
Abstract
Multiple sclerosis (MS) is a heterogeneous disease, both in its pathology and symptomology. This poses a challenge for the medical management and rehabilitation of MS; however, physical activity and exercise training are rehabilitation approaches that have demonstrated beneficial effects on many of the burdensome consequences of MS such as mobility impairment and fatigue. Given the heterogeneous course of MS, it is possible that outcomes of physical activity and exercise training interventions demonstrate heterogeneity both in the magnitude and pattern of change, but there has been little focus on response heterogeneity with these interventions among persons with MS. In this narrative review, a search of the existing literature was performed to identify studies that reported individual participant data, which was used to describe the variability in the response to physical activity and exercise training interventions among persons with MS. Inter-individual variability seemingly occurs across outcomes and modalities, which underscores the consideration of factors that might influence response heterogeneity. Factors related to MS disease characteristics, nervous system damage, and the degree of MS-related disability might influence individual responsiveness. Large-scale studies that permit the examination of heterogeneity and its predictors will inform future research on the area of physical activity and exercise training in MS, and lead to the development of individually tailored rehabilitation approaches that will more effectively elicit change.
Introduction
Multiple sclerosis (MS) is a chronic neuroinflammatory disease that leads to demyelination, degeneration, and transection of axons, and atrophy of neuronal cell bodies and dendrites in the central nervous system (CNS). 1 This disease-related damage occurs throughout the CNS in a heterogeneous pattern, and manifests as a variety of clinical symptoms based on lesion location. People with MS experience common consequences of the disease such as mobility disability, impaired balance, fatigue, cognitive dysfunction, and depressive symptoms, but the frequency and severity of these symptoms is heterogeneous across people with MS. 2 Recognizing that MS is a heterogeneous disease both in its pathology and symptomology is important, as it presents a major challenge for the medical management and rehabilitation of MS.
There is an emerging body of research supporting the beneficial effects of physical activity and exercise training for rehabilitation among people with MS. For example, evidence from meta-analyses have demonstrated positive effects of physical activity and exercise training on mobility,3-5 balance, 6 fatigue,7-9 depressive symptoms,10-12 quality of life, 13 and fitness outcomes. 14 These data exemplify the general improvement in manifestations of MS through the participation in physical activity and exercise. This body of research has further yielded evidence-based guidelines for prescribing exercise in people with MS 15 that are seemingly applicable for people between 18 and 64 years of age with mild through moderate disability with relapsing-remitting or progressive disease courses. 16
Whereas the evidence demonstrating the beneficial effects of physical activity and exercise for rehabilitation among persons with MS is generally promising, there is a dearth of attention directed toward the possibility of heterogeneous outcomes with these interventions. Response heterogeneity, or interindividual variability in the pattern and magnitude of the response to a standardized exercise training or physical activity intervention, likely occurs among persons with MS considering the pathology and expression of MS are heterogeneous and such heterogeneity would likely express itself in the outcomes of these interventions. In addition, the lack of attention on response heterogeneity in persons with MS is surprising given the recognition of response heterogeneity with physical activity and exercise training in the general population of adults without a chronic, disabling disease. For example, results from the HERITAGE Family Study, 17 a large multicenter examination of genetic influences on physiologic adaptations with aerobic exercise training, provided strong evidence of heterogeneity, including changes in maximal oxygen consumption (VO2max), submaximal exercise heart rate, and systolic blood pressure. 18 Such “response heterogeneity” is considered pervasive among all groups of individuals (eg, men and women, old and young), 19 and is likely influenced by a combination of genetic, environmental, and phenotypic factors. 20
