
Abstract
Background. Fatigue is a debilitating symptom in multiple sclerosis (MS) that may be associated with reduced physical activity and increased sedentary behavior. Objective. This study examined the associations among fatigue and device-measured physical activity and sedentary behavior in people with MS. Methods. The participants (n = 252) completed the Patient Determined Disease Steps (PDDS) and Fatigue Severity Scale (FSS) and wore a waist-mounted accelerometer for 7 days. Participants were divided into 2 groups based on fatigue severity as measured by the FSS scale. We compared percentage of wear time spent in sedentary, light physical activity (LPA), and moderate to vigorous physical activity (MVPA) between the 2 groups. Results. Persons in the fatigued group (FSS score ≥ 4) spent a greater percentage of time in sedentary behavior (P = .004) and a lower percentage of time in LPA (P = .035). Persons in the fatigued group further spent a lower percentage of time in nontransformed MVPA (P < .001) and square-root-transformed MVPA (P < .001) than persons in the nonfatigued group. When controlling for PDDS scores and years of education, there were no longer significant differences between groups in sedentary behavior, LPA, or transformed MVPA values; the difference in nontransformed MVPA was still statistically significant but likely the result of nonnormally distributed data. Conclusion. The present study suggests that factors other than fatigue might be associated with physical activity and sedentary behavior in MS, and this group might benefit from focal behavioral interventions that take into account mobility status in persons with MS who have fatigue.
Introduction
Multiple sclerosis (MS) is a chronic, immune-mediated disease of the central nervous system (CNS), with a prevalence of nearly 1 million adults in the United States and 2.5 million adults worldwide.1,2 This disease involves unpredictable episodes of inflammatory demyelination and transection of axons in the brain, optic nerves, and spinal cord and results in lesions that interfere with the conduction of electrical potentials along neuronal pathways.3,4 The damage within the neuronal pathways, depending on its degree and location, can manifest as a number of different symptoms. The symptom of fatigue is one of the most common and debilitating manifestations of MS. 5
Fatigue, defined as “a sense of exhaustion, lack of energy, or tiredness,” 6 is a common and debilitating symptom that occurs among ~80% of people with MS. 5 Fatigue often limits daily activities, restricts participation in social events, and undermines quality of life in people with MS.5,6 The exact cause of fatigue in MS is unclear, although it likely involves latent disease processes such as inflammation and demyelination of axons in the CNS as well as secondary effects of deconditioning, diet, and/or sleep. 7
There is consistent evidence indicating that exercise training, one form of physical activity, is associated with lower levels of fatigue in people with MS, 8 but the relationship between lifestyle physical activity and fatigue is less clear.9,10 Lifestyle physical activity involves bodily movement produced by skeletal muscle contraction, resulting in an increase in energy expenditure as part of self-selected activities during one’s daily routine (eg, gardening, vacuuming), 11 and lifestyle physical activity may be associated with fatigue in MS. Indeed, research indicates that nearly 80% of people with MS do not engage in sufficient amounts of physical activity necessary for accruing health benefits, 12 and persons with MS are less physically active than healthy adults from the general population.13,14 Researchers have identified fatigue itself as a possible barrier to participation in physical activity behavior in MS.15,16 To date, some studies support an association between fatigue and lower levels of physical activity in MS,9,10,17,18 whereas other studies report either a weak association or no association between fatigue and physical activity.19-23 This inconsistency might be associated with a combination of factors, including small sample sizes, lack of device-measured levels of light (LPA) and moderate to vigorous physical activity (MVPA), or application of poorly validated measures of fatigue.
