
Abstract
Background. Reduced physical activity is an important consequence of multiple sclerosis (MS). However, little is known about the real quantity and type of daily activities that people with MS perform in their own home environment. Objective. To gain insight into differences in the amount and patterns of physical activities performed over a 24-hour period in the own community environment of patients with MS and healthy individuals. Methods. A total of 43 ambulatory patients with MS and 26 age- and gender-matched healthy individuals participated. Physical activity recorded with an ambulatory activity monitor was classified into postures and motions. Multilevel analyses were conducted to investigate whether the pattern of physical activities across daily periods (morning, afternoon, and evening) was dependent on the group (MS vs healthy individuals). Results. Results showed a significant overall lower amount of dynamic activity as compared with a group of healthy controls (P < .001). Patients with MS started with lower physical activity levels already in the morning (P < .001), and this difference persisted in the afternoon (P = .002) and evening (P = .032). Conclusion. Activity monitoring gives insight into real-world daily physical behavior. Our findings suggest that patients with MS may adopt a deliberate anticipatory strategy of lower activity in the morning, which persists throughout the day. Future trials evaluating daily changes in physical activity behavior should simultaneously sample self-report measures of energy levels and fatigue to elucidate the complex interaction between symptoms and physical activity.
Introduction
In patients with multiple sclerosis (MS), the variable distribution of demyelination and axonal loss throughout the central nervous system results in motor, sensory, visual, and autonomic disorders, 1 in turn leading to severe progressive limitations of functioning in daily life.
Accumulating evidence suggests that patients with MS are less physically active than nondiseased people.2-5 The observed reduction in the daily activities of patients with MS is often attributed to underlying impairments such as fatigue, depression, muscle weakness, spasticity, and ataxia.6-8
A central issue with regard to assessment of physical activity is objectification of information regarding the real quantity and type of daily activities performed in the patients’ own home environment. Several studies confirm that assessment of physical activity with patient-administered self-report questionnaires does not correspond well with actual performance assessed with more objective methods such as actigraphy and accelerometry.2,5,9 In a previous study, we found that severity of perceived fatigue measured by different validated self-report measurements was not significantly associated with amount of home-based physical activity in patients with MS. 10 It can, therefore, be hypothesized that patients with MS do not let symptoms guide their physical activity levels and subsequently may have a different distribution of their activities during the day, in order to cope with both neurological deficits and feelings of fatigue, as compared with healthy age- and gender-matched individuals.
To the best of our knowledge, no study has investigated the actual free-living physical activity profiles of patients with MS during 24 hours. The aim of the present study was, therefore, to gain insight into the amount, type, and distribution of daily physical behavior in patients with MS living in their own community setting. Daily activity was expressed as motions and postures, performed during the morning, afternoon, evening, and night. The observed motor activity distribution of MS patients during the different daily periods—morning, afternoon, and evening—was compared with that of a group of healthy age- and gender-matched controls.
We hypothesized that, on average, patients with MS show significantly lower levels of physical activity in terms of time spent on dynamic activity (motions) throughout the day when compared with age- and gender-matched healthy individuals. Second, we hypothesized that patients with MS would be less active in the morning because of a slower start as a result of coping with neurological deficits and reduction in activities to prevent depletion of energy because of limited energy levels. Moreover, we expect patients with MS to show earlier decrement in free-living physical activity in the evening because of diurnal increment of fatigue levels11-13 when compared with activity profiles of healthy controls. The slower start in the morning and the earlier decrement in physical activity in the evening of patients with MS were expected to be reflected in less time spent during that period of the day on dynamic activities (motions) when compared with healthy controls.
Methods
Participants and Design
MS patients were recruited over a 6-month period from a local outpatient database of the MS center and by referrals from the neurology department of the VU University Medical Center, the Netherlands. They met the following inclusion criteria: (1) older than 18 years, (2) a definite diagnosis of MS, 14 (3) an Expanded Disability Status Scale (EDSS) 15 score <6.5, (4) no comorbidity that could influence mobility, and (5) written informed consent. In keeping with an EDSS of 6 or lower, all patients with MS were able to walk at least 100 m with or without resting, with intermittent or constant unilateral assistance. None of the participants used a wheelchair.