This article presents an argument that researchers should examine response heterogeneity with physical activity and exercise training interventions in MS. This argument is based on a review of the literature and presentation of data from individual randomized control trials (RCTs) supporting heterogeneity of changes in outcomes across study participants. Included studies often reported mean changes in outcomes and did not specifically focus on heterogeneity, as little attention has been focused on this topic in MS to date. Next, the MS-specific factors that might influence the heterogeneous changes in outcomes with physical activity and exercise training interventions are highlighted. Finally, an outline of future research directions regarding the examination and reporting of heterogeneity within RCTs of physical activity and exercise training interventions in MS is provided. This article will inform future research on the area of physical activity and exercise training in MS and emphasize the need for precision medicine where treatment is tailored to the individual. The provision of such an article might further address the continual problem of exceedingly low participation rates regarding physical activity in MS. 21
Search Strategy and Heterogeneity Analysis
Literature Search Strategy and Study Selection
As an approach for demonstrating response heterogeneity with exercise training and physical activity interventions in persons with MS, a comprehensive literature search was performed in 3 electronic databases (i.e. PubMed, CINAHL, and Google Scholar) with physical activity and multiple sclerosis, exercise training and multiple sclerosis, resistance exercise and multiple sclerosis, and aerobic exercise and multiple sclerosis as search terms. We further searched reference lists from meta-analyses and systematic reviews of physical activity and exercise training interventions in MS. Titles and abstracts of articles were examined to determine if a given article included a physical activity or exercise training intervention among persons with MS. The remaining papers were inspected to determine if data were presented as either individual participant pre-/postintervention values or individual change scores. Individual participant data could be presented in text, in tables, or graphically. If individual participant data were presented as figures, numeric values were obtained using a free, web-based program (https://automeris.io/WebPlotDigitizer/) that enabled extraction of values from graphically presented data. Overall, 13 articles22-34 met the search criteria, and from those articles, a subset of 8 (Table 1) that clearly exemplified response heterogeneity with exercise training and physical activity interventions among persons with MS were included in this review. The other 5 articles are cited, but not included in detail as the outcome measures were outside of the scope of the current review (eg, neuroimaging outcomes),27,29,30,34 and/or the article included a small sample size with incomplete data. 33
Summary of Studies Demonstrating Response Heterogeneity With Exercise Training and Physical Activity Interventions in Persons With MS. a
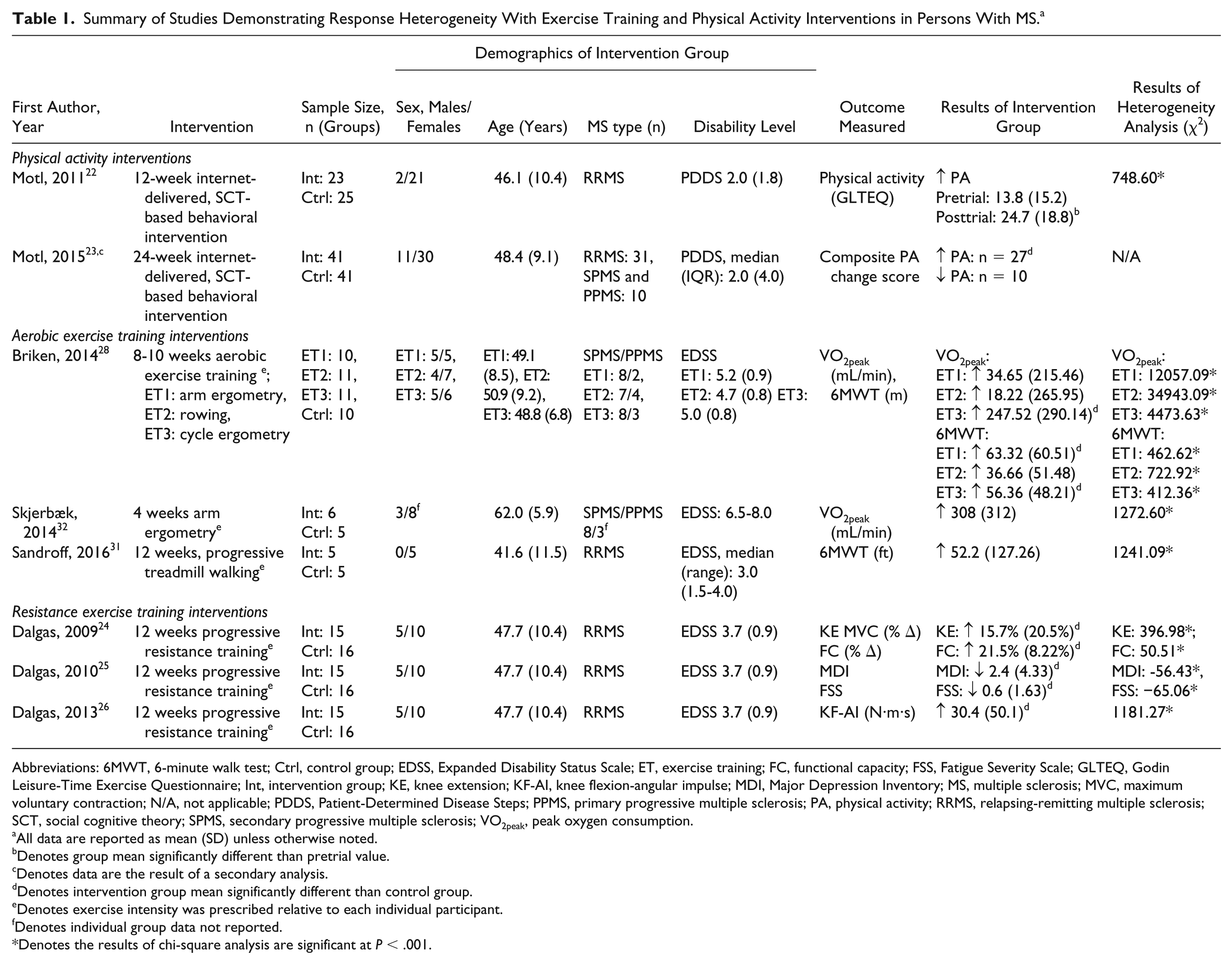
Abbreviations: 6MWT, 6-minute walk test; Ctrl, control group; EDSS, Expanded Disability Status Scale; ET, exercise training; FC, functional capacity; FSS, Fatigue Severity Scale; GLTEQ, Godin Leisure-Time Exercise Questionnaire; Int, intervention group; KE, knee extension; KF-AI, knee flexion-angular impulse; MDI, Major Depression Inventory; MS, multiple sclerosis; MVC, maximum voluntary contraction; N/A, not applicable; PDDS, Patient-Determined Disease Steps; PPMS, primary progressive multiple sclerosis; PA, physical activity; RRMS, relapsing-remitting multiple sclerosis; SCT, social cognitive theory; SPMS, secondary progressive multiple sclerosis; VO2peak, peak oxygen consumption.
All data are reported as mean (SD) unless otherwise noted.
Denotes group mean significantly different than pretrial value.
Denotes data are the result of a secondary analysis.
Denotes intervention group mean significantly different than control group.
Denotes exercise intensity was prescribed relative to each individual participant.
Denotes individual group data not reported.
Denotes the results of chi-square analysis are significant at P < .001.
Heterogeneity Analysis
The primary focus of the current review was to summarize and document interindividual variability of outcomes in response to physical activity and exercise training interventions among persons with MS. To describe the heterogeneity within each study, we borrowed from the tradition of meta-analysis wherein heterogeneity of the average effect is often a focus or point of interest. With a meta-analytic statistical approach, heterogeneity is typically expressed with a q-statistic, which is conceptually the same as a chi-square. To that end, we computed a chi-square (χ 2 ) value per outcome of interest based on the formula:
We then interpreted the significance based on a chi-square distribution for indicating if individual variation around the expected value (ie, mean) was greater than chance. The inclusion of the statistical analysis provides evidence of the interindividual variability present in these studies; however, in general, a more descriptive approach was used to document response heterogeneity with physical activity and exercise training interventions among persons with MS. The results of the chi-square analysis are presented in Table 1, whereas the remainder of the article is dedicated to providing evidence of response heterogeneity via a description of the observed variability within each study.