Physical activity can be viewed as a continuum from sedentary behavior through vigorous physical activity, and there is little known about fatigue and its association with sedentary behavior (ie, sitting or lying down), the other end of the activity continuum. 24 This is important because sedentary behavior may be an entry point for changing LPA and then MVPA in MS (ie, reduce sedentary behavior and replace it with LPA and then MVPA). Sedentary behavior is defined as “any waking behavior characterized by an energy expenditure <1.5 metabolic equivalents (METS) while in a sitting or reclining posture.” 25 (p. 1250) This is exceedingly high in persons with MS, 26 and sedentary behavior (ie, activities performed while sitting, reclining, or lying down) has been recommended as a strategy for energy conservation in MS. To that end, persons with MS who have fatigue may not only have lower levels of LPA and MVPA but may further engage in higher levels of sedentary behavior than those without fatigue, particularly as part of energy conservation.
This study involved a secondary analysis of data from a relatively large sample of persons with MS 27 and examined the associations among fatigue, based on the Fatigue Severity Scale (FSS) 28 and device-measured LPA and MVPA as well as sedentary behavior among people with MS; we focused on sedentary behavior, LPA, and MVPA, rather than steps or other variables, based on a representation of the activity continuum. 24 Such an inquiry overcomes the aforementioned problems of previous research in this area, and provides a novel, comprehensive examination of fatigue and physical activity across the activity continuum. We expected that persons with MS who had elevated fatigue (ie, score of 4 or higher on FSS) would have lower levels of LPA and MVPA and higher levels of sedentary behavior than those without fatigue (ie, score of less than 4 on FSS).7,28 We further controlled for variables (ie, confounders) that significantly differed between groups and have previously demonstrated associations with physical activity in adults with MS (ie, disability status and level of education). 12 The results of this research may inform the development of targeted behavioral interventions that focus on reducing fatigue in persons with MS as an approach to changing physical activity and/or sedentary behavior based on the notion of the physical activity continuum.
Methods
Participant Recruitment and Eligibility
This study involved a secondary analysis of previously published data. 27 Briefly, participants were recruited through the North American Research Committee on Multiple Sclerosis (NARCOMS) patient registry. The recruitment occurred through the random selection of 1000 persons with MS who completed the biannual NARCOMS registry update survey (Fall, 2017) who were mailed letters by NARCOMS staff; this sample size was selected based on an expectation of 25% participation in the current study as estimated by NARCOMS. Those who received study information and were interested in participation contacted the research team either by email or telephone, and members of the research team described the study and its procedures, answered any questions, and then conducted a brief screening interview for inclusion criteria. The inclusion criteria were as follows: (1) randomly selected member of the NARCOMS registry and (2) willing to complete the questionnaires, wear the accelerometers, and return the materials via the United States Postal Service (USPS). Of the 1000 persons with MS who were mailed flyers, 316 persons contacted the research team, and 296 of them underwent screening; 1 person declined participation after the description of the study. The research team then mailed the study materials among the remaining 295 persons, and 284 of them returned the packet. Of those who returned the packet, 9 declined participation based on not signing the informed consent document, and 1 person declined participation based on not being interested in wearing the accelerometer. There were 11 persons who did not return the packets for unidentified reasons, and 22 persons did not have usable accelerometer data. To that end, the final sample for inclusion in the analyses consisted of 252 persons with MS who had complete data (ie, complete questionnaires and device-measured physical activity).
Measures
Demographic and Clinical Characteristics
We measured demographic and clinical characteristics for describing the sample and examining these variables as possible confounders of the association among fatigue and device-measured LPA, MVPA, and sedentary behavior. 12 Demographic and clinical characteristics included age, gender, race, years of education, marital status, number of children, income, MS type, disease duration, and disability status based on Patient Determined Disease Steps (PDDS) scale scores. The PDDS scale contains a single item for measuring self-reported disability status. 29 PDDS scores range between 0 (normal) and 8 (bedridden), and the scores have been validated as a measure of disability status in persons with MS based on the linear and strong correlation with physician-rated Expanded Disability Status Scale (EDSS) scores. 29 The PDDS further contains fewer questions and is less cumbersome than self-report versions of the EDSS.