The controls were matched for age and gender to reduce the probability of confounding by these factors. For the controls, the following criteria were applied: (1) older than 18 years, (2) no morbidity that could influence mobility, and (3) written informed consent. The medical ethics committee of the VU University Medical Center approved the study. All participants gave informed consent, in accordance with the ethical standards of the declaration of Helsinki.
Activity Monitoring
Daily motor activities were assessed by means of a portable activity monitor (AM). In previous studies, we showed that 24-hour activity monitoring is a feasible and reproducible method to measure daily behavior in ambulatory patients with MS.10,16 A detailed description of the system and application protocol is given in previous articles.10,16
Briefly, the system consists of a data recorder and 4 piezoelectric accelerosensors attached to the trunk and legs. The signals from the accelerometers were continuously stored for 24 hours on the compact flash card of the AM. After the measurement, the data were downloaded to a Microsoft Windows XP portable computer (service pack 3) for offline analysis. Data were analyzed and classified into motions, referenced as dynamic activity (primary outcome of the present study), and postures, referenced as static activity, according to the method of Bussmann et al. 17 The AM allows one to distinguish dynamic activity with subclassifications—walking, walking periods >5 s, walking periods >10 s, and transitions between different postures—and static activity with subclassifications—lying, sitting, and standing.
Assessment
Prior to performing the assessments, 6 research assistants were trained to apply the AM (for details see section Activity Monitor); 24-hour monitoring was implemented twice, with an interval of 1 week. Research assistants visited the participants 4 times at home. On the first visit, the AM was applied, and 1 day later at the second visit, the AM was removed. One week later at visit 3, the AM was again applied, and the following day at visit 4, it was removed. Assessments were done on all days of the week. All participants were instructed to continue their usual daily activities performed in their own environment (ie, home and community) and use their walking devices or orthoses as they would normally do but were asked to refrain from showering and swimming. Participants were told that the system measures body movement, but no elaborate explanation of the purpose of the study and the function of the AM was given until the end of the final measurement session.
Statistical Analysis
Descriptive analyses were conducted using SPSS (version 16.0). For all participants, the average scores over the 2 consecutive assessments were determined for all variables to attain stable estimates for analyses. The 24-hour registration period was divided into 4 daily periods—namely, morning from 6.00 to 12.00 hours, afternoon from 12.00 to 18.00 hours, evening from 18.00 to 24.00 hours, and night from 24.00 to 06.00 hours.
Subsequently, we used MLwiN 2.23 (Centre for Multilevel Modeling, University of Bristol, UK) for multilevel analysis. The first level was defined as serial measurements and the second level, the participants. The iterative generalized least squares algorithm was used to estimate the regression coefficients. The Wald test was used to obtain a P value for each regression coefficient. A multilevel model was developed to determine the association between activity and group (MS or healthy individuals). Given the longitudinal data analysis, a fixed and random intercept was used in the analyses. 18 To determine whether the activity level was dependent on daily periods (with “night” as reference category), interaction terms (Group × Daily period) were fitted into the model with activity and group.
The central hypothesis was tested by analyzing time spent on overall dynamic activity throughout the day between patients with MS (n = 43) and healthy participants (n = 26). To address the second hypothesis regarding being less active in the morning and showing earlier decrement in physical activity, the profiles of the subgroup classifications for dynamic activity—walking, walking periods, and transitions—and static activity—lying, sitting, and standing—were compared between patients with MS and healthy participants for the different daily periods. For all tests, a 2-tailed significance level of P < .05 was used.
Results
Patients’ Characteristics
In all, 52 patients with MS were contacted by phone as potential participants; 7 declined the invitation for reasons of unavailability or unspecified reasons. Eventually, 45 patients with MS and 27 healthy participants were included in the study. The AM data of 2 MS patients and 1 healthy participant could not be used because of a malfunctioning sensor. As a consequence, 43 patients with MS (mean age = 48.7 years; median EDSS score = 3.5) and 26 healthy participants 26 (mean age = 51.0 years) were used for analyses. Table 1 shows descriptive information of all included participants.
Participant Characteristics.