Response Heterogeneity With Physical Activity and Exercise Training Interventions
Physical Activity Interventions
Physical activity behavior is associated with improvements in depression, fatigue, pain, and disability, 35 yet persons with MS demonstrate exceedingly low levels of physical activity. 21 Behavioral physical activity interventions are designed using theory-based constructs to systematically modify an individual’s physical activity behavior and subsequently improve consequences of MS that are associated with physical activity. 36 Such interventions have generally been successful in increasing the amount of physical activity among persons with MS,22,37-39 but not all individuals experience an increase in physical activity behavior in response to the intervention. 23 One pilot RCT that investigated the effect of a 12-week internet-delivered behavioral intervention on physical activity reported a large increase in physical activity behavior in response to the intervention; however, while several individuals substantially increased physical activity, others demonstrated no change or even a decrease in physical activity (Figure 1). 22
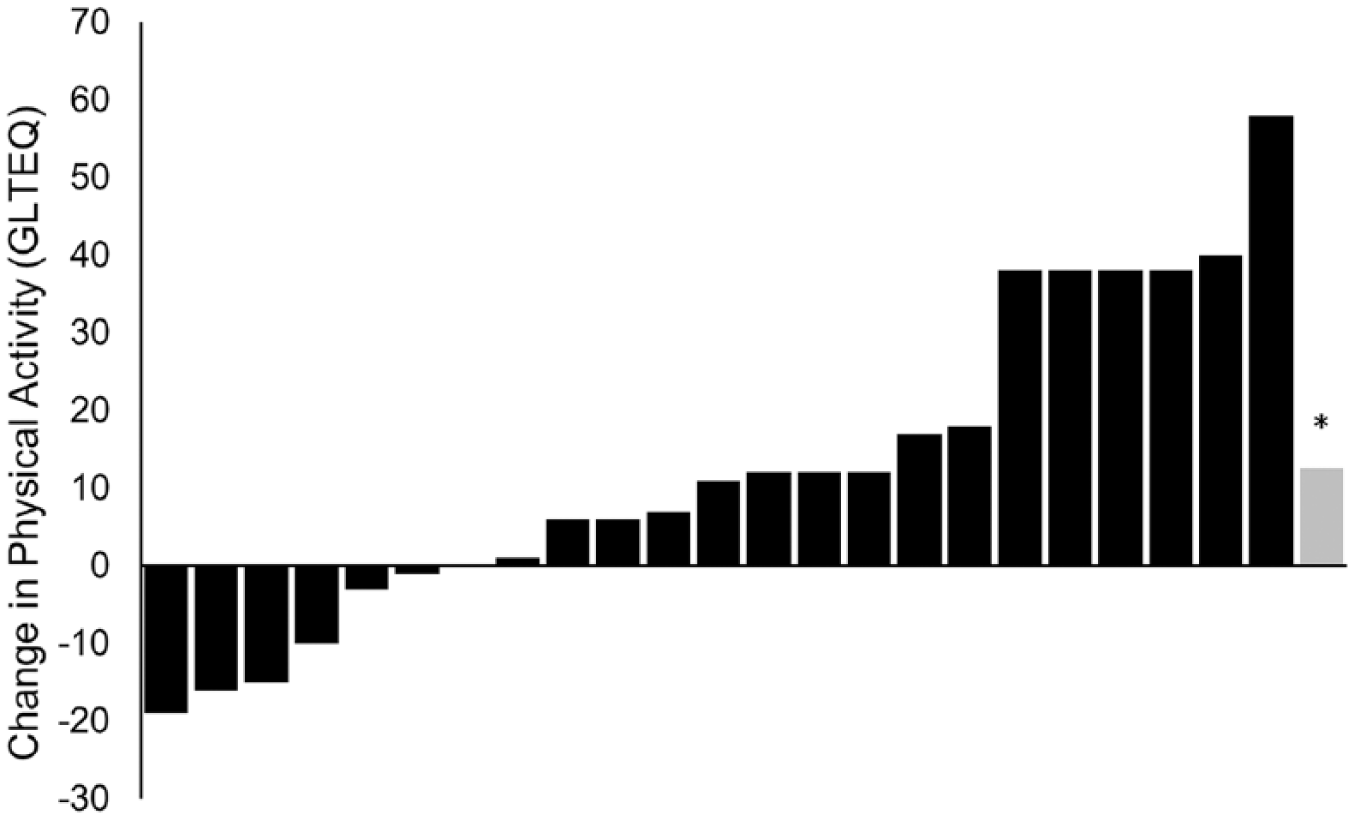
Interindividual variability of the change in physical activity as measured by the Godin Leisure-Time Exercise Questionnaire in response to an internet-based physical activity intervention. 22 Each black bar represents the change in physical activity of an individual participant and the gray bar represents the average change of the group. *Represents a significant difference (p < .01) compared with the pretrial value.
The presence of interindividual variability in response to a behavioral physical activity intervention prompted further investigation of the moderating factors that might influence response heterogeneity with physical activity interventions in MS. 23 One secondary analysis of data from another internet-delivered behavioral intervention designed to increase physical activity among persons with MS 39 demonstrated an overall mean increase in physical activity within the intervention condition compared to the control condition; however, 10 of 37 participants in the intervention condition experienced a decrease in physical activity. The magnitude of change in physical activity was subsequently examined by characteristics that might potentially modify the efficacy of the intervention, and this analysis indicated that MS type, disability status, and weight status were moderators of the intervention effect on physical activity behavior.
Aerobic Exercise Training
The characteristic physiologic response resulting from aerobic exercise training is improved cardiorespiratory fitness. 40 Typically, improved cardiorespiratory fitness reflects the capacity of the body to transport and use oxygen during exercise, and is often measured as peak oxygen consumption (VO2peak), peak power output, and anaerobic or lactate threshold. One recent meta-analysis that examined the effects of exercise training on cardiorespiratory fitness in persons with MS reported a 17.7% increase in VO2peak following exercise training. 14 Indeed, many RCTs involving persons with MS have demonstrated that cardiorespiratory fitness is significantly improved at the group level following aerobic exercise training28,41-48; however, when examining the individual-level data from each study, it is apparent that not all participants improved to the same extent or in a uniform pattern, as some persons do not improve and others demonstrated declines in cardiorespiratory fitness. For example, a considerable amount of heterogeneity in the change in VO2peak after aerobic exercise training was reported in a pilot RCT that examined 3 different aerobic training modalities (arm ergometry, rowing, and cycle ergometry) in persons with MS (Figure 2A). 28 Two out of 11 participants in the cycle ergometer group, which as a whole was reported to have a statistically significant increase in VO2peak, actually demonstrated a sizeable decline in cardiorespiratory fitness after exercise training. There was not a statistically significant mean increase in VO2peak in the arm ergometry or rowing groups, but a large amount of interindividual variability was present with changes that ranged between −358.42 mL/min and +265.35 mL/min in the arm ergometer group and between −518.81 mL/min and +403.96 mL/min in the rowing group. Another study examined the effect of 4 weeks of aerobic exercise training with arm ergometry on cardiorespiratory fitness and reported an average increase in VO2peak of +308 mL/min (trend toward significant change, p = .06) among 6 individuals with progressive MS (Figure 2B). 32 Regarding individual change, 4 participants responded similarly to the exercise training protocol; however, 1 participant demonstrated a −60.97 mL/min decline in VO2peak while another participant had an increase in VO2peak of nearly +800 mL/min; this exemplified that a wide range of responses are evident even within a small sample of participants.
