table 1; Figure 3A: slope parameter b.dose = 0.008 [corresponding to
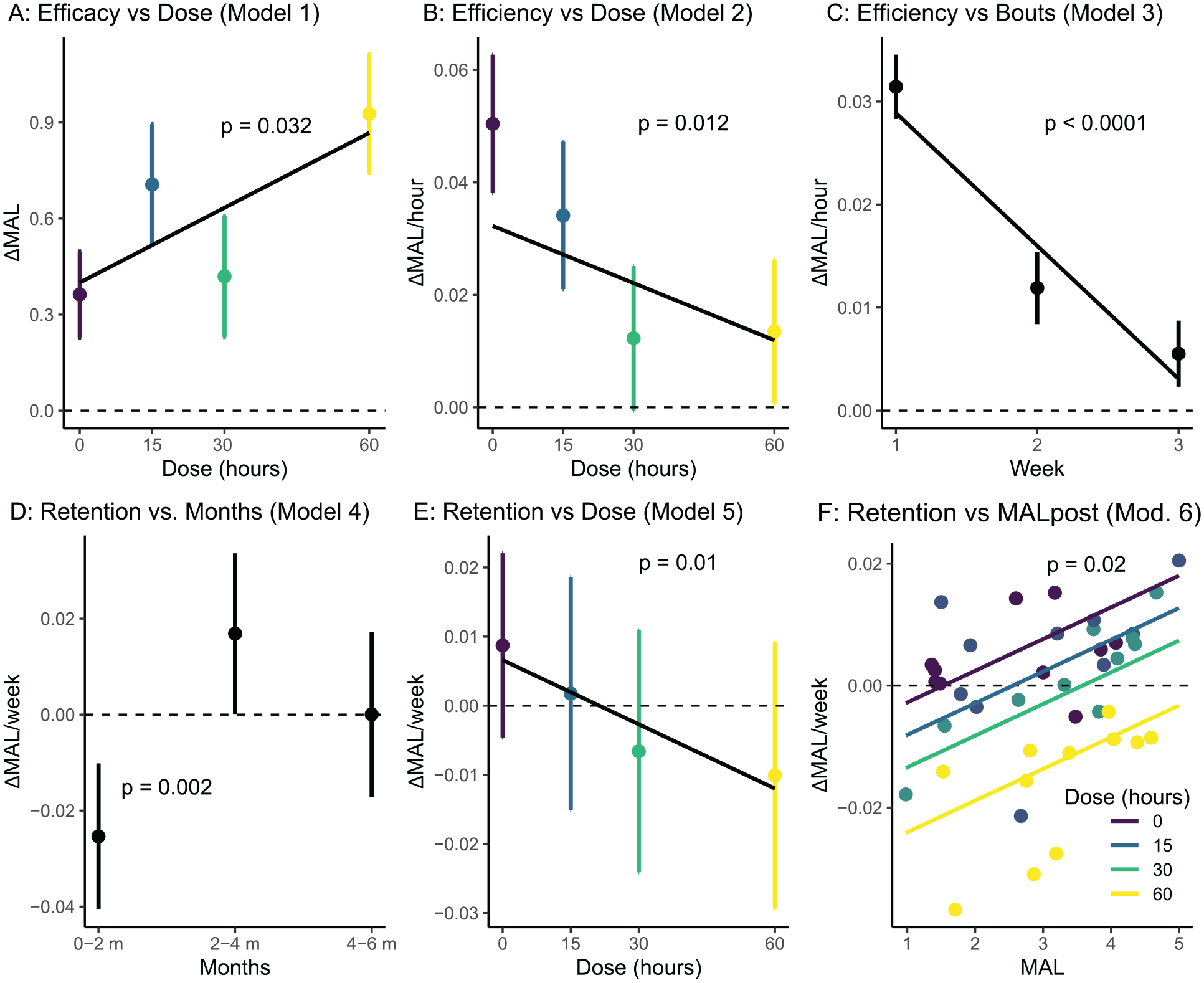
Fixed effect parameters used to test all 6 hypotheses. (A) Effect of dose on the MAL during supervised practice (dose efficacy; Models 1, Table 1). (B) Effect of increasing the dose on gain in MAL per hour of practice (dose efficiency; Models 2). (C) Effect of increasing the number of weeks of formal practice on gain in MAL per hour (duration efficiency; Models 3). (D) Effect of time on retention: Retention rate in the 6 months following supervised practice as a function of months post-practice (0-1 months, 2-3 months, and 3-5 months; Model 4). (E) Effect of dose on retention (Models 5). (F) Effect of average post-practice MAL on gain in MAL (Models 6). The thick dark line shows retention as a function of average post-practice MAL in Model 6.1. The colored lines show retention as a function of average post MAL for different doses and the colored dots show the individual retention rates (mixed effects) in Model 6.2.