Race, marital status, number of children, income, and MS type were all dichotomized—namely, race was categorized into either Caucasian or non-Caucasian, marital status was divorced/other or married, children was either 0 or 1 or more, income was either less than $40 000/year or greater than or equal to $40 000/year, and MS type was either relapsing-remitting MS (RRMS) or progressive MS. This is consistent with previous research 12 and the notion that these variables as measured likely represent a categorical structure. 30
Fatigue
The perception of fatigue severity was measured using the FSS 28 because it is one of the most commonly applied measures of fatigue in MS 31 and there is no gold standard measure of fatigue in this population. We opted for the FSS rather than the Modified Fatigue Impact Scale (MFIS) 32 because it measures the severity of fatigue, and we presumed persons with MS who had more severe fatigue would engage in less physical activity and more sedentary behavior. The FSS has 9 items rated on a 7-point scale of 1 (strongly disagree) through 7 (strongly agree) regarding the severity of fatigue symptoms during the past 7 days. The scores for the 9 items were averaged into a measure of fatigue severity that ranged between 1 and 7. FSS scores of 4 or above were indicative of severe MS-related fatigue,7,28,31 and participants were divided into 2 groups based on FSS scores: fatigued (FSS score ≥ 4) and nonfatigued (FSS score < 4). There is evidence for the internal consistency, test-retest reliability, and validity of FSS scores as a measure of fatigue severity in MS. 28
Device-Measured Physical Activity and Sedentary Behavior
The ActiGraph model GT3X+ accelerometer provided a device measurement of physical activity and sedentary behavior. The accelerometer was positioned in a pouch on an elastic belt worn around the waist above the nondominant hip during the waking hours of the day, except while showering, bathing, and swimming, during a 7-day period. The participants recorded the time that the accelerometer was worn daily in a log; this log was reviewed for verifying wear time during data processing. The accelerometer data were downloaded, and wear time was estimated using the Troiano 33 algorithm and processed into 1-minute epochs with the low-frequency extension; data were then scored for wear time (min/d) and minute-by-minute activity counts representing LPA and MVPA (cut-point 1584 counts/min-1) as well as sedentary behavior per day (100 counts/min-1). 34 We considered a day as valid if there was a minimum of 10 hours of total wear time without continuous zeros exceeding 30 minutes. Participants with 1 or more valid days of data were included in the analyses because this has been commonly done in the general population of adults (eg, National Health and Nutrition Examination Survey).12,35 Within the current study, 143 (56.7%) participants had 7 days of valid data, 43 (17.1%) had 6 days of valid data, 25 (9.9%) had 5 days of valid data, 13 (5.2%) had 4 days of valid data, and 9 (3.6%) had 3 days of valid data; only 19 (7.6%) participants had fewer than 3 days of valid data. This variability in the number of valid days across participants is expected based on variability in compliance with instructions and represents a possible weakness of the study. We expressed these outcomes as a percentage of wear time (ie, percentage of average daily wear time spent in LPA, MVPA, and sedentary behavior).
Procedures
On successful completion of the telephone screening, participants were mailed a packet containing the informed consent document, questionnaire battery, accelerometer along with instructions and log, and prestamped and preaddressed envelopes for return postal service through the USPS. Participants were contacted by researchers to ensure that the packet was received and the directions were understood, and they were instructed to complete the battery of questionnaires and then wear the accelerometer and over a 7-day period. After wearing the accelerometer and completing the questionnaires, participants returned a signed copy of the informed consent along with the study materials through the USPS. All questionnaires were checked for completeness within 48 hours of receipt, and in the event of missing data, a member of the research team contacted participants and collected the data over the phone by reading the scale instructions, item, and rating scale for the missing data. All participants received $10 for voluntary participation. The procedure for this study was approved by a university institutional review board.