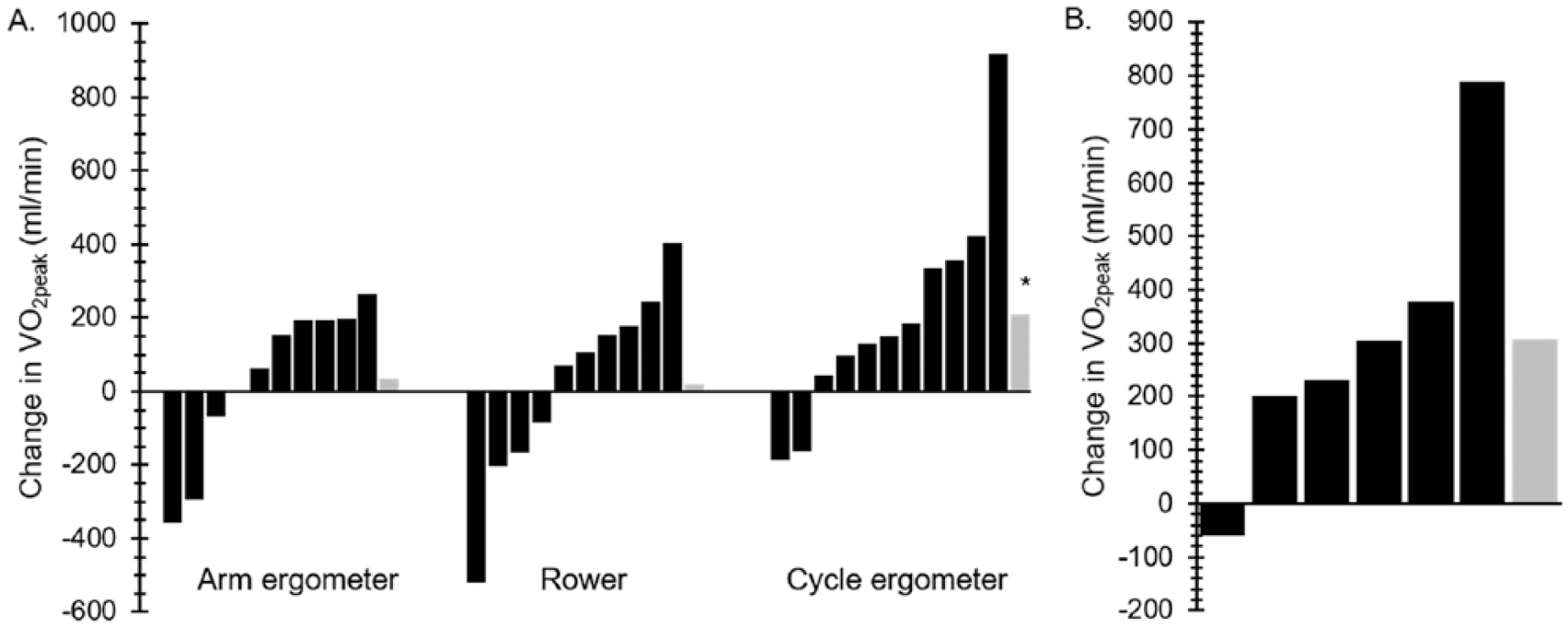
Interindividual variability of the VO2peak response with aerobic exercise training in persons with multiple sclerosis (MS). (A) The individual change in VO2peak after 8 to 10 weeks of standardized aerobic exercise training with arm ergometry, rowing, or cycle ergometry. 28 (B) The individual change in VO2peak after 4 weeks of standardized arm ergometry training. 32 Each black bar represents the change in VO2peak of an individual participant and the gray bar represents the average change of the group. *Represents a significant difference (p < .05) compared with the change in the control group. VO2peak, peak oxygen consumption.
Aerobic exercise training further has yielded positive mean improvements in mobility, indicated by changes in walking speed, walking endurance, and functional mobility, in persons with MS.28,47,49-51 However, response heterogeneity involving mobility outcomes is evident with aerobic exercise training. The previously discussed study that examined the effects of arm ergometry, rowing, and cycle ergometry on VO2peak in persons with MS 28 further investigated the effect of these aerobic exercise training modalities on mobility. There was a significant improvement on the 6-minute walk test (6MWT), a measure of walking endurance, for both the arm ergometry and cycle ergometry conditions (Figure 3A); however, there were some individuals in the conditions that demonstrated minimal change, or even a decline in performance, whereas others more than doubled the improvement compared with the group mean. There was a similar distribution of responses observed in a small pilot RCT that investigated treadmill exercise training in 5 individuals with MS. 31 There was a large intervention effect (d = 0.76) on the 6MWT after 12 weeks of exercise training (mean increase of 52.2 ft), but the change in 6MWT distance ranged between a decline of −80 ft and an increase of +256 ft (Figure 3B).
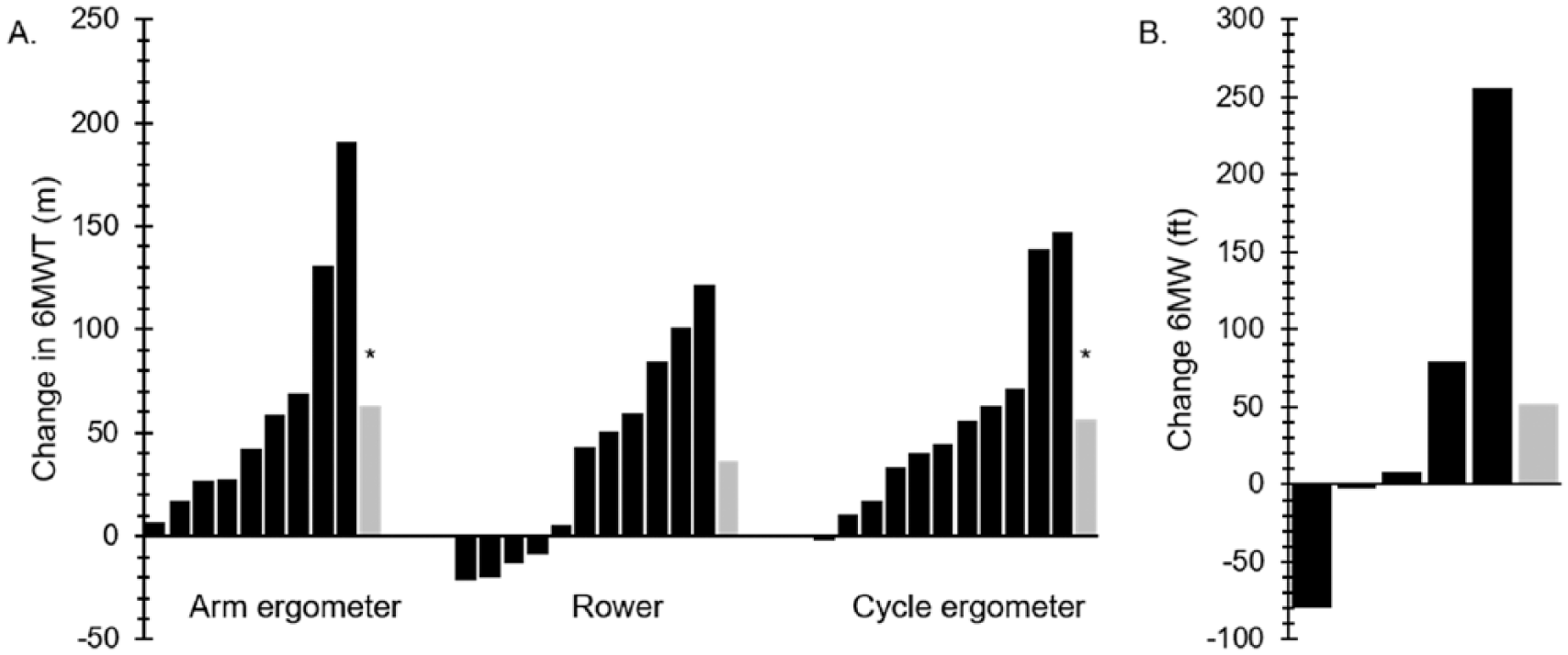
Interindividual variability of the change in 6-minute walk test (6MWT) distance with aerobic exercise training in persons with multiple sclerosis (MS). (A) The individual change in 6MWT distance after 8 to 10 weeks of standardized aerobic exercise training with arm ergometry, rowing, or cycle ergometry. 28 (B) The individual change in 6MWT distance after 12 weeks of standardized treadmill training. 31 Each black bar represents the change in 6MWT distance of an individual participant and the gray bar represents the average change of the group. *Represents a significant difference (p < .05) compared with the change in the control group.