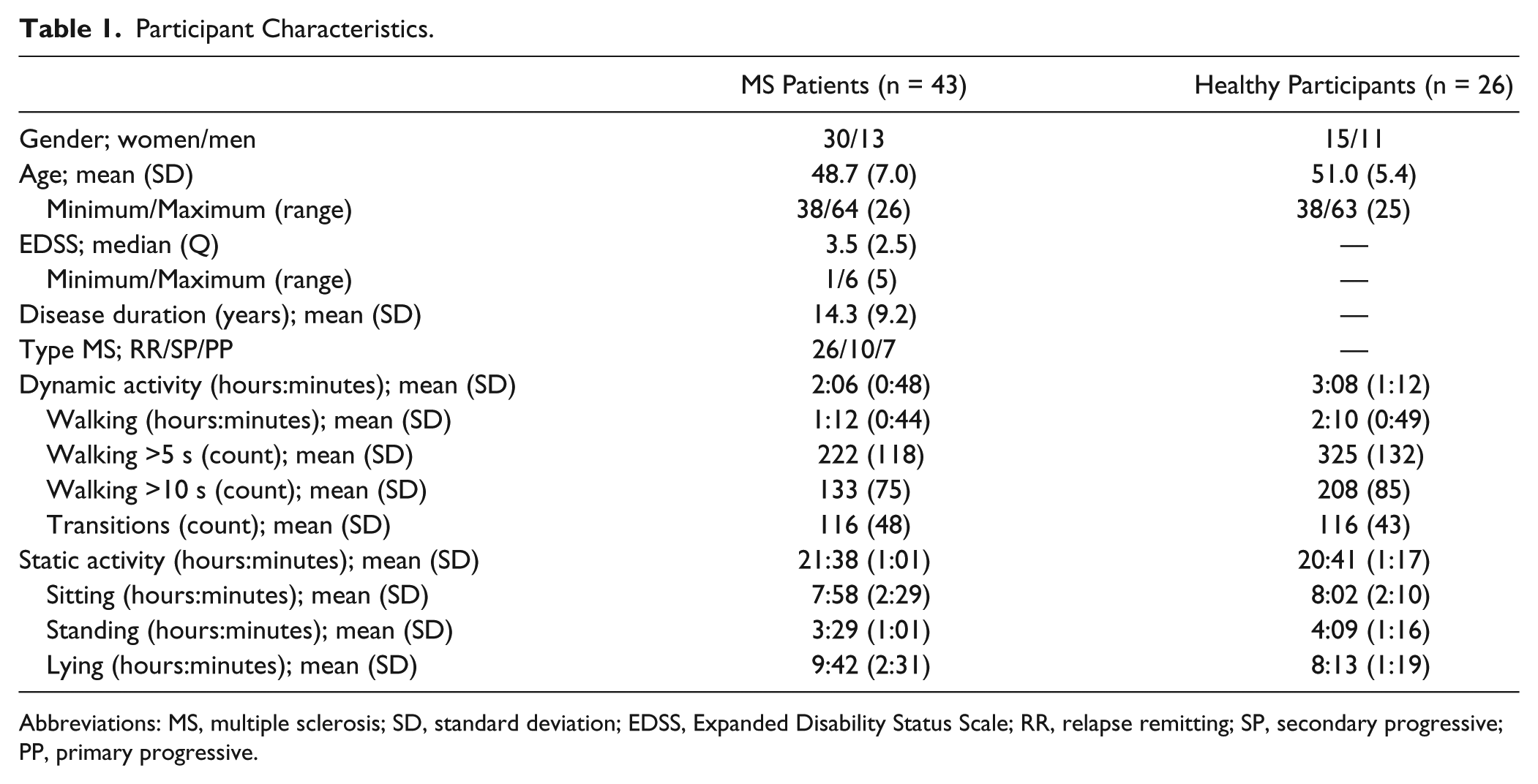
Abbreviations: MS, multiple sclerosis; SD, standard deviation; EDSS, Expanded Disability Status Scale; RR, relapse remitting; SP, secondary progressive; PP, primary progressive.