Data Analysis
The data were analyzed using SPSS Statistics (version 25). We provided descriptive statistics for continuous variables as means and SDs, nominal variables as numbers (n) and percentages (%), and ordinal variables as medians and interquartile ranges. We initially compared the nonfatigued and fatigued groups for differences in demographic and clinical variables using Mann-Whitney U tests, independent samples t-tests, and/or χ2 tests, as appropriate for the type of variable (eg, χ2 for dichotomous variables such as sex). We then compared differences between fatigue groups for percentage of wear time spent in LPA, MVPA, and sedentary behavior using 1-way ANOVA. We tested the assumption of normality by examining histograms with normal distribution curves 36 as well as estimating skewness and kurtosis values and transformed any outcome variables that were not normally distributed. 37 We transformed the data using a square root function and performed the analysis on the original and transformed data because this would indicate if the analysis was biased by a nonnormal distribution and provide greater interpretability, because transformed data are not interpretable in the original units of measurement. 37 We performed final analyses using ANCOVA controlling for demographic and/or clinical variables that differed between fatigue groups (ie, disability status and years of education). Importantly, we applied ANOVA for the initial comparison of groups, rather than independent samples t tests, because those models are isomorphic and the ANOVA and ANCOVA are directly comparable. We further note an absence of an analogue of the t test that controls for covariates. The Cohen d was used to estimate the magnitude of difference in mean scores between groups using the cut-off scores of 0.1, 0.3, and 0.5 for small, moderate, and large, respectively.
Results
Participant Characteristics
The participant characteristics are provided in Table 1. The total sample consisted of 252 participants. The average age was 59.3 ± 10 years. The sample was largely female (80.6%), Caucasian (94.4%), and married (69.8%). The majority (68.3%) of participants reported having RRMS, and the average disease duration was 20.3 ± 9.7 years. The median PDDS score was 3.0, which indicated gait disability.