Resistance Exercise Training
The beneficial effects of resistance exercise training on muscular strength have been well-documented in the general healthy population, and these benefits further have been demonstrated in persons with MS.14,52,53 Resistance exercise training is considered a safe rehabilitative technique in MS that consistently results in improved strength. 54 However, not all individuals experience the same increase in strength with the same exercise training stimulus. For example, after 12 weeks of lower-extremity progressive resistance exercise training in persons with MS, isometric knee extensor muscle strength significantly increased by an average of +15.7%; however, 3 of 15 participants demonstrated a decline in strength after exercise training, whereas one participant increased strength by more than +80% (Figure 4A). 24 There was a similar distribution of change when examining isometric knee flexor strength. 26 Isometric knee flexor strength, indicated as the change in angular impulse during maximal contraction, significantly increased by an average of +30.4 ± 50.1 N·m·s (24.6%) after resistance exercise training, but 4 of 15 participants increased strength less than +5 N·m·s, and 2 of those 4 participants actually had a substantial decrease in strength (–48.63 N·m·s and −66.17 N·m·s; Figure 4B).
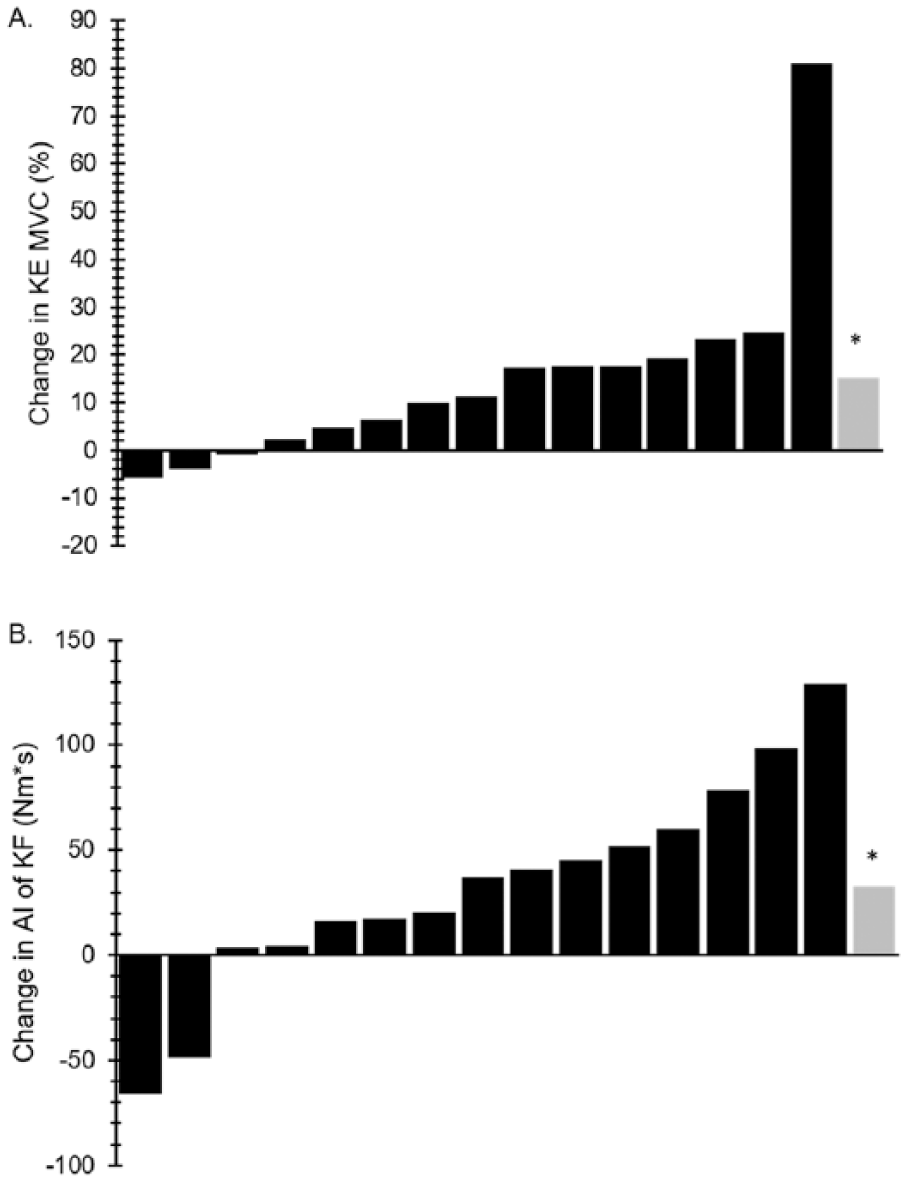
Interindividual variability of the change in knee extensor strength 24 (A) and knee flexion strength 26 (B) after 12-weeks of progressive resistance exercise training. Each black bar represents the change in strength of an individual participant and the gray bar represents the average change of the group. *Represents a significant difference (p < .05) compared with the change in the control group. KE MVC, knee extensor maximal voluntary contraction; AI, angular impulse; KF, knee flexors.