The duration of applying the AM ranged from 10 to 15 minutes for both assessments. The mean monitoring duration for both groups was 23:48 (standard deviation = 0:37) hours:minutes. On average over the 2 measurements, MS patients showed 2:06 (hours:minutes) and healthy participants 3:08 (hours:minutes) of dynamic activity overall during the 24-hour registration (Table 1).
Differences Throughout the Day
The results of the analyses on the 24-hour registration period are shown in Table 2. Checking our matching procedure for the factors age and gender did not reveal confounding. The time spent on dynamic activity (in hours) was on average 0.27 times lower for patients with MS than for the healthy group over the 24-hour registration (P < .001).
Between-Group Differences (MS Patients Compared With Age- and Gender-Matched Healthy Individuals) During 24-Hour Activity Monitoring. a
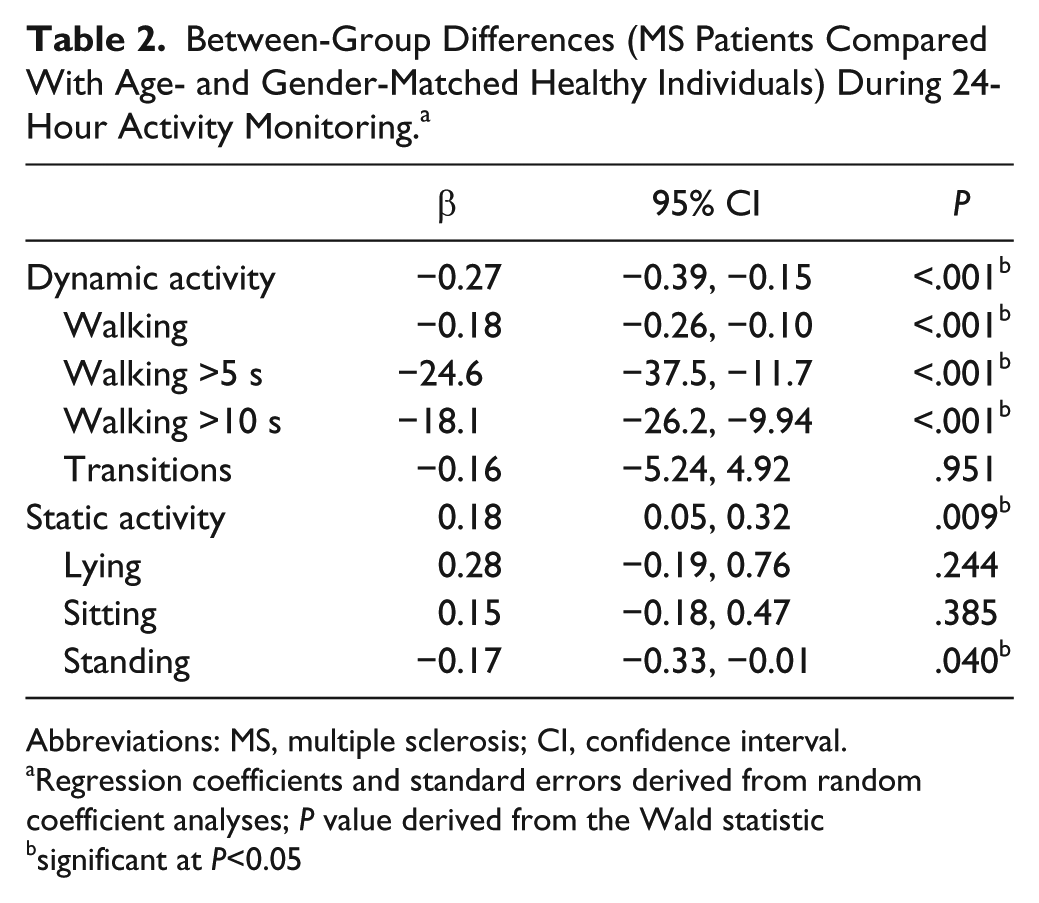
Abbreviations: MS, multiple sclerosis; CI, confidence interval.