Descriptive and Clinical Characteristics of the Overall Sample of Persons With Multiple Sclerosis and the Nonfatigued and Fatigued Groups.
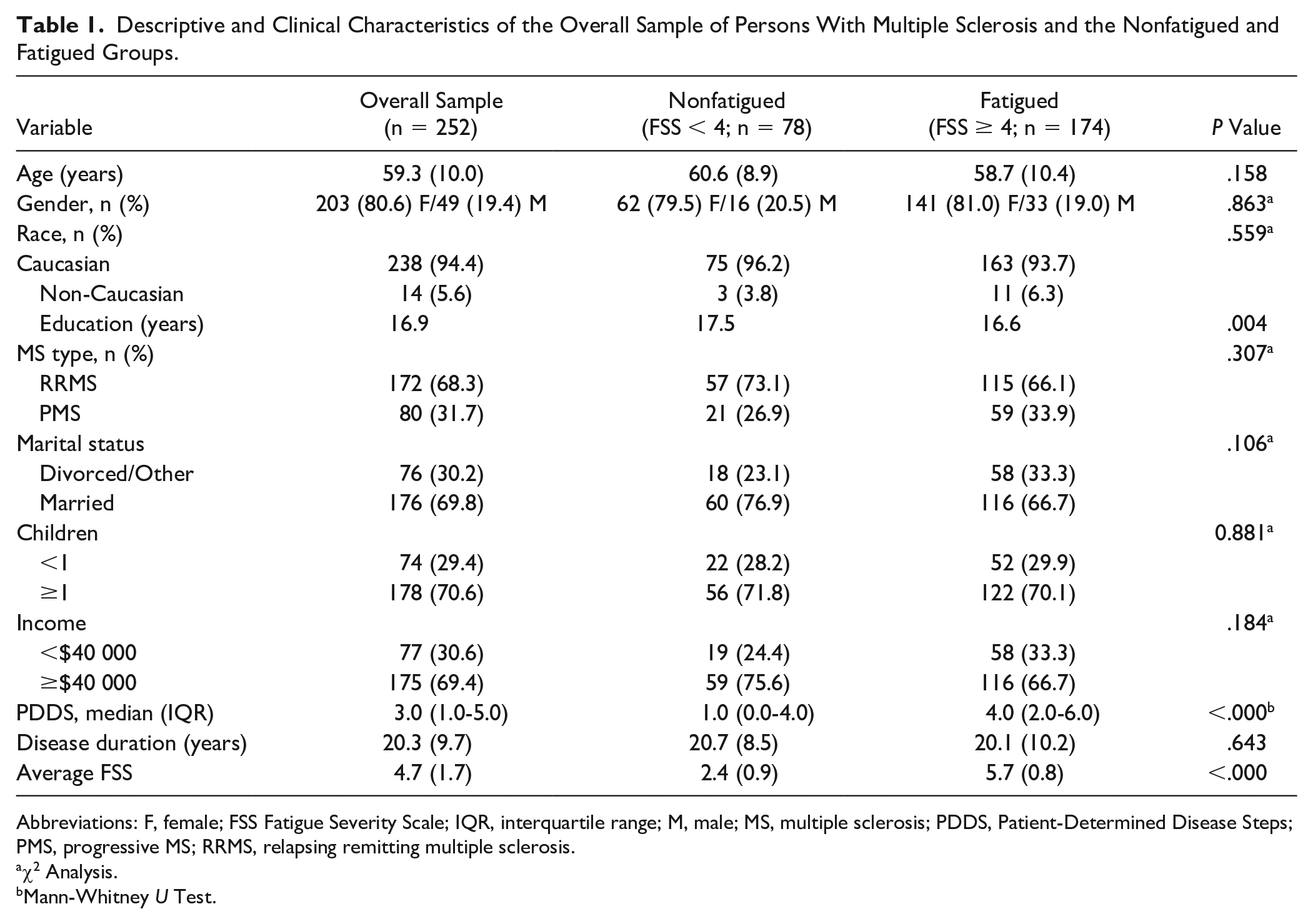
Abbreviations: F, female; FSS Fatigue Severity Scale; IQR, interquartile range; M, male; MS, multiple sclerosis; PDDS, Patient-Determined Disease Steps; PMS, progressive MS; RRMS, relapsing remitting multiple sclerosis.
χ2 Analysis.
Mann-Whitney U Test.
Of the 252 participants, 174 (69%) participants had FSS scores ≥4 and were categorized as fatigued, and the other 78 (31%) participants were categorized as nonfatigued based on FSS scores <4. Persons in the fatigued group had higher levels of mobility disability (P < .01) and fewer years of education (P = .004) than the nonfatigued group; there were no other differences in demographic or clinical characteristics.
Differences in Physical Activity Variables Between Groups
The descriptive data on physical activity and sedentary behavior in the nonfatigued and fatigued groups and overall sample are in Table 2. Percentage of wear time spent in sedentary behavior and LPA were normally distributed overall and within fatigue groups, whereas data for MVPA were not normally distributed and were transformed using a square root function. Persons in the fatigued group spent a greater percentage of wear time in sedentary behavior (P = .004; mean difference = 4.2%; d = 0.399) and a lower percentage of wear time in LPA (P = .035; mean difference = −2.7%; d = −0.290) than persons in the nonfatigued group. Persons in the fatigued group further spent a lower percentage of wear time in nontransformed MVPA (P < .001, mean difference = −1.5%, d = −0.671) and square-root transformed MVPA (P < .001, mean difference = −4.4%, d = −0.595) than persons in the non-fatigued group. When controlling for variables that were significantly different between groups (ie, PDDS scores and years of education), there were no longer significant differences between groups in sedentary behavior, LPA, or transformed MVPA values; the difference in nontransformed MVPA was still statistically significant but likely the result of nonnormally distributed data.