Increasing Dose Decreases the Efficiency of Task Practice
We then studied the efficiency of practice, that is, the gain in MAL per hour for increasing dosages (Models 2, Table 1). As predicted, increasing the dosage of practice decreases the efficiency of task practice, as shown by the negative slope (Model 2.1; Figure 3B; parameter b.dose = −0.001 [corresponding to
Increased Task Practice Duration Decreases the Efficiency of Practice
As was the case for increasing dosages, the efficiency of practice decreases with number of additional weeks of practice (Model 3.1; Figure 3C; bt.weeks = −0.013; P < .0001; see Supplementary Table 3). The categorical model (Model 3.2) shows a more than 2-fold reduction in gain for the second week and almost 5-fold reduction for the third week compared to the first week (see Supplementary Table 3). Interestingly, the b3 coefficient (third week learning rate) in the categorical Model 3.2 is not significantly different from zero (P = .15), showing that across dosages, the third weeklong bout of practice has very little effect on changes in MAL during practice (note that we cannot determine how the third bout influences retention, because we did not vary the number of weeks of practice in the DOSE trial).
Decay Following Task Practice Is Fast Initially but Slows Down Within 2 Months Post-Practice
Across dosages, forgetting following task practice was initially fast: the retention parameter c1 in the 2 months following formal practice is largely negative, but retention is not different from zero in the next two 2-month periods—although there is a nonsignificant trend upward for the next 2 months (Figure 3D; c1 = −0.025, P = .002; c2 = 0.017, P = .50; c3 = 0.0001, P > .999; see Supplementary Table 4).
Retention Following Practice Is Negatively Modulated by the Dose of Task Practice
Following supervised practice, we found an unexpected increase in forgetting for larger dosage, as seen by the negative slope between dose and change in MAL between sessions (Figure 3E; Model 5, Table 1, parameter c.dose_cont = −0.001; P = .01; see Supplementary Table 5). The model with categorical doses (Model 5.2, Table 1) shows that the effect of dose on retention is negative and significantly different from 0 for 30- and 60-hour groups (c.dose_hour30 = −0.015; P = .023, c.dose_hour60 = −0.019; P = .012), but not for 15 hours (P = .28). Note that the best fitting model (Model 7) indicates that 9 out of 11 participants in the 60-hour group show a decrease in MAL following practice; this is to be compared with 9 out of 10 participants in the 15-hour group who show an increase in MAL (Figure 2B).
A Threshold Determines Increase Versus Decrease in the Perceived Quality of Arm Movement Following Practice
Retention in the 6 months following supervised practice is positively modulated by the average MAL, MALpost during these 6 months (Model 6.1 slope = 0.0047, P = .02; see Supplementary Table 6, Figure 3F). Because of the negative intercept (−0.016, P = .019), there is a threshold for spontaneous increase in MAL following practice. On average, across dosages, if MALpost is above a threshold of 3.4 (determined by 0.0047 * MALpost − 0.016 = 0), the retention parameter is positive, that is, the MAL keeps increasing following practice.
A model that includes both MALpost and dose on the retention parameter (Model 6.2) shows that for a smaller dosage (0, 15, and 30 hours), the retention parameter is negative for smaller values of MALpost and positive for larger value (see Figure 3F and Supplementary Table 6). However, because increasing dose leads to lower retention (see above), the threshold above which the MAL increases following practice is dose-dependent, with the counterintuitive results that a smaller average MALpost can be sufficient to increase MAL following formal practice for small doses, but not for the largest dose (see Figure 3F). For instance, for the 15-hour dose, the threshold is approximately 2.5. In contrast, for the 30-hour dose it is just under 4. For the 60-hour dose, this model showed retention is negative for all values of average MAL post.