Regression coefficients and standard errors derived from random coefficient analyses; P value derived from the Wald statistic
significant at P<0.05
On average, patients with MS spent less time walking and had fewer walking periods (P < .001). No significant between-group differences were found for the dynamic activity subgroup, number of transitions (P = .875). Patients with MS spent more time on overall static activity (P = .003) and less time on its subgroup classification, standing (P = .011). No significant between-group differences were found for the subgroup classifications of static activity—namely, lying (P = .244) and sitting (P = .317).
Differences in Daily Periods
Figure 1 shows the free-living activity patterns for different parts of the day for the time-dependent variables used in this study. Visual inspection of the figures of the mean scores for the outcome time spent on dynamic activity and the subgroup classifications time spent on walking and number of walking periods shows that patterns are quite similar across these variables.
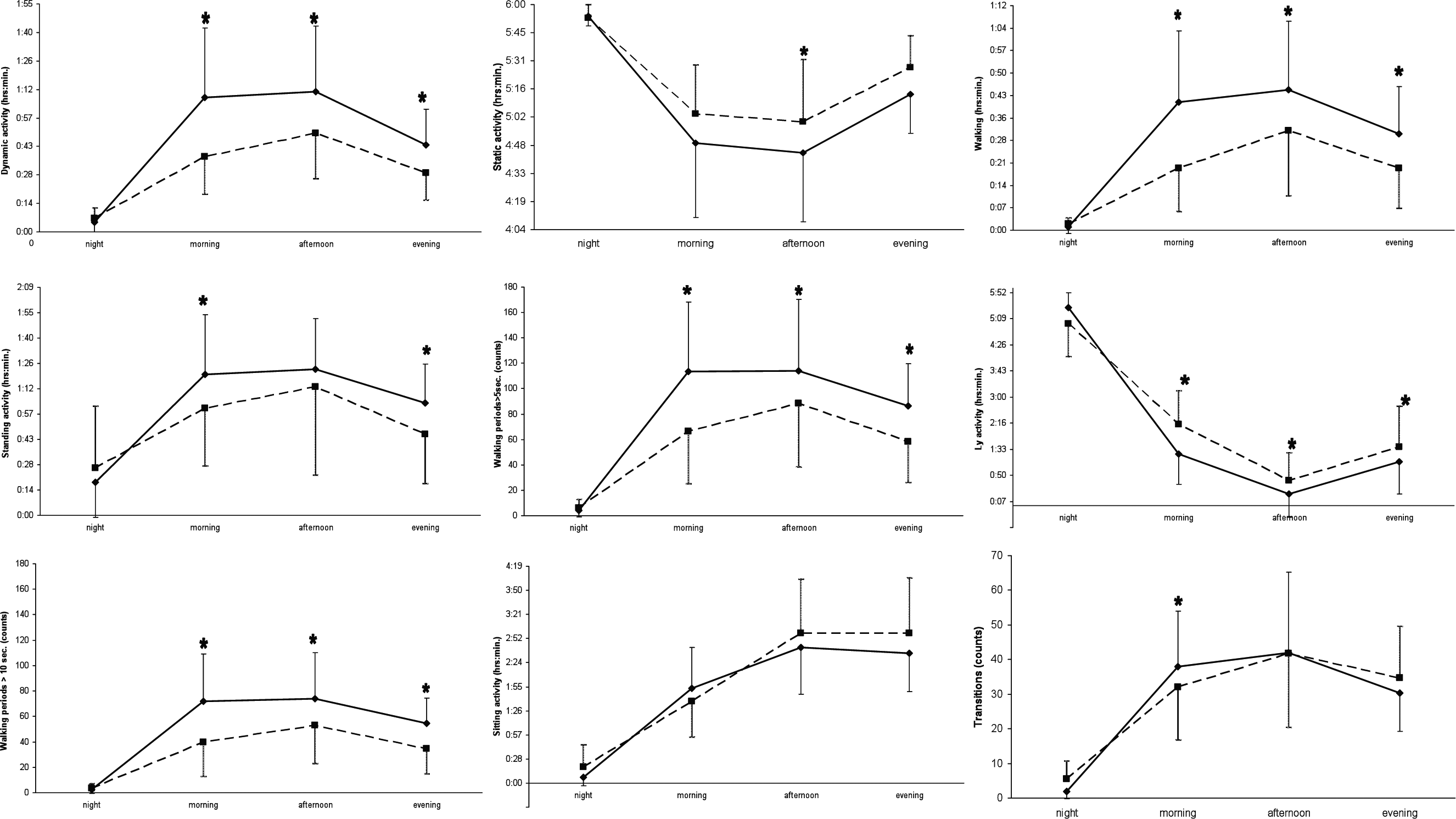
Free-living activity patterns for different parts of the day, means and standard deviations.