The effect of resistance exercise training on mobility-related outcomes is not as consistent as its effect on strength, 52 yet several RCTs have demonstrated a positive effect of resistance exercise training on walking speed,24,55,56 walking endurance,24,55-57 and other functional mobility tasks.24,56-58 For example, mobility, measured as a composite functional capacity score that consisted of a chair stand test, a stair-climbing test, the 10-meter walk test (10MWT), and the 2-minute walk test (2MWT), significantly increased by an average of +21.5% after 12 weeks of progressive resistance exercise training. 24 However, 2 of 15 participants demonstrated less than a 10% increase in performance, illustrating that not all individuals changed similarly in response to the standardized exercise training program (Figure 5).
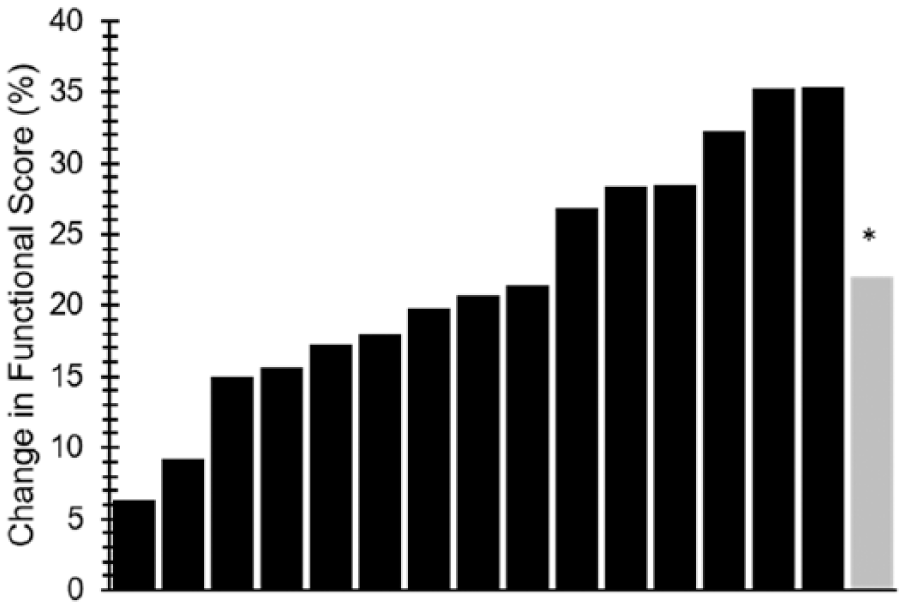
Interindividual variability of the change in functional mobility 24 after 12 weeks of progressive resistance exercise training. Each black bar represents the change in score of an individual participant and the gray bar represents the average change of the group. *Represents a significant difference (p < .05) compared with the change in the control group.
Fatigue and depression are among the most common and burdensome symptoms of MS. 2 Importantly, resistance exercise training has demonstrated positive effects on both fatigue7,9 and depressive symptoms10-12 in persons with MS. One RCT examined the effects of 12 weeks of progressive resistance exercise training on fatigue and depressive symptoms and reported significant improvements in both fatigue (a reduction of 0.6 on the Fatigue Severity Scale) and depressive symptoms (a reduction of 2.4 on the Major Depression Inventory) compared with the nonexercise control group. 25 The average improvement in fatigue was largely driven by 2 high responders who demonstrated substantial reductions in fatigue severity compared with other participants in the exercise group, and this masked the observation that several individuals experienced a worsening of fatigue with the resistance exercise training program (Figure 6A). Although most individuals experienced an improvement in depressive symptoms, 3 of 15 participants reported depressive symptoms that were worse after resistance exercise training, and 1 participant demonstrated a large (>10 points) improvement that greatly influenced the overall average change (Figure 6B).
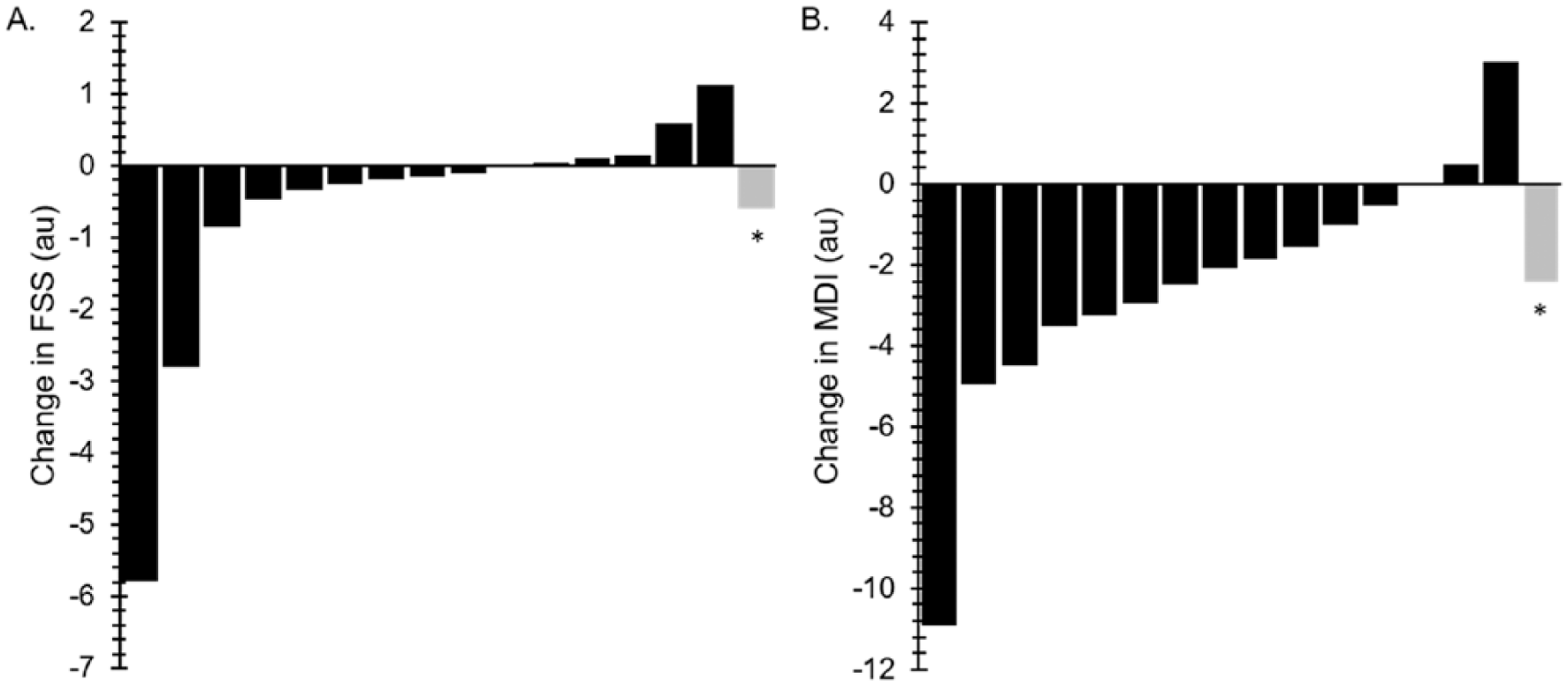
Interindividual variability of the change in fatigue (A) and depressive symptoms (B) after 12 weeks of progressive resistance exercise training. 25 Each black bar represents the change score of an individual participant and the gray bar represents the average change of the group. *Represents a significant difference (p < .05) compared with the change in the control group. FSS, Fatigue Severity Scale; MDI, Major Depression Inventory.