Physical Activity and Sedentary Behavior of Overall Sample of Persons With Multiple Sclerosis and Differences Between Nonfatigued and Fatigued Groups. a
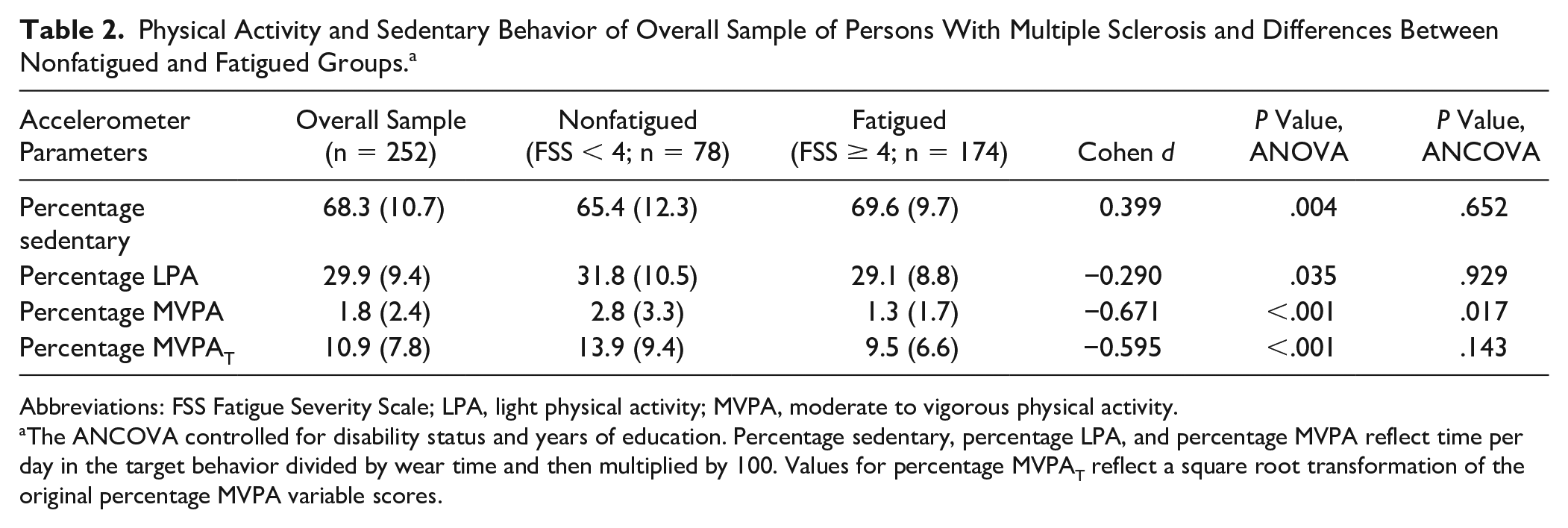
Abbreviations: FSS Fatigue Severity Scale; LPA, light physical activity; MVPA, moderate to vigorous physical activity.
The ANCOVA controlled for disability status and years of education. Percentage sedentary, percentage LPA, and percentage MVPA reflect time per day in the target behavior divided by wear time and then multiplied by 100. Values for percentage MVPAT reflect a square root transformation of the original percentage MVPA variable scores.
Discussion
The current study examined the association among self-reported fatigue and device-measured physical activity and sedentary behavior in people with MS. There were differences in LPA, MVPA, and sedentary behavior between fatigue groups when expressing those data as a percentage of total wear time; however, when controlling for disability status and education as possible confounders, there were no longer significant differences between groups. Collectively, we provided data indicating that factors other than fatigue severity may be associated with physical activity levels and sedentary behavior in persons with MS.
The existing research indicates that persons with MS generally engage in less physical activity and more sedentary behavior compared with samples that do not have MS or other chronic, disabling disease conditions.13,14 The current study did not have a healthy or non-MS control group, but comparison of our mean scores with those from previous research 12 indicates that our sample overall engaged in low levels of MVPA and high levels of sedentary behavior. Of particular note, our sample overall only spent 2% of daily wear time engaged in MVPA and 68% of daily wear time engaged in sedentary behavior. This is important because it indicates that our sample overall is consistent with previous research on physical activity and sedentary behaviors in MS,12,38 and this further supports our examination of the association between fatigue status and rates of physical activity and sedentary behavior across the activity continuum.