Table 3 shows the group differences based on random-coefficient analysis for several free-living activities during different daily periods. Significant Group × Daily period interaction effects are also presented and denoted by asterisks in Figure 1. Briefly, for dynamic activity, patients with MS showed significantly lower activity levels than healthy controls starting in the morning and persisting in the afternoon and evening when compared with the night (P < .05). The profiles for the subgroup classifications of dynamic activity, walking time and walking periods, were quite similar across groups. However, for the dynamic activity subgroup classification amount of transitions, patients with MS had a significantly lower performance level in the morning (P = .045).
Between-Group Differences (MS Patients Compared With Age- and Gender-Matched Healthy Controls) in Dynamic and Static Activities During Daily Periods, Using Night as the Reference Category. a
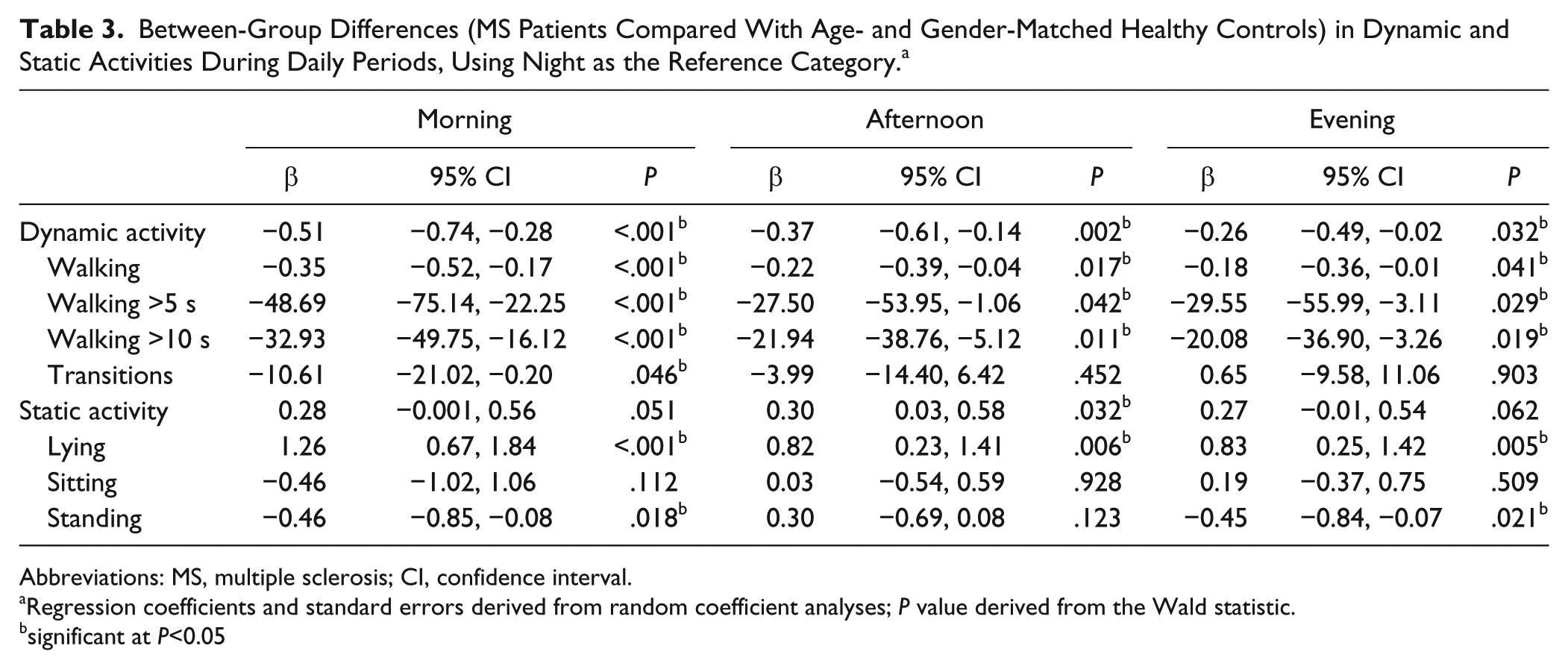
Abbreviations: MS, multiple sclerosis; CI, confidence interval.