Factors Contributing to Response Heterogeneity
There is clear evidence of response heterogeneity with exercise training and physical activity interventions among persons with MS. This variability seemingly occurs across outcomes and exercise modalities, which underscores the consideration of factors that might influence response heterogeneity and guide the development of individualized exercise prescriptions that optimize the efficacy of exercise and physical activity interventions. To that end, a brief overview of non-MS-specific factors that may influence response heterogeneity in the general population is provided (see Bouchard and Rankinen, 18 Bouchard et al, 59 and Mann et al 60 ), as these factors are likely to influence response heterogeneity among persons with MS. Next, specific factors that might explain interindividual variability in outcomes with exercise training and physical activity interventions in MS are highlighted.
The response to exercise training and physical activity interventions is explained by a myriad of factors. Among these factors, genetics is thought to be one of the main contributors to individual variation.20,59 For example, an analysis of data from the HERITAGE Family Study indicated that the heritability (ie, an estimate of the variance that is attributable to genetics) of the VO2max response to aerobic exercise training was 47%. 61 Sex and age have been considered as sources of variability, but these traits have not consistently demonstrated direct influence on the response to exercise training.18,62 There is evidence that an individual’s baseline level or pretraining measurement of a specific characteristic may influence the magnitude of the response of that characteristic after exercise training wherein individuals with poorer baseline performance experience a greater response to training, although this notion may be limited by a ceiling effect that prevents those with better baseline measures from demonstrating improvement. 60 Other molecular and biological factors such as microRNA expression,63,64 muscle fiber type concentration,65,66 androgen receptor concentration, 67 and phosphorylation status of signaling proteins, 68 among others69,70 might influence individual responsiveness with exercise training and physical activity interventions. Of note, the significance or impact of these factors may be different when considering them within the context of persons with MS compared with the general population, as many of these potentially modifying characteristics are altered by the pathophysiology of MS. For example, persons with MS may experience a shift in muscle fiber type concentration 71 that influences their responsiveness to an intervention differently compared with persons without MS. Factors related to study design should also be considered as a source of variability. These may include factors such as the validity and reliability of the outcome measure, the fidelity/adherence to the training protocol or intervention, and the protocol-specific training parameters (eg, exercise mode, duration, frequency). Particular consideration should be given to unspecified, subjective influences on seemingly objective outcome measures. For example, spiroergometric cardiorespiratory fitness testing may be susceptible to both the participant’s perception of the test (eg, motivation to continue, perceived exertion) and the influence of the examiner (eg, ability or inability to motivate a participant to continue). In addition, participant-specific subjective variables such as motivation, sleep quality, and mood may influence the efficacy, and thereby responsiveness, of an intervention and should also be considered.
Beyond those general factors, response heterogeneity with exercise training and physical activity interventions in persons with MS is likely explained by disease-related factors. MS-specific phenotypic factors are the result of an individual’s genetics and the environment (Figure 7), and these factors may strongly influence a participant’s response to an exercise training or physical activity intervention. There are 3 core categories of phenotypic factors that should be considered as moderators of an individual’s responsiveness to these interventions. MS disease characteristics, such as MS type and disease duration; CNS damage, including the severity and the location; and MS burden, which incorporates symptomology and the degree of disability.
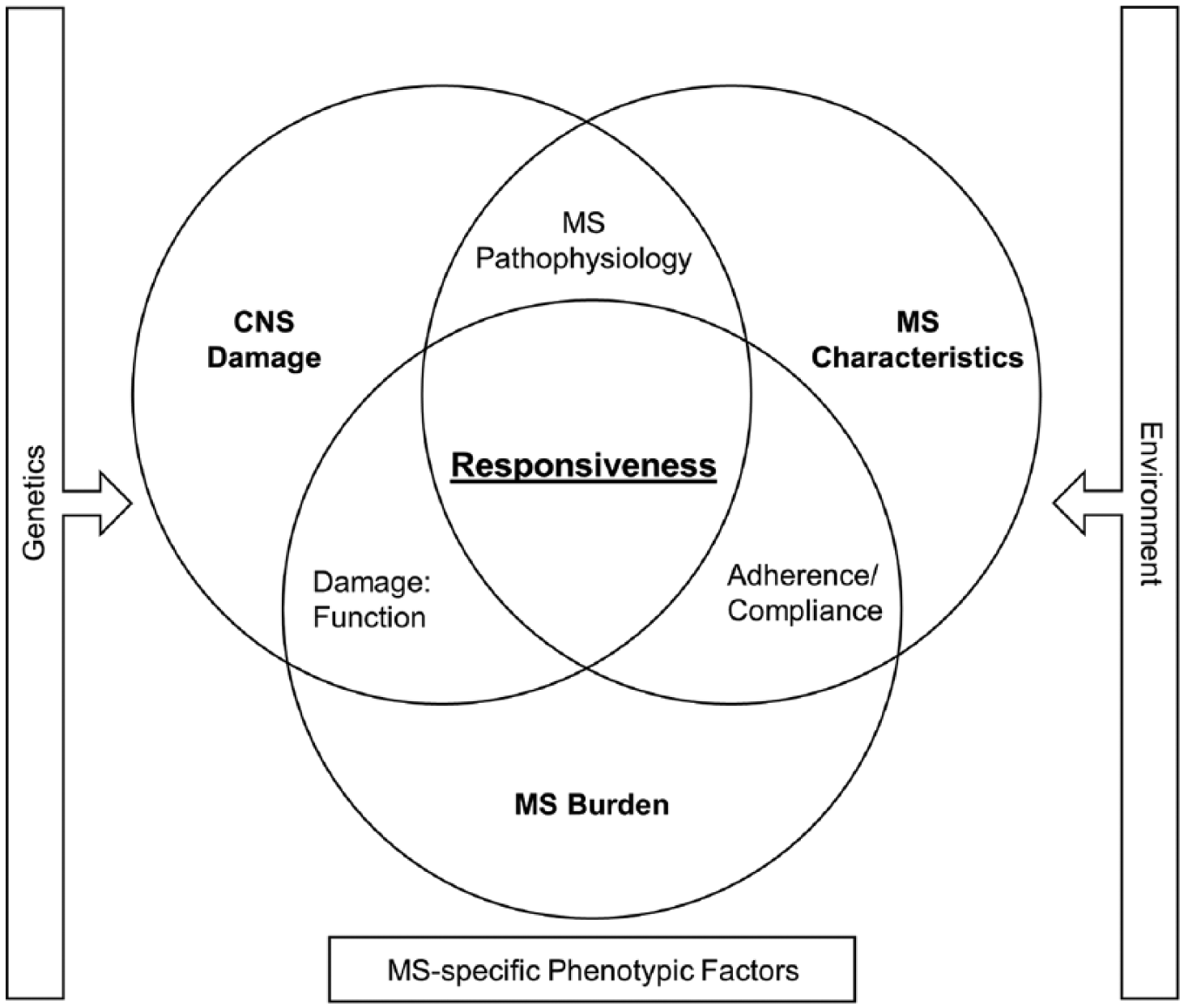
Multiple sclerosis (MS)–specific phenotypic factors that possibly influence response heterogeneity with exercise training and physical activity interventions. Relationships between the 3 core factors (central nervous system [CNS] damage, MS burden, and MS characteristics) create additional factors that also need to be accounted for when considering individual responsiveness.
There is evidence among persons with MS that supports these factors as determinants of responsiveness with exercise training and physical activity interventions. For example, an increase in lower-extremity muscular strength correlated with an increase in neural drive after a 12-week progressive resistance training program among persons with MS. 26 This suggests that individuals who were incapable of altering neural drive, possibly due to preexisting MS-related CNS damage, were unable to demonstrate the expected response to the training stimulus (ie, increased strength). However, it should be noted that the degree of CNS damage was not characterized in these individuals and therefore it is impossible to determine if MS pathology directly prevented neuroplasticity and ultimately the lack of improved strength among these low-responding individuals.