Discussion
Increasing the efficacy of practice, the efficiency of practice, and the long-term retention of motor skills following practice after stroke form the cornerstones of neurorehabilitation. 38 Here, using a combination of novel piece-wise linear models with mixed effects and a novel practice design, we were able to dissociate the effects of dose and duration of task-specific practice on the efficacy, efficiency, and retention of a valid and reliable neurorehabilitation outcome, 39 the MAL.
Our findings show that large dosages of practice increase MAL from pre- to post-practice (Figure 3A). This result reproduces the previously reported dose-response relationship in the DOSE trial, which was only determined from the changes due to the 3 practice bouts. 10
In contrast, a model with inputs that scale to the dose (Model 2, and Equation 3) showed a clear decrease in efficiency with additional hours of practice (Figure 3B). Each hour of practice in the 60-hour dose group is about 2 times less effective at increasing the MAL than an hour in the 15-hour dose. Similarly, there is a strong decrease in the efficiency of weeks of practice (Figure 3C): the third week is more than 5 times less efficient than the first. Such decreases in efficiency are consistent with the well-known diminishing returns law of motor learning, where each additional unit of practice yields a smaller gain. Note that our findings on the efficacy and efficiency results are not surprising given their pervasiveness in behavioral motor learning research. 6 However, it is the first time, to our knowledge, that the efficiency of motor learning has been systematically studied with respect both to treatment dose and duration of practice on the change of a clinical outcome in chronic stroke survivors.
Across dosages, retention following practice resembles exponential-like decay (Figure 3D), because it is initially fast in the 2 months following formal practice before tapering back near baseline in the next 4 months. Such decay is compatible with behavioral and computational results of motor learning and adaptation studies,27-35 in which memories follow exponential-like decay following deliberate practice. Note, however, that an alternative interpretation is that the participant’s perceptions of their competence with the affected hand is highest at the end of intensive practice. Following practice, actual motor competence might remain the same, but perceptions of that competence might decrease, as the “novelty” of initial gains wears off.
In addition, and contrary to our hypothesized effect of increasing dose on retention, we found that large doses increase decay in the 6 months post-practice (Figure 3E). Two nonexclusive mechanisms can explain these results. First, higher levels of skills require more maintenance. According to this view, if the participants reach higher levels of compensatory skills with 60 hours of practice, and no additional practice is given, there will be decay of these skills. Second, according to the “guidance hypothesis,” 40 as guidance and encouragement are removed following practice, performance decays; such decay is greater for larger doses in which more supervision and encouragement were given.
In addition, and in opposition to such dose-dependent decay, our results suggest that spontaneous arm use post-practice can improve retention. We previously postulated the existence of a threshold post-stroke (see also MacLellan et al 41 ) in which arm and hand use in daily activities acts as “self-practice” and reinforces performance, which then further reinforces use in a virtuous cycle.18,21,22 In line with this finding, we showed that retention is positively modulated by the average post-practice MAL (Figure 3F). Across dosages, the threshold for MAL is ~3.4. Thus, if MAL post-practice is relatively high, then it will keep increasing following formal practice. Such an effect is more pronounced in the low dosage groups, as can be seen in Figure 2B for several participants, because in these groups, the negative effects of dose on retention is less strong.
Finally, as noted the 0-hour group shows a significant increase in MAL during and post-practice. In addition to the MAL, participants performed the WMFT test (in which participants perform goal-directed arm and hand movements) and the BART assessment, which consisted of arm reaching tests comprised of approximately 200 movements with the more affected arm. 15 Thus, the assessments may have resulted in more task practice.
Note that because MAL decreases following practice for the large dose groups, and MAL increases following practice for smaller dosages, the dose response curve observed during practice (Figure 3A) does not hold from pre-practice to 6 months post-practice. Indeed, there is no difference in response across dosages in the differences in the initial MAL before practice with the last MAL after practice (medians of the first 3 MAL in assessments 1, 2, and 3, and medians of the last 3 MAL in assessments 12, 13, and 14; ANOVA, P = .27).