Regression coefficients and standard errors derived from random coefficient analyses; P value derived from the Wald statistic.
significant at P<0.05
Overall, patients with MS spent significantly more time in the afternoon (P = .03) on static activities compared with healthy controls. In addition, patients with MS spent significantly more time on the static activity subgroup classification “lying” in the morning (P < .001), afternoon (P = .006), and evening (P = .005) and less time on static activity subgroup classification “standing” in the morning (P = .014) and the evening (P = .017) compared with controls. For time spent on static activity subgroup classification sitting, no significant differences (.112 ≤ P ≤ .928) were found between MS patients and healthy individuals for the different periods of the day.
Discussion
This is the first study in which detailed 24-hour motor activity behavior of patients with MS was monitored and analyzed across 3 different time periods of the day and compared with that of healthy controls. As hypothesized, results showed significantly reduced physical activity performed in patients’ own community environment as compared with a group of healthy controls. These findings substantiate previous studies showing that patients with MS are significantly less physically active than nondiseased people.2-5
Despite the growing evidence on lower global activity levels of patients with MS compared with healthy people, diurnal patterns of performed activities, such as patterns of ambulatory activity that characterize cycles of work and rest, and peak activity levels still need to be quantified. 19 We hypothesized that patients with MS have different patterns of activity because of, for example, motor symptoms and fatigue.6-8 Moreover, based on clinical observations and the literature, we expected patients with MS to be less active in the morning because of a slower start as a result of coping with neurological deficits and, to prevent depletion of energy, and earlier decrement in physical activity in the evening, related to diurnal increment of fatigue levels,11-13 when compared with healthy controls. The expected lower motor activity level of MS patients compared with the healthy group for dynamic activity and its subgroup categories walking time and walking periods was indeed found for the morning, and this pattern persisted throughout the day. On average, patients with MS did have lower dynamic activity levels in the morning and the evening as compared with the afternoon. In addition, patients with MS showed a similar pattern but of different magnitude when compared with a healthy age- and gender-matched group. This finding may have important implications for planning exercise interventions in patients with MS and designing clinical trials.
Two previous studies investigated whether testing of walking capacity 13 or walking pattern, 11 with walking being an important component of dynamic activity, in patients with MS was affected by time of day. Walking capacity was measured with the 6-minute walk test and the 10-m walk test performed at usual or fastest speed. 13 The walking pattern was quantified in terms of gait speed, stride length, cadence, and the percentage of the gait cycle spent in double-limb support. These were measured during 10-m gait trials on preferred walking speed. 11 Both studies found that despite higher levels of fatigue toward the evening, walking capacity and walking patterns remain consistent. These results suggest that mechanisms controlling locomotion are separated from those regulating perceived fatigue 11 and that objective measures of performance, rather than self-report, should be used to monitor change in patients with MS. 11 Our study used an objective measure of physical activity. Moreover, patients were not asked to perform a specific activity, but patients’ natural activity was measured in their own living environment. Our results show a quite strong diurnal pattern for both patients with MS and healthy people, with peak activity during the afternoon hours. This latter finding suggests that the actual performed physical activity is mainly driven by both personal beliefs and perceptions regarding engagement in physical activity as well as anticipation on inflexible activities like work or household chores, rather than by capacity, energy levels, and/or fatigue directly. The patients with MS in our study consisted of a sample from a local outpatient database and referrals from the neurology department. The healthy people in our study were a mix of partners of the patients with MS, students, and colleagues. So activities both between and within groups were very heterogeneous. We did not include assessment of working status. However, working status may have an influence on the physical activity pattern performed. For example, going to work requires a rather inflexible sequence of standard physical activity like getting up, washing oneself, dressing, eating, and traveling in the morning. Future studies should, therefore, combine assessment of physical activity with participation measures, such as work, social involvement, or leisure.