Similar to how poorer baseline function has been associated with greater improvement in function in the general population, baseline function may be a determinant of change in persons with MS. One RCT that examined the effects of an internet-based exercise training intervention on fatigue in persons with MS did not yield a statistically significant change in fatigue in response to the intervention; however, a subgroup analysis indicated that there was a beneficial effect on fatigue for those with lower baseline aerobic capacity and those with lower aerobic capacity plus more severe fatigue at baseline. 72 A randomized crossover controlled study that investigated the effect of aerobic exercise training on walking capacity yielded a similar response wherein individuals who were more disabled tended to benefit more from the exercise training intervention. 48
Conversely, a greater MS-related disease burden may limit an individual’s ability to fully participate in the exercise training or physical activity intervention at the prescribed frequency or intensity thereby undermining the robustness of the response. For example, a secondary analysis of data from an internet-delivered behavioral physical activity intervention suggested that individuals with less disability, indicated by a Patient-Determined Disease Steps (PDDS) score of ≤2, demonstrated greater benefit from the intervention compared to individuals with greater disability (PDDS score of 3-6). 23 The authors suggest that participants with less accumulative burden of disease may possess the greatest capacity to adopt a walking-based physical activity intervention. However, whether related to the factor being considered, the intervention, and/or the outcome of interest, baseline status may not influence responsiveness. One study that compared the effect of short-term interval exercise training on fatigue, depression, and fitness between normal-weight and overweight persons with MS reported no significant relationship for weight status interactions for any outcome, suggesting that exercise was effective independent of baseline weight status in persons with MS. 73
Limitations
We completed a thorough search of the literature and identified exemplar articles that demonstrated response heterogeneity with exercise training and physical activity interventions among persons with MS, but a formal systematic review was not performed. In addition, when data were presented in figure form, numeric values were extracted with a web-based software program that may have returned values slightly different from the original study data. However, the mean value derived from the extracted data was compared to the reported mean value to ensure the accuracy of the extracted data. Only a small number of studies that provided individual participant data or evidence of response heterogeneity were located; however, this is likely related to the dearth of studies that have investigated inter-individual variability with outcomes of these interventions in persons with MS, rather than the fault of the literature search. Many studies continue to emphasize average group differences and main effects, whereas information regarding the individual response to an intervention remains limited. Such a heavy focus on group differences overshadows participants who experienced little, if any, response to an exercise training or physical activity intervention. Additionally, many studies that have reported individual participant data have done so in small samples that are poorly characterized limiting the value of the information that can be derived from such data.
Future Research Directions and Conclusion
The beneficial effects of exercise and physical activity in persons with MS is undeniable; however, the efficacy of these interventions is not ubiquitous. While currently under studied among persons with MS, evidence of response heterogeneity with exercise training and physical activity interventions exists and suggests that participant-specific factors differentially influence the adaptations typically observed with these interventions. To identify the moderating factors that might explain the variability in responsiveness to such interventions, researchers should develop large-scale studies that permit the examination of heterogeneity and its predictors. For example, an ongoing study comparing the effectiveness of a clinic-based versus a home-based exercise intervention among 820 participants with MS will examine each study outcome by age, race, sex, severity of MS, and other demographics to assess the effectiveness of the intervention across groups of individuals. 74 Another phase III RCT is currently investigating the effects of a behavioral intervention for increasing physical activity in persons with MS and will examine the moderating variables of physical activity behavior change and secondary outcomes in 280 persons with MS. 75 These large-scale studies that examine response heterogeneity with exercise training and physical activity interventions are a strong first step in a systematic line of research designed to (a) identify the specific factors that contribute to the effectiveness of such interventions and (b) promote the development of exercise training and physical activity treatment plans that are individually tailored to elicit the greatest response. Altogether, a specific focus on the study of heterogeneity provides the opportunity to distinguish factors that limit change in response to exercise training and physical activity interventions, and subsequently develop strategies to overcome or circumvent these limitations.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JFB is supported by the National Institutes of Health training grant (2T32HD071866-06).a