Our initial analyses indicated that percentage of time spent in LPA, MVPA, and sedentary behavior differed between fatigued and nonfatigued groups of persons with MS. Interestingly, there were no differences in physical activity and sedentary behavior between groups after controlling for disability status and years of education; those 2 characteristics differed between groups and represented important covariates for inclusion in the ANCOVA. Such results have 2 important implications. The first implication is that disability may account for the putative differences in physical activity and sedentary behavior between fatigued and nonfatigued persons with MS. Indeed, those in the fatigued group had an average PDDS score of 4.0 (early cane), whereas the average score for the nonfatigued group was 1.0 (normal), and this is consistent with other studies that examined the association between physical activity levels and mobility status. 38 Because this is a cross-sectional analysis, one could propose that these individuals may be less active and more sedentary based on a higher level of mobility disability that co-occurs with fatigue. The second implication is that the relationship between fatigue and physical activity is not straightforward, and thus, other confounders such as disability and education should be considered in future analyses.
Our findings may have important implications for the development of physical activity interventions among persons with MS with higher mobility disability. There is evidence that larger improvements in physical activity occur with behavioral interventions delivered among those with mild disability, 39 and we now provide clear evidence that disability status is associated with less participation in physical activity in those with elevated fatigue. Previous studies have reported that many interventions for people with MS typically target less-disabled samples. 40 This supports the design and delivery of interventions that consider baseline disability status for promoting physical activity among persons with MS who have fatigue for managing this symptom and other outcomes of MS. Such interventions might be informed by qualitative and mixed-methods research because these methods would provide new insight into the relevant targets of behavioral interventions. To date, researchers have not designed and tested such behavioral interventions for changing physical activity in those with MS who have higher mobility disability, and this represents a fertile opportunity for future research.
The strengths of the study include an examination of the association among fatigue and device-measured physical activity and sedentary behavior (ie, activity continuum) in a relatively large sample of persons with MS. However, the study is not without limitations. Notably, the cross-sectional design precludes conclusions and inferences about the causal and directional relationships between fatigue and behavior. 41 We further note that the sample primarily consisted of middle-aged Caucasian women with RRMS, and although this is consistent with the changing demographic landscape of MS, 2 we cannot make generalizations among younger persons with progressive forms of MS who are either non-Caucasian or male. We further note that general guidelines for valid accelerometer data are that the device is worn for 10+ hours per day, and we only included days of data that satisfied this criterion. There further was variability in the number of valid days of accelerometer data across participants, and this might represent a weakness, if the variability reflects poor compliance with wearing the device. We only included a single measure of perceived fatigue severity under the assumption that fatigue is stable over time, and there might be differential results for the perceived impact of fatigue, as measured by the MFIS, 32 on physical activity and sedentary behavior in MS. Future analyses might consider other approaches for measuring fatigue and examining its association with physical activity and sedentary behaviors, including capturing cognitive or psychosocial aspects of fatigue that could be associated with these outcomes.42,43 Finally, we did not account for other fatigue management approaches such as energy conservation or medications that might account for association between fatigue and physical activity/sedentary behavior in our analyses because this was a cross-sectional study.
Overall, the present study suggests that factors other than fatigue may be associated with physical activity and sedentary behavior in persons with MS. Our findings encourage the consideration of developing and delivering behavioral interventions that take into account mobility status in persons with MS who have fatigue because this approach might both increase physical activity as a health behavior and decrease fatigue itself.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was supported, in part, by a pilot grant from the National Multiple Sclerosis Society (PP 1412), a mentor-based postdoctoral fellowship from the National Multiple Sclerosis Society (MB 0011), and a predoctoral fellowship from the National Heart, Lung, and Blood Institute of the National Institutes of Health (T32HL105349). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.