It is interesting to note that patients with MS performed significantly fewer transitions in the morning period. Together with the lower dynamic activity from the morning onward, this latter finding may suggest that patients implement some deliberate strategy to be energy efficient by being less variable in switching between activities (ie, between sitting and standing/walking) early in the day.
Strengths and Limitations
A major strength of the present study is the use of an objective tool that provides information about the effects of a disease on daily physical functioning in terms of postures and motions in the home situation. Measures of ambulatory activity reflect the life situations of individuals interacting with their environment. 19 Following the International Classification of Functioning, Disability and Health, 20 AM measures should be classified at the “Participation” domain.21,22 Moreover, the use of the AM provides a more continuous assessment as well as an objective indication of the type of activities performed as compared with instruments such as self-report questionnaires, and (semi-) structured interviews that are subjective and rely on short- and long-term memory.
Detailed information about the motion and posture profile of patients with MS allows clinicians not only to investigate how patients cope with their neurological deficits but also to evaluate intervention effects and target treatment strategies to keep patients in an optimal physical condition. Future pharmacological and nonpharmacological trials aimed at improving activities and participation should preferably use AM as one of the secondary outcomes in addition to self-report measures and physical performance tests because they may lead to significantly different findings. Accurate measurement allows behavioral changes to be observed in regard to an individual’s ability to adapt during interventions and to incorporate new skills into real-world behaviors. 22 Using outcomes such as AM allows identification of, next to responders and nonresponders in trials, those who show a mismatch between subjective questionnaires and objective outcomes. 5
The present study does have some limitations, which should be considered when interpreting the results. First, a key question in this kind of research is what should be measured to describe normal daily physical activity levels. To describe participants’ activity levels, we used the concept of classification of postures and motions. 17 The output is no more and no less than a set of postures and motions performed during the recording period. 17 It does not provide information on what participants were doing while performing daily activities such as sitting and standing and with that may provide an underestimation of upper body activities. A more elaborate AM setup with accelerometers on the arms could provide such information on participants’ normal daily physical functioning. Furthermore, such a setup enables assessment of nonambulatory, wheelchair-bound patients with MS as well and would provide relevant physical activity information on, for example, wheelchair propulsion activity. Second, there may be variables other than age and gender (eg, fatigue, pain, mood/depression, and quality of life) that may interfere with performed activity level, but these factors were not included in our multilevel models because they were not assessed during 24 hours. To capture the dynamics of everyday fluctuations in such variables, experience sampling methods could be used in which participants are asked to stop at certain times and make notes of their experiences or feelings in real time. 23 Third, the present study involves a registration period limited to 24 hours. However, it is conceivable that dynamic activity patterns show variation over longer timescales (eg, weekly or seasonal variations). Such variability in activity patterns does require a large group size and number of assessments to decrease the within-participant variability and, thus, the measurement error. An intensive repeated measurement design over a prolonged period of time with concurrent assessment of possible influential factors may, therefore, be preferred. On the other hand, we have previously shown that 24-hour AM is a reproducible estimate of physical activity for group evaluation in patients with MS. 16 Finally, although participants were instructed to maintain their usual daily routines, the physical presence of the AM may have influenced daily activity behavior of the participants because they were aware of being tested (so-called reactivity). Moreover, participants were instructed to refrain from showering, which may prevented participants from exercising. 17 We assume that this influence is negligible because of the clear instructions and relatively short recording period of 24 hours. In addition, these effects, if present at all, are expected to be equal between patients and controls.
Conclusions
Activity monitoring gives insight into real-world daily physical behavior. Based on our findings, we conclude that patients with MS show less dynamic activity compared with healthy controls. Similar diurnal dynamic activity patterns, but of different magnitude, were seen for both groups. Our findings suggest that patients with MS may adopt a deliberate anticipatory strategy of lower activity in the morning, which persists throughout the day. Future trials evaluating daily changes in physical activity behavior should simultaneously sample self-report measures of energy levels and fatigue to elucidate the complex interaction between symptoms and physical activity.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Dutch MS Research Foundation (project number 04-553 MS).