Limitations
There are 3 primary limitations of our study. First, despite the MAL’s good validity and reliability, 39 as well as its significant association with subjective perception of recovery, 42 using the changes in MAL as a proxy for motor learning is not ideal, as the MAL relies on self-reported ratings of the quality of movements across a range of tasks. As such, the MAL is not always strongly associated with functional changes and accuracy in responding to a structured interview may be influenced by practice. 43 In addition, different outcomes poststroke follow different dose-dependent relationships. 44 Thus, it is unclear whether our results generalize to all poststroke outcomes, as we cannot disentangle if the changes in MAL reflect changes in (1) impairment, (2) function in which compensatory changes enable greater use, (3) choice to use the arm, 45 or (4) any combination of the above. Future work will need to model the changes in kinematic outcomes, which are more sensitive and suffer less from ceiling effects than clinical outcome measures.46,47
Second, whether our results also apply to neurorehabilitation in the acute/subacute phase is to be seen. A main difference between the chronic and acute/subacute phases is the critical window of plasticity, which is thought to enhance the effect of practice following stroke, 48 but has a time course of a few weeks/months following stroke. 49 A prediction, therefore, is that, in the acute/subacute phase, the efficacy of task-specific practice would be higher, but the efficiency would decrease even faster over weeks of practice than in our study.
Third, because of the relatively small sample, the groups were not well balanced for initial level of MAL. In particular, because the initial MAL is larger in the 30-hour dose group, participants in this group appeared to have benefited less from task-specific practice. This affected the dose-dependent results (see Figure 3A). Re-running the linear dose efficacy Model 1.1 without the 4 participants with MALinit > 3.5 (3 participants in the 30-hour group and 1 participant in the 15-hour group) improved the significance of the slope from P = .032 to P = .019. Thus, larger samples are needed in future studies.
Conclusions: Implications for Clinical Practice
Our results paint a contrasted view of the effect of task-specific practice in the chronic stage poststroke: although practice increases MAL, the gains per hour becomes small as dosage becomes large and these gains are often reduced in the months following practice, notably for larger dosages. However, our results suggest 4 methods to maximize the efficacy and the efficiency of task practice in chronic stroke survivors: First, task practice should be given in relatively small bouts distributed over months. Such a strategy would not only maximize gains, but also maintain these gains (because smaller dosages lead to less decay). This practice strategy is consistent with the “spacing effect,” according to which the spacing of presentations improves retention compared to massed presentations.33,50-52 Second, these smaller bouts of practice should contain a high number of movements. The number of movements in the 0-dose group was approximately 200 movements during WMFT and BART testing. We previously showed that large gains in reaching movements were achieved with approximately 300 fast movements delivered in one session. 25 Third, our results suggest a personalized dosage duration of task practice based on arm and hand use measurements: We showed that, on average, for individuals with MAL above a threshold of ~3.4, supervised practice could be stopped, as self-practice in daily activities will continue to increase arm use. For individuals with MAL below this threshold, our results suggest a need for the development of personalized strategies to overcome barriers to arm and hand use in the natural environment, to foster more effective engagement in self-practice. Finally, models such as those proposed here could be simulated to determine, in advance, the best timing, dose, and schedules of practice to maximize the gains given resources to reach the necessary threshold.
Supplemental Material
Supplementary_Methods_NNR_final_resubmit_final – Supplemental material for The Efficiency, Efficacy, and Retention of Task Practice in Chronic Stroke
Supplemental material, Supplementary_Methods_NNR_final_resubmit_final for The Efficiency, Efficacy, and Retention of Task Practice in Chronic Stroke by Chunji Wang, Carolee Winstein, David Z. D’Argenio and Nicolas Schweighofer in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
We thank Bokkyu Kim and Sujin Kim for their help in preprocessing the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Institute of Neurological Disorders and Stroke of the National Institutes of Health under Award Numbers R01 HD065438 and R56 NS100528, also by the National Institute of Biomedical Imaging and Bioengineering P41-EB001978 and the Alfred E. Mann Institute at USC. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
1*
Please note that we are not proposing a model of motor adaptation poststroke, nor claiming that motor learning due to task-specific practice is akin to motor adaptation—it is presumably not—however, these models allow us to characterize the dynamics of motor learning, with 2 simple assumptions: increase in performance during supervised practice and retention of performance following formal practice.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.